Embed Size (px)
Citation preview

Imaging of genetic diseases.
Dr/ ABD ALLAH NAZEER. MD.

Genetic diseases
Classification:• 4 groups of genetic diseases
• 1. Disorders with multifactorial inheritance (polygenic).
• 2. Monogenic (Mendelian) disorders.• 3. Chromosomal aberrations. • 4. Environmental
(Drugs, infections).

1. Disorders with multifactorial inheritance (polygenic).
• Influence of multiple genes + environmental factors• relatively frequent• Diabetes mellitus.• Hypertension.• Gout.• Schizophrenia (Psychiatry)• Congenital heart disease - certain forms.• Some types of cancer (ovarian, breast, colon). • Often familial occurrence - probability of disease is in 1st
degree relatives about 5-10%; 2nd degree relatives - 0,5-1%.

2. Monogenic (Mendelian) disordersMutation of 1 gene, Mendelian type of inheritancetoday about 5000 diseases Autosomal dominant.Autosomal recessive.X-linked.
Autosomal dominant disorders.
Both homozygote's and heterozygote's are affectedusually heterozygote's (inherited from one parent)both males and females are affected transmission from one generation to the other 50% of children are affected.

Mutations.
A mutation may be defined as a permanent change in the DNA. Mutations
that affect the germ cells are transputted to the progeny and may give rise
to inherited diseases. Mutations thar aries in somatic cells are important in
the genesis of cancers and some congeital malformations.
Mutations may be classified into three catagories:
Genome mutations – involve loss or gain of whole chromosomes (giving rise to monosomy or trisomy).
Chromosome mutations – result from rearrangement of genetic material and give rise to visible structural changes in the chromosome.
Gene mutations – may result in partial or complete deletion of a gene or, more often, affect a single base. For example, a single nucleotide base may be substituted by a different base, resulting in a point mutation.

Autosomal dominant disorders (neurofibromatosis, tuberous sclerosis, polycystic kidney disease, familiar polyposis coli, hereditary spherocytosis, Marfan syndrome, osteogenesis imperfecta, achondroplasia, familiar hypercholesterolemia).
Autosomal recessive disorders (cystic fibrosis, phenylketonuria, homocystinuria, hemochromatosis, sickle cell anemia, thalassemias, alkaptonuria, neurogenic muscular atrophies).X-linked disorders (glucose-6-phosphate dehydrogenase deficiency), Hemophilia A (defect of Factor VIII), Hemophilia B (defect of Factor IX).
Biochemical and molecular basis of single-gene disorders.
1) Enzyme defects and their consequences.
2) Defects in receptors and transport systems.
3) Alterations in structure, function or quantity of nonenzyme proteins.
4) Genetically determined adverse reactions to drugs.

Disorders associated with defects in structural proteins.
Marfan syndrome: A disorder of the connective tissues of the body, manifested principally by changes in the skeleton, eyes, and cardiovascular system.
Ehlers-Danlos syndromes: A clinically and genetically heterogeneous group of disorders that result from some defect in collagen synthesis or structure (other disorders resulting from mutations affecting collagen synthesis include osteogenesis imperfecta, Alport syndrome, epidermolysis bullosa)
Disorders associated with defects in receptor proteins.
Familiar hypercholesterolemiaA disease that is the consequence of a mutation in the gene encoding the receptor for low-density lipoprotein (LDL), which is involved in the transport and metabolism cholesterol. More than 150 mutations, including insertions, deletions, and missense and nonsense mutations, involving the LDL receptor gene have been identified. These can be classified into five groups: Class I mutations - uncommon, they lead to a complete failure of synthesis of the receptor protein. Class II mutations - common, they encode receptor proteins that accumulate in the endoplasmic reticulum because they cannot be transported to the Golgi complex. Class III mutations - affect the LDL-binding domain of the receptor. Class IV mutations - encode proteins that are synthesized and transported to the cell surface efficiently, they bind LDH normally, but the bound LDL is not internalized. Class V mutations - encode proteins that are expressed on the cell surface, can bind LDL, and can be internalized, however, the acid-dependent dissociation of the receptor and the bound LDL fails to occur.

Disorders associated with defects in enzymes.
Lysosomal storage diseases: Lysosomes contain different types of hydrolytic enzymes, which can cleave various substrates in the acid milieu and can be secreted. With an inherited deficiency of a functional lysosomal enzyme, catabolism of its substrate remains incomplete, leading to the accumulation of the partially degraded insoluble metabolite within the lysosomes. These organells become large and numerous giving rise to the lysosomal storage disorders. These disorders result exclusively from mutations that lead to reduced synthesis of lysosomal emzymes There are also other defects: Synthesis of a catalytically inactive proteins that cross-react immunologically with normal enzymes, so the enzyme level appear to be normal.,.defects in post-translational processing of enzymes (example is a failure of mannose-6-phosphate receptor), lack of an enzyme activator or protector protein, lack of a substrate activator protein, lack of transport protein. The lysosomal storage disorders can be divided into (1) glycogenoses, (2) sphingolipidoses (lipidoses), (3) mucopolysaccharidoses, and (4) mucolipidoses. Examples follow:

Disorders associated with defects in enzymes.
Tay-Sachs disease – GM2 gangliosidosis, hexosaminidase -subunit deficiency,GM2 ganglioside accumulates in heart, liver, spleen etc., destruction of neurons, proliferation of microglia and accumulation of lipids in phagocytes within the brain.Niemann-Pick disease – types A and B, two related disorders with lysosomal accumulation of sphingomyelin, deficiency of sphingomyelinase, 80% of all cases repreents type A – the severe infantile form with neurologic involvement, visceral accumulation of sphingomyelin and early death within the first 3 years of life.Gaucher disease – a cluster of autosomal recessive disorders resulting from mutations in the gene encoding glucocerebrosidase, the most common lysosomal storage disorder, accumulation of glucocerebrosides, types I-III, the glucocere¨brosides accumulate within phygocytes (Gaucher cells) throughout the body – spleen, liver, bone marrow, lymph nodes, tonsils thymus etc.

Disorders associated with defects in enzymes.
Mucopolysaccharidoses (MPS) – the deficiencies of lysosomal enzymes involved in the degradation of mucoplysaccharides (glycosaminoglycans), several clinical variants classified from MPS I (Hurler syndrome) to MPS VII, each resulting from the deficiency of one specific enzyme, all the MPS except one are autosomal recessive disorders, the exception (Hynter syndrome) is an X-linked recessive disorder, involvement of multiple organs including liver, spleen, heart, blood vessels, joint stiffness, mental retardation.
Glycogen storage diseases – resulting from a hereditary deficiency of one of the enzymes involved in the synthesis or sequential degradation of glycogen, 3 forms: hepatic, myopathic, miscellaneous (deficiency of -glucosidase and lack of branching enzymes, type II – Pompe disease and type IV, death early in life.
Alkaptonuria (Ochronosis) – an autosomal recessive disorder in which the lack of homogentisic oxidase blocks the metabolism of phenylalanine-tyrosine at the level of homogentisic acid, homogentisic acid accumulates in the body, it selectively binds to collagen in connective tissues, tendons, and cartilage, these tissues have a blue-black pigmentation (ochronosis) most evident in the ears, nose, and cheeks, the deposits of the pigment in the articular cartilages cause the cartilage to lose its normal structure and function resulting in osteoarthritis.

Disorders associated with defects in proteins that regulate cell growth
Neurofibromatosis: types 1 and 2 – two autosomal dominant disorders, neurofibromatosis type 1 previously called von Recklinghausen disease, neurofibromatosis type 2 previously called acoustic neurofibromatosis. Although there is some overlap in clinical features, these two entities are genetically distinct.
Neurofibromatosis-1: The neurofibromatosis 1 gene (NF-1) has been mapped to chromosome 17q11.2. It encodes a protein called neurofibromin, which down-regulates the function of the p21ras oncoprotein. NF-1 therefore belongs to the family of tumor-suppressor genes. Three major features of disorder – multiple neural tumors (neurofibromas) dispersed anywhere on or in the body, numerous pigmented skin lesions, and pigmented iris hamartomas, also called Lisch nodules. A wide range of associated abnormalities has been reported in these patients – skeletal lesions like erosive defects, scoliosis, intraosseous cystic lesions, subperiosteal bone cysts, pseudoarthrosis of the tibia. Patients have also a twofold to fourfold greater risk of developing other tumors (Wilm´s tumor, rhabdomyosarkoma, meningioma, optic glioma, pheochromocytoma, chronic myeloid leukemia). There is also tendency for reduced intelligence. Whem neurofibromas arise within gastrointestinal tract, intestinal obstruction or bleeding may occur. A frequency about 1 in 3000.

Neurofibromatosis-2: an autosomal dominant disorder in which patients develop a range of tumors – bilateral acoustic schwannomas, multiple meningiomas, gliomas, ependymomas of the spinal cord, and/or non-neoplastic lesions – nodular ingrowth of Schwann´s cells into the spinal cors, meningiomatosis, glial hamartia. Pigmented (café au lait) spots like NF-1 are present, but Lisch nodules are not found. The NF-2 gene, located on chromosome 22q12, is also a tumor-suppressor gene, the product of this gene called merlin shows structural similarity to a series of cytoskeletal proteins, but is function remains uncertain. An frequency about 1 in 45,000.

Disorders with multifactorial inheritance.Down syndrome (trisomy 21): The incidence in newborns is about 1 in 700, the most common cause is meiotic nondisjunction of genetic material, symptoms: the mental retardation (IQ of 25 to 50), 40% congenital heart malformations, atresias of esophagus and small bowel, 10-fold to 20-fold increased risk of developing acute leukemia, 100% patients after 40 years of age haveneuropathologic changes.Edwards syndrome (trisomy 18), Patau syndrome (trisomy 13): like Down sy., however, the malformations are much more severe and wide-ranging. These infants only rarely survive beyond the first year of life.DiGeorge syndrome (chromosome 22q11 deletion – a small deletion of band 11 on the long arm of chromosome 22): Thymic hypoplasia, congenital heart defects, abnormalities of the palate, facial dysmorphism, developmental delay, and variable degrees of T-cell immunodeficiency and hypocalcemia. The molecular basis of this syndrome is not known. The similar clinical and cytogenetic feature has velocardiofacial syndrome, which includes facial dysmorphism (prominet nose, retrognathia), cleft palate, cardiovascular anomalies, and learning disabilities, the immunodeficiency is less frequent.

Disorders with multifactorial inheritance.Klinefelter syndrome (2 or more X chomosomes and 1 or more Y chromosomes): male hypogonandism, eunuchoid body habitus, infertility, cryptorchidism, hypospadias, skeletal changes.
XYY syndrome: Individuals are excessively tall, may be susceptible to severe acne, the intelligence is in the normal range, only 1-2% of individuals exhibit deviant behavior.
Turner syndrome (complete or partial monosomy of the X chromosome): hypogonandism with female phenotype, short body, webbing of neck, heart anomalies, infertility, amenorrhea, pigmented nevi, peripheral lymphedema at birth.
Single-gene disorders with nonclassic inheritance.
Diseases caused by triplet-repeat mutations (fragile X chromosome syndrome): The mutation which is characterized by a long repeating sequence of three nucleotides CGG. It is the second most common genetic cause of mental retardation after Down sy. The affected males are mentally retarded (IQ 20-60) with a long face and large mandibule, large everted ears, and large testicles (macro-orchidism). 50% of affected females have mental retardation.Diseases caused by mutations in mitochondrial genes (leber hereditary optic neuropathy)Diseases associated with genomic imprinting (Prader-Willi syndrome)Diseases associated with gonadal mosaicism (germ line mosaicism, gonadal mosaicism)

Short metacarpals in Turner syndrome

Most common disorders.P – Point mutation, or any insertion/deletion entirely inside one geneD – Deletion of a gene or genes.C – Whole chromosome extra, missing, or both. T – Trinucleotide repeat disorders: gene is extended in length.

Genetic diseases of the CNS.Several diseases that directly affect the CNS have a genetic component: some due to a mutation in a in a single gene, other are proving to have a more complex mode of inheritance. As our understanding of the pathogenesis of neurodegenerative disorders deepens, common themes begin to emerge: Alzheimer brain plaques and the inclusion bodies found in Parkinson disease contain at least one common component, while Huntington disease, fragile X syndrome and spinocerebellar atrophy all are dynamic mutation diseases in which there is an expansion of a DNA repeat sequence. Apoptosis is emerging as of the molecular mechanism invoked in several neurodegenerative diseases , as are other, specific , intracellular signaling events. The biosynthesis of myelin and the regulation of cholesterol traffic also figure in Charcot-Marie-Tooth and Neiman-Pick disease respectively.

Diseases:Adrenoleukodystrophy. Parkinson disease.Alzheimer disease. Phenylketonuria. Amyotrophic lateral sclerosis. Prader-Willi syndrome.Angelman syndrome. Refsum disease.Ataxia telangiectasia. Rett syndrome.Charcot-Marie-Tooth syndrome. Spinal muscular atrophy.Cockayne syndrome. Spinocerebellar ataxia.Deafness. Tangier disease.Duchenne muscular dystrophy. Tay-Sachs disease.Epilepsy. Tuberous sclerosis.Essential tremor. Von Hippel-Lindau syndrome.Fragile X syndrome. Williams syndrome.Friedreich's ataxia Wilson's disease.Gaucher disease Zellweger syndrome.Huntington disease.Lesh-Nyhan syndrome.Maple syrup urine disease.Menkes syndrome.Myotonic dystrophy.Narcolepsy.Neurofibromatosis.Niemann-Pick disease.


































BackgroundRecent developments in genetics have significantly improved our understanding of the role of genetic mutations in certain diseases where there is a familial component. Genetic testing is offered for a number of mutations such as Von-Hippel Lindau (VHL), familial paraganglioma-pheochromocytoma, multiple endocrine neoplasia (MEN) and Birt-Hogg-Dube. In these individuals, malignancy tends to present at an earlier age in subsequent generations and often with multi-organ disease. Imaging can play an important role in surveillance of a these patients and allow earlier detection and treatment of malignancy as part of a multi-disciplinary approach. Multi-organ malignancy often develops at an earlier stage in those with familial cancer syndromes.Targeted imaging has an important role in these patients for surveillance and therefore can affect further management.Imaging plays a vital role in the early diagnosis of these diseases to improve outcome.
Imaging of genetic genitourinary disease.

Hereditary Renal Cell CarcinomaThe number of conditions known to cause hereditary renal cell carcinoma is increasing. 4% of renal cancers are familial in origin. They cause multiple bilateral tumours and occur at a earlier age than non-hereditary tumours. The more common syndromes are Von Hippel Lindau (VHL), hereditary papillary renal carcinoma and Birt-Hogg-Dube.Imaging plays an important role in the management of these tumours through early detection. VHL provides a paradigm for illustrating how studies of a rare familial cancer syndrome can produce advances in clinical medicine and important insights into basic biological processes.

Syndrome Frequency of carcinoma (%)
Predominant cell type
Associated anomalies
Von-Hippel Lindau (VHL)
28-45 Clear cell Haemangioblastomas, retinal angiomas, pancreatic cysts and islet cell tumours, phaeochromcytomas
Tuberous Sclerosis (TS)
1-2 Clear cell CNS tubers, angiofibromas of skin, cardiac rhabdomyomas
Hereditary papillary renal ca
19 Papillary type 1 None
Hereditary Leiomyoma
Unknown Papillary type 2 Cutaneous and uterine leiomyomas
Birt-Dogg-Dube syndrome
8-15 Chromophobe Fibrofolliculomas, lung cysts, pneumothorax
Hereditary renal cell oncocytoma
Unknown Oncocytoma Renal dysfunction

Von Hippel Lindau (VHL)VHL is an autosomally dominant cancer syndrome caused by mutations in the VHL tumour suppressor gene. It is characterised by marked phenotypic variability. The typical age of onset is 2nd - 3rd decade, but can be earlier. The prevalence in the population is 1:35000-50000. Male and female predominance is equal. The commonest causes of death are neurological sequelae or renal cell carcinoma. There is a 70% life time risk of developing cancer.FeaturesMultiple hemangioblastomas of the central nervous system and retinal angiomas (usually precede RCC).Clear cell renal cell carcinoma (75% bilateral, multifocal disease)Pancreatic cysts and islet cell tumors.Pheochromocytomas (25% lifetime risk)Endolymphatic sac tumours. Recommended surveillanceYearly MRI abdomen (axial T1, T2 and post contrast axial T1).Three yearly MRI brain and spine or earlier if the patient is symptomatic.Urinary catecholamines from 6 - 7 years. Imaging with MR, MIBG or PET-CT (if positive catecholamines).Annual retinal screen.

An axial T2 image through the abdomen showing bilateral renal cysts in a patient with Von Hippel disease.

Bilateral multiple renal tumours in a patient with Von Hippel disease.

Cerebellar and spinal hemangioblastomas in Von Hippel Lindau syndrome.

Serous cystadenoma in the head of pancreas which proved cystadenoma. Islet cell tumour of pancreas
in pheochromocytoma.

Pancreatic neuroendocrine tumours are solid enhancing tumours , occurring in 8% of patient with VHL disease.

Familial LeiomyomatosisAutosomal dominant inheritance. Individuals affected show germ line mutations in the classical tumor suppressor gene encoding fumarate hydratase (FH).FeaturesMultiple cutaneous leiomyomas are uncommon and usually benign. They may cause pain and paraesthesia and can increase in size over time.Uterine leiomyomas (fibroids) are associated with infertility, pain and bleeding. They usually manifest at 20-35 years. In some patients, leiomyomas may become malignant.There is predisposition to type 2 papillary renal cell carcinoma which is very aggressive and metastases can present at early stages. Therefore, early management of renal tumours is required in these patients.Recommended surveillanceImaging from the age of 16, although patients may be screened from an earlier age in some families.Annual MRI of abdomen. Include pelvis if the patient is symptomatic although US can be performed for uterine lesions initially.If renal lesions, 6 monthly follow-up MRI is advised.

A,B & C – the cutaneous leiomyomata were confirmed histologically. There were no renal lesions in this patient.

Subtype Medullary Thyroid Carcinoma
Phaeochromocytoma
Parathyroid Disease
MEN 2A 95% 50% 20%-30%
FMTC 100% 0% 0%
MEN 2B 100% 50% Uncommon
The types of MEN 2 syndrome and the frequency of each type of condition.

Familial Pheochromocytoma-Paraganglioma syndrome.Pheochromocytomas occur in MEN 2A and 2B, neurofibromatosis (von Recklinghausen disease), and VHL disease. In the familial pheochromocytoma-paraganglioma syndrome, the abnormality is on the SDH (succinate dehydrogenize) gene. There are B, C and D subunit mutations with the most severely affected individuals being the B mutation. B mutation cause a higher risk of developing paragangliomas and renal cell carcinoma. B and D mutations tend to cause extra-adrenal disease.FeaturesPheochromocytomas - avid enhancement on T1W and high signal on T2W. Washout from pheochromocytomas may be variable depending on the composition (can include fat). Metastases and extra-adrenal lesions are detected on MIBG.Paragangliomas - undergo hemorrhage, cystic degeneration and are hypervascular. Have a typical ‘salt and pepper’ appearance on MR due to slow flow or hemorrhage and signal voids. They occur in:-Carotid body, Jugular foramen, Middle ear, Aorto-pulmonary window, Posterior mediastinum and Para aortic region/retroperitoneumRecommended surveillanceAnnual MRI abdomen from age 7 (RCC and pheochromocytoma).Urinary catecholamines and metabolites. Can be imaged with CT/MR.Extra-adrenal lesions detected with MIBG/PET-CT.Three yearly MRI neck and thorax (paraganglioma). Axial T1 and T2 including fat saturation with gadolinium if needed.

Right jugular foramen lesion in keeping with a glomus jugulare.
CT scan of the temporal bones showing a glomus tympanicum

A carotid body tumour on angiography. It is an extremely vascular tumour which can metastasize.

Birt-Hogg-Dube (BHD) syndromeIs named after three Canadian physicians. BHD has an autosomal dominant inheritance caused by a FLCN (folliculin) gene mutation. The differential diagnosis includes tuberous sclerosis (TS). TS has CNS lesions, different cutaneous features, leiomyomatosis and angiomyolipomas.FeaturesFibro-folliculomas - skin lesions (hair follicular tumours), trichodiscomas (early fibrofolliculomas), and acrochordons (skin tags).Renal cell carcinoma of varying histological types, most commonly Chromophobe type.Pulmonary cysts, recurrent spontaneous pneumothoraces and bullous emphysema. Other differentials are lympangioleiomyomatosis, Langerhans cell histiocytosis and pneumocystis and lymphocytic interstitial pneumonia.Recommended surveillanceSolid enhancing renal tumours - are distinguished from cysts on post-gadolinium sequences.CT thorax for well-circumscribed cysts in the lower lobe

Axial CT thorax image showing lung cysts in a patient with a patient with Birt-Hogg-Dube (BHD) syndrome.

An enhancing left renal lesion with mixed signal on T2W and solid appearances of renal cell carcinoma in a patient with BHD.

Multiple Endocrine Neoplasia type 2 (MEN 2)There are 3 categories of MEN 2 (table 2):-MEN type 2AMEN type 2B (includes ganglioneuromatosis and marfanoid features)Familial medullary thyroid carcinoma (FMTC)All patients are at risk of medullary thyroid carcinoma with differing ages of onset (MEN 2B - early childhood , FMTC - middle age, MEN 2A – early adulthood). The RET oncogene is associated with 88% of patients with familial MTC.FeaturesMedullary thyroid carcinoma arises from parafollicular cells. It nearly always spreads to lymph nodes, lung, liver. It causes elevated calcitonin levels. The tumour is low attenuation on CT (no radio-iodine uptake).Surveillance ProtocolProphylactic thyroidectomy by 5-10 years in FMTC depending on mutation. Annual calcitonin stimulation test thereafter. Parathyroid and calcium levels (parathyroid adenomas). Urinary catecholamines and metabolites (pheochromocytoma). MRI abdomen if positive catecholamines or features of pheochromocytoma and MIBG or PET-CT (extra-adrenal disease).

A large heterogeneous nodule in the left thyroid lobe, secondary to a medullary thyroid carcinoma in a patient with MEN 2 disease.

Multiple calcified liver metastases and a left renal calculus in a patient with MEN 2 syndrome.

Neurofibromatosis Type 2Neurofibromatosis type 2 is an autosomal dominant neurocutaneous condition which is compromised of vestibular schwannomas, spinal tumours, meningiomas and retinal hamartomas.FeaturesSchwannomas – symptoms include hearing loss, tinnitus and loss of balance. Bilateral tumours often occur and age of onset is 30 years.Meningiomas – 50% of patients develop meningiomas. They are usually intracranial but can be spinal. Other neural axis tumours include gliomas and ependymomas.Hamartomas – retinal hamartomas and cataracts can cause decreased visual acuity and diplopia.Recommended SurveillanceAnnual MRI brain and spine from 10-12 years. Imaging until the fourth decade of life at least.Hearing evaluation for detecting acoustic schwannomas before presentation on imaging.If known to have vestibular schwannomas, followed -up with MR IAMS/brain and ENT clinic.Regular ocular screening for retinal lesions.

There are multiple meningiomata in this patient with NF2.

Pre, post-contrast T1 and dedicated IAM sequences of bilateral acoustic neuroma of NF2.

Tuberous sclerosis (TS)A neuroectodermal disorder characterised by hamartomas of the skin, brain and viscera (heart, lung, kidney). Prevalence is 1:10000. Clinically patients have adenoma sebaceum, epilepsy and mental retardation.FeaturesHamartomas – occur on subependymal surface of caudate lobe, foramen of Munro (foM) protruding into the ventricles.Astrocytoma – in region of foM, uniform enhancement and extension into ventricle. Low signal on T1W and high on T2W. May cause hydrocephalus.Cortical or subcortical tubers – are multiple in 75%. They are hyperintense lesions on T2W.Angiomyolipomas – usually bilateral and multiple. The hallmark is fat content and hypervascularity on angiography. They can lead to hemorrhage but have very low malignant potential.Recommended surveillanceNo recommended protocol in our trust.Angiomyolipomas are at risk of bleeding if more than 4cm and can followed up 6-monthly with MR or yearly if less than 4cm.Large lesions can be treated with embolisation.

Pre and post contrast MR showing subependymal lesions and a mass in the right anterior lateral ventricle, proved giant astrocytoma in tuberous sclerosis.

Bilateral fat containing lesions in both kidneys with typical features for angiomyolipoma in a patient with MS.

Genetic diseases of the musculoskeletal system. There are a number of diseases that are caused by defects in gene important for the formation and functions of muscles, and connective tissues. Defects in fibrillin - a connective proteins that is important in making tissue strong yet flexible cause Marfan syndrome, while diastrophic dysplasia is caused by a defect in a sulfate transporter found in cartilage.Diseases:Achondroplasia, Amyotrophic lateral sclerosis, Charcot-marie-tooth syndrome, Diastrophic dysplasia, Duchene muscular dystrophy, Ellis-van Creveld syndrome, Fibrodysplasia ossificans progressiva, Marfan syndrome and Myotonic dystrophy.

Marfan Disease.

Annuloaortic ectasia of Marfan Disease, Reformatted CT images shows marked dilatation of the Valsalva sinus and the sinotubular junction.

Marfan syndrome with aortic dissection and background severe pectus excavatum

Marfan syndrome. A. CT demonstration of the left undescended testis, high scrotal in position (arrow). B.CT image shows funnel chest. A 56-years-old male with Marfan syndrome. C. CT image shows the dissection of the descending aorta. D. 3D-CTA shows aneurysmal dilation of the aortic root.

Achondroplasia is a congenital genetic disorder and the most common skeletal dysplasia. It has numerous distinctive radiographic features and is the most common cause of short limb dwarfism. Radiograph / CT / MRI: Features on radiographs, CT, and MRI are similar and discussed together here. Cranial: relatively large cranial vault with small skull base, prominent forehead with depressed nasal bridge, narrowed foramen magnumcervico medullary kink, relative elevation of the brainstem resulting in a large suprasellar cistern and vertically-oriented straight sinus, communicating hydrocephalus (due to venous obstruction at sigmoid sinus).Spinal: posterior vertebral scalloping, progressive decrease in interpedicular distance in lumbar spine, gibbus: thoracolumbar kyphosis with bullet-shaped/hypoplastic vertebra (not to be confused with Hurler syndrome), short pedicle canal stenosis, laminar thickening, widening of intervertebral discs , increased angle between sacrum and lumbar spineChest: anterior flaring of ribs, anteroposterior narrowing of ribsPelvis and hips: horizontal acetabular roof (decreased acetabular angle), small squared (tombstone) iliac wings, small trident pelvis, champagne glass type pelvic inlet, short sacroiliac notchesLimbs: metaphyseal flaring 8: can give a trumpet bone type appearance, the femora and humeri are particularly shortened (rhizomelic shortening), long fibulathey may also appear thickened but in fact normal in absolute terms compared to the normal adult diameter (thickening is perceived due to reduced length), V-shaped growth platestrident hand

Achondroplasia

Amyotrophic lateral sclerosis (ALS), also known as Lou Gehrig disease or Charcot disease is the most common form of motor neuron disease , resulting in progressive weakness and eventual death. Radiographic featuresMRIThe earliest MR manifestation is hyperintensity on T2WI in the corticospinal tracts, seen earliest in the internal capsule, as the fibers are most concentrated here. Eventually the entire tract from motor strip to the spinal cord is affected with increased T2 signal and volume loss 3. Iron deposition in the cortex is demonstrated as loss of signal, most evident on T2* weighted sequences, it is seen on T2WI in 40-60% (SWI is presumably more sensitive).It is important to note that both of these features are present in varying degrees in normal control patients, and as such an appreciation of what is too much is essential if MRI is to be of benefit. MR spectroscopy:decreased NAAdecreased glutamateincreased cholineincreased myoinositol


Diastrophic dysplasia (DTD) is a type of short limb skeletal dysplasia (micromelic dwarfism). In adulthood patients have a stature between 100 and 140 cm. Radiographic features: Characterised by a micromelic dwarfism with hand deformities (abducted or hitchhiker’s thumb), multiple flexion contractures, and a scoliosis. The bones are characterised by crescent-shaped flattened epiphyses, a short, broad femoral neck, and shortening and metaphyseal widening of the tubular bones. There is irregular deformity and shortening to the metacarpal bones, metatarsal bones, and phalanges. Abduction of the great toes and clubfeet may also be observed.
Diastrophic dysplasia.

Duchenne muscular dystrophy (DMD) is a recessive X-linked form of muscular dystrophy, affecting around 1 in 3,600 males, which results in muscle degeneration and premature death. The disorder is caused by a mutation in the dystrophin gene, located on the human X chromosome, which codes for the protein dystrophin. Dystrophin is an important structural component within muscle tissue that provides structural stability to the dystroglycan complex (DGC) of the cell membrane. While both sexes can carry the mutation, females rarely exhibit signs of the disease.

Myositis ossificans progressiva (MOP), now known as Fibrodysplasia ossificans progressiva (FOP), is a rare, inherited disorder characterized by progressive fibrosis and ossification of muscles, tendons, fasciae, aponeurosis and ligaments of multiple sites that is disabling and ultimately fatal. The process of heterotopic ossification starts between 2 and 5 years old.
Myositis ossificans progressiva.

Charcot-Marie-Tooth disease (CMT) also known as Hereditary Motor and Sensory Neuropathy (HMSN), is the most commonly inherited neuropathy of lower motor (to a lesser degree sensory) neurons. The disease is divided into the following types:CMT type 1
this form of CMT disease is a disorder of peripheral myelination.repeated cycles of demyelination and remyelination result in a thick layer of abnormal myelin around the peripheral axons.these changes cause what is referred to as an onion bulb appearance.
CMT type 2this primarily is a neuronal (i.e., axonal) disorder, not a demyelinating disorder. CMT type 2 results in peripheral neuropathy through direct axonal death and Wallerian degeneration.
CMT type 3 (also known as Dejerine-Sottas disease)characterized by infantile onset, this condition results in severe demyelination with delayed motor skills; it is much more severe than type 1.
CMT X (X-linked CMT) and CMT 4: these are also demyelinating neuropathies.

Charcot-Marie-Tooth syndrome.

Myotonic dystrophy (dystrophia myotonica, myotonia atrophica) is a chronic, slowly progressing, highly variable, inherited multisystemic disease. It is an autosomal-dominant disease. It is characterized by wasting of the muscles (muscular dystrophy), cataracts, heart conduction defects, endocrine changes, and myotonia. There are two main types of myotonic dystrophy. Myotonic dystrophy type 1 (DM1), also called Steinert disease, has a severe congenital form and an adult-onset form. Myotonic dystrophy type 2 (DM2), also called proximal myotonic myopathy (PROMM) is rarer than DM1 and generally manifests with milder signs and symptoms. Myotonic dystrophy can occur in patients of any age. Both forms of the disease display an autosomal-dominant pattern of inheritance. Both "DM1" and "DM2" have adult-onset forms.
DTI IN MYOTONIC DYSTROPHY

DTI IN MYOTONIC DYSTROPHY.

X-linked deafness, also termed incomplete partition type III, is a rare genetic disorder associated with a mutation in the POU3F4 gene located on the X chromosome. Clinical presentationMale patients present with progressive mixed hearing loss. Female carriers have normal hearing or only mild hearing loss. Vestibular function is impaired in affected males, however normal in females.Radiographic featuresX-linked deafness, also termed X-linked deformity, has typical imaging findings:bilateral and symmetrical widening of the fundus of the internal auditory canal; absence of the bony partition between the fundus and the basal turn of the cochlea's. carrier females can have mild dilatation of internal auditory canal.There may also be an abnormal bony modioli, vestibular aqueducts and facial nerve canals (labyrinthine and tympanic segments).

CT show the typical findings of X-linked deafness, with bilateral absence of the bony partition between the fundus and the basal turn of the cochlea's. On the left side there is an abnormally enlarged vestibular aqueduct.

MRI show the typical findings of X-linked deafness, with bilateral absence of the bony partition between the fundus and the basal turn of the cochlea's. On
the left side there is an abnormally enlarged vestibular aqueduct.

Cystic fibrosis is a genetic disorder that affects the respiratory and digestive systems. People with cystic fibrosis inherit a defective gene on chromosome 7 called CFTR (cystic fibrosis transmembrane conductance regulator). The cells most seriously affected by this are the lung cells. This mucus clogs the airways in the lungs, and increases the risk of infection by bacteria.
Organs Affected By Cystic Fibrosis.

Cystic lung fibrosis with multiple cysts of variable size. Bottom images show the presence of renal and hepatic angiomyolipomas.

Genetic Liver DiseaseSome liver diseases are inherited, and our specialist physicians have extensive experience in diagnosing and treating these disorders. In addition, genetic counseling and screening tests are available to the families and relatives of our patients.Hereditary Haemochromatosis – Hereditary haemochromatosis is the most common adult genetic liver disease and results from excessive iron accumulation in the body, particularly in the liver. Specific and effective treatment is available, but lifelong monitoring in particularly important.Alpha-1-Antitrypsin Deficiency – This inherited liver disease may affect the liver and /or lungs of children and adults. It is caused by the inability to produce enough A1AT, a protein which protects cells from injury. Management involves education, nutrition counseling and close monitoring for any complications. Liver transplantation may be an option if the disease progresses.Wilson’s Disease – This is a rare genetic disorder that results from excessive accumulation of copper in the liver and brain. Oral medications effectively prevent copper buildup, but liver transplantation may be required in some cases. Wilson’s disease is a particular clinical and research interest of the hepatologists at the Yale School of Medicine Liver Center and the Norwalk Hospital Liver Center

Iron deposition from hemochromatosis.

Honeycomb Appearance of the Liver in Wilson's disease.

Swyer syndrome is a condition that affects sexual development. Sexual development is usually determined by an individual's chromosomes; however, in Swyer syndrome, sexual development does not match the affected individual's chromosomal makeup.People usually have 46 chromosomes in each cell. Two of the 46 chromosomes, known as X and Y, are called sex chromosomes because they help determine whether a person will develop male or female sex characteristics. Girls and women typically have two X chromosomes (46,XX karyotype), while boys and men usually have one X chromosome and one Y chromosome (46,XY karyotype). In Swyer syndrome, individuals with one X chromosome and one Y chromosome in each cell, the pattern typically found in boys and men, have female reproductive structures.People with Swyer syndrome have typical female external genitalia. The uterus and fallopian tubes are normally-formed, but the gonads (ovaries or testes) are not functional; affected individuals have undeveloped clumps of tissue called streak gonads. Because of the lack of development of the gonads, Swyer syndrome is also called 46,XY complete gonadal dysgenesis. The residual gonadal tissue often becomes cancerous, so it is usually removed surgically early in life.

MRI, rudimentary uterus (in white circle).MRI, gonadal mass within the
left pelvis (in white circle).
Swyer syndrome

Mayer-Rokitansky-Küster-Hauser (MRKH) syndrome. = a disorder that occurs in females and mainly affects the reproductive system. The cause of MRKH syndrome is unknown, although it probably results from a combination of genetic and environmental factors.●Incidence: 1/5,000●Symptoms.Primary amenorrheaCyclic abdominal pain due to cyclic endometrial shedding without a patent drainage pathwayInfertilityRenal malformations
Kallmann syndrome = a genetic disorder with the distinctive features of hyposmia or anosmia and hypogonadotropic hypogonadism●Incidence: 1/10,000-86,000 (Male> female)●Symptoms.A condition characterized by delayed or absent puberty and an impaired sense of smell.Cryptorchidism, Microphallus in males, primary amenorrhea, Bimanual synkinesis affects about one-fifth of males with the disorder

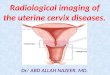
MRKH syndrome. She married nulliparous presented with complaints of primary amenorrhea. On examination, the patient’s secondary sexual characteristics were found to be normal. A.B. MRIs show the absence of uterus and vagina. C. MR axial image shows both ovaries, which appear normal.

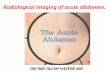
Kallman syndrome. She had delay in puberty and anosmia. A. MRI shows the incomplete aplasia of the uterus. B. Single coronal T2 image through the frontal lobes demonstrates abnormal anatomy with absence of the olfactory bulbs and olfactory sulcus. C. The normal anatomy of the region consists of the olfactory bulbs (pink arrows) located in the olfactory grooves of the anterior cranial fossa. The inferior surface of the frontal lobes usually consists gyrus rectus (straight gyrus) (R) separated from the medial orbital gyrus (M) by the olfactory sulcus (green arrow). These are absent in Kallman syndrome.

Turner syndrome is a chromosomal condition that affects development in females. The most common feature of Turner syndrome is short stature, which becomes evident by about age 5. An early loss of ovarian function (ovarian hypofunction or premature ovarian failure) is also very common. The ovaries develop normally at first, but egg cells (oocytes) usually die prematurely and most ovarian tissue degenerates before birth. Many affected girls do not undergo puberty unless they receive hormone therapy, and most are unable to conceive (infertile). A small percentage of females with Turner syndrome retain normal ovarian function through young adulthood.About 30 percent of females with Turner syndrome have extra folds of skin on the neck (webbed neck), a low hairline at the back of the neck, puffiness or swelling (lymphedema) of the hands and feet, skeletal abnormalities, or kidney problems. One third to one half of individuals with Turner syndrome are born with a heart defect, such as a narrowing of the large artery leaving the heart (coarctation of the aorta) or abnormalities of the valve that connects the aorta with the heart (the aortic valve). Complications associated with these heart defects can be life-threatening.Most girls and women with Turner syndrome have normal intelligence. Developmental delays, nonverbal learning disabilities, and behavioral problems are possible, although these characteristics vary among affected individuals.

Turner syndrome. MRIs show the incomplete aplasia of the uterus and absence of ovaries.

Hands and foot abnormalities associated with genetic diseases
Ellis-van Creveld syndrome, Fibrodysplasia ossificans progressiva , Achondroplasia, Kniest dysplasia, pseudohypoparathyroidism, Acromegaly, Nail-patella syndrome, Marfan,s syndrome, Mucopolysaccharidosis, Cartilage-hair hypoplasia.
X-ray and photograph of the hands of a child with Ellis–van Creveld syndrome. b Note the polydactyly with an extra small digit on the ulnar side. Several other digits are distorted and the third and fourth metatarsals on the right side are fused. There is also curvature of the fifth metatarsal on the left side.

Hands of a patient with fibrodysplasia ossificans progressiva. b The hands like the rest of the body may show production of new bone adjacent to the skeletal segments but there is a striking shortening and deformity of the thumbs

Hands of a child with Kniest disease. Not the long knobby fingers and the “squared off epiphyses” for the digits as well as the distal radius and ulna.

Almost all forms of the mucopolysaccharidoses show gross distortion of the hand and foot structure. a Shows a child with Hurler syndrome with hepatosplenic enlargement. Note the hand flexion deformities. As noted in the X-ray, the metacarpals and phalanges are wide and the distal radius and ulna have a V-shaped deformity. The child is severely mentally impaired. b (1) A photograph of a child with Morquio’s syndrome. She is short and grossly deformed but mentally normal. (2)Her hands and feet show gross digital distortion

The hands of children with cartilage–hair hypoplasia show skin and structural alterations consisting principally of short digits often bent. The metacarpals are short, and the carpal bone are poorly structured and calcified

Tumors.Benign vs. Malignant:Benign (hemangioma - nevus flammeus - port wine stains, lymphangioma - hygroma colli cysticum, sacrococcygeal teratoma)Malignant (hematopoietic - malignant lymphomas, leukemia's; neurogenic (Neuroblastoma, Ewing sarcoma, primitive neuroectodermal tumor - PNET, CNS-medulloblastoma), sarcomas (rhabdo-, osteosarcoma), kidneys (Wilms' tumour), thyroid (papillary ca).

Thank You.