Embed Size (px)
Citation preview

New Approaches to Anticoagulation in
Atrial Fibrillation
Hugh Calkins M.D.
Nicholas J. Fortuin Professor of Cardiology Professor of Medicine
Director of Electrophysiology
Johns Hopkins Medical Institutions
1

Outline
Overview of Atrial Fibrillation
Treatment Strategies
Stroke Risk
Anticoagulation Options
Rate and Rhythm Control
Conclusion
2

Disclosures
Consultant, Research Support, or Honoraria
Biosense Webster, CryoCor, ProRhythm, Ablation
Frontiers,
Medtronic, Boston Scientific, AtriCure, Sanofi
Adventis
3

4
Epidemiology of AF
Most common sustained cardiac arrhythmia1
Currently affects 5.1 million Americans2
Prevalence expected to increase to 12.1 million by 2050
(15.9 million if increase in incidence continues)2
Preferentially affects men and the elderly1,2
Lifetime risk of developing AF: ~1 in 4 for adults 40
years of age3
1. Lloyd-Jones D, et al. [published online ahead of print December 17, 2009].
Circulation. doi:10.1161/CIRCULATIONAHA.109.192667.
2. Miyasaka Y, et al. Circulation. 2006;114(2):119-125. 3. Lloyd-Jones DM, et al. Circulation. 2004;110(9):1042-1046.

5
AF Is Associated With
Increased Thromboembolic Risk
Major cause of stroke in elderly1
5-fold in risk of stroke1,2
15% of strokes in US are attributable to AF3
Stroke severity (and mortality) is worse with AF
than without AF4
Incidence of all-cause stroke in patients
with AF: 5%1
Stroke risk persists even in asymptomatic AF5
1. Fuster V, et al. J Am Coll Cardiol. 2001;38(4):1231-1266.
2. Benjamin EJ, et al. Circulation. 1998;98(10):946-952.
3. Atrial Fibrillation Investigators. Arch Intern Med. 1994;154(13):1449-1457. 4. Dulli DA, et al. Neuroepidemiology. 2003;22(2):118-123.
5. Page RL, et al. Circulation. 2003;107(8):1141-1145.

6
AF Is the Leading Cause of
Hospitalizations for Arrhythmia
Hospital Days (thousands)
N=517,699 (representing 10% of CV admissions).
Hospital Admissions in US
VT
VF
Unspecified
Sick sinus
Premature beats
Junctional
Conduction disease
Cardiac arrest
AFL
AF
0 200 400 600 800 1000
VF, ventricular fibrillation; VT, ventricular tachycardia.
Adapted from Waktare JE, et al. J Am Coll Cardiol. 1998;81(suppl 5A):3C-15C.

7 Reproduced with permission from Miyasaka Y, et al. J Am Coll Cardiol. 2007;49(9):986-992.
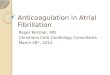
Mortality After Diagnosis of AF
4-month
HR, 9.62 Post-4 months
HR, 1.66
100
80
60
40
20
0 0 2 4 6 8 10 0 2 4 6 8 10
Years From AF Dx Years After 4 Mo
From AF Dx
Su
rviv
al, %
P<.0001 P<.0001
MN-white expected
Observed

8
1. Ware JE, et al. New England Medical Center Health Survey; 1993.
2. Dorian P, et al. J Am Coll Cardiol. 2000;36(3):1303-1309.
*Higher numbers indicate higher QoL.
SF-36 = Medical Outcomes Study Short Form 36.
Baseline score
Physical
functioning
Vitality General
health
Mental
health
index
Emotional
role
Social
functioning
SF
-36 s
cale
*
100
90
80
70
60
50
40
General population1
Recent MI1
AF2
HF1
Impact on QoL: AF vs Other CV Illness

9
Pathogenesis of AF
Multiple-wavelet hypothesis1
Focal mechanism with fibrillatory
conduction2
“Autonomic” hypothesis3
1. Moe GK, Abildskov JA. Am Heart J. 1959;58(1):59-70.
2. Konings KT, et al. Circulation. 1994;89(4):1665-1680.
3. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Circulation. 1996;93(5):1043-1065.

10
Conditions Frequently Associated
With Nonvalvular AF1-4
1. Wattigney WA, et al. Circulation. 2003;108(6):711-716.
2. Gersh BJ, et al. Eur Heart J Suppl. 2005;7(suppl C):C5-C11.
3. Fuster V, et al. J Am Coll Cardiol. 2006;48(4):854-906. 4. Mozaffarian D, et al. Circulation. 2008;118(8):800-807.
Hypertension
Aging
Male sex
Obesity/metabolic syndrome/diabetes
Ischemic heart disease
Heart failure/diastolic dysfunction
Obstructive sleep apnea
Physical inactivity
Thyroid disease
Inflammation?

11
% of Patients With AF
Class I – II Class III – IV
Prevalence of AF Increases With Severity
of HF
0
0.1
0.2
0.3
0.4
0.5
0.6

12
Classification of AF
Recurrent AF* ( 2 episodes)
Paroxysmal Persistent
Permanent
• Arrhythmia terminates spontaneously
• AF is sustained
7 days
• Arrhythmia does not terminate spontaneously
• AF is sustained
>7 days • Both paroxysmal and persistent AF can become permanent
*Termination with pharmacologic therapy or direct-current cardioversion does not change the designation.
Fuster V, et al. Circulation. 2006;114(7):e257-e354.

13
Treatment

14
Treatment Goals and Strategies
Maintenance of SR
Pharmacologic
Stroke prevention
Nonpharmacologic
Class IA
Class IC
Class III
-blocker
Catheter ablation
Pacing
Surgery
Implantable devices
Pharmacologic • Warfarin
• Aspirin
• Thrombin Inhibitor
Nonpharmacologic • Removal/isolation
LA appendage
Rate control
Pharmacologic • Ca2+ blockers
• -blockers
• Digitalis
• Amiodarone
Nonpharmacologic • Ablate and pace
Prevent Remodeling CCB
ACE-I, ARB
Statins
Fish oil

15
CHADS2 Risk Criteria for Stroke
in Nonvalvular AF
Risk Factors Score
C Recent congestive heart failure 1
H Hypertension 1
A Age 75 y 1
D Diabetes mellitus 1
S2 History of stroke or transient ischemic attack
2
Gage BF, et al. JAMA. 2001;285(22):2864-2870.

16 Gage BF, et al. JAMA. 2001;285(22):2864-2870.
Stroke Risk in Patients With Nonvalvular AF Not Treated With Anticoagulation Based on the CHADS2 Index
CHADS2, Congestive heart failure, Hypertension, Age >75, Diabetes mellitus, and prior Stroke or
transient ischemic attack.
Warfarin
0 5 10 15 20 25 30

17
Risk Stratification for AF:
Antithrombotic Therapy
Risk Category Recommendation
Low Risk
No moderate-risk factors
CHADS2 = 0
Aspirin, 81-325 mg a day
Moderate Risk
One moderate-risk factor
CHADS2 = 1
Aspirin, 81-325 mg a day
or warfarin (INR 2.0-3.0)
High Risk
Any high-risk factor or 2 moderate-risk factors
CHADS2 = 2
Warfarin (INR 2.0-3.0*)
*INR 2.5-3.5 for prosthetic valves. What to do about “weaker” risk factors?
Fuster V, et al. Circulation. 2006;114(7):e257-e354.
ACC/AHA/ESC 2006 Atrial Fibrillation Guidelines

www.escardio.org/guidelines

www.escardio.org/guidelines

www.escardio.org/guidelines

21
Limitations of Warfarin
Limitations Consequences
Slow onset of action Overlap with parenteral anticoagulant
Genetic variation in metabolism Variable dose requirements
Multiple food and drug interactions Frequent coagulation monitoring
Narrow therapeutic window Frequent coagulation monitoring
Hirsh J. N Engl J Med. 1991;324(26):1865-1875.
Bates SM, Weitz JI. Br J Haematol. 2006;134(1):3-19.
Courtesy of PR Kowey, MD.

22
Limitations of Warfarin
Limitations Consequences
Slow onset of action Overlap with parenteral anticoagulant
Genetic variation in metabolism Variable dose requirements
Multiple food and drug interactions Frequent coagulation monitoring
Narrow therapeutic window Frequent coagulation monitoring
Hirsh J. N Engl J Med. 1991;324(26):1865-1875.
Bates SM, Weitz JI. Br J Haematol. 2006;134(1):3-19.
Courtesy of PR Kowey, MD.

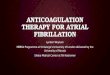
Targets of New Anticoagulant Agents
23 Becattini Throm Res 2012

Main Features of New Anticoagulant
Agents
Becattini Throm Res 2012

Clinical Trials and new Anticoagulant Agents
- A Summary -
Becattini Throm Res 2012

Dabigatran versus Warfarin in Patients with Atrial Fibrillation (RE-LY)
Connolly SJ et al. N Engl J Med 2009;361:1139-1151
• In patients with atrial fibrillation, dabigatran given at a dose of 110 mg was associated with rates of stroke and systemic embolism that were similar to those associated with warfarin, as well as lower rates of major hemorrhage
• Dabigatran administered at a dose of 150 mg, as compared with warfarin, was associated with lower rates of stroke and systemic embolism but similar rates of major hemorrhage

Patel MR et al. N Engl J Med 2011;365:883-891
Rivaroxaban versus Warfarin in Nonvalvular Atrial Fibrillation (ROCKET AF)
• In this trial, 14,264 patients with atrial fibrillation were randomly assigned to receive either rivaroxaban or warfarin.
• In a per-protocol, as-treated analysis, rivaroxaban was noninferior to warfarin with respect to the primary end point of stroke or systemic embolism.

Connolly SJ et al. N Engl J Med 2011;364:806-817
Apixaban in Patients with Atrial Fibrillation
(AVERROES)
• In this trial, the factor Xa inhibitor apixaban was shown to reduce the risk of stroke or systemic embolism, as compared with aspirin, without a significant increase in the risk of major bleeding.
• Apixaban is an alternative to aspirin for patients who cannot take warfarin.

Apixaban versus Warfarin in Patients with Atrial Fibrillation (ARISTOTLE)
Granger CB et al. N Engl J Med 2011;365:981-992
Apixaban was superior to warfarin in preventing stroke or systemic embolism, caused less bleeding, and lowered mortality.

Which New Agent Should We
Recommend ?
Raise the issue / Pop the question
Variables to consider:
- coumadin experience
- approach to new drugs
- cost considerations
- h/o GI symptoms
- compliance issues

31
Treatment Goals and Strategies
Maintenance of SR
Pharmacologic
Stroke prevention
Nonpharmacologic
Class IA
Class IC
Class III
-blocker
Catheter ablation
Pacing
Surgery
Implantable devices
Pharmacologic • Warfarin
• Aspirin
• Thrombin Inhibitor
Nonpharmacologic • Removal/isolation
LA appendage
Rate control
Pharmacologic • Ca2+ blockers
• -blockers
• Digitalis
• Amiodarone
Nonpharmacologic • Ablate and pace
Prevent Remodeling CCB
ACE-I, ARB
Statins
Fish oil

32
Rate Control
End point – Resting and ambulatory ventricular rates similar
to those expected in sinus rhythm
– Best assessed with Holter monitoring
– Determining pulse on exam and heart rate on ECG are not sufficient
Methods
– Digitalis: in sedentary patients or CHF
– -blockers and/or CCBs (verapamil, diltiazem): needed in most active individuals
– AVN ablation plus pacemaker: in resistant patients
Special considerations
– Brady-tachy syndrome (pindolol, or pacer plus drugs)
– Preexcitation (focus on the BT as well as the AVN)

33
No (or minimal) heart disease
Amiodarone Dofetilide
HF CAD Hypertension
Amiodarone Dronedarone Flecainide
Propafenone Sotalol
Yes
Maintenance of SR
Substantial LVH
No
Dronedarone Flecainide
Propafenone Sotalol
Catheter ablation
Amiodarone Dofetilide
Catheter ablation
Catheter ablation
Amiodarone Catheter ablation
Dofetilide Dronedarone
Sotalol
Amiodarone Dofetilide
Catheter ablation
Rhythm Control Therapies to Maintain Sinus Rhythm
2011 ACCF/AHA/HRS Focused Update on the Management of AF
Reproduced with permission from Wann LS, et al. Circulation. 2011;123(1):104-123.


35
Current Efficacy of AF Ablation:
Estimates
Surgical Ablation Single Procedure Multiple
Optimal patient
Less optimal patient
Poor candidate
70%-90%
60%-80%
50%-60%
Catheter Ablation
Optimal patient
Less optimal patient
Poor candidate
60%-80%
50%-70%
40%
80%-90%
70%-80%
40%-60%
Calkins H, et al; Heart Rhythm Society Task Force on catheter and surgical ablation of atrial
fibrillation. Heart Rhythm. 2007;4(6):816-861.
Calkins H, et al. Circ Arrhythmia Electrophysiol. 2009;2(4):349-361.


37
Patient Selection for Ablation
Courtesy of Hugh Calkins, MD.
Variable
Symptoms Highly symptomatic Minimally symptomatic
Class I and III drugs failed 1 0
AF type Paroxysmal Long-standing persistent
Age Younger (<70 years) Older ( 70 years)
LA size Smaller (<5.0 cm) Larger ( 5.0 cm)
Ejection fraction Normal Reduced
Congestive heart failure No Yes
Other cardiac disease No Yes
Pulmonary disease No Yes
Sleep apnea No Yes
Obesity No Yes
Prior stroke/TIA No Yes

38
Treatment Goals and Strategies
Maintenance of SR
Pharmacologic
Stroke prevention
Nonpharmacologic
Class IA
Class IC
Class III
-blocker
Catheter ablation
Pacing
Surgery
Implantable devices
Pharmacologic • Warfarin
• Aspirin
• Thrombin Inhibitor
Nonpharmacologic • Removal/isolation
LA appendage
Rate control
Pharmacologic • Ca2+ blockers
• -blockers
• Digitalis
• Amiodarone
Nonpharmacologic • Ablate and pace
Prevent Remodeling CCB
ACE-I, ARB
Statins
Fish oil

Conclusions
Atrial fibrillation is common
Atrial fib is an important risk factor for stroke.
Stroke risk can be determined using CHADS
and CHADSvasc
Patients at increased risk of stroke should be
anticoagulated.
Aspirin does little.
The era of new anticoagulants is here and
now.

Thank You
40