Embed Size (px)
Citation preview
Presenter: Shoujun Li, Kai Ma
Department of Pediatric Cardiac Surgery,Fuwai hospital & National Center for Cardiovascular Disease,
PUMC&CAMS, Beijing, China
Neo-aortic Valve Regurgitation after Arterial Switch: Ten Years
Outcomes from A Single Center
Disclosure
No relationship to disclose
Background
Arterial switch operation ( ASO)
The procedure of choice:
Ventriculoarterial discordance
Favorable outcomes acquired
Less coronary lesion, Low mortality…
Pulmonary valve Neo-aortic valve
Long-term neoaortic regurgitaiton (NAR) ?Circulation 2004, 110:II-128-II-132
J Am Coll Cardiol 2006;47:2057– 62
Background
Different histological nature between pulmonary and
aortic root
Unfavorable neo-aortic root geometry
• Suture placement
• AO:PA diameter discrepancy
• Previous pulmonary banding
Mechanism of NAR
J Thorac Cardiovasc Surg. 2003 Oct;126(4):1053-60.
Ann Thorac Surg 2008;85:823–30.
Aims
To report the results of NAR after ASO for TGA & CTGA
incidence?
risk factors?
To determine the role of neo-aortic sino-tubular junction
reconstruction (NSJR)
2003-2013 , 614 consecutive pts
Groups: TGA group, n=583
CTGA group, n=31
All pts underwent ASO
(as part of double switch in CTGA)
Methods
Methods
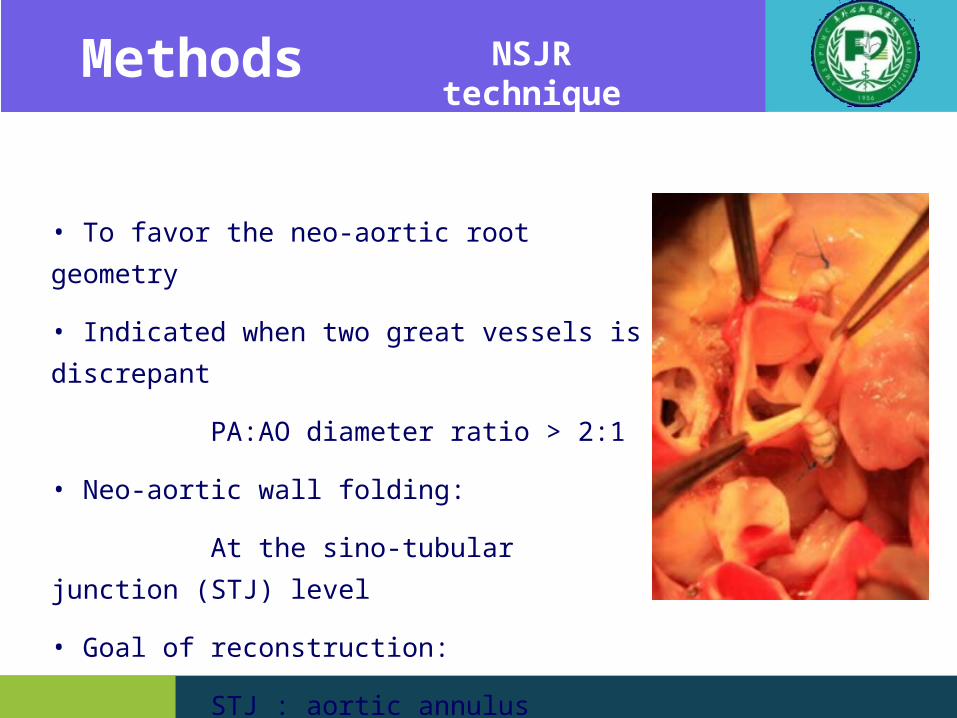
• To favor the neo-aortic root geometry
• Indicated when two great vessels is discrepant
PA:AO diameter ratio > 2:1
• Neo-aortic wall folding:
At the sino-tubular junction (STJ) level
• Goal of reconstruction:
STJ : aortic annulus diameter ratio < 0.8
NSJR technique
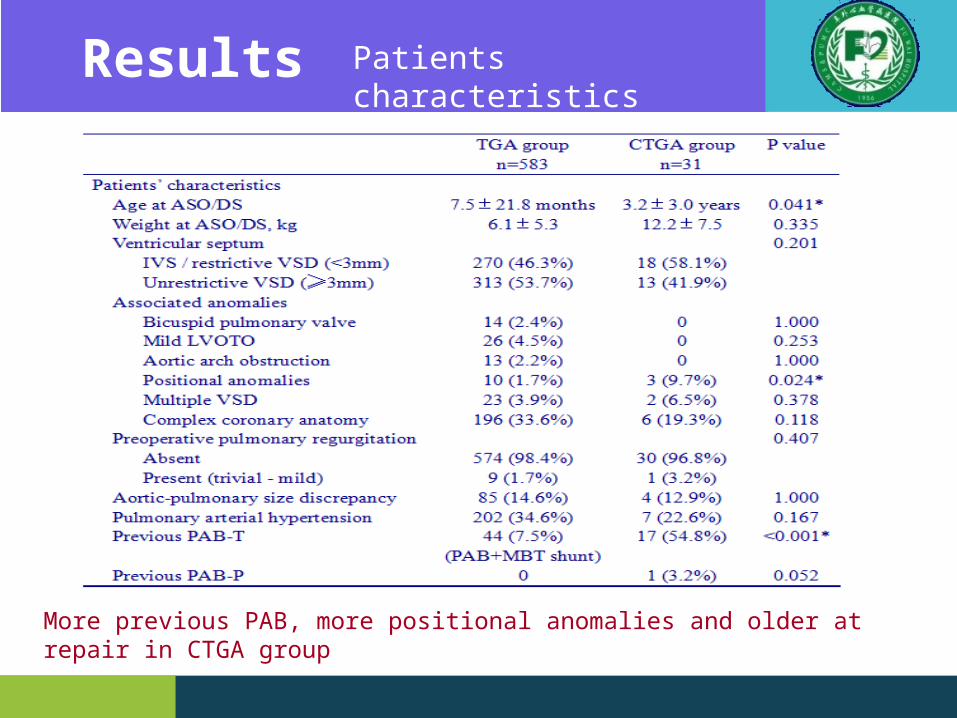
Results Patients characteristics
More previous PAB, more positional anomalies and older at repair in CTGA group
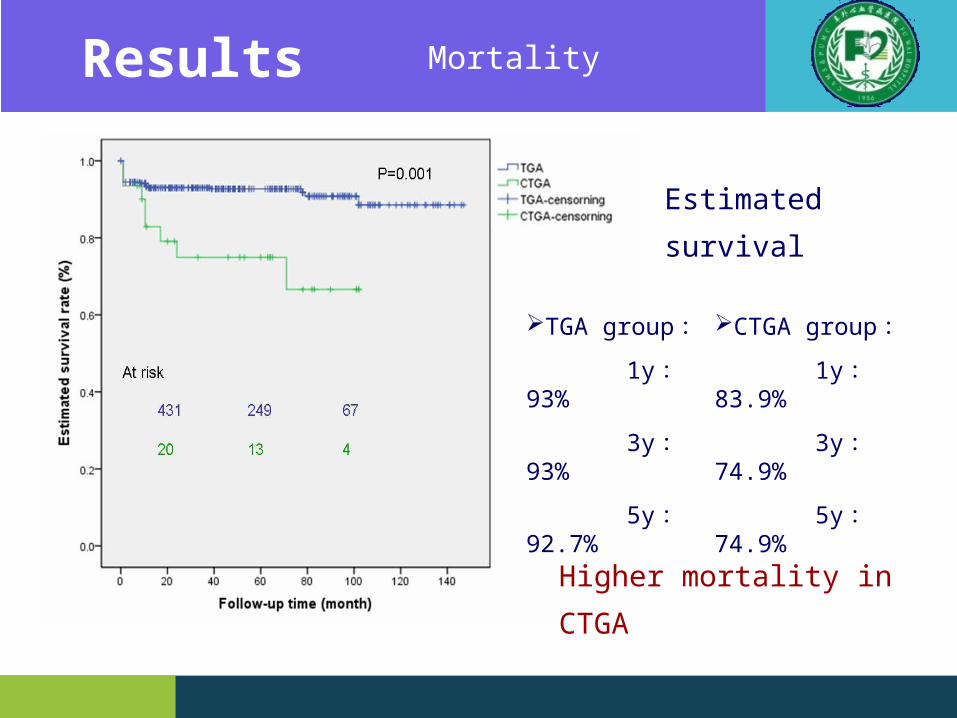
Estimated survival
TGA group:
1y : 93%
3y : 93%
5y : 92.7%
CTGA group:
1y : 83.9%
3y : 74.9%
5y : 74.9%
Higher mortality in CTGA
Results Mortality
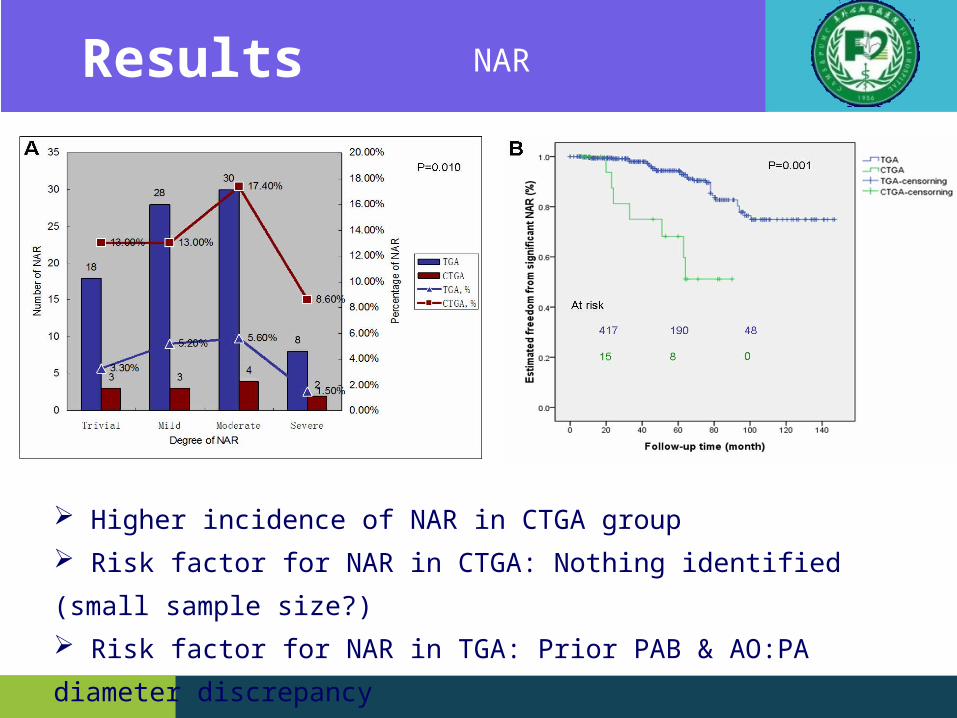
Higher incidence of NAR in CTGA group
Risk factor for NAR in CTGA: Nothing identified (small sample size?)
Risk factor for NAR in TGA: Prior PAB & AO:PA diameter discrepancy
Results NAR
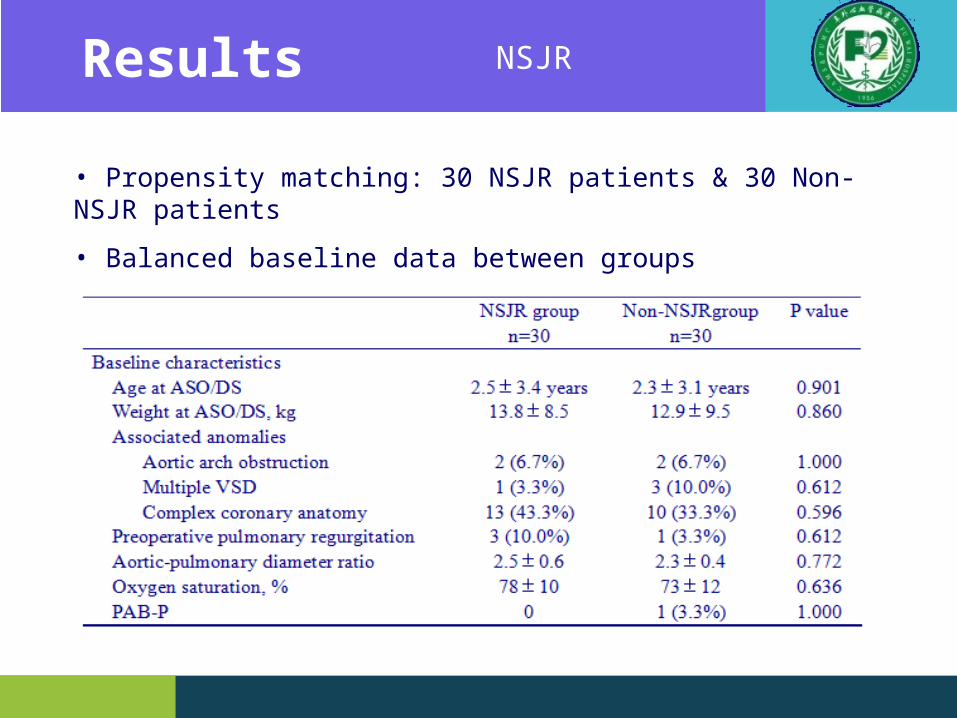
• Propensity matching: 30 NSJR patients & 30 Non-NSJR patients
• Balanced baseline data between groups
Results NSJR
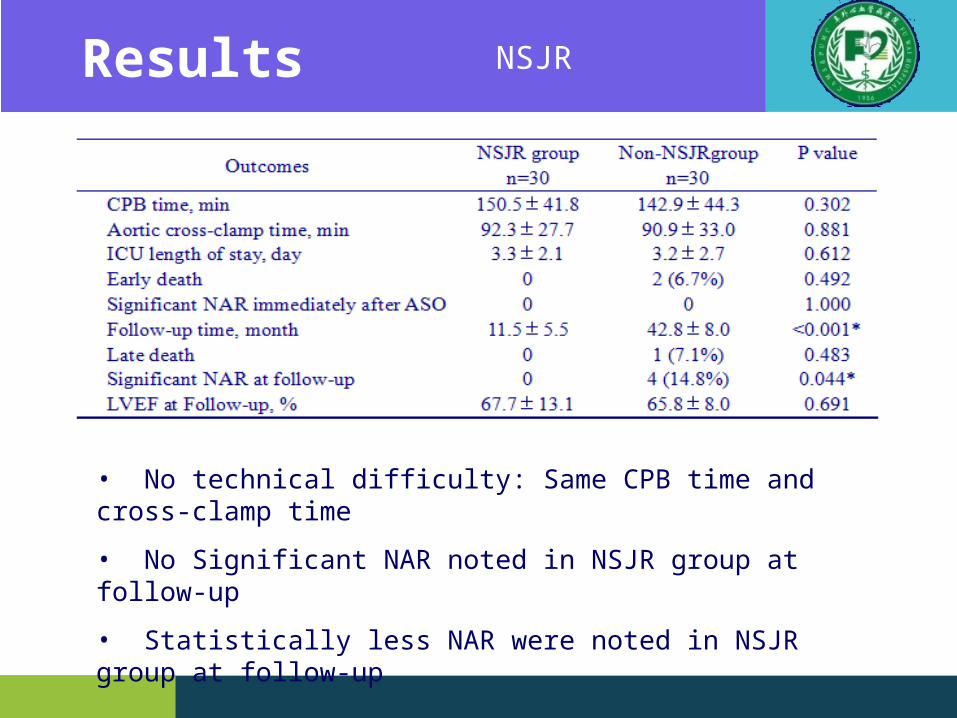
• No technical difficulty: Same CPB time and cross-clamp time
• No Significant NAR noted in NSJR group at follow-up
• Statistically less NAR were noted in NSJR group at follow-up
Results NSJR
5 reoperations (3 TGA & 2 CTGA)
2 CTGA pts all underwent prior PAB
All valve replaced, no valvuloplasty
(for enlarged annlus and unfavorable anatomy)
Time duration from ASO to reoperation :50.1±19.5 m
Optimal result achieved
No death and no valvular dysfunction noted at follow-up
Results Neo-aortic reoperation
Conclusion
ASO for TGA: optimal outcomes (less NAR, less reoperation)
DS for CTGA: higher mortality, more NAR
May related to the diagnosis itself
Significant NAR may associated with prior PAB & AO:PA discrepancy
Patients with AO:PA discrepancy may benefit from NSJR
Aortic replacement is effective as neo-aortic reoperation






























