Embed Size (px)
DESCRIPTION
Citation preview

Radiological imaging of benign breast diseases.
Dr/ ABD ALLAH NAZEER. MD.




Imaging modalities.








Benign breast diseases.














Ductal ectasia with inspissated secretion inside.







Fibroadenoma


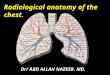
a) Raw dynamic contrast-enhanced MR image on lesion, which exhibits high signal intensity. The mass-like enhancement area is marked by purple arrow and the lesion; (b) Raw Diffusion-weighted MR image (b = 800 s/mm2); (c) Calculated ADC map from (b). Lesion area exhibits with light green (pointed in purple arrow), implying a high ADC value. ADC measured in this lesion is 1.91×10−3 s/mm2. doi:10.1371/journal.pone.0087387.g002

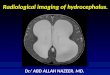
a: Dynamic contrast MR demonstrates a breast lesion with rim enhancement. b: Plateau (type 2) enhancement pattern. Signal intensity values were obtained from the area of greatest enhancement. c: Spectroscopy detected no Cho signal (SNR 1.7) at 3.2 ppm in representative spectrum and magnified (50) region in the lesion. Histological analysis of the tissue was benign breast tissue.(Fibroadenoma).

Type I enhancement curve – Fibroadenoma.


Proton MRI and MRSI in a 38-year-old patient (#7) with a fibroadenoma. a: Post-GdDTPA T1-weighted MR image. b: MRSI of water, Cho, and lipids. c: Unmagnified spectra from the lesion, demonstrating water and lipid peaks, and a weak Cho signal (SNR ! 4). d: Magnified ($50) spectrum from a voxel in the lesion demonstrating the weak Cho resonance.

A 37-year-old woman with fibroadenoma. Sagittal fat-saturated postcontrast MRI image (a) shows a well-defined mass lesion with dark internal septa, indicative of a fibroadenoma. MRS (b) shows a Cho peak at 3.28 ppm, possibly representing GPC, mI, and taurine instead of Cho and PC.



Cystosarcoma phyllodes of the breast (CSPB).




Fibrocystic disease of both breast.

Fibrocystic disease of the breast.

Fibrocystic disease of the left breast.

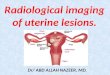
Cysts are fluid-filled, round or ovoid structures that are found in as many as one third of women between 35 and 50 years old. Although most are subclinical “microcysts,” in about 20%–25% of cases, palpable (gross) cystic change, which generally presents as a simple cyst, is encountered . Cysts cannot reliably be distinguished from solid masses by clinical breast examination or mammography; in these cases, ultrasonography and fine needle aspiration (FNA) cytology, which are highly accurate, are used. Cysts are derived from the terminal duct lobular unit. In most cysts, the epithelial lining is either flattened or totally absent. In only a small number of cysts, an apocrine epithelial lining is observed. Because gross cysts are not associated with an increased risk of carcinoma development, the current consensus on the management of gross cysts is routine follow-up of the patient, without further therapy.

Simple cyst. Nonenhancing



Idiopathic granulomatous mastitis

Bilateral Lupus Mastitis.







Epidermal inclusion cyst with smooth margins.

Breast MRI shows homogeneous enhancement of perilobular hemangioma (left), with a type 2 T-SI curve (right)



Thank You.