Embed Size (px)
Citation preview
6/19/2017
1
PREVENTING INTERPERSONAL
VIOLENCE BY BUILDING PROUD BRAINSRON KAISER, PH.D, ABPP & CARYN SEEBACH, PSY.D.
JEFFERSON HEADACHE CENTER
SIDNEY KIMMEL MEDICAL COLLEGE AT THOMAS JEFFERSON UNIVERSITY
PHILADELPHIA, PA
DISCLOSURES
• We have no actual or potential conflict of interest in relation to this program/presentation.
PART I: A NEW WAY OF THINKING ABOUT DOING PSYCHOTHERAPY
• Everybody knew that the Earth was flat…………..
• until they learned it was round
The brain was fully developed by early adulthood
Learning took place without the brain changing through either:
Classical conditioning: S – R (Pavlov)
Operant conditioning: S – O – R (Skinner)
HISTORICAL CONCEPTS OF BRAIN FUNCTIONING
Implications for special education
Mandatory retirement
Sedentary retirement
Little attention given to activities that could prolong neurogenesis and ward off decline.
Psychotherapies were developed that emphasized overcoming problems rather thriving.
CONSEQUENCES OF THE NON-PLASTIC BRAINPSYCHOLGY’S CONTRIBUTIONS TO GROWTH
AND CHANGE HAVE IMPACTED ON
• Schools
• Parenting
• Sports
• Industry
But not necessarily on the conduct of psychotherapy
6/19/2017
2
• Between stimulus and response there is a space. In that space is the power to choose our response. In our response lies our growth and our freedom.
VIKTOR FRANKL QUOTE CORE VALUES FOR EFFECTIVE THERAPY TODAY
• Commitment to personal mental health
• Coherent psychotherapeutic philosophy
• Recognition that the brain can rewire itself
• Orientation toward growth rather than pathology
• Understanding that change spreads from the therapy setting outward
THESE CORE VALUES ARE REFLECTED IN….
• Positive psychology
• Neuroplasticity
• The popularity of coaching (a largely unregulated field)
BRAIN FACTS
• The brain ‘reads’ information from the body 30 times per second for your entire lifespan
• The adult brain adapts throughout the lifespan based on information it receives from the body
• We only experience pain when electrical signals reach the cognition parts of the brain
• The brain has 100 billion nerve cells and 1000 trillion synapses which are used to communicate between the brain and body
NEUROPLASTICITY
• A process by which the brain is constantly changing in response to inputs from our senses, memories, cognitions, beliefs, movement, and emotions.
• These changes likewise occur in
response to aversive events such as disease, traumatic events, stressful
situations, and injuries
Moskowitz, M.H. & Golden, M.D., (2013). Neuroplastic Transformation: Your Brain on Pain.
NEUROPLASTIC TRANSFORMATION
What fires together,
wires together
Use it or lose it
When we make them we break
them..
6/19/2017
3
Initial studies dealt with localization and the abilities of areas of the brain to take over the functions of other areas – rather than neurogenesis (the growth of new neurons)
EARLY UNDERSTANDING OF BRAIN PLASTICITY CAME FROM ANIMAL STUDIES
• Described learning as a function of the brain.
• “When an axon of cell A is near enough to excite cell B and repeatedly and persistently takes place in firing it, some growth process or metabolic change takes place in one or both cells such that A’s efficiency, as one of the cells firing B, is increased” (1949)
• Hebb’s Law: Neurons that fire together wire together
D. O. HEBB
• Won a Nobel prize for their work on neuroplasticity in young cats.
• Brain had to receive visual stimulation between 3rd & 8th week of life.
• When 1 eye was sewn shut during that period, the cat remained blind in that eye for life.
• But the brain didn’t remain idle, and started to process visual input from the other eye –i.e., the brain rewired itself.
HUBEL AND WEISEL
• In the 1930’s, Penfield began mapping the human brain by stimulating different parts of the brain during neurosurgery with cancer and epilepsy patients who could be awake during surgery.
• He mapped the sensory and motor parts of the brain.
• The maps were assumed to be useful only for anatomy study because it was believed that the brain couldn’t change.
WILDER PENFIELD
• Experiments with monkeys (e.g., severing the median nerve, sewing 2 fingers together) resulted in the concept of competitive plasticity (competition for brain map space).
• The importance of practice: Use it or lose it.
• Explains problems for adults in learning foreign languages, computer skills, etc., as well as
difficulty in breaking habits.
• Merzenich was a prime mover behind cochlear implants and Fast ForWord.
MICHAEL MERZENICH
Shaping behavior of deafferented monkeys
Spinal shock 1st 2-6 months
Using rewards for small positive moves
Bad arm returned to functioning
Applied the same principles in labor-intensive stroke rehab (using slings and mitts) – suggesting that learned nonuse during cortical shock period plays a role in continued loss of function
EDWARD TAUB
6/19/2017
4
• The role of both playing the piano and mentally rehearsing playing increased the area of the motor cortex associated with finger flexor and extensor muscles (Pacal-Leone, 2003)
• Research on the posterior hippocampi of London taxi drivers (Maguire, 2001)
• Brain changes among meditators and yoga practitioners (Sarah Lazar’s work)
OTHER EXAMPLES OF NEUROPLASTICITY
• Neural pathways can change
• Neurogenesis can occur
• Proactive positive change can occur
WHY POSITIVE NEUROPLASTICITY?
100 billion cells in the human brain – but there may be a few billion less.
Although it was known that neurogenesis occurs it rats and birds, the knowledge of adult human neurogenesis is a late 20/early 21st century finding based upon research in multiple labs.
The implications are profound
Potential growth is present throughout life.
We have the ability to change.
NEUROGENESIS AREAS MOST INVOLVED IN NEUROGENESIS AND POSITIVE NEUROPLASTICITY
Meta-analysis of over 200 studies involving an n of almost 275,000 people found that happiness was correlated with success in almost every domain measured – including marriage, health, friendships, community involvements, career success (productivity,
leadership, and earnings).
“Study after study shows happiness precedes success”
(Lyubomirsky et al, 2005)
POSITIVE NEUROPLASTICITY RESEARCH FINDINGS (1)
• Happiness as college freshmen predicted income 19 years later regardless of initial wealth.
• Happiness predicted fewer objective symptoms of illness among subjects exposed to a cold virus.
• Retrospective study of content of early diaries of 180 nuns showed that 90% of the happiest quartile were still alive at age 85 compared with 34% of the least happy quartile.
POSITIVE NEUROPLASTICITY RESEARCH FINDINGS (2)
6/19/2017
5
Even if equal in intensity, things of a more negative nature have a greater effect on one’s psychological state than neutral or positive events. (Baumeister et al, 2003, 2014)
Evolutionary adaptation.
Cognitive accompaniment of the Fight, Flight or Freeze response.
Seen during imaging as early as infancy.
THE NEGATIVITY BIAS
Divorce has consistently been correlated more with negative interactions than with positive ones.
Superior recall exists for unpleasant childhood memories than for good ones – even among those who regarded themselves as having had good childhoods.
2004 Harvard Crimson depression survey
Track and field records.
CBT arises out of widespread research reflecting the common tendency to interpret events negatively.
NEGATIVITY BIAS FINDINGS
• Survey of research through 1998 showed a 17 to 1 negativity to positivity ratio.
• Researchers tend to get rid of healthy outliers and focus upon averages rather than learning from them.
• Required Psychology CE courses include Suicide Prevention & Child Abuse – not Positive
Psych or Neuroplasticity
NEGATIVITY BIAS RESEARCH IN PSYCHOLOGY
• Becoming reactive when conditions are challenging.
• Feeling uneasy & dissatisfied even when conditions are fine.
• Over-learning from bad experiences.
• Become quickly sensitized toward reactivity.
• Slowness in returning to comfort even when the threat is out of the way.
5 BASIC FEATURES OF THE NEGATIVITY BIAS (FROM HANSON)
The limbic system releases “happy” neurotransmitters in a positive state:
Dopamine
Endorphins
Oxytocin
Serotonin
Brain-derived neurotropic factor (BDNF) is increased to “fertilize” the brain, grow new neurons, & help existing neurons to survive.
Cortisol production is reduced in positive states.
NEUROCHEMICAL DIFFERENCES BETWEEN POSITIVITY AND NEGATIVITY
Connection (associated with neocortex)
Acceptance (associated with subcortex)
Safety (associate with the brain stem)
The more primitive the need, the more work that needs to be done to change the brain.
HANSON’S 3 BASIC NEEDS RELATED TO DEVELOPMENT OF THE HUMAN BRAIN
6/19/2017
6
• Chronic criticism, especially from parents
• Trauma
• Abuse
• Unsuccessful experiences
• Chronic medical, psychological, or educational conditions
REINFORCERS OF THE NEGATIVITY BIAS IMPLICATIONS FOR TRAUMA
• Brain wiring in the trauma exposed brain
• The psychopathological signs of trauma are not static over time, nor is the form of the expression of traumatic memories. This fluidity is a consequence of the sensitization that is driven by reminders of the traumatic event and the vulnerability of memory to being modified with repeated recall (Jones, et al., 2003; Grillon, et al., 1996; Shalev, et al., 2000; Shalev, 2002; Moscovitch, et al., 2005)
IMPLICATIONS FOR TRAUMA (2)
• The diversity of findings and the heterogeneity of symptomatology among people suffering psychological traumas suggest that it may not be possible to identify one specific neural circuit underlying PTSD.
• Nevertheless, neuroimaging studies of symptom provocation have identified some consistent patterns, including reduced left hemisphere activity, and hypoperfusion in the anterior cingulate (AC), dorsolateral prefrontal cortex (PFC), hippo- campus, and Broca’s area. Other areas have shown consistently increased activation, including the para- hippocampal gyrus, posterior cingulate, and amygdala.
• Lanius et al., (2004) using a script-driven symptom provocation paradigm, have observed greater activity in the right posterior cingulate, right parietal lobe, and right occipital lobe in PTSD and less activity in the left hemisphere[28]. These findings support the suggestion of the inherently non-verbal nature of traumatic memory recall in PTSD subjects, compared to a more verbal pattern of traumatic memory recall in subjects without PTSD.
IMPLICATIONS FOR TRAUMA (3)
• It appears that disruption of activity in the left frontal region is of particular importance in PTSD and the propensity to engage right hemisphere networks. It has been suggested that the left hemisphere sequentially organizes information and is responsible for problem solving and categorization operations which may explain why traumatic memories are experienced as ‘belonging to the present’, because brain regions necessary for sequencing and categorizing experiences are not adequately activated (Hull, 2002; Pissiota, et al., 2002; Van der Kolk, 1997)).
• The reorganization and reconstruction of past traumatic experiences into more adaptive memories is used as the model guiding the therapeutic process for trauma survivors (Peres, et al., 2008).
6/19/2017
7
TREATMENT APPROACHES TO TRAUMA BASED IN NEUROSCIENCE
• Neuroscience findings provide crucial insight for psychotherapy, highlighting that emotionally charged memories are peculiar representations of an event, distant from the original episode, but salient in their significance for the individual (Peres, McFarlane, et al., 2008)
• Neuroimaging studies of traumatic recall and hypnotic processes have demonstrated the same brain structures (thalamus, hippocampus, amygdala, medial PFC, and AC cortex) involved in both research lines (Vermetten & Bremner , 2004).
• Therapeutic interventions focusing on emotions and the conscious processing of these events will modulate the memory for these events, effectively changing the interactions between underlying neural networks. It is argued that this shift of consciousness, will result in changes in the perception of the same event (Dietrich, 2003).
IMPLICATIONS FOR PERPETRATORS OF VIOLENCE
• The “cycle of violence” hypothesis postulates that children exposed to abuse and neglect will develop abusive tendencies themselves in adulthood (Widom, 1989b).
• Nevertheless, recent investigation was unable to confirm this hypothesis consistently (Forsman & Langstrom, 2012)
• So what is the missing link…..?
THE BRAINS OF VIOLENT OFFENDERS ARE DIFFERENT
• Structure (lower volume) and function (failure of fear conditioning) of the amygdala is different among criminals when compared with non-criminals (Pardini, 2013; Glenn,2009; (Raine et al, 2010)
• Violent offenders have been found to have a trifecta of symptoms (Pincus, 2002):
• Brain damage (often poorly documented)
• Exposure to violent environments, including being victims of chronic abuse
• Paranoid personality characteristics
PERPETRATORS OF VIOLENCE CONT’D
• Witnessing domestic violence has demonstrated the strongest risk for adult violence through a direct pathway, with psychotic symptoms and Antisocial Personality Disorder (ASPD) as partial mediators.
• Childhood physical abuse is associated with intimate partner violence (IPV), mediated by
ASPD and alcohol dependence.
• Neglect is associated with violence toward strangers, mediated by ASPD.
NEUROPLASTICITY AND VIOLENCE
• Just like Merzenich found with learning difficulties, early intervention focusing on nutrition, exercise & cognitive skills led to reduced criminal potential years later (Raine et al, 2003)
• 10-week yoga class led to reduced impulsivity & improved positive affect among prisoners (Bilderbeck et al, 2013)
• Violent Offenders Therapeutic Program• Parklea Correctional Centre in Australia targeting violent offenders with highest risk of recidivism
• Multidisciplinary team approach
• 12-14 months duration
• Initial Preparation phase followed by 6 treatment focused modules and completed with a relapse prevention phase
• Participants in readiness phase more likely to complete program
• Participants showed reductions in: levels of anger/anger expression, reduced level of criminal thinking, increase ability to see perspective of others, improved ability to regulate anger, and significant improvements in empathic ability
Epidemiologic studies consistently find a relationship between headache and depression. (Lipton et al 2003; Merikangas et al, 1990; Breslau & Rasmussen, 1992)
Catastrophizing in headache patients (Kaiser & Weatherby, 2004; Kaiser, 2016)
Catastrophizing is the major predictor of reduced headache-related QOL. (Holroyd et al,
2007)
NEGATIVITY BIAS AND HEADACHE
6/19/2017
8
NEGATIVITY BIAS AND CHRONIC PAIN
• People who are fearful of pain tend to report more negative pain experiences
• Mechanisms of attention may be particularly important in the perception of painful stimuli, especially amongst pain fearful individuals (Keogh, et al., 2001)
• One reason why those with a high fear of pain are particularly susceptible to negative pain experiences could be due to biased attentional processes
• Psychological inflexibility partly accounts for the variance observed between self-discrepancy (when a person feels the failure to fulfill one’s hopes or responsibilities) and pain outcomes (Kwok, et al., 2016).
• The way in which psychological (in)flexibility accounts for the relationship between self-discrepancy and pain outcomes can be explained by this essential notion of adjustment with an accepting and open attitude towards internal and external events (Hayes et al., 2006).
THE NEGATIVITY BIAS AS TOLD BY LOUIS CK
PART TWO: A NEW WAY OF DOING PSYCHOTHERAPY
POSITIVE PSYCHOLOGY DEFINED
• Positive psychology is that branch of psychology that involves the study and promotion of well-being.
• The gold standard for measuring well-being is flourishing.
• The goal of positive psychology is the increase of flourishing.
Seligman, 2011
POSITIVE PSYCHOLOGY DEFINED (2)
• Psychology is not just the study of pathology, weakness, and damage. It is also the study of strength and virtue.
• Treatment is not just fixing what is broken. It is nurturing what is best.
Seligman & Csikszentmihalyi (2000)
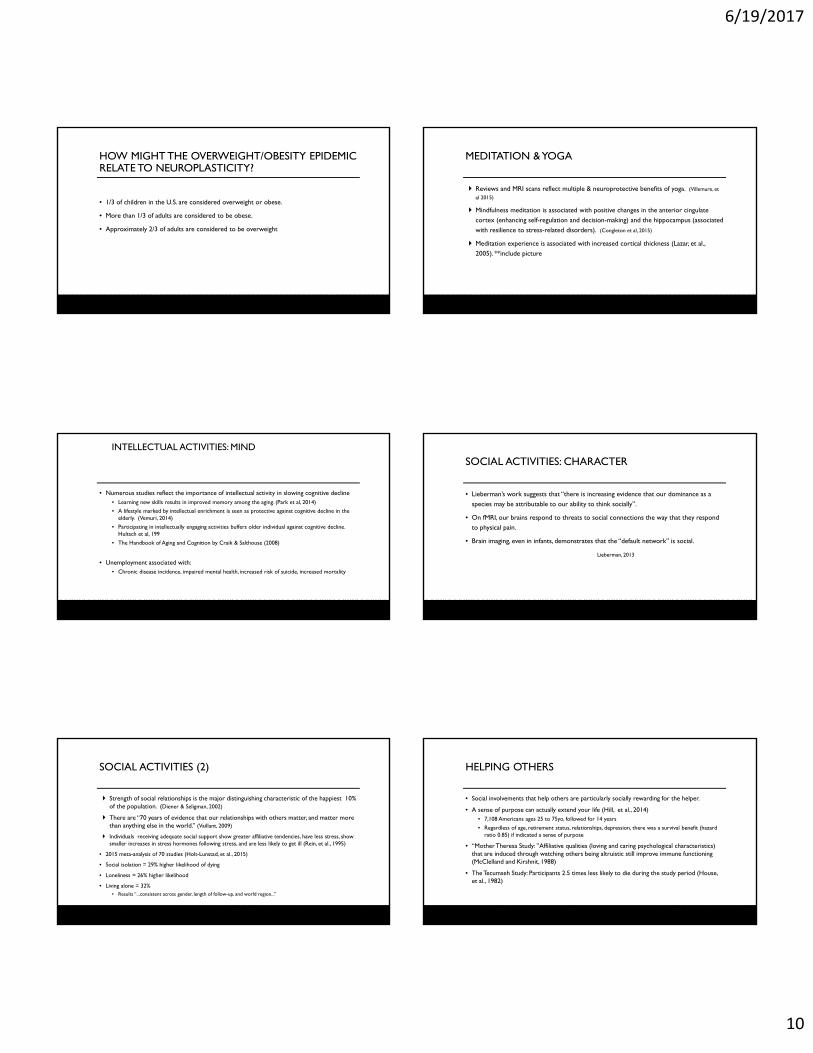
WHAT DETERMINES HAPPINESS?LYUBOMIRSKY, 2007
•
6/19/2017
9
PSYCHOTHERAPY COMES FROM A DISEASE REDUCTION MODEL
• Historical definition of health = Absence of disease.
• Psychoanalytic goal of tension-reduction.
• CBT focuses on irrational beliefs, automatic negative thoughts, etc.
• DSM gold standard is “No Diagnosis”.
• Reportable scales on the MMPI are the elevated ones.
• NIMH funding is primarily granted for disease research.
WHO DEFINITIONS OF HEALTH AND MENTAL HEALTH HAVE CHANGED
• Health is a state of complete physical, mental and social well-being, and not merely the absence of disease or infirmity.
• Mental Health is a state of well-being in which an individual realizes his or her own abilities, can cope with the normal stresses of life, can work productively, and is able to make a contribution to his or her community.
MORE MOTIVATING THAN MONEY(AFTER A CERTAIN POINT)
• Autonomy
• Mastery
• Purpose
Health & fitness Body
Intellectual activities Mind
Social activities – Character
with bonus points for doing good
OVER TIME, 3 TYPES OF ACTIVITIES HAVE CONSISTENTLY CONTRIBUTED TO POSITIVE NEUROPLASTICITY
HEALTH AND FITNESS: BODY
• “What if there was one prescription that could prevent and treat dozens of diseases, such as diabetes, hypertension, and obesity?”
• Robert E. Sallis, M.D., M.P.H. FACSM,
Exercise is Medicine Task Force Chairman
Naperville School District study (Ratey,2008)
• Following a program that included daily gym classes and “small sided” sports, Naperville 8th graders scored 1st in the world in science and 6th in math.
Multiple studies demonstrate correlation between fitness, self-esteem, improved standardized test scores, and a reduction in disciplinary incidents.
Potential for warding off cognitive decline in the elderly Increased brain volume and density among senior adults who exercise (Kramer, 1999-)
The role of exercise to increased BDNF to neurogenesis to reduced dementia (Cotman, 2015)
Multiple studies demonstrate correlation between fitness, self-esteem, improved test scores, and fewer disciplinary incidents.
THE BENEFITS OF EXERCISE
6/19/2017
10
• 1/3 of children in the U.S. are considered overweight or obese.
• More than 1/3 of adults are considered to be obese.
• Approximately 2/3 of adults are considered to be overweight
HOW MIGHT THE OVERWEIGHT/OBESITY EPIDEMIC RELATE TO NEUROPLASTICITY?
Reviews and MRI scans reflect multiple & neuroprotective benefits of yoga. (Villemure, et
al 2015)
Mindfulness meditation is associated with positive changes in the anterior cingulate cortex (enhancing self-regulation and decision-making) and the hippocampus (associated with resilience to stress-related disorders). (Congleton et al, 2015)
Meditation experience is associated with increased cortical thickness (Lazar, et al., 2005). **include picture
MEDITATION & YOGA
• Numerous studies reflect the importance of intellectual activity in slowing cognitive decline• Learning new skills results in improved memory among the aging. (Park et al, 2014)
• A lifestyle marked by intellectual enrichment is seen as protective against cognitive decline in the elderly. (Vemuri, 2014)
• Participating in intellectually engaging activities buffers older individual against cognitive decline. Hultsch et al, 199
• The Handbook of Aging and Cognition by Craik & Salthouse (2008)
• Unemployment associated with:• Chronic disease incidence, impaired mental health, increased risk of suicide, increased mortality
INTELLECTUAL ACTIVITIES: MIND
SOCIAL ACTIVITIES: CHARACTER
• Lieberman’s work suggests that “there is increasing evidence that our dominance as a species may be attributable to our ability to think socially”.
• On fMRI, our brains respond to threats to social connections the way that they respond to physical pain.
• Brain imaging, even in infants, demonstrates that the “default network” is social.
Lieberman, 2013
Strength of social relationships is the major distinguishing characteristic of the happiest 10% of the population. (Diener & Seligman, 2002)
There are “70 years of evidence that our relationships with others matter, and matter more than anything else in the world.” (Vaillant, 2009)
Individuals receiving adequate social support show greater affiliative tendencies, have less stress, show smaller increases in stress hormones following stress, and are less likely to get ill (Rein, et al., 1995)
• 2015 meta-analysis of 70 studies (Holt-Lunstad, et al., 2015)
• Social isolation = 29% higher likelihood of dying
• Loneliness = 26% higher likelihood
• Living alone = 32% • Results “...consistent across gender, length of follow-up, and world region...”
SOCIAL ACTIVITIES (2) HELPING OTHERS
• Social involvements that help others are particularly socially rewarding for the helper.
• A sense of purpose can actually extend your life (Hill, et al., 2014)• 7,108 Americans ages 25 to 75yo, followed for 14 years
• Regardless of age, retirement status, relationships, depression, there was a survival benefit (hazard ratio 0.85) if indicated a sense of purpose
• “Mother Theresa Study: ”Affiliative qualities (loving and caring psychological characteristics) that are induced through watching others being altruistic still improve immune functioning (McClelland and Kirshnit, 1988)
• The Tecumseh Study: Participants 2.5 times less likely to die during the study period (House, et al., 1982)
6/19/2017
11
• Positive Psychology
• Mindset (Carol Dweck)
• Barbara Frederickson’s Broaden and Build theory
• Cascade of positive social consequences (Sonja Lyubomirsky)
• Flow (Mihaly Csikszentmihalyi)
• The HEAL Method (Rick Hanson)
• Goal-Achieving Psychotherapy
WAYS OF PROMOTING POSITIVE NEUROPLASTICITY
POSITIVE PSYCHOLOGY
POSITIVE PSYCHOLOGY
• First articulated by Seligman and Czikszentmihalyi (2000) it represented a new way of using psychology and psychological research to focus on helping individual to flourish and achieve well-being rather than focusing on overcoming pathology.
• It represents a psychology of hope, optimism, and strength-building
• A major strength is its commitment to scientific research.
• A major weakness is that it was not primarily developed by therapists.
SELIGMAN
• His journey went from Learned Helplessness to Learned Optimism to Authentic Happiness to Flourish - and the psychology of well-being.
• Developed the MAPP program at Penn.
• Instrumental in developing major positive psychology concepts – including Signature
Strengths and PERMA.
• Collaborated with Chris Peterson in researching and writing Character Strengths and
Virtues.
PERMA
• Positive Emotion
• Engagement
• Relationships
• Meaning
• Accomplishment
CHARACTER STRENGTHS AND VIRTUES
• Positive Psychology’s answer to the DSM and ICD – “A Manual for the Sanities”.
• The focus is on what is right about people rather than what is wrong.
• Based on substantial research across cultures.
• 6 Virtues encompass 24 Character Strengths.
6/19/2017
12
6 VIRTUES
• STRENGTHS OF WISDOM AND KNOWLEDGE
• STRENGTHS OF HUMANITY
• STRENGTHS OF JUSTICE
• STRENGTHS OF TEMPERANCE
• STRENGTHS OF TRANSCENDENCE
• STRENGTHS OF COURAGE
OTHER INDICATORS OF STRENGTHS
• Resilience
• Savoring
• Grit
• Posttraumatic Growth
ASSESSING SIGNATURE STRENGTHS
• Go to www.authentichappiness.org
• VIA Survey of Character strengths (240 items)
• Brief Strengths Test (24 items)
• Several other tests
• Test results are used for research as well as your own benefit
MINDSET: THE CONTRIBUTIONS OF CAROL DWECK
• Mindset: The view that you adopt for yourself.
• Fixed Mindset: The belief that your qualities are unchangeable – and you have to keep proving yourself over and over.
Related to being praised for your attributes.
• Growth Mindset: The belief that your basic qualities can be changed by your efforts.
Related to being praised for your efforts.
• Substantial research supports the benefits of the growth mindset.
• Have a positive experience
• Enrich it
• Absorb it
• Link positive and negative experience so that the positive soothes and even replaces the negative. (optional)
(From Rick Hanson)
PRACTICAL TOOLS FOR THE THERAPIST: THE HEAL METHOD
PILOT STUDY ON THE HEAL PROCESS
• A randomized waitlist control pilot study on the Taking in the Good course (46 subjects), not yet peer-reviewed.
• Course participants, compared to the control group, reported significantly more Contentment, Self-Esteem, Satisfaction with Life, Savoring, and Gratitude.
• After the 7-week course and also at 2-month follow-up, pooled participants also reported significantly more Love, Compassion, Self-Compassion, Mindfulness, Self-Control, Positive Rumination, Joy, Amusement, Awe, and Happiness and less Anxiety and Depression (Hanson, 2016).
6/19/2017
13
ARE WE TALKING ABOUT PRACTICE? GOAL-ACHIEVING PSYCHOTHERAPY
GOAL-ACHIEVING PSYCHOTHERAPY: A MODEL FOR POSITIVE PRACTICE
• GAP builds upon the research orientation and philosophy of positive psychology.
• GAP builds upon effective techniques of practice from several approaches, primarily CBT.
• GAP introduces unique concepts involving the role of the therapist, the purpose of psychotherapy, history, the goals of treatment, and the process.
GOAL-ACHIEVING PSYCHOTHERAPY (GAP)
• Bridges the GAPs between:
• Thinking and doing
• Gaining and maintaining
• The past and the future
• Science and practice
PRINCIPLES AND PRACTICES OF GAP (1)
• The approach is forward looking and positive.
• The approach is geared toward building personal strengths to manage change and growth.
• The focus is primarily on the solution, not the problem.
• The past is meaningful – especially as it relates to character strengths and achievements.
• The therapist is active, directive, supportive and a cheerleader for growth and change.
PRINCIPLES AND PRACTICES OF GAP (2)
• The patient/client is active in preparing a Mission Statement and setting an achieving goals.
• Goal setting is designed to ensure maximum success by utilizing small and measureable forward steps.
• Wallowing is avoided.
• Activity is the default.
• Once positive commitment and direction is implemented, other forms of therapy can be incorporated.
• Positive personality change can take place throughout the life span.
6/19/2017
14
PRINCIPLES AND PRACTICES OF GAP (3)
• The Type P Personality is the model of the healthy personality.
• Emotional health is always a work in progress.
• GAP principles can be pursued on a do-it-yourself basis, in therapy, or through coaching –depending upon your needs at any specific time.
• GAP-specific materials are available to aid in the implementation and maintenance of progress.
• www.thementalhealthgym.com is the ongoing source of GAP resources and information.
THE GYM AS A MODEL
• Wellness is a central concept
• Open to all shapes and sizes
• Individual measureable goals
• Diagnosis is descriptive, not prescriptive.
GAP ASSESSMENT ALTERNATIVES TO TRADITIONAL DIAGNOSIS
• Competent Person’s Disease – “the addiction to 2nd place”
• The “Too Excuse”
• Over-thinking
• Under-rating (A/Fail thinking: Ascribing unimportance to achievements; Luck)
• Waiting for an A
THE TYPE P PERSONALITY
• The ultimate goal
• Assessment is done throughout the process
• Roughly comparable to PERMA
TYPE P PERSONALITY
• Personal goal-directed
• Proactive
• Positive
• Passionate
• Persistent
• Playful
GAP: THE INTRODUCTORY SESSION
• Understanding the reason for treatment
• Expression of therapist gratitude as part of informed consent
• Explanation of process and philosophy
• History-taking within the context of strength-building
• Introduction to the role of activity level and homework
6/19/2017
15
THE ROLE OF HISTORY
• Establish early the importance of moving forward to develop strengths.
• Identify unhappy aspects of history – to primarily use in the future.
• Identify positive aspects of history.
“When was the best time in your life?”
“What things do you like most about yourself?”
“What makes you so resilient?”
• Be prepared to revisit history from a position of strength.
GETTING UNSTUCK: THE CRITICAL QUESTIONS
1. Are you a fortune teller?
2. What can go right?
3. What does this have to do with you?
4. How is this getting you where you want to go?
5. What will you do now to maintain your success?
WHY A PYRAMID?
• There is a progression (more or less).
• As you move up, more of the work and more of the change takes place outside of the office.
• As you move up, the emphasis is placed more on general than specific changes.
HEALTHY PSYCHOTHERAPIST AND PATIENT WITH NEEDS (1)
• It has long been recognized that certain characteristics are associated with therapist effectiveness – such as empathy, trust, verbal fluency, optimism, and comfort addressing problems. (APA Education Directorate)
• Survey of physical therapists revealed 81% engage in regular physical activity, 99+% don’t smoke, and 79% maintain a healthy weight. (Black et al, 2012)
• Physicians who practice healthy lifestyles are more likely to encourage such practices among their patients. (AMA, 2012)
HEALTHY PSYCHOTHERAPIST AND PATIENT WITH NEEDS (2)
• Healthy therapist can fulfill 3 role-modeling functions: (Morgenroth et al, 2015)
Behavioral
Representations of the possible
Inspirational
• Patient with identified needs provides a structure to implement use of the pyramid
• Identified needs lead to focus on changing rather than wallowing.
6/19/2017
16
CONTRACTED COMMITMENT TO CHANGE
• Positive-oriented Informed consent
• Mutual involvement: “We’re in this together”, “So long as you honor your commitment, “I won’t give up on you”
• Identify what change will look like
• Provider expectations of the client matter (Witt, et al., 2010)
• Study of acupuncture for pain, controlling for everything else including disease severity, pain intensity decreased and physical functioning improved if a physician had high expectations
WHAT IS A MISSION STATEMENT?
• A personal mission statement provides clarity and gives you a sense of purpose.
• It defines who you are and how you will live.
(MissionStatements.com)
MISSION STATEMENT GUIDANCE
• “Describe the way you want to present yourself to the world.”
• Positive
• Grounded in reality
• Focus is on who you are, not who you aren’t
• Sets the tone for the rest of the process
MISSION STATEMENT: EXAMPLES
• Self-oriented: “I want to be the kind of person who has her life pulled together. It is very important that I remain focused and organized in my personal and professional life. I want to be able to trust myself and my decisions. I want to be able to revel in my quirks.”
• Other-oriented: “I want to be respected as useful and important. I want to create positive change in other people’s lives. I want to be remembered by the people I come in contact with.”
MOVING FROM PAST TO FUTURE ORIENTATION
• Acknowledging the past
• Not taking responsibility for someone else’s misdeeds
• What resources can you pull from the past: “When was the best time of your life?” “What do you like about yourself?”
• Not confusing process with outcome.
SETTING MEASUREABLE AND MEANINGFUL GOALS
• The behavioral component of the mission statement
• Identifying 3 areas for meaningful change
Health & fitness
Intellectual functioning
Social
• Selecting one area as your starting point (If in doubt, choose health & fitness)
6/19/2017
17
BUILDING A POSITIVE PROACTIVE ORIENTATION
• Therapist as a cheerleader
• Overcoming Inertia
• Overcoming the Negativity Bias
• Overcoming “The Too Excuse”
• Overcoming “Competent Person’s Disease” – the addiction to 2nd place.
HEALTH AND FITNESS CHANGES
• Exercise
• Diet
• Sleep hygiene
• Yoga
• Meditative exercises - including mindfulness and biofeedback
INTELLECTUAL ACTIVITIES
• Growing and making positive changes throughout the lifespan
• Protective against dementia in the aged
• Overcoming wiring deficits among those with learning deficits (Merzenich)
SOCIAL INVOLVEMENTS
• Social support takes many forms: (emotional, financial, mentorship, affirmation, information)
• Peer-led and clinician-led support groups
• http://www.mentalhealthamerica.net/find-support-groups
• Volunteering and other community activities
• Spiritual communities
• Animal-assisted therapy
• The care team
HELPING OTHERS
• There is a body of research demonstrating a “helper’s high” among volunteers (Piliavin, 2003)
• A small study of MS patients who volunteered as peer supporters of other patients experienced an even greater degree of positive change in themselves than in their patients (Schwartz & Sendor, 1999)
• Therapy should include helping patients to volunteer.
• As Yogi Berra famously stated, “ You should always go to other people’s funerals. Otherwise they won’t come to yours.”
“TAKING IN THE GOOD”
• Actively default to focusing on the positive
• Learn to “emotionally ignore”
• Mindfulness skills are helpful here
• Activate multiple modalities
• Utilize in vivo and planned opportunities to take in the good
• Make it part of your personality’s core
• For gratitude to be of benefit, it must be expressed
6/19/2017
18
PLAYFULNESS
• Playfulness enhances our ability to learn – including increasing BDNF levels (Dewar, 2014)
• Playfulness is associated with lower levels of perceived stress (Magnuson & Barnett, 2012)
• The ability to be playful is correlated with character strengths & psychological well being (Proyer & Ruch, 2011)
• And don’t forget…..that it’s fun to be playful.
PASSION
• Vallerand et al. (2003) define passion as a strong inclination toward a self-defining activity that one likes (or even loves), finds important, and in which one invests time and energy on a regular basis.
• Activities pursued with passion become part of your identity.
• As opposed to obsessive passion, harmonious passion correlates with psychological well-being
PERSISTENCE
• Related to resilience
• Related to grit (passion + perseverance) Duckworth, 2017
• Provides a strategy for coping with both the negativity bias and the fear of maintaining success
SELF-AWARENESS AND CONFIDENCE
• The capacity for introspection
• Whether they agree with a particular reference group or not, decisions and behaviors are based on internal ethical standards and positive changes in the brain.
• “Comfort in one’s own skin”; Absence of jealousy; Not wanting to trade places with
anyone else; Owning your journey.
PRIDE
……..and the process continues
TOOLS/TECHNIQUES FOR THE THERAPIST
6/19/2017
19
THE TECHNIQUES OF GAP (1)
Vision without execution is hallucination.
Thomas Edison
THE TECHNIQUES OF GAP (2)
• The Mission Statement
• The current goals
Benefits
Impediments
Strengths to overcome impediments
• Areas for change and growth
Health and fitness
Cognitive functioning
Social
THE TECHNIQUES OF GAP (3)
• Exercise Cards
• Create Your Proactive Positive Explosion Form
• Type P Personality Development Form
• DEFAULTS ARE ACTIVE
• The What-Went-Well (or 3 Good Things or 3 Blessings) Exercise
• The Gratitude Visit or Letter
• The 21 day rule for positive behavior change
• The 20 second rule
• The Reverse 20 second rule
• The Modified Presidential Campaign Assessment
SOME POSITIVE NEUROPLASTICITY EXERCISES
MINDFULNESS
• Mindfulness training helps client de-centralize from negative cognitions and experience themselves in the moment to moment process more (Germer, 2005)
• MBSR as an intervention associated with reduced impact of stress, higher quality of life and increased sense of vitality (Nyklicek and Kuijpers, 2008)
• Even when people are in high stress conditions, mindfulness practice is associated with lower levels of negative cognitive and emotional effects (Jha, et al., 2010)
• “The greater sense of autonomy arising from mindfulness practice comes not from a need to control thoughts, sensations, and emotions, but rather from the experience of not having to be controlled by them” (Kostanski & Hassed, 2008, p. 16)
THERAPEUTIC CONSIDERATIONS
• The therapist as a role model
• Phone calls
• No shows
• Suicidal ideation or threats
• Patient sabotage
• Session intensity
6/19/2017
20
HOW DO YOU KNOW WHEN YOU ARE DONE?
• Does the person conform to the mission statement?
• How well does s/he meet the criteria for Type P Personality?
• Has the personal tipping point (Proactive Positive Explosion) been achieved?
• Has a maintenance program been put in place?
• Are conditions right for continued flourishing?
WHY DOESN’T IT WORK FOR EVERYONE?
• Nothing does.
• Expectancy of therapy as a place to wallow may not be met.
• Using the gym as a model, it is notable that people who drop out may successfully return in the future.
• Intensity and/or homework turn some people off.
• It’s still a work in progress without a lot of external input.
CHALLENGES IN WORKING WITH DIFFERENT GROUPS
• Assessing readiness for change• The Habits Lab, UMBC (Substance Abuse): http://habitslab.umbc.edu/processes-of-change-questionnaire/
• Pain Stage of Change Questionnaire
• Health Net Assessing Readiness for Healthy Change Questionnaire: https://www.hnfs.com/content/hnfs/home/tn/bene/wellness/wellness_programs/online-programs/AYR4HClanding.html
• Building a multi-modal/multidisciplinary care team
• Preparation phase• Values exploration
• Meaningfulness AND confidence
• Motivational interviewing techniques• Discrepancies
• Visualization
• Pros versus cons of change
THE OVERARCHING CHALLENGE: RAMPANT DYSPHORIA
• The incidence of depression has risen every year since the early 20th
century.
• Depression is the leading cause of disability in the U.S. for individuals
between the ages of 15-44.
• The average age of initial diagnosis is getting younger.
• Depression is the most costly disease in he world although up to half of the cases that meet the criteria for depression at any one time go untreated.
IT IS HARD TO BE POSITIVE AND DEPRESSED AT THE SAME TIME.
PROTECTING AGAINST THERAPIST BURNOUT
• Key indicators of burnout include: (the shadow side of resilience)
• Emotional exhaustion
• Depersonalization & decreased empathy
• Lack of personal accomplishment • http://www.headington- institute.org/Portals/32/Resources/Test_Are_you_ burnout.pdf
• Occupational conditions that typically contribute to burnout:
• Conflict between individual values and organizational goals and demands
• Lack of managerial and/or social support
• Overload of responsibility
• Role confusion
• Sense of having no control over quality or outcome of work
• Little emotional or financial reward
• Existence of inequity, lack of respect
• Consistent exposure to traumatic material • http://www.headington-institute.org/files/understanding-and-coping-with-traumatic-stress_updated-nov-2014_63458.pdf
PROTECTING AGAINST THERAPIST BURNOUT (2)
RISK FACTORS PROTECTIVE FACTORS
The nature and intensity of any traumatic events experienced in the past The nature and intensity of the traumatic or stressful events that trigger the current reactions The number of stressors experiencedThe length of exposure to stressful situations Organizational factorsHistory of previous psychiatric illness Lack of social supportPronounced introversionNegativity and pessimism
Social supportOptimism and healthy self-esteem SpiritualityAdaptabilityTendency to find meaningCuriosity and openness to experience Aptitude
6/19/2017
21
MINDFULNESS FOR THE THERAPIST
• Randomized, double-blind control study comparing group of therapy students trained in Zen meditation + regular clinical training and group of therapist trainees provided traditional training only (Grepmair, et al., 2007)
• Patients of the therapists practicing meditation showed significantly greater improvement in sx
• Training therapists in mindfulness increases acceptance and equanimity for the therapist (Aggs & Bambling, 2010)
• Mindfulness significant contributor to counselor self-efficacy including ability to maintain attention within the counseling session and promotion of deeper/more effective empathic responses within the counseling relationship (Greason & Cashwell, 2009)
• It is important that counselors wishing to offer mindfulness as a therapeutic approach be well versed in the nuances of mindfulness through their own self-practice ( Khong, 2009)
EXERCISE, SOCIAL CONNECTIONS, AND INTELLECTUAL ACTIVITIES FOR THERAPISTS
• What do you do…?
PROMOTION OF POSITIVE GROWTH FOR ALL AND ON THAT NOTE…..
Do you know what my favorite part of the game is?
The opportunity to play. (Mike Singletary)
REFERENCES
• Posted on www.thementalhealthgym.com
For more information on this initiative, please visit the registration desk or contact PPA at (717) 232-3817.