Embed Size (px)
Citation preview

ORIGINAL ARTICLE
Primary failure of eruption: Furthercharacterization of a rare eruption disorderSylvia A. Frazier-Bowers,a Karen E. Koehler,b James L. Ackerman,c and William R. Proffitd
Chapel Hill, NC, and Jacksonville, Fla
Introduction: Posterior open bite has several possible causes, including primary failure of eruption (PFE) thataffects all teeth distal to the most mesial involved tooth, mechanical failure of eruption (MFE) (primarilyankylosis) that affects only the involved tooth or teeth, and soft-tissue interferences with eruption (other).Methods: Radiographs and other clinical records for 97 cases of failure of posterior eruption submitted forconsultation were analyzed to further characterize PFE and distinguish it from MFE. Results: Of the 97 cases,38 were judged to be clear-cut PFE; 19 were diagnosed as MFE; 32 were classified as indeterminate failurebecause they were too young to be certain of the distinction between PFE and MFE; and 8 were placed inthe “other” category. Two subtypes of PFE were observed. In type 1, eruption failure occurred at or near thesame time for all teeth in an affected quadrant. In type 2, a gradient of the time of failure was present, so thatsome further development of the teeth posterior to the most mesial affected tooth was observed beforeeruption failure. A family history of eruption problems was noted in 10 of the 38 PFE subjects (26%), and apedigree analysis was done for 4 families. This was consistent with autosomal dominant transmission.Conclusions: The distinction between PFE and MFE is clinically important because it determines whether allposterior teeth, or only individual affected teeth, will not respond to orthodontic force. Certain diagnosis oftenrequires progress radiographs so that the pattern of eruption of teeth distal to the most mesial affected toothcan be observed. (Am J Orthod Dentofacial Orthop 2007;131:578.e1-578.e11)
Normal eruption of teeth is of fundamentalimportance to dentists and orthodontists. Thenormal eruptive process involves navigation
through bone and oral epithelium in a precise, bilater-ally timed sequence that must be coordinated with thegrowth of the jaws in all 3 planes of space. It isincorrect to think that an erupting tooth forces its waythrough the overlying tissues. Instead, the controllingelement is resorption of overlying bone, tooth roots,and the alveolar mucosa. Experiments in dogs, andinadvertent experiments in humans, showed clearly thatan eruption path is cleared, and then the tooth movesalong� the� path� that� has� been� created� for� it.1,2
Eruption failure can be attributed to various envi-ronmental and genetic factors. Obstacles to eruption
can include cysts, other teeth, bone, unfavorable tongueposture, and a digit habit. The obstruction can also beintegral to the tooth in the form of fusion of cementumto bone. The resulting ankylosis prevents further erup-tion. Eruption failure due to mechanical obstructionmight be considered a secondary failure, because theeruption mechanism is normal. If the obstruction isremoved, eruption usually resumes; if not, the previ-ously obstructed tooth or teeth can be moved orthodon-tically. Because an area of the periodontal ligament(PDL) is abnormal or absent when ankylosis occurs,permanently removing this type of mechanical obstruc-tion is impossible. If a small area of ankylosis is brokenby manipulating the tooth, it might be possible to moveit for a short time, but reankylosis is inevitable.
The term primary failure of eruption (PFE) wascoined� by� Proffit� and� Vig3� to� describe� a� condition� inwhich malfunction of the eruption mechanism causesnonankylosed teeth to fail to erupt. The primary iden-tifying characteristic is failure of an affected tooth tomove along the eruption path that has been cleared forit. Involved teeth can erupt partially and then cease toerupt, becoming relatively submerged although notankylosed. Only posterior teeth are affected, so theresult is a posterior open bite, and all teeth distal tothe most mesial affected tooth also are affected. Thecondition is rarely symmetric and frequently unilateral,but it can affect any or all of the posterior quadrants. A
aAssistant professor, Department of Orthodontics, School of Dentistry, Uni-versity of North Carolina, Chapel Hill.bPrivate practice, Jacksonville, Fla.cAdjunct professor, Department of Orthodontics, School of Dentistry, Univer-sity of North Carolina, Chapel Hill.dKenan professor, Department of Orthodontics, School of Dentistry, Universityof North Carolina, Chapel Hill.Supported in part by NIH grant 1K23RR17442 from NIDCR and UNC(GCRC) grant RR-00046.Reprint requests to: Sylvia A. Frazier-Bowers, Department of Orthodontics,School of Dentistry, University of North Carolina, Chapel Hill, NC 27599-7450; e-mail, [email protected], July 2006; revised and accepted, September 2006.0889-5406/$32.00Copyright © 2007 by the American Association of Orthodontists.doi:10.1016/j.ajodo.2006.09.038
578.e1

key characteristic is an abnormal or complete lack ofresponse to orthodontic force, so that affected teethcannot be moved into their proper positions. A nonan-kylosed tooth with PFE is likely to become ankylosedwhen force is applied. Although the cause of PFE isunknown, it was presumed that a genetic disturbancewith varying penetrance and expressivity is the mostlikely� explanation,3� and� subsequent� reports� of� PFEhave� described� a� familial� component.4-8
Since the original article describing PFE, orthodon-tists have been sending patient records with unusualproblems in eruption of posterior teeth to the Universityof North Carolina (UNC) for evaluation and consulta-tion.3� By� 2005,� 112� cases� had� been� obtained.� Using� thiscollection of clinical records, we further characterizedPFE, offering guidelines to distinguish it from othercauses of posterior open bite (especially first-molarankylosis with which it easily can be confused inyounger patients) and examining its hereditary nature.
MATERIAL AND METHODS
For inclusion in this study, the minimum record wasa clear panoramic radiograph showing a problem witheruption of posterior teeth, but photographs, follow-uppanoramic radiographs, and cephalometric radiographswere available for many patients. Any informationfrom the referring orthodontist was recorded, such aspatient demographics, significant medical and dentalhistories, family history, treatment approaches, andresponse to treatment if it was attempted. From theinitial sample, 2 subjects were excluded due to success-ful orthodontic correction that was evidence of delaybut not of failure of eruption, and 13 others wereremoved from the sample because of a missing pan-oramic radiograph, a suspected syndrome, or surgery ina location that might have interfered with eruption. Theremaining 97 subjects in the study included 50 males,
46 females, and 1 sex unknown (data not provided).The sample population represented 24 states and Ire-land, with ages ranging from 7 to 29 years. Dental agewas� established� according� to� the� method� of� Demirjian.9
Observation periods ranged from a single time to 9years, with an average of 3 years. There was a reportedfamily history of eruption disturbances in 9 families,comprising 15 of the 97 subjects.
The subjects were classified into 1 of 4 categories,based on their radiographic characteristics. PFE was thediagnosis� if� the� characteristics� listed� in� Table� I� (underPFE) were present. If the radiographic appearance wastypical of ankylosis, with apparently normal eruption ofteeth distal to the affected tooth (usually a permanentfirst molar), the diagnosis was mechanical failure oferuption (MFE), which acknowledges that a morerigorous definition of ankylosis was not possible fromthe records available for this study. A key distinguish-ing characteristic between PFE and MFE is whetherdistal teeth are normal or affected, but this cannot bedetermined in the early stages of development. Patientsin whom the distinction could not be made were labeledas indeterminate failure of eruption (IFE). Eruptionproblems that were neither PFE nor MFE were placedin the “other” category.
Subjects whose referring orthodontist indicated a fam-ily history of eruption problems were interviewed, per-mission was requested to contact the family, and theirfamilies were recruited to participate in this study. This
Fig 1. In sample of 97 subjects, 39% had PFE, 33%had IFE, 20% had MFE, which includes impaction andankylosis, and 8% did not fit into any category (other).
Table I. Diagnostic characteristics of posterior open bite
1. PFE! Eruption path cleared, no eruptive movement along path! Teeth distal to most mesial affected tooth also involved! Any or all posterior quadrants involved
2. MFE! Radiographic appearance of submergence due to ankylosis! No clearance of eruption path! Teeth distal to most mesial affected tooth apparently normal
3. IFE! Distinction between PFE and MFE not clear! Too young to determine whether teeth distal to most mesial
affected tooth are affected or normal4. Other
! Affected teeth not in occlusion but not submerged as in PFEor MFE
American Journal of Orthodontics and Dentofacial OrthopedicsMay 2007
578.e2 Frazier-Bowers et al

study was reviewed and approved by the UNC Biomed-ical Institutional Review Board. Consent was obtained foreach subject who participated and by the parents of theminors. When possible (4 of the 9 families that wereidentified), family members were interviewed (1 group atUNC, the other 3 families by telephone), and dentalrecords obtained (in the UNC clinic or by the referringorthodontist). Participants were categorized as affected orunaffected. Based on these diagnoses, pedigrees wereconstructed and analyzed in a preliminary effort to deter-mine the pattern of inheritance.
RESULTS
The number of subjects in each category issummarized� in� Figure� 1.� In� 32� of� the� 97� subjects,� adefinitive diagnosis could not be made withoutadditional longitudinal data (representative subject
shown� in� Fig� 2),� and� 19� subjects� showed� MFE(representative� subject� shown� in� Fig� 3).� Eight� sub-jects did not fit the description of PFE or MFE(example� shown� in� Fig� 4).
The distribution of affected teeth in the PFE groupis� shown� in� Figure� 5.� A� few� subjects� had� affectedteeth forward as far as the first premolars, but thefrequency of affected teeth increased toward thesecond premolars and the first and second molars. Inmost cases, the subjects were too young to havemuch development of the third molars, and only thirdmolars that were obviously affected were counted inthe distribution.
The PFE group had 3 distinguishable forms. Onegroup (17 of 38), designated type I, had a similar lackof eruption potential of all affected teeth with a pro-gressive� open� bite� from� anterior� to� posterior� (Fig� 6).� A
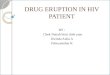
Fig 2. Representative example of IFE: 8-year-old with ankylosis of deciduous molars in the upperright quadrant. This might be PFE, but at this point, second molars bilaterally are developed to thesame extent and in the same position. Eruption progress should be monitored.
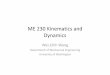
Fig 3. Subject exhibits ankylosis of upper right first molar. Adjacent teeth have erupted and driftedinto the space.
American Journal of Orthodontics and Dentofacial OrthopedicsVolume 131, Number 5
Frazier-Bowers et al 578.e3

second group (11 of 38), designated type II, had a toothdistal to the most mesial affected tooth with greateralthough inadequate eruption; therefore, the eruptionpotential� varied� among� the� affected� teeth� (Fig� 7).� Ten
patients had both 2 types coexisting in different quad-rants. There appeared to be no difference in the sub-types of PFE between those with and without a familyhistory of eruption problems.
Fig 4. Subject with mild lateral open bite on right side and moderate lateral open bite on left, shownin A, panoramic, B, clinical photos, and C, cephalometric radiograph. There is no indication of failederuption mechanism.
American Journal of Orthodontics and Dentofacial OrthopedicsMay 2007
578.e4 Frazier-Bowers et al

At least 1 ankylosed deciduous tooth was noted in24 of the 97 subjects (PFE ! 8, IFE ! 12, MFE ! 2,other ! 2). Four subjects had hypodontia (IFE ! 3,MFE ! 1), 5 subjects had hyperdontia (PFE ! 2,IFE ! 2, MFE ! 1), and 3 subjects had taurodontism(all 3 in IFE). No other dental anomalies were noted.
For the 29 subjects for whom cephalometric radio-graphs were submitted, skeletal classifications werenoted. Of these, 26% were Class III, and one-third(35%) of those with PFE were Class III.
Twenty-six percent of the PFE subjects in thissample appeared to be familial (10 of 38). There was noobvious difference in the types of PFE expressed byfamily� members� vs� the� isolated� cases.� Figure� 8� showsPFE in a mother and a daughter. Five other subjects inthe sample reported familial eruption problems. Twosubjects who were brothers were classified as IFEbecause they were too young for diagnosis, and theother 3 (classified as either IFE or MFE) were related toPFE subjects. Other than a high prevalence of anky-losed deciduous molars (5 of 15, or 33%), no otherdental anomalies were found in the familial group.
Of the 9 families with a reported familial history oferuption problems, 4 pedigrees were constructed. Onepedigree� is� shown� in� Figure� 9.� Pedigree� analysis� byinspection strongly suggests an autosomal dominant in-heritance pattern. Both sexes were affected without pref-erence; about half the members in the kindred wereaffected, and the trait did not skip generations. Thepossibility of an X-linked autosomal dominant inheritancepattern cannot be excluded; however, this mode of inher-itance is extremely rare and therefore less likely.
DISCUSSION
New findings from this study indicate 2 distinguish-able types of PFE that seem to be related to the timing
of onset. In type I, the classic form described initially,loss of eruption potential appears to strike at a certainchronologic time, leading to a similar lack of eruptionpotential of all affected teeth. In type II, the timing ofonset might be related to the stage of root development,leading to a varied eruption potential among affectedteeth. In a significant number of subjects, a combinationof the 2 types was found, and a few subjects showedPFE in 1 quadrant coupled with a single ankylosedtooth in a different quadrant. Therefore, PFE andankylosis might be closely related, as the studies byRaghoebar� et� al10,11� seem� to� show.� Perhaps� an� abnor-mal PDL can lead to either condition.
In the small subset for whom lateral cephalogramswere available, a high percentage of the subjects,especially those with PFE, had skeletal Class III rela-tionships. This was not reported previously. In ourstudy population, the possibility that lateral cephalo-grams were sent only when a skeletal discrepancy waspresent cannot be ruled out; therefore, the high percent-age of Class III subjects might be a biased representa-tion. Of the other articles on PFE, only a few accountfor the skeletal relationships of some of their subjects.Proffit� and� Vig3� reported� a� subject� with� a� Class� IIIrelationship,� Ireland6� had� 2� Class� I� subjects,� and� Brady5
reported 1 of 2 with a Class II pattern. Dibiase andLeggat8� reported� that� both� of� their� subjects� were� ClassII. Because failure of permanent molars to erupt is sorare, finding a sample size large enough to study thecharacteristics� is� difficult.12-15
Reports of a definite familial tendency associatedwith PFE indicate that the cause of the developmentaldisturbance in the PDL might be inheritable. In thisstudy, 26% of the PFE cases were familial. Raghoebaret� al7� reported� a� heritable� component� to� eruption� failurein 10% of his cases, whereas other case reports pro-vided� studies� of� a� few� single� families.5-9,16
Pedigree analysis of the familial cases in this studywas highly suggestive of an autosomal dominant inher-itance pattern with complete penetrance and variableexpressivity. Most of the familial studies in the litera-ture also report an autosomal dominant inheritancepattern4,5,16;� however,� Winter� et� al16� reported� a� familyas autosomal recessive.
Although� no� patients� examined� by� Proffit� and� Vig3
in the original study had similarly affected relatives,they supposed that a genetic disturbance of varyingpenetrance and expressivity was the likely etiology.The current reports of affected families support thishypothesis4-8� and� suggest� that� spontaneous� mutationsmight account for the subjects with no previous familyhistory. One can speculate that this genetic distur-bance leads to a local disruption in metabolic activity
Fig 5. Distribution of affected teeth in PFE group.Overall distribution among 4 quadrants and betweenmaxillary and mandibular teeth was fairly equal, al-though individual subjects were rarely symmetric.
American Journal of Orthodontics and Dentofacial OrthopedicsVolume 131, Number 5
Frazier-Bowers et al 578.e5

or altered blood flow, which then hinders the erup-tion� mechanism.� Raghoebar� et� al,10� based� on� histo-logic examination of 26 molars from 20 patients,suggested that the mechanism is replacement ofcementoblasts by osteoblasts due to a local distur-bance in the PDL during the repair process of localphysiologic resorption.
The best evidence of failure in the eruption mech-anism is bone resorption that clears a path for theerupting tooth, without tooth movement. Affected teeththat were surgically exposed are generally reported tobe easily movable in the crypt and not ankylosed.Although these teeth might have some slight re-sponse to orthodontic forces, the response is abnor-mal, and the teeth invariably become ankylosedbefore reaching occlusion. Case studies illustrate thatnot only do affected teeth fail to respond to treat-ment, but also adjacent normal teeth are adverselyaffected by intrusion to the level of the affected teeth(Fig� 10).� Raghoebar� et� al10� and� Winter� et� al16� alsoconcluded that ankylosis in the failed eruptive pro-cess can be a secondary rather than the initiatingprocess and reiterated that orthodontic proceduresdesigned to improve eruption are doomed to failurein patients with PFE.
In the diagnosis of eruption failures, the first step isto rule out local, systemic, and endocrine factors.Endocrine abnormalities (at least to this point) have notbeen identified in PFE or ankylosis patients. Ultimately,the principal differential diagnosis is mechanical ob-struction (ankylosis) vs failure of the eruption mecha-nism. Distinguishing between the 2 is key to determin-ing the prognosis for the affected teeth. Unfortunately,MFE and PFE can have similar presentations in theearly stages. If so, a definitive diagnosis cannot bemade without sufficient longitudinal data and therapeu-tic diagnosis (an attempt at orthodontically erupting thetooth or teeth that might or might not be affected).
The first encounter with these patients often occursaround age 8 or 9 when asymmetry in the eruptionpattern of the permanent first molars is noticed. Theconservative approach is to take a panoramic radio-graph with the patient’s teeth together and recall him orher in 6 to 12 months to determine eruption progress.Evaluation at recall will show progress, no change, orrelative submergence. If there is eruption progress, PFEand ankylosis can be ruled out. Ultimately assessing theeruption capacity of the neighboring teeth is the onlyway to distinguish PFE from ankylosis. The number ofteeth affected and a positive family history can provide
Fig 6. Classic example of PFE type I in all 4 quadrants, showing cleared eruption path inA, panoramic film and B, clinical photos.
American Journal of Orthodontics and Dentofacial OrthopedicsMay 2007
578.e6 Frazier-Bowers et al

Fig 7. Subject with characteristics of PFE type II in A, panoramic radiograph and B, clinical photos,with C, Class III skeletal relationship. Affected teeth were easily surgically luxated and notankylosed. Treatment with vertical elastics was not successful.
American Journal of Orthodontics and Dentofacial OrthopedicsVolume 131, Number 5
Frazier-Bowers et al 578.e7

valuable clues. Differentiation between the 2 types ofPFE cannot be made until at least age 14 or 15 when thesecond molar either completely fails to erupt or eruptspartially and then stops.
Once PFE has been diagnosed, treatment optionsare disappointing and limited. Patients and orthodon-tists must often either accept the premolar occlusion oropt for more invasive techniques, which unfortunatelyare unlikely to succeed. In the mildest cases, teeth canbe� restored� with� onlays� and� crowns,17� but� definitiverestorations should not be placed before completion ofvertical growth. For moderately severe cases, extractionof teeth with placement of implants might be an option,but bone grafts before implants are likely to be re-quired. Another option could be a small segmental os-
teotomy to surgically reposition the teeth into occlusion,but there are few if any documented successes with thisapproach. In severe cases, a significant deficit in alveolarbone height precludes implant restorations and subapicalosteotomy. One report of distraction osteogenesis to cor-rect an extreme posterior open bite provides an interestingpotential� treatment� alternative.18� Often� the� only� feasibleoption� is� a� removable� prosthesis.19
CONCLUSIONSPFE is a rare condition that can lead to spectacular
posterior open bites. It is difficult to diagnose at youngages, and even more difficult to treat due to the lack ofresponse to orthodontic forces, but proper diagnosis cansave the patient and the orthodontist years of frustration
Fig 8. PFE in A and B, mother and C-E, daughter. Mother was affected in all 4 quadrants and wastreated with multiple extractions. Daughter had ankylosed deciduous teeth and was bilaterallyaffected, although more severe on right side.
American Journal of Orthodontics and Dentofacial OrthopedicsMay 2007
578.e8 Frazier-Bowers et al

Fig 8. (Cont’d)
American Journal of Orthodontics and Dentofacial OrthopedicsVolume 131, Number 5
Frazier-Bowers et al 578.e9

and disappointment. The observation that PFE canoccur in families suggests that the developmental dis-turbance leading to PFE is heritable. Future studies todetermine the genetic etiology of PFE are neededbecause this can aid in differential diagnosis, allowearly identification of affected family members, andeventually lead to new treatment modalities.
An overview of types of posterior eruption problems,summarizing� our� current� concepts,� is� given� in� Table� II.
This study would not have been possible withoutthe many concerned orthodontists who sent cases 1 or2 at a time for evaluation. We thank Thomas Ahman,Loring Ross, Fidel Del Toro, and Peter Shapiro for
II:1 II:2
III:1 III:2 III:3 III:4 III:5
I:2
II:3 II:4 II:5II:1 II:2
III:1 III:2 III:3 III:4 III:5
I:2I:1
II:3 II:4 II:5
Fig 9. Pedigree of PFE subject. Analysis by inspection shows autosomal dominance with completepenetrance.
Fig 10. Attempt at orthodontic treatment led to intrusion of normal teeth mesial to affected teeth.
American Journal of Orthodontics and Dentofacial OrthopedicsMay 2007
578.e10 Frazier-Bowers et al

submitting many cases and their continued support ofthis research, and Christopher Planer and MelodyTorain for their assistance with data collection andpreparation of this manuscript.
REFERENCES
1. Cahill DR. Eruption pathway formation in the presence ofexperimental tooth impaction in puppies. Anat Rec 1969;164:67-77.
2. Proffit WR. Contemporary orthodontics. 3rd ed. St Louis:Mosby; 2000.
3. Proffit WR, Vig KW. Primary failure of eruption: a possiblecause of posterior open-bite. Am J Orthod 1981;80:173-90.
4. Bosker H, Ten Kate LP, Nijenhuis LE. Familial reinclusion ofpermanent molars. Clin Genet 1978;13:314-20.
5. Brady J. Familial primary failure of eruption of permanent teeth.Br J Orthod 1990;17:109-13.
6. Ireland AJ. Familial posterior open bite: a primary failure oferuption. Br J Orthod 1991;18:233-7.
7. Raghoebar GM, Ten Kate LP, Hazenberg CA, Boering G,Vissink A. Secondary retention of permanent molars: a report offive families. J Dent 1992;20:277-82.
8. Dibiase AT, Leggat TG. Primary failure of eruption in thepermanent dentition of siblings. Int J Paediatr Dent 2000;10:153-7.
9. Demirjian A, Goldstein H, Tanner JM. A new system of dentalage assessment. Hum Biol 1973;45:211-27.
10. Raghoebar GM, Boering G, Jansen HW, Vissink A. Secondaryretention of permanent molars: a histologic study. J Oral PatholMed 1989;18:427-31.
11. Raghoebar GM, Boering G, Vissink A, Stegenga B. Eruptiondisturbances of permanent molars: a review. J Oral Pathol Med1991;20:159-66.
12. O’Connell AC, Torske KR. Primary failure of tooth eruption: aunique case. Oral Surg Oral Med Oral Pathol Oral Radiol Endod1999;87:714-20.
13. Grover PS, Lorton L. The incidence of unerupted permanentteeth and related clinical cases. Oral Surg Oral Med Oral Pathol1985;59:420-5.
14. Johnsen DC. Prevalence of delayed emergence of permanentteeth as a result of local factors. J Am Dent Assoc 1977;94:100-6.
15. Nagpal A, Sharma G, Sarkar A, Pai KM. Eruption disturbances:an aetiological-cum-management perspective. DentomaxillofacRadiol 2005;34:59-63.
16. Winter GB, Gelbier MJ, Goodman JR. Severe infra-occlusionand failed eruption of deciduous molars associated with eruptiveand developmental disturbances in the permanent dentition: areport of 28 selected cases. Br J Orthod 1997;24:149-57.
17. Yatani H, Watanabe EK, Kaneshima T, Yamashita A, Suzuki K.Etched-porcelain resin-bonded onlay technique for posteriorteeth. J Esthet Dent 1998;10:325-32.
18. Kater WM, Kawa D, Schafer D, Toll D. Treatment of posterior openbite using distraction osteogenesis. J Clin Orthod 2004;38:501-4.
19. Siegel SC, O’Connell A. Oral rehabilitation of a child withprimary failure of tooth eruption. J Prosthodont 1999;8:201-7.
Table II. Overview of types of posterior eruption problems
ClassificationNumber of
affected teeth
Impact onneighboring
teeth
Clinicalappearanceof ankylosis
Affected teeth visibleintraorally
Typical treatmentresponse
Proposed cause offailure
MFE Usually only firstmolars
Adjacent teethnormal
Yes Maybe Other teeth respond,affected teethmight respond toluxation
Ankylosis, possible otherobstruction
PFE Unilateral orbilateral, caninvolve wholequadrants
Distal teethalso affected
No Usually some portionof at least 1 tooth
No response toorthodontic force
Failure of eruptionmechanism
IFE Too early todetermine
Unknown atthis stage
No Maybe Depends on finaldiagnosis
Ankylosis or PFE
Other Any Unknown No Yes Might respond buttends to relapse
Possible tongue orsoft-tissue interference
American Journal of Orthodontics and Dentofacial OrthopedicsVolume 131, Number 5
Frazier-Bowers et al 578.e11