Embed Size (px)
Citation preview
Primary Care Atrial Fibrillation Update:Anticoagulation and Left Atrial Appendage OcclusionGreg Francisco, MD, FACC
DISCLOSURES
• None to declare
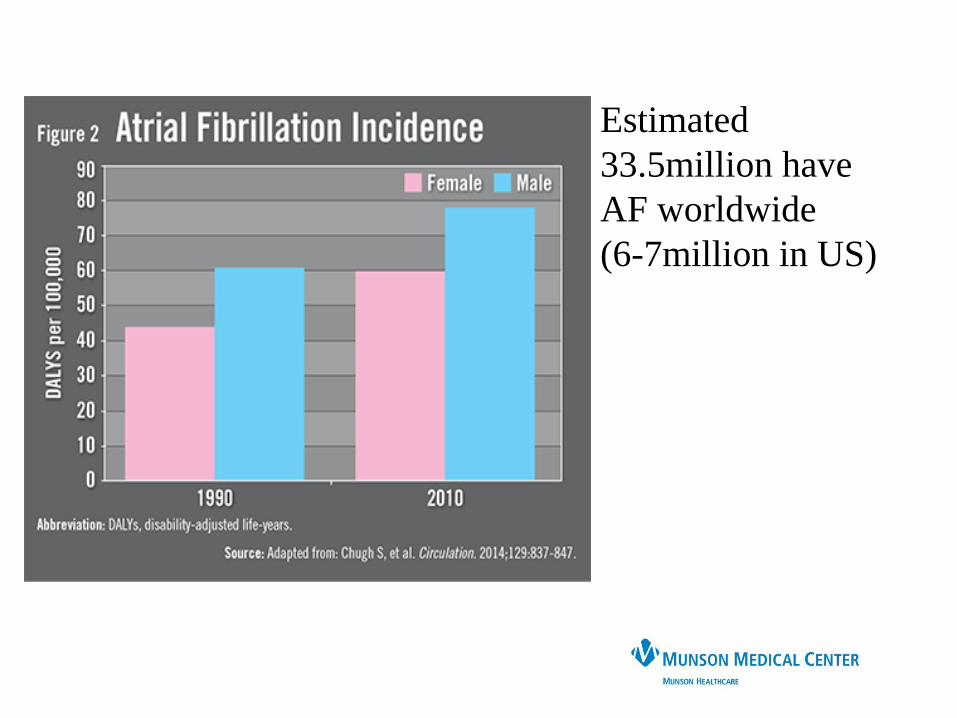
Estimated
33.5million have
AF worldwide
(6-7million in US)
Atrial Fibrillation
- Most common arrhythmia (incidence 1% of
all US adults)
- 2% of Medicare beneficiaries <65 have AF
- 12% in 75-85year olds
- 5X increased risk of stroke
- 3X increased risk of Heart Failure
- 2X increased dementia
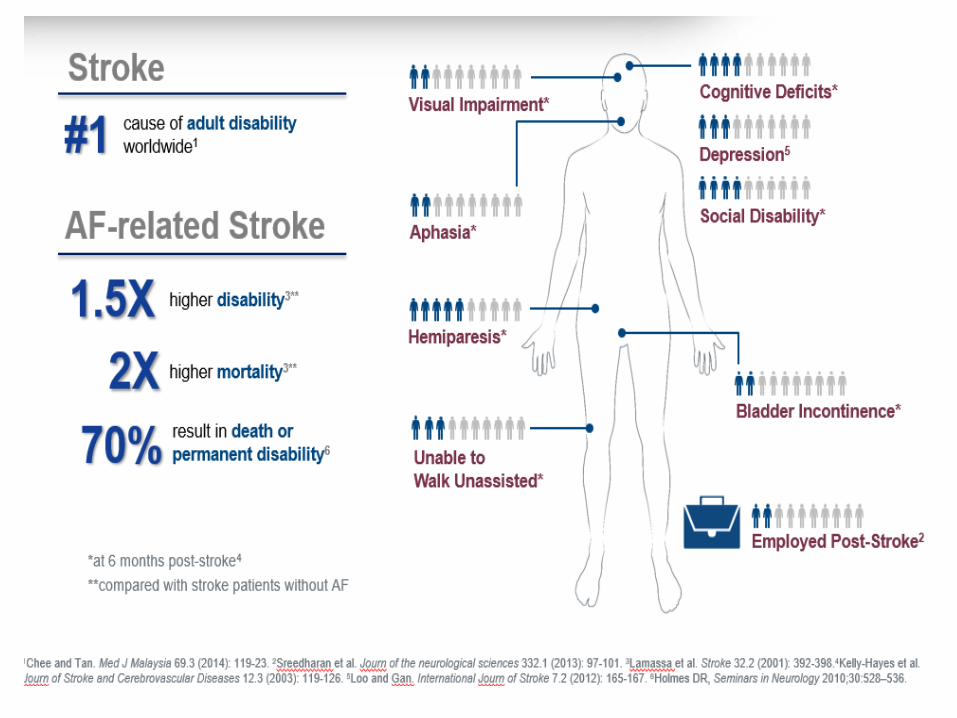
- 1/3 of all ischemic strokes are due to AF
- Embolic strokes are devastating – up to 50%
mortality, and of survivors, up to 50% disability
- Highest risk in those with prior stroke and >75
years old
Atrial Fibrillation
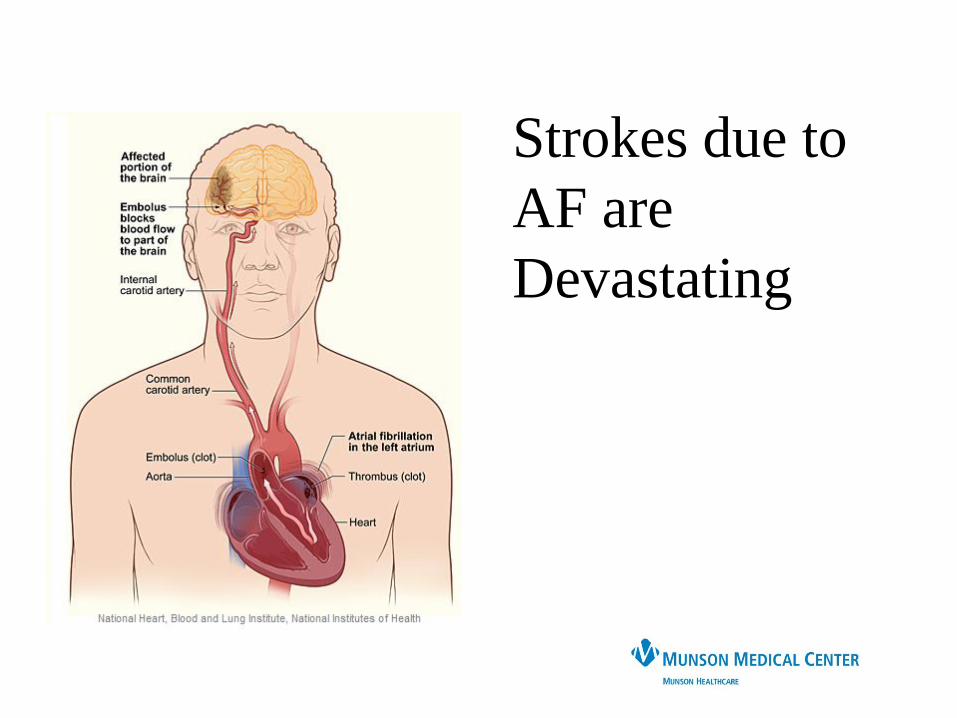
Strokes due to
AF are
Devastating
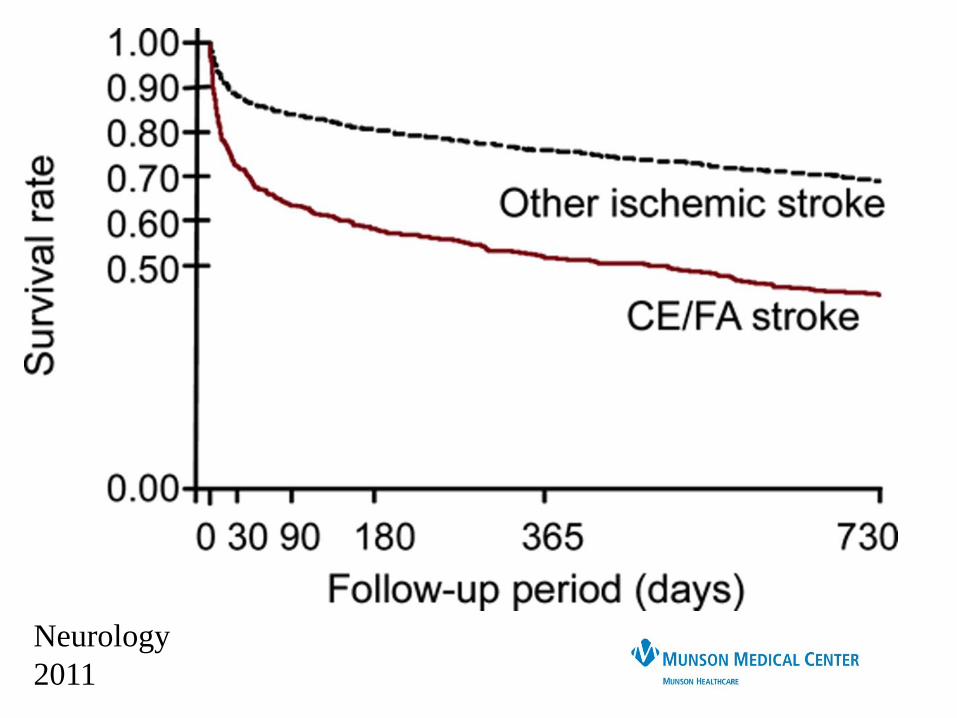
Neurology
2011
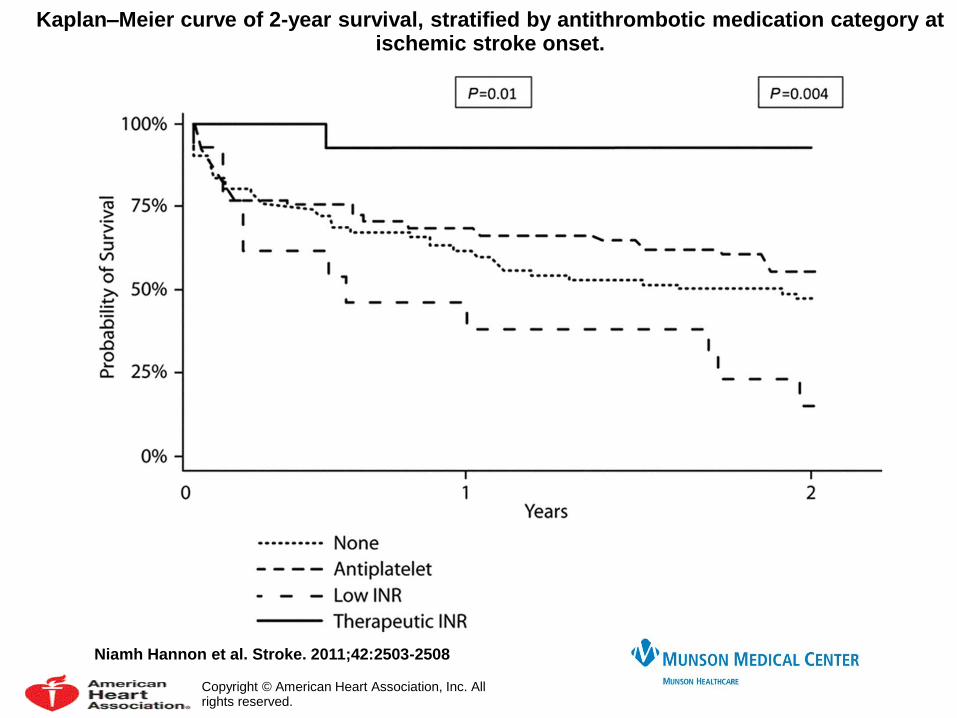
Kaplan–Meier curve of 2-year survival, stratified by antithrombotic medication category at ischemic stroke onset.
Niamh Hannon et al. Stroke. 2011;42:2503-2508
Copyright © American Heart Association, Inc. All rights reserved.

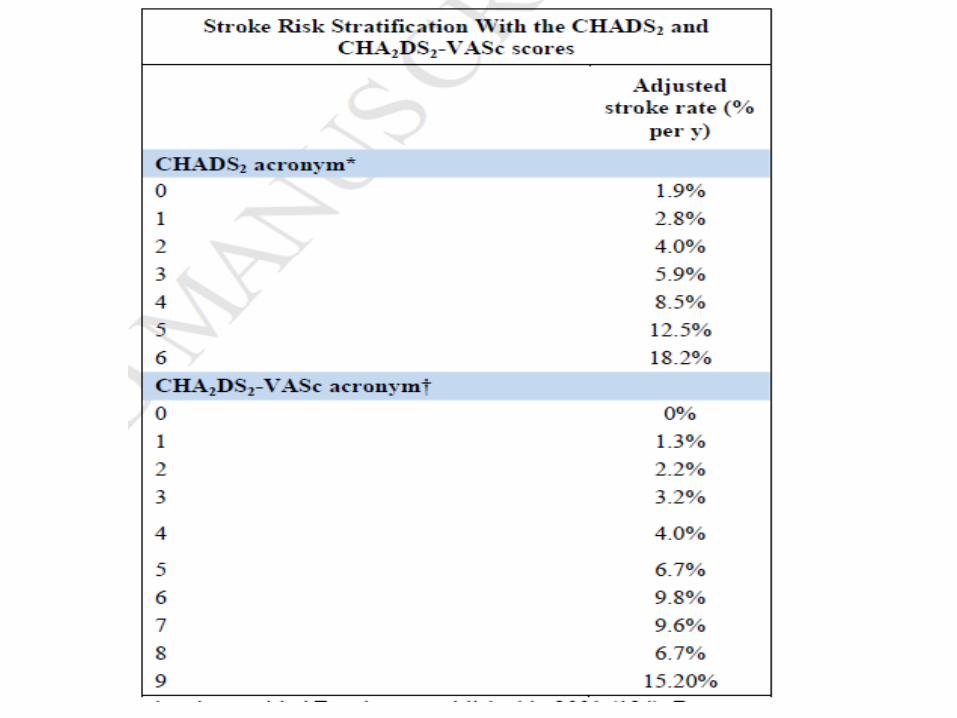
CHADS2 -> CHA2DS2VASc
CHA2DS2-VASc Risk Score
CHF or LVEF < 40% 1
Hypertension 1
Age > 75 2
Diabetes 1
Stroke/TIA/
Thromboembolism
2
Vascular Disease 1
Age 65 - 74 1
Female 1
CHADS2 Risk Score
CHF 1
Hypertension 1
Age > 75 1
Diabetes 1
Stroke or TIA 2
From ESC AF Guidelines
http://www.escardio.org/guidelines-surveys/esc-
guidelines/GuidelinesDocuments/guidelines-afib-FT.pdf
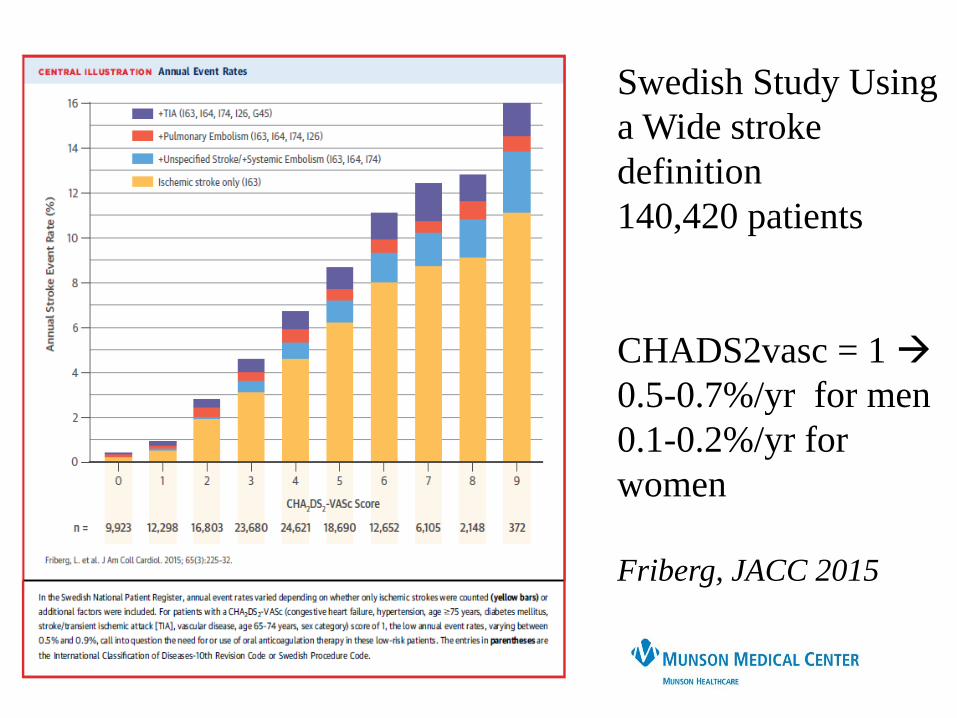
Swedish Study Using
a Wide stroke
definition
140,420 patients
CHADS2vasc = 1
0.5-0.7%/yr for men
0.1-0.2%/yr for
women
Friberg, JACC 2015
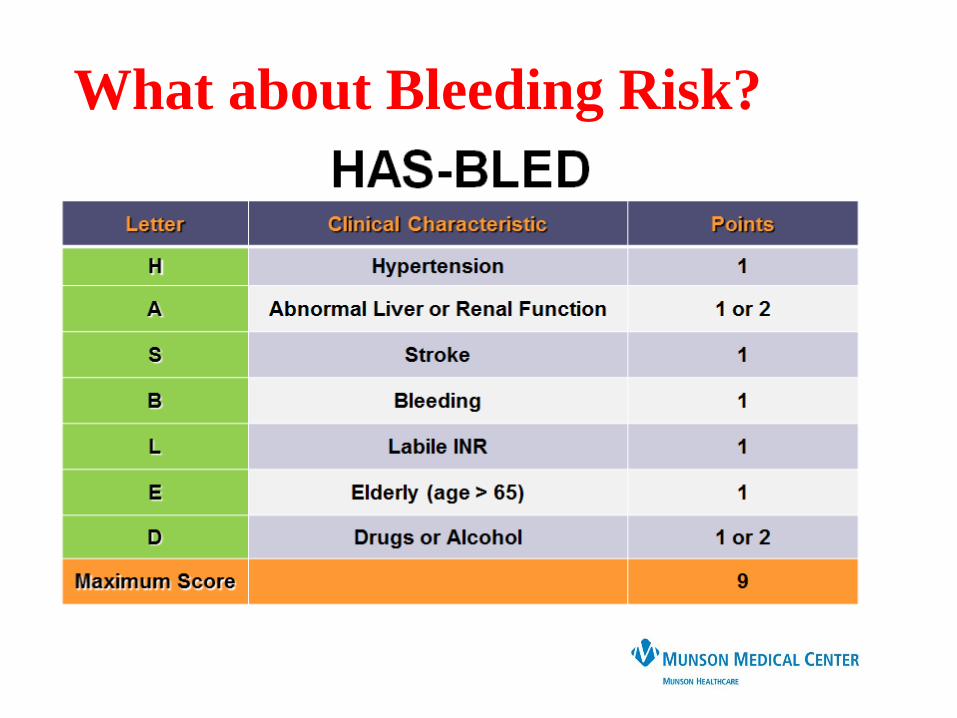
What about Bleeding Risk?

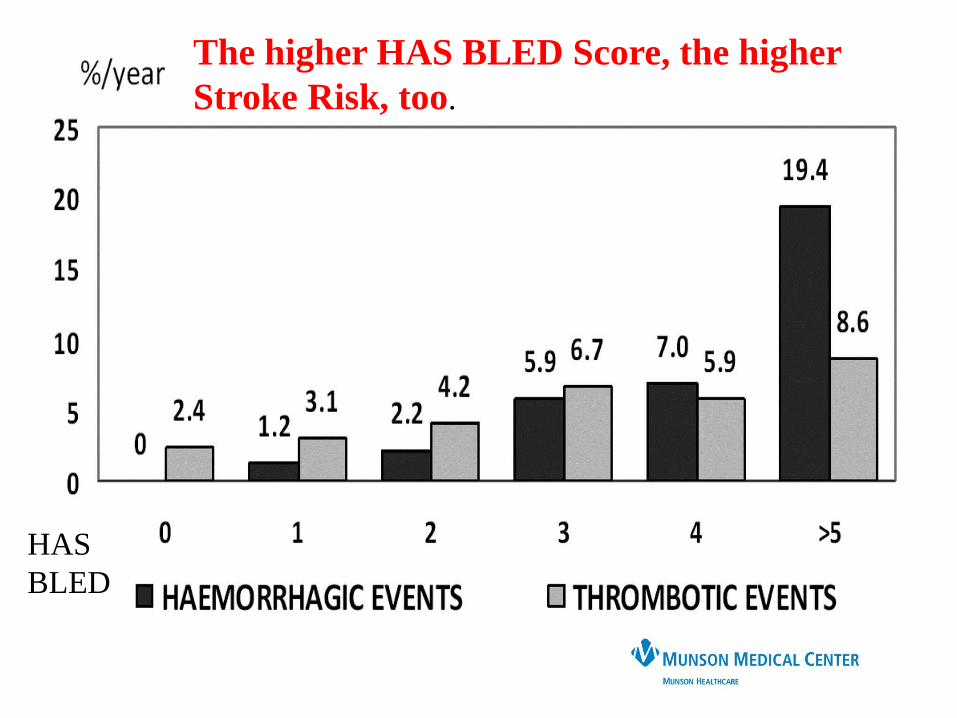
HAS
BLED
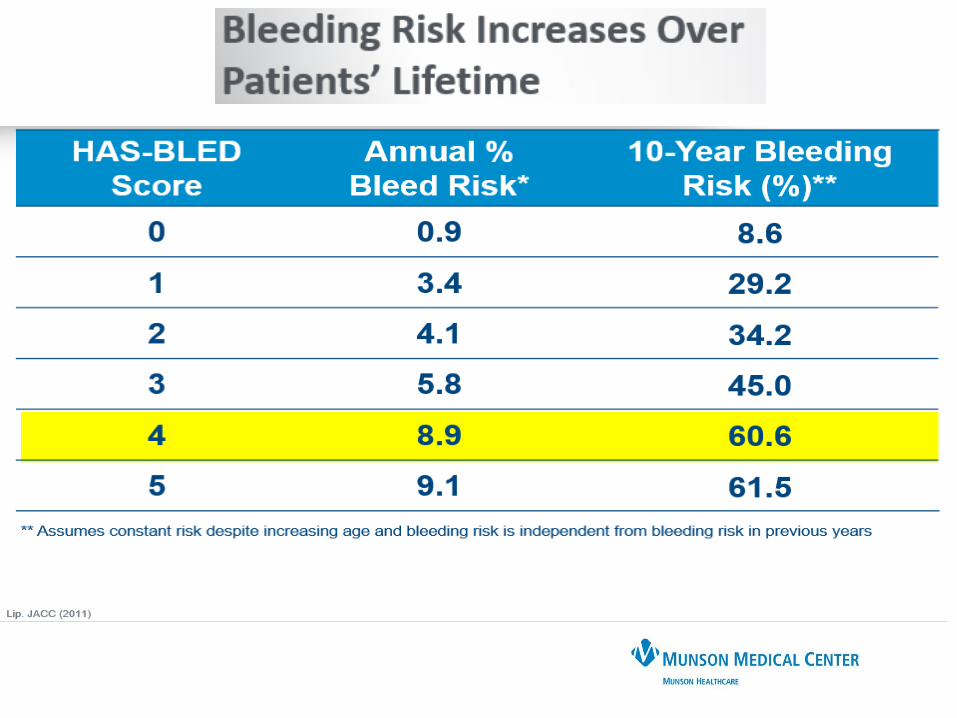
The higher HAS BLED Score, the higher
Stroke Risk, too.
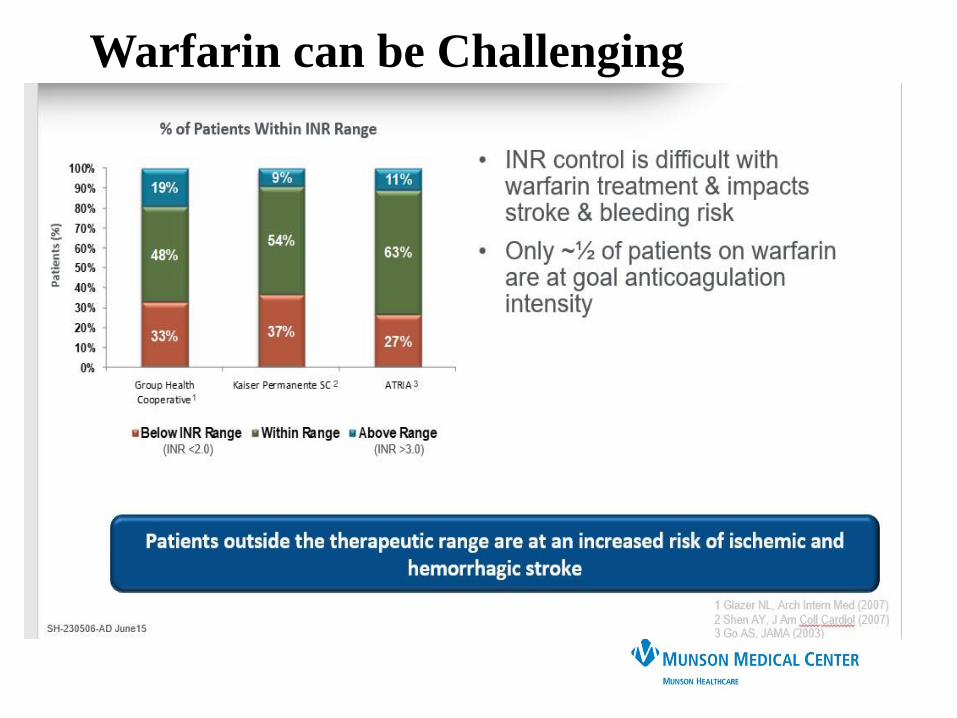
Warfarin can be Challenging
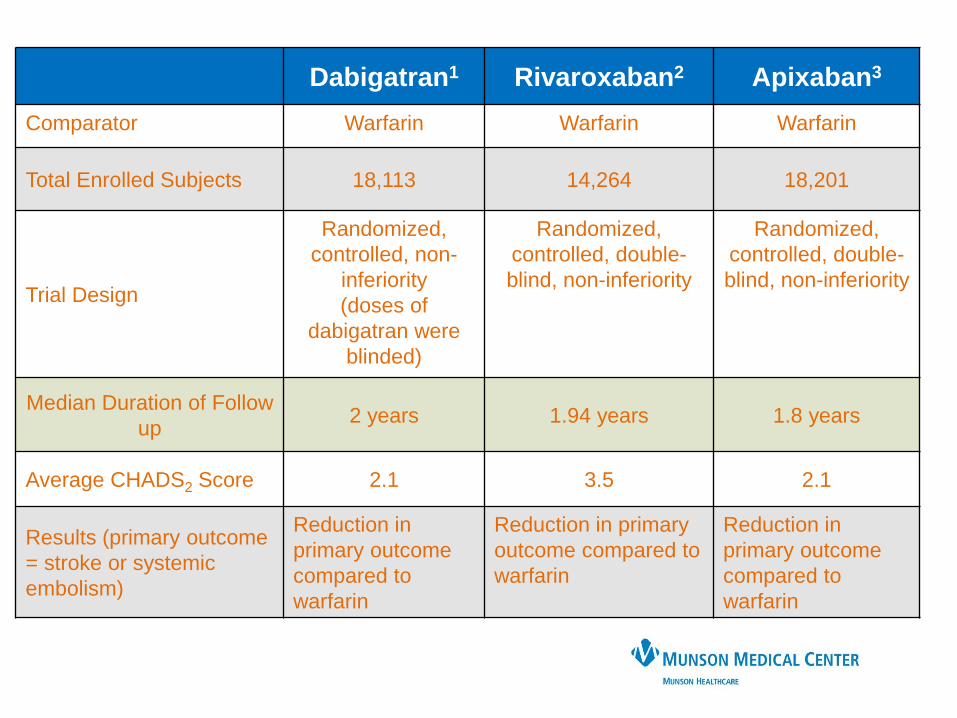
Dabigatran1 Rivaroxaban2 Apixaban3
Comparator Warfarin Warfarin Warfarin
Total Enrolled Subjects 18,113 14,264 18,201
Trial Design
Randomized,
controlled, non-
inferiority
(doses of
dabigatran were
blinded)
Randomized,
controlled, double-
blind, non-inferiority
Randomized,
controlled, double-
blind, non-inferiority
Median Duration of Follow
up2 years 1.94 years 1.8 years
Average CHADS2 Score 2.1 3.5 2.1
Results (primary outcome
= stroke or systemic
embolism)
Reduction in
primary outcome
compared to
warfarin
Reduction in primary
outcome compared to
warfarin
Reduction in
primary outcome
compared to
warfarin
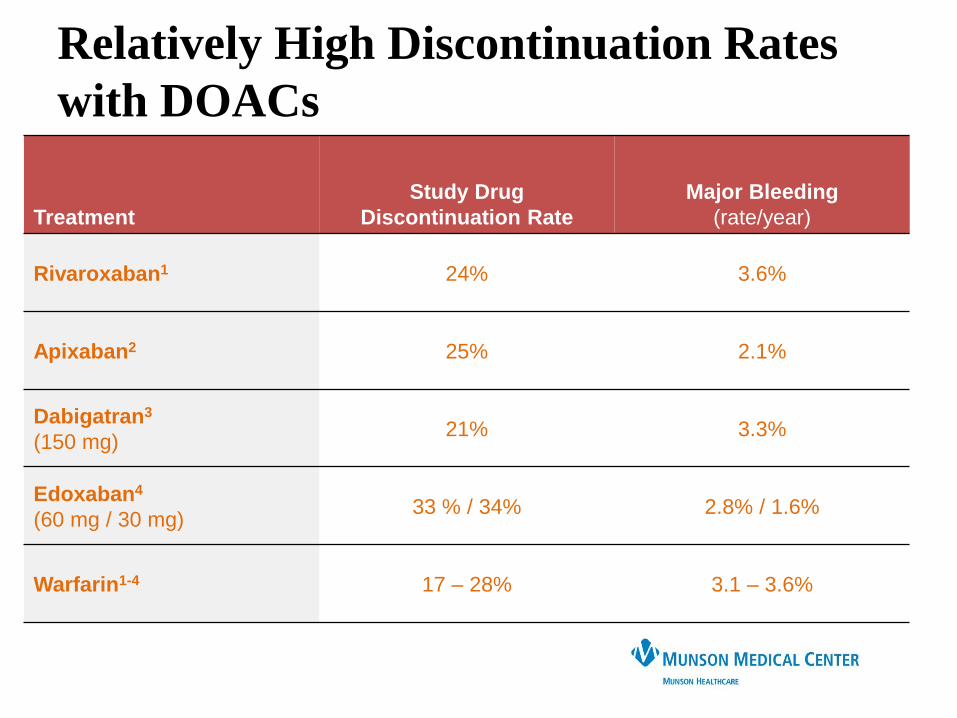
Treatment
Study Drug
Discontinuation Rate
Major Bleeding
(rate/year)
Rivaroxaban1 24% 3.6%
Apixaban2 25% 2.1%
Dabigatran3
(150 mg)21% 3.3%
Edoxaban4
(60 mg / 30 mg)33 % / 34% 2.8% / 1.6%
Warfarin1-4 17 – 28% 3.1 – 3.6%
Relatively High Discontinuation Rates
with DOACs

Left Atrial Appendage Occlusion:
Watchman Lariat
Atriclip

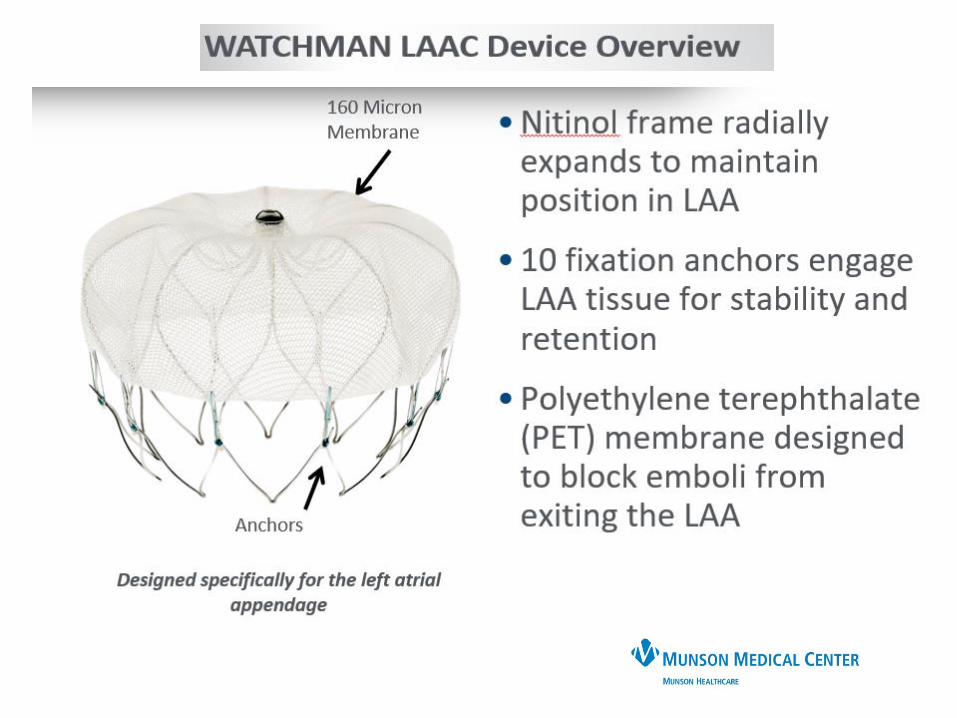
Watchman

FDA Approves Watchman March 2015For patients who are:
• At risk for stroke
• Deemed by be suitable for warfarin
• Have appropriate rationale to seek a nonpharmacological alternative
to warfarin
CMS Covers Watchman 8 February 2016For Patients with:
• CHADS2vasc >/= 3
• Formal shared decision with independent non-interventional
physician (internist, cardiologist, neurologist) – must be documented
in record
• Suitable for short term warfarin but deemed unable to take long term
OAC
• Experienced Interventional, EP, or CT surgery perfom
• Must be enrolled in prospective, national, audited registry
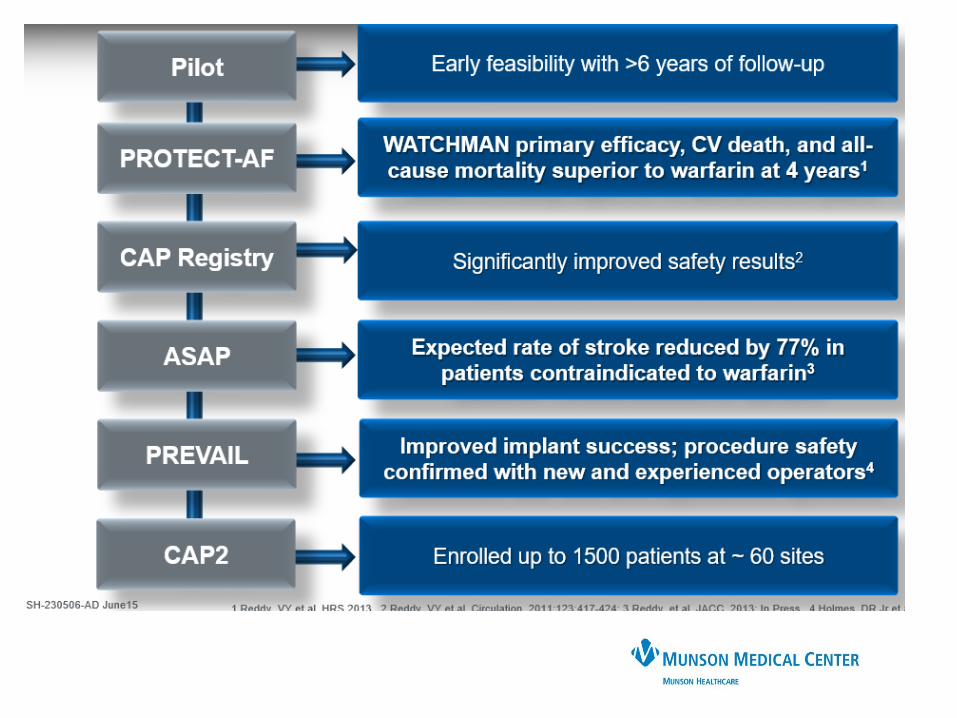

PROTECT
AF
CAP
Registry
PREVAIL CAP2
Registry Totals
Enrollment 2005-2008 2008-2010 2010-2012 2012-2014
Enrolled 800 566 461 579 2406
Randomized 707 --- 407 --- 1114
WATCHMAN:
warfarin (2:1)463 : 244 566 269 :138 579
1877:
382
Mean Follow-up
(years)4.0 3.7 2.2 0.58 N/A
Patient-years 2717 2022 860 332 5931
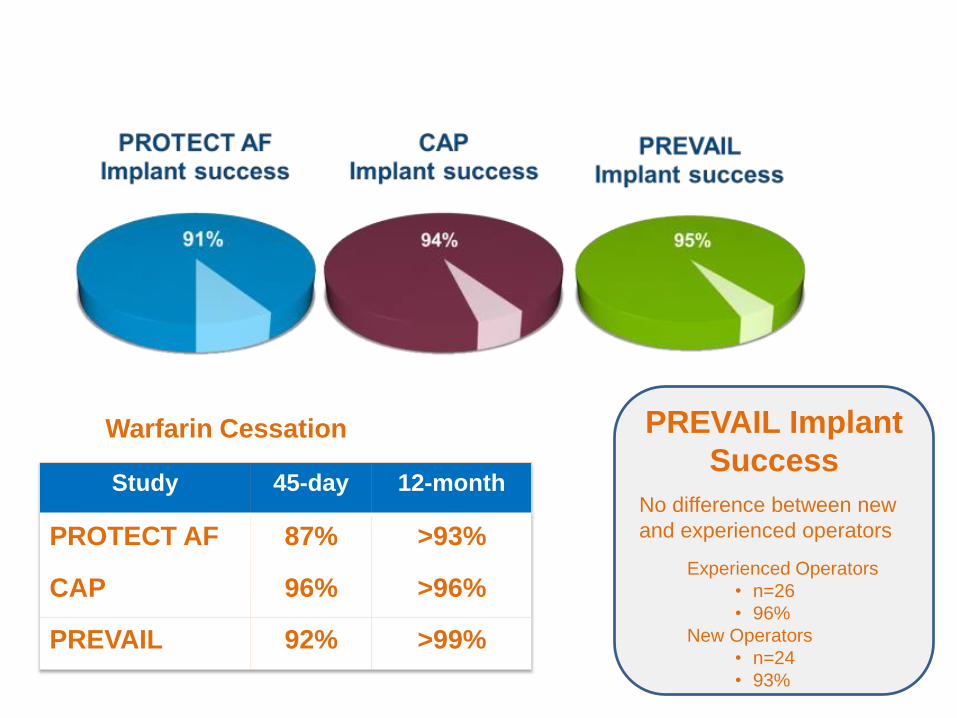
Warfarin Cessation
Study 45-day 12-month
PROTECT AF 87% >93%
CAP 96% >96%
PREVAIL 92% >99%
PREVAIL Implant
Success
No difference between new
and experienced operators
Experienced Operators
• n=26
• 96%
New Operators
• n=24
• 93%

Boersma et al. Heart Rhythm Journal 2017
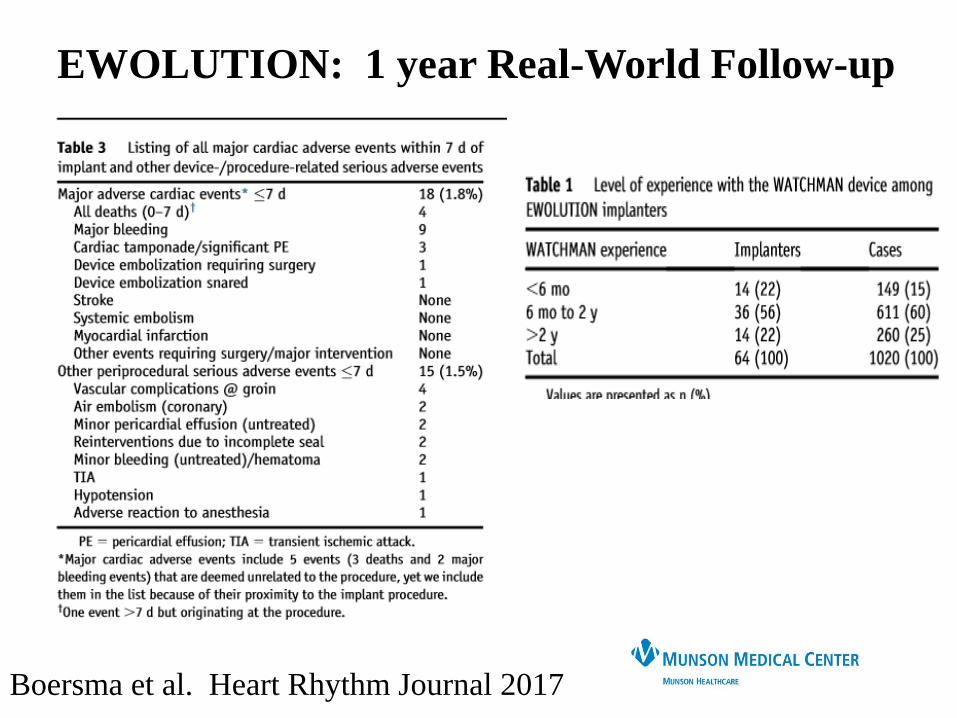
EWOLUTION: 1 year Real-World Follow-up
EWOLUTION: 1 year Real-World Follow-up
Boersma et al. Heart Rhythm Journal 2017
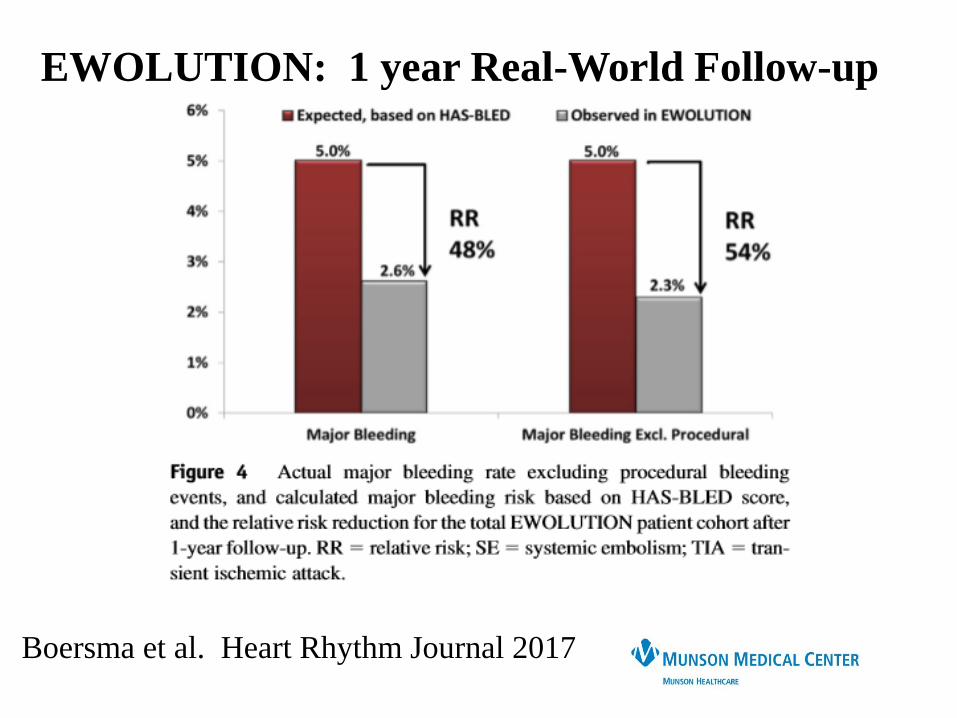
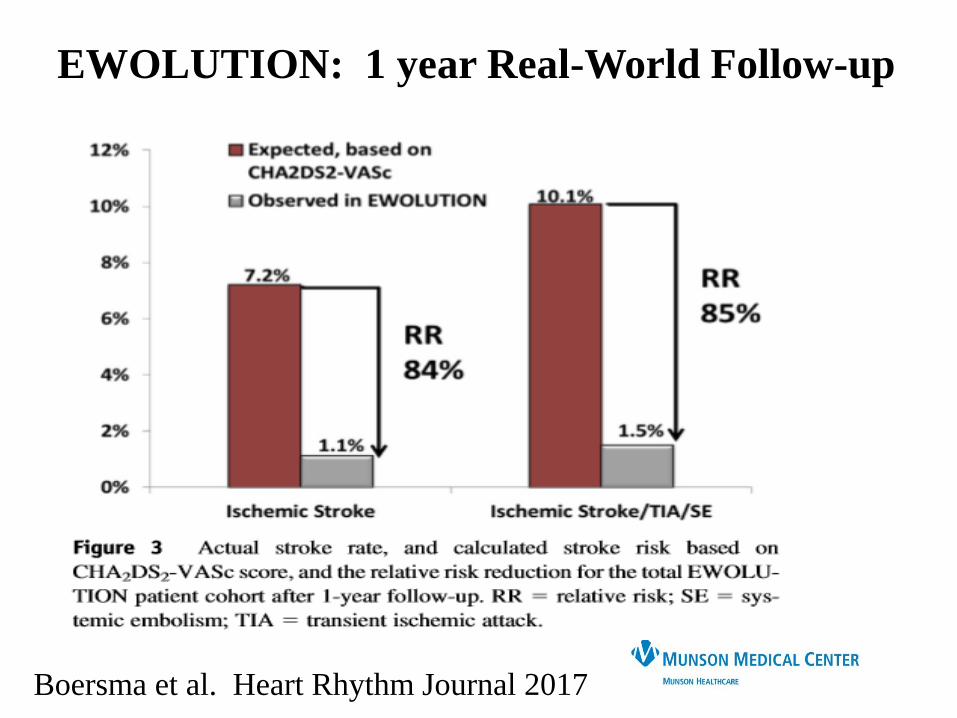
EWOLUTION: 1 year Real-World Follow-up
Boersma et al. Heart Rhythm Journal 2017
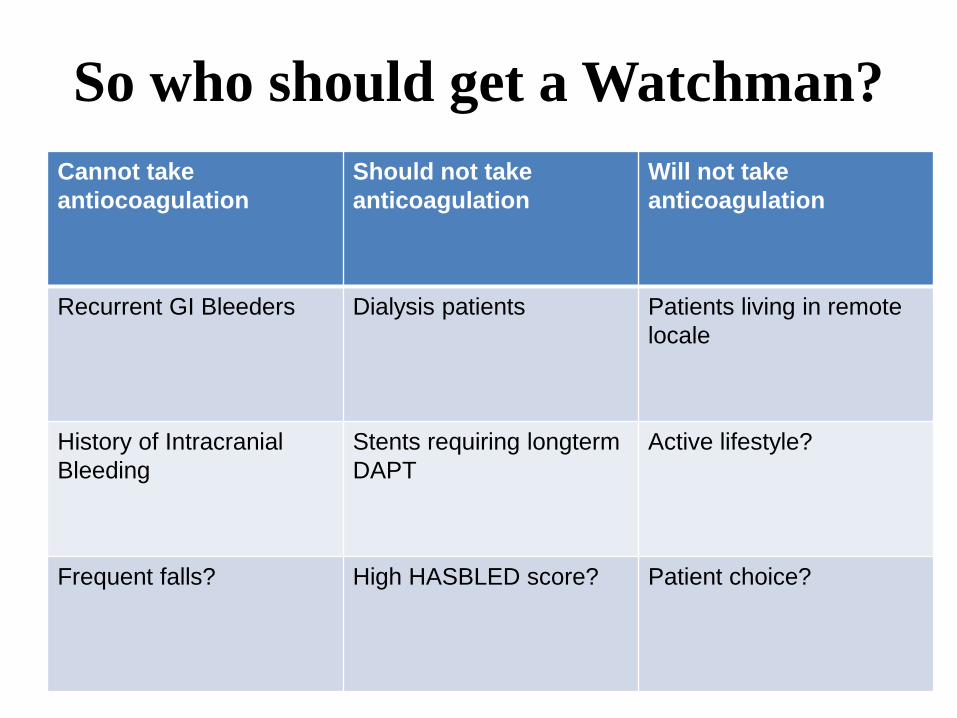
Cannot take
antiocoagulation
Should not take
anticoagulation
Will not take
anticoagulation
Recurrent GI Bleeders Dialysis patients Patients living in remote
locale
History of Intracranial
Bleeding
Stents requiring longterm
DAPT
Active lifestyle?
Frequent falls? High HASBLED score? Patient choice?
So who should get a Watchman?
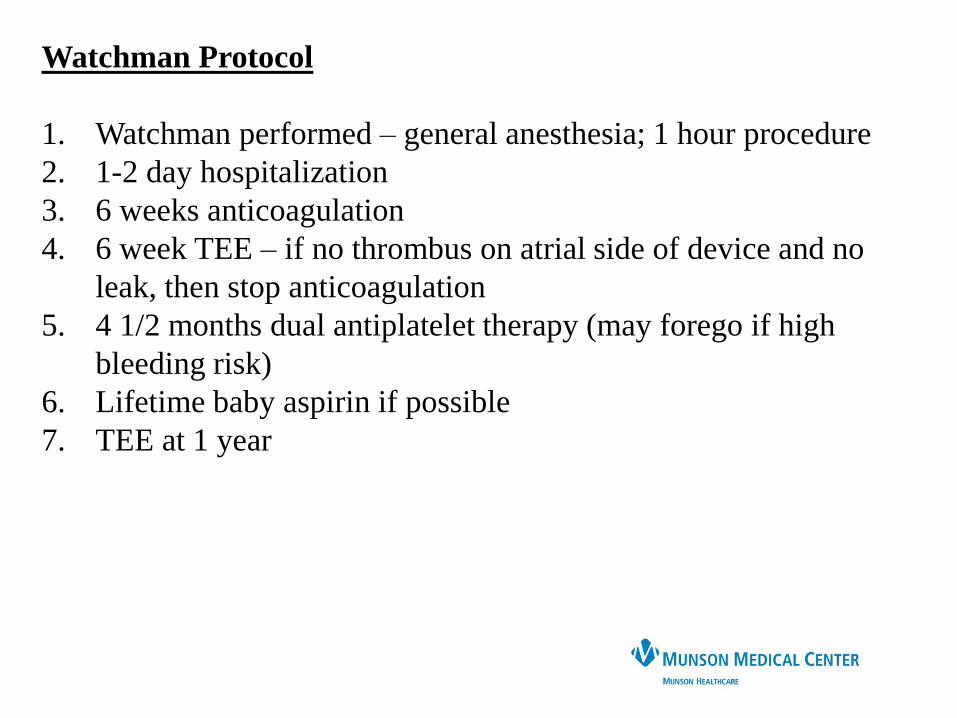
Watchman Protocol
1. Watchman performed – general anesthesia; 1 hour procedure
2. 1-2 day hospitalization
3. 6 weeks anticoagulation
4. 6 week TEE – if no thrombus on atrial side of device and no
leak, then stop anticoagulation
5. 4 1/2 months dual antiplatelet therapy (may forego if high
bleeding risk)
6. Lifetime baby aspirin if possible
7. TEE at 1 year
CASE STUDY:-EV is an 88 year old woman who suffered a
stroke and was found to have paroxysmal AF
-apixiban was started
-Subdural hematoma after a fall 6 months
later.
Apixiban stopped
-Neurosurgeon states that anticoagulation is
safe for the short-term, but not preferable for
longterm therapy
-Watchman was recommended
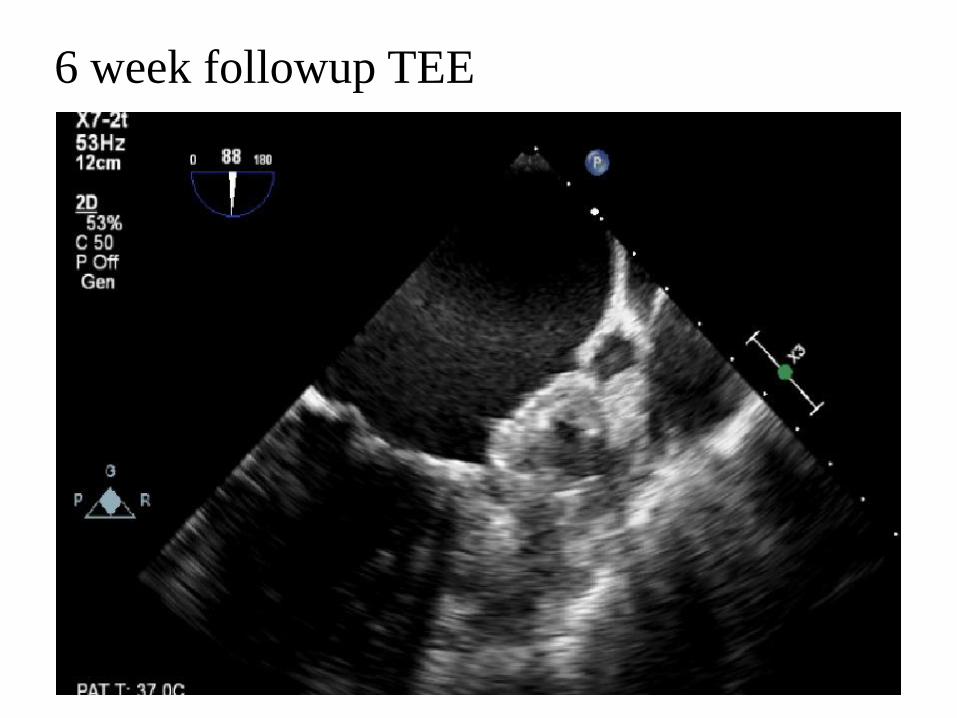
6 week followup TEE
Case 242 year old Active Duty Navy sailor presented
with 24 hours of palpitations. Atrial fibrillation
identified
CHADS2VASC = 0
He underwent chemical cardioversion with
flecainide.
No anticoagulation given
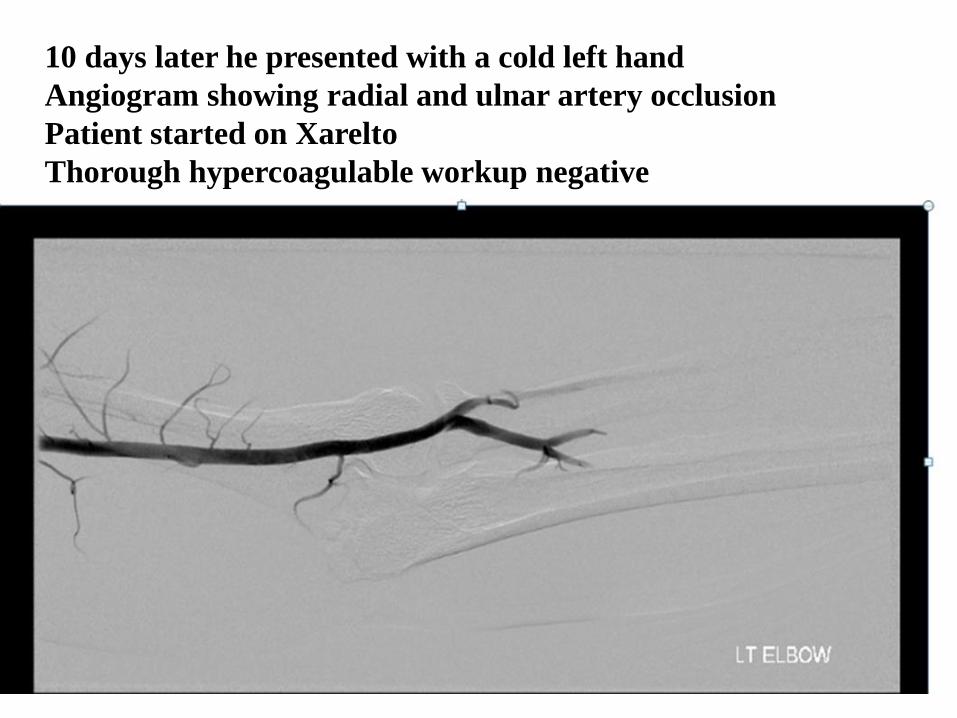
10 days later he presented with a cold left hand
Angiogram showing radial and ulnar artery occlusion
Patient started on Xarelto
Thorough hypercoagulable workup negative
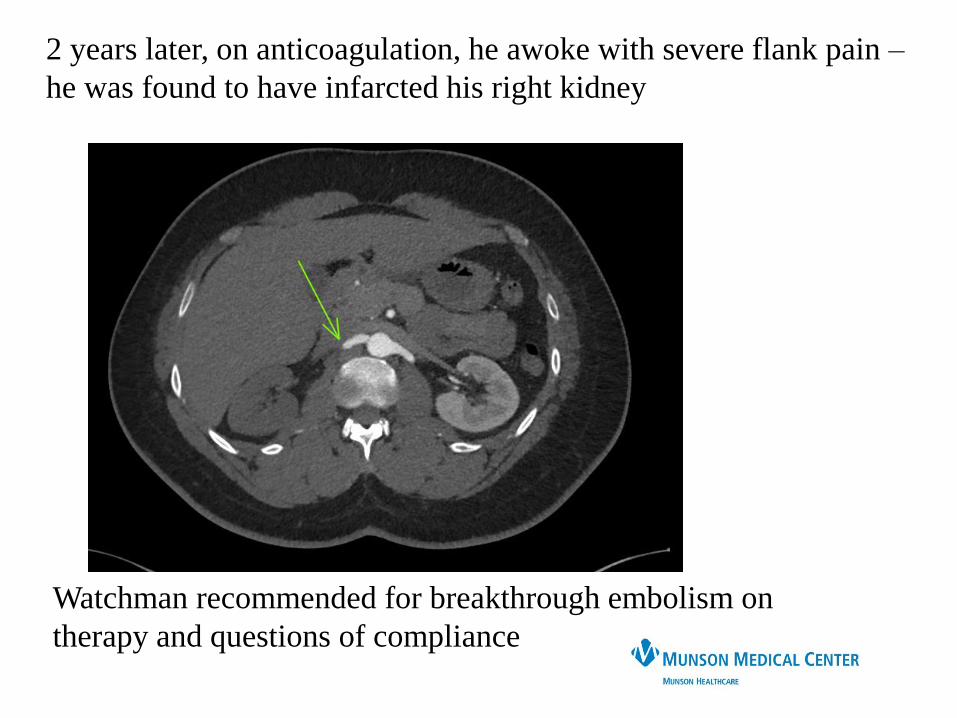
2 years later, on anticoagulation, he awoke with severe flank pain –
he was found to have infarcted his right kidney
Watchman recommended for breakthrough embolism on
therapy and questions of compliance
Thank you
QUESTIONS?