-
8/18/2019 Present and Future Therapies of Hepatitis B From
Discovery to Cure
1/16
REVIEW
Present and Future Therapies of Hepatitis B: From
Discovery to Cure
T. Jake Liang,1
Timothy M. Block,2
Brian J. McMahon,3
Marc G. Ghany,1
Stephan Urban,4
Ju-Tao Guo,2
Stephen Locarnini,5 Fabien Zoulim,6 Kyong-Mi Chang,7 and Anna S.
Lok 8
Hepatitis B virus (HBV) is a significant global pathogen,
infecting more than 240 mil-lion people worldwide. While treatment
for HBV has improved, HBV patients oftenrequire lifelong therapies
and cure is still a challenging goal. Recent advances in
tech-nologies and pharmaceutical sciences have heralded a new
horizon of innovative thera-peutic approaches that are bringing us
closer to the possibility of a functional cure of chronic HBV
infection. In this article, we review the current state of science
in HBV therapy and highlight new and exciting therapeutic
strategies spurred by recent scientificadvances. Some of these
therapies have already entered into clinical phase, and we will
likely see more of them moving along the development pipeline.
Conclusion: With grow-ing interest in developing and efforts
to develop more effective therapies for HBV, thechallenging goal of
a cure may be well within reach in the near future.
(HEPATOLOGY 2015;62:1893-1908)
Despite the availability of effective vaccines forthree decades
and improvement of treatment,the prevalence of chronic hepatitis B
viral
(HBV) infection worldwide has declined minimally from 4.2%
in 1990 to 3.7% in 2005.1 Moreover, the
actual number of persons who are chronically infected
isestimated to have increased slightly from 223 million to240
million during this same period. Treatment for thisinfection, while
advancing to the stage that viral replica-tion can be effectively
suppressed and disease success-fully controlled, is still
handicapped by variouslimitations and cannot be considered as
curative. Recog-nizing that HBV therapeutics is at the cusp of
innova-tions and breakthroughs, this review summarizes
new targets among the HBV viral and host immune systemsfor
which drugs are now in late preclinical developmentand clinical
testing. In addition, novel and potentially promising
therapeutic strategies that would likely result
in more durable and complete responses are highlighted.To put
these advances in the context of the current stateof the science,
we summarize the current HBV therapiesand their limitations and
spotlight the continued impactof fundamental scientific discoveries
in advancing the
research and development of new HBV therapies.
Natural History of Chronic Hepatitis B
The course of chronic HBV infection has beengrouped into four
phases: the immune tolerant phase,the immune active/hepatitis B e
antigen (HBeAg)–posi-tive chronic hepatitis phase, the
HBeAg-negative inac-tive phase, and the immune
active/HBeAg-negativechronic hepatitis phase. However, these terms
may notaccurately reflect the immunological status of patients
ineach phase but are useful for prognosis and determining need
for therapy.2,3 The duration of each phase varies
Abbreviations: anti-HBs, antibody to HBsAg; CAR, chimeric
antigen receptor; cccDNA, covalently closed circular DNA; HBeAG,
hepatitis B e antigen; HBsAg,
hepatitis B surface antigen; HBV, hepatitis B virus; IFN,
interferon; IL, interleukin; ISG, interferon-stimulated gene; NRTI,
nucleos(t)ide reverse transcriptase
inhibitor; NTCP, sodium/taurocholate cotransporter; PEG-IFN,
pegylated interferon; RNAi, RNA interference; TLR, toll-like
receptor; WHV, woodchuck hepatitis virus.
From the 1Liver Diseases Branch, National Institute
of Diabetes and Digestive and Kidney Diseases, National Institutes
of Health, Bethesda, MD; 2 Baruch S.
Blumberg Institute, Doylestown, PA; 3National Center for
Emerging and Zoonotic Infectious Diseases, Centers for Disease
Control and Prevention, Anchorage, AK;
4 Department of Infectious Diseases, Molecular Virology and
German Center for Infection Diseases, University Hospital
Heidelberg, Heidelberg, Germany;5 Hepatology Department, Lyon
University and Cancer Research Center of Lyon, INSERM U1052, Lyon,
France; 6 Victorian Infectious Diseases Reference
Labora-
tory, Doherty Institute, Melbourne, VIC, Australia;
7 Department of Medicine, Philadelphia Veterans Affairs
Medical Center and the University of PennsylvaniaPerelman School of
Medicine, Philadelphia, PA; 8 Division of
Gastroenterology and Hepatology, University of Michigan, Ann Arbor,
MI.
Received March 29, 2015; accepted July 31, 2015.
1893
-
8/18/2019 Present and Future Therapies of Hepatitis B From
Discovery to Cure
2/16
from months to decades. Transition can occur from anearlier to a
later phase, but regression back to an earlierphase can also
occur.4 It should be noted that not allpatients go through all four
phases. Furthermore, whilethe cutoff levels of alanine
aminotransferase used todefine different phases were traditionally
based on upperlimits of normal determined by clinical diagnostic
labo-ratories, recent studies suggest that the true normal val-ues
are lower.5
HBV Replication: From Basic Science toDrug Development
Advances in understanding the molecular biology
andreplication cycle of HBV have provided unprecedentedinsight into
the mechanisms of action and treatmentresponse of currently
available drugs against HBV as
well as potential future targets for therapeutic
develop-ment (Fig. 1). HBV gains entry into hepatocytes
initially through a low-affinity interaction between heparan
sul-fate proteoglycans on the hepatocytes involving the anti-genic
loop (“a” determinant or antibody neutralizationdomain) of the HBV
envelope proteins6,7 and then a high-affinity interaction of
the myristoylated pre-S1domain with the liver-specific receptor
sodium/tauro-cholate cotransporter (NTCP).8 NTCP is
exclusively expressed on the basolateral/sinusoidal membrane
of hepatocytes. Its natural function is to transport
conju-gated bile salts (e.g., taurocholate) into hepatocytes as
part of the enterohepatic pathway.9 Accordingly, NTCPplays
a key role in the liver tropism of HBV.10,11 NTCPis also crucial
for the host specificity of HBV. Two shortsequence motifs within
NTCP are sufficient to renderthe respective proteins from
cynomolgus monkey andmouse functioning as an HBV receptor.12,13
Additionalhost factors are probably required for efficient
HBV entry. Fusion of HBV particles and release of
nucleocap-sids into the cells involves
receptor-mediatedendocytosis.14,15
The HBV genome–containing nucleocapsid is trans-
ported into the nucleus through a yet-undefined path-
way, probably involving microtubule and nuclearimportin
machinery.16 In the nucleus, the relaxed circu-lar, partially
double-stranded genome is then repaired toa full-length, circular
DNA by covalently attached viralpolymerase (P) and other
incompletely understood
mechanisms probably involving tyrosyl DNA phospho-diesterase of
the topoisomerase and DNA repair path- way.17 The circularized
protein-free genome thencomplexes with host histone and nonhistone
proteinsincluding various histone-modifying enzymes into
a minichromosome that functions as the template
fortranscription.18 Its transcriptional activity is regulatedby
epigenetic modifications and specific host transcrip-tional
factors, such as hepatocyte nuclear factor 4.19
HBV core and X proteins are also present on the mini-chromosome
and probably play an important role inHBV transcription.18,20,21
The covalently closed circular
DNA (cccDNA) is transcribed to three classes of HBV RNAs:
genome-length RNAs (pregenomic and precoreRNAs coding for core gene
products and P protein), SRNAs (S proteins), and X RNA (HBx
protein). Thepregenomic RNA transcript is reverse-transcribed by
theP protein to relaxed circular DNA in the core-containing
nucleocapsid. The nucleocapsid can eitherassemble into an
infectious virion with the envelopeproteins through the
multivesicular body pathway 22 orrecycle back to the nucleus
for cccDNA amplification ina process probably controlled by the
pre-S1 envelope
protein and other host factors.
23
The steady-state popu-lation of cccDNA is about one to 10
molecules perinfected hepatocyte.24
Current Therapies of Hepatitis B andMechanisms of Action
There are currently two classes of drugs approved forthe
treatment of hepatitis B: nucleos(t)ide reverse tran-scriptase
inhibitors (NRTIs) and interferon-a (IFN-a).The first-line
antiviral HBV medications include a nucleoside analogue,
entecavir; a nucleotide analogue,
tenofovir; and pegylated IFN-a (PEG-IFN-a), used as
Address reprint requests to: T. Jake Liang, LDB/NIDDK/NIH,
Bldg. 10-9B16, 10 Center Drive, Bethesda, MD 20892-1800. E-mail:
[email protected]; tel:
11-301-496-1721. fax: 11-301-402-0491.
Copyright VC 2015 by the American Association for the
Study of Liver Diseases. This article has been contributed to by
U.S. Government employees and their work is in the public
domain in the U.S.A.
View this article online at wileyonlinelibrary.com.
DOI 10.1002/hep.28025 Potential conflict of interest: Dr.
Guo received grants from Janssen. Dr. Block is on the Board of and
owns stock in Contravir. He received grants and holds
intellectual property rights with Oncore-Tekmira. Dr. Lok
consults and received grants from Gilead. She consults from
GlaxoSmithKline, Merck, MYR, and
Tekmira. She received grants from Bristol-Myers Squibb. Dr.
Chang advises Genentech, Arbutus, and Alnylam. Dr. Zoulim consults
and received grants fromRoche, Gilead, and Novira. He consults for
Janssen. Dr. Locarnini received royalties and holds intellectual
property rights with Melbourne Health. He consults and
received fees from Arrowhead. He consults for Gilead.
1894 LIANG ET AL. HEPATOLOGY, December 2015
-
8/18/2019 Present and Future Therapies of Hepatitis B From
Discovery to Cure
3/16
monotherapy.25-27 PEG-IFN is administered for 48-52 weeks.
While it has a weaker antiviral activity thanNRTIs, it is
associated with a higher rate of HBeAg andhepatitis B surface
antigen (HBsAg) loss, possibly through a combination of direct
antiviral and immuno-modulatory effects. By contrast, NRTIs target
only thereverse-transcription of pregenomic RNA to HBV DNA and
have no direct effect on cccDNA. Long-term treat-ment with more
potent NRTIs can lead to progressive
loss of HBeAg and HBsAg with time.IFN-a, as a front-line host
defense against viral infec-
tions, is known to induce IFN-stimulated genes
(ISGs), which have promiscuous antiviral functions against
a variety of viruses. Depending on the viruses, these ISGsplay
a diverse and pleiotropic role in targeting variousviral functions
at different steps of the viral replicationcycle and potently
suppress viral infection and spread.IFN-a has a direct
anti-HBV effect and acts on multiplesteps of the HBV replication
cycle (Fig. 1).28,29 In addi-tion, it has an immunomodulatory
effect that can indi-
rectly inhibit HBV replication by affecting
cell-mediatedimmunity in vivo.30 Studies of the HBV
kinetics inIFN-a-treated patients suggest a more relevant role
of the latter mechanism in mediating IFN-a’s
anti-HBV effects.31
Despite targeting multiple steps of HBV replication,the
molecular mechanisms underlying IFN-a’s actionremain to be fully
defined. IFN-a is thought to inducespecific ISGs that
inhibit HBV transcription or prevent
the formation of nucleocapsid or target it for
degrada-tion.28,29,32 The responsible ISGs have not been
clearly defined. IFN-a’s effect on HBV transcription is
partly mediated by epigenetic modifications of the
cccDNA minichromosome.33 Recent development of infectiousHBV
cell culture systems provided the much neededtools and models to
study the effects of antivirals,including IFN, on HBV
replication.33,34 A recent study demonstrated that
IFN-a and another putative antiviralcytokine, lymphotoxin-b,
induce the degradation of cccDNA in infectious cell culture
systems.35 This effect
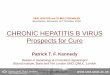
Fig. 1. HBV life cycle and targets of therapeutic development.
The complete HBV life cycle including entry, trafficking, cccDNA
formation, tran-
scription, encapsidation, replication, assembly, and secretion
is shown. The functions of the HBV gene products are incorporated
into the life
cycle. Drugs or biologics, in clinical use or development,
targeting various steps of the HBV life cycle, are illustrated in
red. See text for detailsof these drugs. Abbreviations: ER,
endoplasmic reticulum; HSPG, heparan sulfate proteoglycan; siRNA,
small interfering RNA.
HEPATOLOGY, Vol. 62, No. 6, 2015 LIANG ET AL. 1895
-
8/18/2019 Present and Future Therapies of Hepatitis B From
Discovery to Cure
4/16
is mediated by induction of the APOBEC3 family of proteins,
specifically APOBEC3A by IFN-a and APO-BEC3B by
lymphotoxin-b; APOBEC3 functions torestrict foreign DNAs, such as
those from invading microbial genomes, which activate the IFN
response
including induction of APOBEC3s as ISGs.
36
The APOBEC3s are DNA editing enzymes and deaminateforeign
double-stranded DNA cytidines to uridines.36
This conversion can lead to either C to T mutations
ordegradation of foreign DNA. In contrast, cellulargenomic DNA is
unaffected. APOBEC3s are known totarget human immunodeficiency
virus, adeno-associatedvirus, and possibly other DNA viral genomes
for degra-dation.36 For HBV, the role of APOBEC3 has been
con-troversial. APOBEC3G was shown to inhibit HBV replication
in cell culture, but the mechanism had beenattributed to either
direct inhibition of HBV replication
or hypermutations from DNA editing.37-40 All of theearlier
studies were performed in HBV DNA transfec-tion systems that could
not be used to investigatecccDNA. In an HBV infectious culture
system, theinduced APOBEC3 interacted with the core proteinand
translocated to the nucleus to target cccDNA.35
The development of nucleoside analogues owes muchof its success
to the comprehensive understanding of how HBV replicates.
Based on the model of HBV repli-cation, the P protein has been the
primary therapeutictarget in HBV drug development (Fig. 1). While
this
advance represents a pivotal step in the chronicle of HBV
treatment, knowledge of the mechanism of actionof this class of
anti-HBV drugs also exposes its limita-tion, as discussed
above.
While the second-generation NRTIs, such as enteca-vir and
tenofovir, can potently suppress the DNA syn-thesis step of HBV
replication, they have little effect onthe level and activity of
cccDNA, which has a long half-life and can persist for decades in
the infected liverdespite successful antiviral treatment.24 This
limitationexplains the necessity for a prolonged, possibly
indefi-nite, treatment with this class of anti-HBV drugs. The
turnover of cccDNA has been the subject of intenseresearch
because of its fundamental importance in HBV replication and
therapy. Several mechanisms appear toexplain the turnover of
cccDNA in vivo. First, the directcytopathic effect of
activated HBV-specific T lympho-cytes can cause death of infected
cells. Second, gradualloss of the cccDNA pool by cell proliferation
in injuredliver can account partly for gradual loss of
cccDNA.Finally, a noncytopathic mechanism of
eliminating cccDNA from infected cells contributes to the
turnoverof cccDNA.41 IFNs and other cytokines have been
implicated in this “cell cure” mechanism, but the
precisemechanism is unknown.41
Entecavir and tenofovir can decrease the level of HBV DNA
by 6 logs within 1 year of treatment andhave low rates of antiviral
drug resistance (0%-1% after
5 years of continued treatment).
42-44
However, rates of HBeAg seroconversion (20% after 1 year
and 40%-50% after 5 years) and HBsAg loss (5%-10% after 5years) are
low. Therefore, most patients require many years and often
lifelong treatment with associated costsand risks of adverse
reactions, drug resistance, and non-adherence.45 Despite these
limitations, antiviral treat-ment can reverse liver fibrosis and
even cirrhosis,prevent cirrhosis complications, and reduce, though
noteliminate, the risk of hepatocellular carcinoma.44,46
Derivatives of tenofovir as prodrugs with
improvedpharmacological properties are being developed and
may be of benefit in certain situation.47For patients who do not
have cirrhosis or do not
require immunosuppressive therapy, professional
society guidelines recommend treating those in the
immuneactive phase,25-27 although treatment at an earlier stagehas
been proposed to minimize unrecognized yet signifi-cant liver
damage.48 However, treatment during theimmune tolerant phase is
associated with a low rate of HBeAg seroconversion and failure
to completely sup-press HBV DNA to nondetectable levels.49
The ultimate goal of antiviral therapy would be to
eliminate all forms of potentially replicating HBV, butthis may
not be feasible because even in persons whorecover from acute HBV
infection with HBsAg to anti-body to HBsAg (anti-HBs)
seroconversion, HBV per-sists in the liver in the form of cccDNA
and can bereactivated during immunosuppressive therapy. A
morerealistic goal is a “functional cure” in which HBV DNA is
not detectable after the completion of a finite courseof treatment
with loss of HBsAg and minimization of hepatocellular
carcinoma risk over time. To accomplishthis goal, a combination of
antiviral drugs that targetdifferent steps in the HBV life cycle or
immunomodula-
tory therapies to restore host immune response to
HBV will be needed.
Combination Studies of Current Therapies
Given that only two classes of anti-HBV agents arecurrently
available, combination therapy consist of twoNRTIs or an NRTI plus
PEG-IFN. In the latter case, anNRTI and PEG-IFN may be combined
simultaneously,sequentially, starting with either drug first, or as
an add-on strategy with either drug first.
1896 LIANG ET AL. HEPATOLOGY, December 2015
-
8/18/2019 Present and Future Therapies of Hepatitis B From
Discovery to Cure
5/16
Initially, the clinical need to increase the potency
of first-generation antivirals and to prevent emergence
of antiviral resistance was the primary reason to test
combi-nation therapy with NRTIs. Unfortunately, thisapproach
suffered from the fact that all NRTIs have thesame virological
target, the HBV polymerase. Thus, thetreatment response observed in
patients was similar tothat of the most potent agent in the
combination. Theissue of antiviral resistance is now greatly
diminished
with the development of second-generation NRTIs,such as
entecavir and tenofovir. The efficacy and safety of entecavir
and tenofovir combination therapy werecompared to entecavir
monotherapy in previously untreated HBV patients.50 A
greater proportion of sub-
jects receiving combination therapy achieved viral
sup-pression compared to entecavir alone, but the difference
was not statistically significant.50 However, HBeAg-
positive subjects with baseline HBV DNA 108
IU/mLreceiving combination therapy had a significantly
higherrate of virological response compared to those
receiving monotherapy.50
Conceptually, combination of PEG-IFN with anNRTI would be more
likely to result in synergy becausethe drugs have different
mechanisms of action, the con-cept being that inhibition of viral
replication with anNRTI may augment the immune effects of
PEG-IFN.Unfortunately, while studies of PEG-IFN in combina-tion
with first-generation NRTIs did show synergy inachieving viral
suppression and reducing the incidence
of antiviral resistance, off-treatment responses were simi-lar
to that of PEG-IFN alone.51,52 The availability of more
potent, second-line NRTIs together with a renewed interest in
achieving HBsAg clearance hasstimulated interest in combining these
agents togetheror in combination with PEG-IFN.
Simultaneous PEG-IFN and tenofovir was evaluatedin
treatment-naive patients with HBeAg-positive andHBeAg-negative
chronic hepatitis B.43 Patients receiving PEG-IFN and
tenofovir had a higher rate of HBsAg lossthan those receiving
either drug along.43 Although theseresults are encouraging,
they represent a small increase
(6%) in HBsAg loss over PEG-IFN monotherapy, and a benefit
was mainly observed in those with genotype A infection.
Sequential therapy beginning either with an NRTIfollowed by
PEG-IFN or vice versa for variable dura-tions has been conducted in
both HBeAg-positive andHBeAg-negative subjects. In general, these
studies havenot demonstrated a substantial benefit in terms of
eitheron-treatment or sustained off-treatment HBV
DNA suppression or HBeAg and HBsAg loss compared toPEG-IFN as
a historical control.53-55
Starting with NRTI first and adding PEG-IFN later would
seem to be the most logical approach to combi-nation therapy. The
idea is that the NRTI would rapidly lower viral load and
restore T-cell responsiveness, thenadding PEG-IFN might hasten the
decline of circulating
and intrahepatic viral antigens leading to an improve-ment in
the innate immune response.56 Several recentstudies seem to support
such an approach.57-59 Among HBeAg-positive subjects,
higher rates of HBeAg sero-conversion were achieved with add-on
combinationtherapy of PEG-IFN and NRTI (27%) compared toNRTI only
(0%).58 Among HBeAg-negative subjects,HBsAg loss was reported
in 6.6% of subjects at the endof therapy in the combination arm
versus 1% in theNRTI-only arm.59 None of these studies included
anarm using PEG-IFN monotherapy, and when comparedto historical
studies of PEG-IFN monotherapy, the
results obtained with combination therapy arecomparable.
A recent study compared PEG-IFN alone to PEG-IFN followed
by add-on entecavir or entecavir followedby add-on PEG-IFN.60 Rates
of HBeAg seroconversionposttreatment were similar across treatment
groups.60
With an add-on strategy, a longer duration of NRTIbefore
add-on PEG-IFN and a longer duration of PEG-IFN therapy was
associated with higher rates of HBeAg and HBsAg loss.
In summary, there are insufficient data at present torecommend
the use of combination therapy except in
very special circumstances, such as in subjects with
very high baseline viral levels (>108 IU/mL) or for
manage-ment of subjects who have failed a first-line agent due toa
suboptimal response or the development of
multidrug resistance. Further studies are needed to address
the ben-efit of various formats of combination therapy withPEG-IFN
and more potent NRTIs.
HBV Entry Inhibitors
Entry inhibitors have been used successfully in treat-ing viral
infections. In particular, small molecules and
antibody-based treatments are quite effective in
treating acute viral infections.61 For chronic viral infection
likehuman immunodeficiency virus, entry inhibitors havealso been
successfully developed.62 For HBV, entry inhibitors can be
applied in two ways. The first is in a preventive setting:
entry inhibition, such as using anti-HBs antibodies, blocks
de novo HBV infection. Thisapplication has been successfully
demonstrated in ani-mal models63 and is clinically a standard of
care using HBsAg-specific immunoglobulins to prevent
reinfectionafter liver transplantation, to avoid vertical
transmission
HEPATOLOGY, Vol. 62, No. 6, 2015 LIANG ET AL. 1897
-
8/18/2019 Present and Future Therapies of Hepatitis B From
Discovery to Cure
6/16
of HBV from infected mothers to children, and forpostexposure
prophylaxis.64 Regarding chronic hepatitisB patients, whether entry
inhibition would be a viabletherapeutic option is debatable. It is
conceivable thatpotent blockade of HBV reinfection in
chronically infected patients can reduce viral load due to the
turn-over of HBV-infected hepatocytes.65 Previous studiessuggested
that hepatocyte turnover is indeed much fasterin HBV-infected liver
than in healthy hepatocytesbecause of immune-mediated
cytotoxicity.66 A sustainedinhibition of de novo
formation of cccDNA in hepato-cytes may contribute to the
eventual clearance of thevirus with prolonged therapy, especially
if it is used incombination with other potent anti-HBV
drugs.Because hepatitis D virus shares the same entry
pathway,another potential application of entry inhibitors is
inHBV/hepatitis D virus coinfection.
HBV entry depends in part on the pre-S1 sequence,more
specifically the myristoylated N terminus of thelarge envelope
protein. Both the myristoylation and theN-terminal 75 amino acids
are required for infectivity of HBV.67,68 It was shown that
synthetic lipopeptidesrepresenting this subdomain potently inhibit
HBV infection. The mode of action of such peptidic inhibi-tors
(Myrcludex B, for example) can be attributed tospecific receptor
binding.11 Myrcludex B successfully passed phase 1 clinical
trials.69 Moreover, because thenatural role of NTCP as a bile salt
transporter has beenstudied in some detail, molecules already known
to bind
or inhibit the function of NTCP have been tested.Cyclosporin A
and its derivatives (e.g., alisporivir) orapproved drugs like
ezetimibe are among those thathave been demonstrated to inhibit HBV
entry.70-72
Myrcludex B, cyclosporin A, and other substrate ana-logues
inhibit bile salt transport by NTCP. Accordingly,these molecules
may elevate bile salts and other trans-ported substrates in the
serum of patients. This concernmay be a clinically manageable
problem. First, people withpolymorphisms in NTCP resulting in a
functional knock-down show very moderate clinical symptoms and do
notdevelop any specific pathology.73 Second, NTCP knock-
out mice are viable and show elevated conjugated bile saltlevels
without symptoms but have a slight retardation ingrowth during
development.74 Most importantly, the anti-viral effect of Myrcludex
B and cyclosporin A is already apparent at a much lower
concentration than that requiredfor inhibiting bile acid transport
(>100-fold differ-ence).12,71 Thus, entry inhibition should be
clinically achievable without significant interference with
the trans-porter function of the receptor.
Myrcludex B is currently being tested in two
ongoing clinical trials.75 Preliminary results suggested that
Myr-
cludex B is safe and well tolerated in HBsAg-positivepatients
with or without HDV coinfection. A decline inthe HBV DNA level
(>1 log 10) was reported in 87% of patients at 12
weeks of treatment (10 mg/day), and thedecline continued with
extended treatment beyond 12
weeks. Myrcludex B treatment at high doses was associ-ated
with some bile acid elevation.
HBV Capsid Inhibitors
Several classes of inhibitors of pregenomic RNA pack-aging and
HBV capsid assembly have been identified.They function to
dysregulate or selectively inhibit eitherpregenomic RNA
encapsidation or nucleocapsid assem-bly or both. The first of these
were the phenylpropena-mide derivatives AT-61 and AT-130.76
Thesecompounds selectively inhibit viral pregenomic RNA
packaging
77
and are active against both wild-type andlamivudine-resistant
HBV.78,79 As a class and at themolecular level, these agents
have been shown to inducetertiary and quaternary structural changes
in HBV cap-sids. AT-130 binds to a promiscuous pocket at the
coredimer–dimer interface.80 This binding decreases viralproduction
by initiating virion assembly prematurely inthe replication cycle,
resulting in morphologically nor-mal capsids that are empty and
noninfectious.77
The second group of inhibitors is the
heteroaryldihy-dropyrimidines, which inhibit HBV virion
productionin vitro and in vivo by preventing
capsid formation.81
The best studied of the heteroaryldihydropyrimidines,Bay
41-4109, has a dual mechanism of action by inhibi-ting
encapsidation directly and causing a concomitantreduction in the
half-life of the core protein. Structuralstudies of this class of
inhibitors revealed that they induce inappropriate capsid
assembly at low concentra-tions and, when in excess, promote a
misdirected assem-bly reaction and decreased capsid stability.82,83
Like thephenylpropenamides, the heteroaryldihydropyrimidinesare
active against NRTI-resistant strains of HBV.79
Other inhibitors targeting the nucleocapsid are being
developed by several biotech companies (Tables 1).
84
Invitro studies have demonstrated strong synergy
whenthese inhibitors are used in combination with
currently approved NRTIs.78,79
Inhibition of HBV Gene Expression
Persistence of HBV results from an ineffective antivi-ral immune
response against the virus, and one of the
ways HBV orchestrates this is through excess productionof
subviral particles containing HBsAg. These noninfec-tious subviral
particles may act as a decoy for the
1898 LIANG ET AL. HEPATOLOGY, December 2015
-
8/18/2019 Present and Future Therapies of Hepatitis B From
Discovery to Cure
7/16
immune system,85 especially for mopping up
potentially neutralizing anti-HBs. High levels of HBsAg, in
therange of 400 lg/mL (0.4% of total serum protein),
arecommonly found in the blood of patients with chronichepatitis
B86 and may interfere with HBV-specificimmune responses.87,88
A molecular approach to inhibit HBV gene expres-sion has
been successfully achieved in vitro
using molecule-based therapies targeting the viral
messengerRNA. Viral messenger RNA can be directly targetedusing
antisense oligonucleotides, ribozymes, or RNA interference
(RNAi).89 Of these, RNAi appears most
Table 1. Experimental HBV Therapeutics in Late Preclinical
or Clinical Stage*
Compound Mechanism/ Target†
Stage of Development Sponsor Reference
Direct-acting antivirals:
GS-7340 (tenofovir
alafenamide fumarate
Polymerase (prodrug of
tenofovir)
Phase 2/3 Gilead Sciences 47; NCT0194047;
NCT01940341‡
CMX157 Polymerase (prodrug of
tenofovir)
Phase 1/2§
Contravir (Chime rix) 14 6; NCT01080820‡
NVR1221/3778 Capsid Phase 1/2 Novira 84; NCT02112799‡
Sulfamoylbenzamides Capsid Animal Oncore 147
GLS4 Capsid Phase 1 HEC Pharm Group, China 148
Bay41-4109 Capsid Phase 1 AiCuris 83
REP 2139-Ca Assembly/HBsAg Phase 1/2 Replicor NCT02233075‡
ARC-520 RNAi Phase 1/2 Arrowhead 94; sponsor’s website;
NCT02065336‡
TKM-HBV RNAi Phase 1 Tekmira Sponsor’s website;
NCT02041715‡
ALN-HBV RNAi Animal Alnylam Sponsor’s website
DNA-directed RNAi RNAi Animal Benitec Sponsor’s website
ISIS HBV Antisense Phase 1 Isis Sponsor’s website
Host targeting agents:
Myrcludex B Entry/NTCP Phase 1/2 Myr-GmbH/Hepatera 75
Birinapant Apoptosis/second
mitochondrial activator of caspases
Phase 1 Tetralogic Sponsor’s website; NCT02288208‡
Flavonoids STING agonist (pattern
recognition receptor)
Animal Oncore 149
NVP018 Cyclophilins, IRF-9 Animal Oncore (NeuroVive) Sponsor’s
website
Epitope HBV Glucosidase/therapeutic
vaccine
Animal Blumberg Institute 150
Immune modulatory agents:
GS-9620 TLR-7 agonist Phase 2 Gilead Sciences 122;
NCT02166047‡
Nivolumab PD-1 blockade Phase 1||
BMS 151; Sponsor’s website,
NCT01658878‡
SB 9200HBV RIG-I and NOD2 activation Phase 1/2 INC/Springbank
152; NCT01803308‡
GS-4774 Therapeutic vaccine Phase 2/3 Gilead
Sciences/GlobeImmune 144; NCT02174276‡
ANRS HB02 Therapeutic vaccine Phase 1/2 French National Agency
for
Research on AIDS and Viral
Hepatitis
141; NCT02166047‡
Heplisav B Dynavax 601 Therapeutic vaccine Phase 1 Dynavax 153;
NCT01023230‡
Nasvac Therapeutic vaccine Phase 2/3 CGEB, Cuba 154
TG1050 Therapeutic vaccine Phase 1/1b Transgene
NCT02428400
HBIG1GM-CSF 1HBV vaccine Therapeutic vaccine Phase 1/2
Beijing 302 Hospital NCT01878565
HBV vaccine1 IFN-a2b1 IL-2 Therapeutic vaccine Phase 2/3 Tongji
Hospital NCT02360592 (labeled as Phase 4)
HBV vaccine–activated dendritic
cells
Therapeutic vaccine Phase 1/2 Third Affiliated Hospital,
Sun
Yat-Sen University
NCT01935635
Euvax 1 PEG-IFN-a Therapeutic vaccine P hase 2/3
Seoul National University N CT0 2097004 ( labeled as Phas e 4)
PD-1 monoclonal antibody PD1 blockade Animal AcadSin 155
Altravax HBV Therapeutic vaccine Animal Altravax Sponsor’s
website
INO-1800 Therapeutic vaccine Animal Innovio Sponsor’s
website
*Compounds are organized by names and targets with developmental
phase based on authors’ estimates derived from the literature where
available or the spon-
sor’s website and presentation information.†
Mechanisms are characterized as either direct acting antiviral,
indicating action against a virus-specified gene product; immune
modulatory agent, activating
host immune response; or host targeting agent, which targets a
host function required for the HBV replication cycle.‡
Identifier for Clinicaltrials.gov.§
In phase 2 for human immunodeficiency virus.k Trial i
ndication is for treatment of HBV-associated hepatocellular
carcinoma.
Abbreviations: GM-CSF, granulocyte-macrophage colony-stimulating
factor; HBIG, hepatitis B immune globulin.
HEPATOLOGY, Vol. 62, No. 6, 2015 LIANG ET AL. 1899
-
8/18/2019 Present and Future Therapies of Hepatitis B From
Discovery to Cure
8/16
promising because efficient in vivo delivery systems
havebeen developed by a number of biotech companies(Table 1).
RNAi is a process by which small interfering RNA molecules
of 21-25 nucleotides induce gene silencing at
the posttranscriptional level to effectively knock downthe
expression of the gene(s) of interest. Such shortinterfering RNA
can lead to transcriptional silencing ortranslational repression.90
These processes are critical incell growth regulation and tissue
differentiation andinvolve the Drosha and Dicer enzyme complexes,
theRNA-induced silencing complex, and the nuclease
Argo.90 The extensive use of overlapping RNAs andopen
reading frames within the HBV genome makes foran attractive target
for inhibition by RNAi.91 Both cellculture and mouse model studies
have shown thatRNAi, delivered as an expression plasmid, is able
to
inhibit all steps of HBV replication.92
In transgenicmice, RNAi expression has been shown to
significantly reduce the secretion of HBsAg in serum, reduce
bothHBV messenger RNAs and genomic DNA in the liver,and eliminate
hepatocytes stained positive for core anti-gen.93 These mouse
studies have been extended to a chronically infected
chimpanzee.94 Currently, a phase 2placebo-controlled
dose-escalation study with the DPC-NAG-ARC-520 formulation has been
initiated inHBeAg-negative chronic hepatitis B whose viremia
wascontrolled by entecavir and showed a 50% drop inHBsAg levels in
treated compared to placebo patients.95
Another RNAi platform has demonstrated similarsuccess in
its preclinical evaluation with a 2.3-log 10reduction in HBsAg
in chronically HBV-infected chim-panzees (Alnylam’s company press
release).96 OtherRNAi-based regimens are currently being developed
andtested (Table 1).
Inhibitors of HBV cccDNA Formation andStability
Because the cytoplasmic nucleocapsid DNA is theprecursor for
cccDNA biosynthesis, complete inhibition
of viral DNA replication in the nucleocapsids with poly-merase
inhibitors should preclude de novo cccDNA for-mation.
However, clinical studies demonstrated thatalthough NRTI
monotherapy for 48-52 weeks reducedcirculating viremia
by 5 log 10 and cytoplasmic HBV DNA
levels in hepatocytes by approximately 2 log 10,reduction of
cccDNA was much less pronounced, only by 0.11 to 1.0
log 10.
24,97 Moreover, sequential analysesof viral DNA replicative
intermediates and core antigen-positive hepatocytes in the livers
of woodchuck hepatitisvirus (WHV)-infected woodchucks before and
during
clevudine (an NRTI) therapy revealed that after morethan 6 weeks
of therapy, all WHV DNA replicativeintermediates were markedly
reduced, with the excep-tion of cccDNA, which remained as the
predominantviral DNA species in the liver.98
Concerning the failure of prolonged NRTI therapy toeradicate
cccDNA, one possibility is that the currently available NRTIs
do not completely inhibit viral DNA synthesis in every
infected hepatocyte in vivo, allowing for continuous
replenishment of the cccDNA poolthrough the intracellular
amplification pathway. NRTIsare prodrugs requiring activation by
host cellularnucleoside kinases, the expression and function of
whichmay be heterogeneous in the liver. Therefore, hepato-cytes may
have varying abilities to activate the NRTIs,resulting in
incomplete inhibition of HBV DNA repli-cation. Emergence of
drug-resistance mutations during
apparently effective NRTI therapy suggests that residualHBV
replication and de novo cccDNA synthesis stilloccur
at a low level.99
Alternatively, failure to eradicate cccDNA by pro-longed
NRTI therapy may also be due to the extraordi-nary stability of
cccDNA.100 cccDNA may persist in a “latent” state amid the
host chromosomes and remain asa reservoir for later HBV
replication. Healthy hepato-cytes in the absence of immune response
or inflamma-tory reaction have a half-life of over 6
months.101,102
What we have learned from NRTI therapy is thateradication
of cccDNA is essential for the cure of
chronic hepatitis B. Combination therapies with NRTIsand one or
multiple novel antiviral drugs targeting dif-ferent steps of HBV
replication may completely inhibitHBV DNA replication and thus
accelerate the reductionof cccDNA. The other approach would be to
directly purge the preexisting cccDNA or permanently
silencecccDNA transcription.
A recent strategy to cleave cccDNA molecules orinhibit
their transcription by generating cccDNA sequence-specific
endonucleases with zinc-finger nucle-ase, transcription
activator-like effector nuclease, orCRISPR/cas9 technology has been
tested in cell cultures
and a mouse model103,104; but efficient and targeteddelivery of
these antiviral genes to all HBV-infected cellsin vivo is a
major challenge for clinical application.
Another approach is to target the other enzymatic
func-tion of HBV polymerase, RNaseH, which is requiredfor HBV
replication and cccDNA formation. Recentstudies have identified
potential inhibitors of HBV RNaseH.105
Further understanding the molecular mechanism of cccDNA
metabolism and functional regulation is essen-tial for identifying
and validating molecular targets for
1900 LIANG ET AL. HEPATOLOGY, December 2015
-
8/18/2019 Present and Future Therapies of Hepatitis B From
Discovery to Cure
9/16
rational development of antiviral drugs to eradicate
ortranscriptionally silence cccDNA. As discussed above,recent
studies on the molecular mechanism of immunecontrol of HBV
infection by IFN-a demonstrated thatcccDNA can be
specifically targeted for degradation by
a cytidine-deamination mechanism
35
and its transcrip-tion can be silenced by epigenetic
modification.33,106
These findings raise a potentially exciting possibility
of targeting cccDNA through pharmacological activationor
augmentation of the host intrinsic antiviral pathways.Moreover,
investigation into the role and mechanism of HBx and core
protein in cccDNA metabolism and func-tion may reveal virus–host
interactions for selectiveelimination or silencing of cccDNA.20
Additional efforts have been made to
discovercccDNA-targeting compounds through
high-throughputcell-based phenotypic screening. This unbiased
approach,
while attractive, is currently hampered by a lack of
effi-cient HBV infection cell culture systems and convenientassays
for high-throughput quantification of HBV replica-tion and cccDNA
quantification. Disubstituted sulfona-mides were identified as
cccDNA formation inhibitors ina screen of 85,000 small molecular
compounds.107 Therecent rapid progress in the establishment of an
efficientHBV infection cell culture system may ultimately
allow the development of cell-based assays for
high-throughputscreening of cccDNA-targeting antivirals.
Immune Mechanisms of HBV Control and
Implications for Therapy
The pathogenesis of chronic HBV infection involvesnot only viral
mechanisms by which HBV establishes a persistent infection but
also the host responses to infec-tion. The latter includes the
response of hepatocytes toHBV infection as well as the interplay of
the virus andinfected cells with the other parenchymal and
nonpar-enchymal cells in the liver, i.e., Kupffer cells,
endothe-lial cells, fibroblasts, and nonresident immune cellsthat
are recruited to the site of infection. HBV hasevolved mechanisms
to counteract and escape these dif-
ferent host responses to establish a chronic infection.Recent
studies point out a critical role of the livermicroenvironment in
the elimination or control of HBV (Fig. 2). 108,109
While much has been learnedabout the HBV-specific adaptive
immunity, the early and innate immune response during acute
HBV infec-tion remains largely unknown. In addition, few
studieshave examined intrahepatic immune responses inpatients with
chronic HBV infection. Available data suggest impaired
responses, but the mechanism of thisimpairment is unclear.109
In chronic hepatitis B, the antiviral B- and T-cellresponses are
quantitatively and/or qualitatively defec-tive. For example,
anti-HBs is generally undetectable inthe setting of excess
circulating HBsAg. Furthermore,antiviral T cells show impaired
antiviral effector func-tion in vitro. However, this host
immune response,despite being dysfunctional, exerts at least
partial viralcontrol in vivo because immune
suppression withimmunosuppressive therapies results in increased
vire-mia.58,110 HBV persistence with antiviral immune dys-function
is also associated with the induction of immune inhibitory
pathways including PD-1, CTLA-4,Bim, arginase, and FoxP31
regulatory T cells.111-116
These pathways, likely induced in response to
continuedinflammation, viral replication, and antigen
expression,can dampen both cytopathic inflammatory responses as
well as noncytopathic antiviral effector functions.
Thus,
the antiviral effector T-cell function may be enhancedby
blocking one or more of these inhibitory path- ways,112,117
raising the possibility for potential thera-peutic application in
chronic viral infections such aschronic hepatitis B.
Based on our knowledge of the immune mechanismsof chronic HBV
infection, several approaches to restoreinnate or adaptive immunity
or both to control HBV infection in combination with other
direct antiviralstrategies have been applied.108,109 These
approachescan be broadly divided into virus-nonspecific and
virus-specific modalities. The first involves general immuno-
modulatory agents, and the latter aims to activate
theHBV-specific immune response by applying the tech-nologies of
therapeutic vaccination. As discussed above,the efficacy of
IFN-a therapy can be partly attributed toits immunostimulatory
effect. A promising approachemerges from the field of toll-like
receptors (TLRs). Var-ious TLR agonists with potent
immunostimulatory effects have been developed.118 Their
administration toHBV patients leads to both intrahepatic and
extrahe-patic induction of type 1 interferons and other
cytokinesthat may contribute directly to antiviral activity or
indi-rectly result in activation of innate and adaptive immune
responses. The second approach involves the blockadeof negative
immunoregulatory pathways (i.e., coinhibi-tory signals, inhibitory
cytokines, regulatory T cells),
which may induce a partial restoration of HBV-specificT
cells. Third, engineering of redirected T cells may result in
a de novo reconstitution of functionally
activeHBV-specific T cells and activation of heterologous Tcells.
Whether inhibition of a suppressive effect(s) of HBV can lead
to restoration of HBV-specific innate andadaptive immune responses
remains a challenging ques-tion. Several lines of evidence suggest
that HBV
HEPATOLOGY, Vol. 62, No. 6, 2015 LIANG ET AL. 1901
-
8/18/2019 Present and Future Therapies of Hepatitis B From
Discovery to Cure
10/16
interferes negatively with these host immune responses. A
more detailed understanding of the specific mecha-nisms is
mandatory before new ways of restoring immune responses by
targeting virus-specific factors canbe explored. HBV-specific
strategies may prove moreeffective and safer than virus-nonspecific
approaches.
A concern of the various immunotherapies is thepotential
risk of autoimmunity and/or exacerbation of liver damage by
immune-mediated death of hepatocytesin vivo. Careful consideration
of benefit versus risk and
close clinical monitoring would be needed in
theseapproaches.
HBV-Nonspecific Immunomodulatory Agents
TLR Agonists. The antiviral effect of TLR
agonists,particularly TLR-7, through activation of innate immu-nity
has been evaluated in HBV chronically infectedchimpanzees and
woodchucks. Upon stimulation of TLR-7, plasmacytoid dendritic
cells produce IFN-a and
Fig. 2. Innate and adaptive HBV-specific immune responses and
immune-based therapeutic development. Immune cells involved in
innate
and adaptive immune responses activated by HBV infection and
their mechanisms of antiviral actions are shown. They are
virus-specific CD81 T
cells that inhibit viral replication by both direct killing of
infected hepatocytes and cytokine-mediated antiviral mechanisms;
virus-specific CD41
T
cells, which provide essential help for CD81
T-cell priming and effector functions as well as antiviral
cytokines; regulatory T cells, which suppress
virus-specific T-cell functions; B cells, which mature to plasma
cells, producing neutralizing antibodies and potentially
participating in antigen pre-
sentation; natural killer cells, which display antiviral but
also regulatory activity by eliminating activated virus-specific
CD81
T cells; natural killer
T cells that sense virus-infected hepatocytes, produce
antiviral cytokines, and activate adaptive immune responses; other
immune cells in the
liver that play important roles in the activation and
coordination of the innate and adaptive responses such as Kupffer,
myeloid, and plasmacy-
toid dendritic cells. Therapeutic approaches designed to
activate various pathways of the innate and adaptive immunities are
illustrated in red.
See text for details of these approaches. Abbreviations: CTL,
cytotoxic T lymphocyte; DC, dendritic cell; IFNAR, IFN-a
receptor; IFNGR, IFN-creceptor; IFNLR, IFN-k receptor;
JAK/STAT, Janus kinase/signal transducer and activator of
transcription; Mu, macrophage; NK, natural killer; NKT,NK T cell;
TNF-L, tumor necrosis factor–like molecule (e.g., lymphotoxin-b);
TNF-LR, TNF-L receptor; Treg, regulatory T cell.
1902 LIANG ET AL. HEPATOLOGY, December 2015
-
8/18/2019 Present and Future Therapies of Hepatitis B From
Discovery to Cure
11/16
other cytokines/chemokines and induce the activation
of natural killer cells and activation of cytotoxic
lympho-cytes, thereby orchestrating both innate and adaptiveimmune
responses.119 The altered responsiveness of plasmacytoid
dendritic cells may contribute to the
reduced innate and adaptive immune responses during chronic
viral infections. Agonist-induced activation of TLR-7
therefore represents a novel approach for thetreatment of chronic
viral infections.120 GS-9620, anorally administered agonist of
TLR-7, was tested inHBV-infected chimpanzees.121 Short-term
administra-tion of the TLR-7 agonist provided long-term
suppres-sion of serum and liver HBV DNA. Serum levels of HBsAg
and HBeAg and numbers of HBV antigen-positive hepatocytes were
reduced. In parallel, GS-9620administration induced the production
of IFN-a andother cytokines and chemokines, up-regulated
ISG
expression, and activated natural killer cells and lympho-cyte
subsets, confirming the activation of TLR-7 signal-ing. Similar
effects were also observed in chronically infected woodchucks.
Phase 1 clinical evaluation hasbeen performed, and patients are now
being enrolled ina phase 2 trial combining tenofovir and GS-9620
incomparison to tenofovir monotherapy.122
PD1 and Other Coinhibitory Blockers. In chronicHBV
infection, loss of viral control has been explainedby exhausted T
cells. One approach would be to recoverexisting T cells by
correcting the balance between coin-hibitory (PD1, CTLA-4, Tim-3,
Lag-3) and costimulat-
ing (41BB, interleukin-12 [IL-12]) signals.123 Recentstudies in
the field of cancer therapy have highlightedthe clinical relevance
of PD1 blockade to restore antitu-mor immunity to improve
survival.124 As chronic HBV infection and tumor
immunology share similar charac-teristics in terms of immune
subversion and the role of PD1, PD1 blockade may be an
attractive concept forHBV therapy. A recent study in chronically
infected
woodchucks tested the combination therapy of entecavirand
an anti-PD1 ligand monoclonal antibody together
with a WHV DNA vaccine. PD1 blockade was shown
to synergize with entecavir and therapeutic vaccinationto
control viral replication and restore WHV-specific T-cell
responses.125
HBV-Specific Modified T Cells
As discussed above, HBV-specific T cells are
eitherexhausted or nonresponsive in chronic HBV infection.This
therapeutic approach is designed to provide geneti-cally engineered
T cells to target and eliminate HBV-infected hepatocytes. The
strategy to genetically modify patient’s T cells to express
HBV-specific T-cell receptors
and then infuse them into the same patients with HBV-associated
hepatocellular carcinoma showed some prom-ise.126,127 But the
variable and major histocompatibility complex–restricted
nature of the interaction between T-cell receptor and its ligand
and the skepticism that
whether one or two such modified T cells would be
suf-ficient to mount an effective T cell–based immuneresponse may
limit the clinical application of thisapproach. The recent emerging
technology of chimericantigen receptor (CAR) in the field of cancer
therapeu-tics has been extended to treatment of persistent
viralinfections.128 The CAR approach is to generate a chi-meric
receptor expressing an extracellular target-binding domain, a
hinge and membrane-anchoring region, andone (or more) intracellular
signaling domain.128 Thetarget-binding domain is derived from the
light andheavy chain sequences of a single-chain variable frag-
ment of the immunoglobulin. In the case of HBV, thetarget could
be the cell-surface form of HBsAg and thesingle-chain variable
fragment derived from a construct
with high-affinity anti-HBs activity.129 The binding
of the CAR-modified T cells to HBV-infected hepatocytescan
trigger proliferating or activating signals to initiatean effective
anti-HBV T-cell response. This strategy hasbeen applied to HBV
animal models with some prom-ise.130 It remains to be seen whether
CAR-modified Tcells can achieve a broadly acting and potent
anti-HBV response that is sufficient for viral clearance in
chronicHBV-infected patients.
Therapeutic Vaccines
The goal for therapeutic vaccination in chronic hepa-titis B is
to induce sufficient anti-HBV immuneresponses to eliminate and/or
cure infected hepatocytes
without undue host cell damage, prevent viral spread tonew
hepatocytes, and promote long-term viral control.These approaches
leverage our accumulating knowledgeof the adaptive immune responses
of HBV infectionand focus on restoring or activating endogenous
HBV-specific immune responses that initially targeted
HBsAg
and later expanded to other HBV antigens using recombinant
proteins, cytotoxic T-lymphocyte epitopevaccine, viral vectors, and
DNA vaccination. These vac-cines are being combined with antiviral
drugs andimmune modulators to maximize their effects. Anintriguing
strategy to personalize antigen presentation toinduce anti-HBV
immune response involving mono-cytes has been recently
proposed.131
HBsAg-Based Vaccine. Because HBsAg-based pro-phylactic
vaccine can induce protective virus-neutralizing antibodies, the
initial studies involved the
HEPATOLOGY, Vol. 62, No. 6, 2015 LIANG ET AL. 1903
-
8/18/2019 Present and Future Therapies of Hepatitis B From
Discovery to Cure
12/16
use of HBsAg in small trials, with virological and sero-logical
responses in some patients.132,133 Combinationof an HBsAg vaccine
with lamivudine showed promiseinitially in smaller studies.134
However, no difference inclinical efficacy was shown between
vaccinated and con-trol groups despite the induction of vigorous
HBsAg-specific cellular and humoral immune responses in
a large open-labeled randomized controlled trial of
HBV patients receiving 12 doses of recombinant HBsAg and
ASO2 adjuvant with 52 weeks of lamivudine.135 Simi-larly,
the use of yeast-derived recombinant HBsAg andhepatitis B immune
globulin immune complex showedpromise in a phase 1/2 study,136 but
this was not repro-duced in a larger phase 3 study.137
Cytotoxic T-Lymphocyte Epitope Vaccine. Immu-nization
with recombinant proteins (e.g., HBsAg) canpromote antibody and CD4
helper T-cell responses, but
generally not those of CD8 T cells, which require endo-genously
processed viral peptides. Given the relevance of antiviral CD8
T cells in HBV clearance, direct augmen-tation of HBV-specific CD8
T cells was attempted in a pilot study using a lipopeptide
encoding a single immu-nogenic human leukocyte antigen
A2–restricted HBV core 18-27 CTL epitope.138 Despite their
immunoge-nicity in healthy adults, this epitope vaccine was
notimmunogenic in patients with chronic hepatitis B anddid not
significantly change the HBV DNA titers orHBeAg status. Inclusion
of other epitopes in thisapproach may be necessary.
DNA Vaccination With or Without Immunomo-dulators. DNA
vaccination can promote antiviralCD8 T-cell as well as CD4 T-cell
and antibody responses.139 In this regard, intramuscular
injection of DNA encoding only pre-S2/S was safe,
well-tolerated,and at least transiently immunogenic but only
margin-ally effective in reducing HBV DNA levels in a phase 1study
of chronic hepatitis B patients who did notrespond to IFN-a
and/or lamivudine.140,141 It also didnot prevent viremic relapse in
the phase 1/2 ANRSHB02 VAC-AND trial.141 Another phase 1
study using plasmid DNA encoding all HBV open reading
frames
and human IL-12 in addition to daily lamivudineshowed a 50% HBV
DNA suppression at 1 year post–treatment cessation.142 However, in
a subsequent largerstudy, a related HBV plasmid DNA (all HBV open
read-ing frames except HBx) and human IL-12 with
daily adefovir showed only a tendency for greater HBeAg
lossand HBV DNA suppression compared to adefoviralone.143
Other Therapeutic Vaccine Trials. Currently,open-label
therapeutic HBV vaccine trials on clinical-trials.gov (as of May
2015) include (1) GS4774, a heat-
killed recombinant yeast expressing HBV S, core, andHBx fusion
protein144; (2) ABX203 with recombinantHBsAg and hepatitis B core
antigen in the setting of PEG IFN-a and oral antivirals;
(3) INO-1800, a multi-antigen DNA vaccine encoding HBsAg and
hepatitis Bcore antigen electroporated alone or combined
withINO-9112 encoding IL-12 in patients on either enteca-vir or
tenofovir; (4) TG1050, a nonreplicative E1/E3-deleted human
adenovirus encoding a fusion proteincombining modified HBV core,
polymerase and enve-lope145; (5) HBV vaccine with hepatitis B
immuneglobulin and granulocyte-macrophage colony-stimulat-ing
factor; (6) HBV vaccine with IFN-a2b and IL-2; (7)HBV vaccine
activated dendritic cells combined withPEG IFN-a or
nucleos(t)ide analogues; (8) intensifiedEuvax (HBV S) vaccination
with PEG-IFN-a.
Therapeutic Pipeline and ConclusionBased on the
literature, expert input, publicly dis-
closed information of various pharmaceutical compa-nies, the
clinicaltrial.gov website, we generated a tablesummarizing the
current status of various anti-HBV drugs or biologics in the
development pipeline (Table1). While many of them are still in
preclinical develop-ment, several have advanced to clinical trials.
As dis-cussed above, some of them showed early promise and
will likely advance to the late clinical trial phase
formore definitive proof of the preliminary success. In this
review, we have summarized the major therapeuticapproaches and
novel molecular targets for anti-HBV drug development and
provided a knowledge-basedrationale behind these various
strategies. It is possiblethat new and additional technologies may
emerge as thefield advances. To achieve a more sustained and
effectivecontrol of HBV infection, a combination of the
existing HBV therapies and one or more of the above
modalities,either small-molecule drugs or biologics, will be
neces-sary. With the concerted efforts of private and
publicsectors, the next milestone in the therapy of HBV infec-tion,
a functional “cure” that has remained elusive, is
likely within our grasp within the next decade.
References
1. Ott JJ, Stevens GA, Groeger J, Wiersma ST. Global
epidemiology of
hepatitis B virus infection: new estimates of age-specific HBsAg
sero-
prevalence and endemicity. Vaccine 2012;30:2212-2219.
2. Kennedy PT, Sandalova E, Jo J, Gill U, Ushiro-Lumb I, Tan
AT,
et al. Preserved T-cell function in children and young adults
with
immune-tolerant chronic hepatitis B. Gastroenterology
2012;143:637-
645.
3. Vanwolleghem T, Hou J, van Oord G, Andeweg AC, Osterhaus
AD,
Pas SD, et al. Re-evaluation of hepatitis B virus clinical
phases by
1904 LIANG ET AL. HEPATOLOGY, December 2015
-
8/18/2019 Present and Future Therapies of Hepatitis B From
Discovery to Cure
13/16
systems biology identifies unappreciated roles for the innate
immune
response and B cells. HEPATOLOGY 2015;62:87-100.
4. McMahon BJ. The natural history of chronic hepatitis B virus
infec-
tion. HEPATOLOGY 2009;49:S45-S55.
5. Prati D, Taioli E, Zanella A, Della Torre E, Butelli S, Del
Vecchio E,
et al. Updated definitions of healthy ranges for serum alanine
amino-
transferase levels. Ann Intern Med 2002;137:1-10.
6. Schulze A, Gripon P, Urban S. Hepatitis B virus infection
initiates with a large surface protein-dependent binding to
heparan sulfate pro-
teoglycans. HEPATOLOGY 2007;46:1759-1768.
7. Salisse J, Sureau C. A function essential to viral entry
underlies the
hepatitis B virus “a” determinant. J Virol
2009;83:9321-9328.
8. Yan H, Zhong G , Xu G, He W, Jing Z, Gao Z,
et al. Sodium tauro-
cholate cotransporting polypeptide is a functional receptor for
human
hepatitis B and D virus. Elife 2012;1:e00049.
9. Doring B, Lutteke T, Geyer J, Petzinger E. The SLC10 carrier
family:
transport functions and molecular structure. Curr Top Membr
2012;
70:105-168.
10. Schieck A, Schulze A, Gahler C, Muller T, Haberkorn U,
Alexandrov
A, et al. Hepatitis B virus hepatotropism is mediated by
specific
receptor recognition in the liver and not restricted to
susceptible
hosts. HEPATOLOGY 2013;58:43-53.
11. Urban S, Bartenschlager R, Kubitz R, Zoulim F. Strategies to
inhibitentry of HBV and HDV into hepatocytes. Gastroenterology
2014;
147:48-64.
12. Ni Y, Lempp FA, Mehrle S, Nkongolo S, Kaufman C, Falth M, et
al.
Hepatitis B and D viruses exploit sodium taurocholate
co-transporting
polypeptide for species-specific entry into hepatocytes.
Gastroenterol-
ogy 2014;146:1070-1083.
13. Yan H, Peng B, He W, Zhong G, Qi Y, Ren B, et al.
Molecular
determinants of hepatitis B and D virus entry restriction in
mouse
sodium taurocholate cotransporting polypeptide. J Virol
2013;87:
7977-7991.14. Huang HC, Chen CC, Chang WC, Tao MH, Huang C.
Entry of
hepatitis B virus into immortalized human primary hepatocytes
by
clathrin-dependent endocytosis. J Virol 2012;86:9443-9453.
15. Macovei A, Radulescu C, Lazar C, Petrescu S, Durantel D,
Dwek
RA, et al. Hepatitis B virus requires intact caveolin-1 function
for
productive infection in HepaRG cells. J Virol
2010;84:243-253.
16. Schmitz A , Schwarz A , Foss M, Zhou
L, Rabe B, Hoellenriegel J,
et al. Nucleoporin 153 arrests the nuclear import of hepatitis B
virus
capsids in the nuclear basket. PLoS Pathog 2010;6:e1000741.
17. Koniger C, Wingert I, Marsmann M, Rosler C, Beck J, Nassal
M.
Involvement of the host DNA-repair enzyme TDP2 in formation
of
the covalently closed circular DNA persistence reservoir of
hepatitis B
viruses. Proc Natl Acad Sci USA 2014;111:E4244-E4253.
18. Bock CT, Schwinn S, Locarnini S, Fyfe J, Manns MP, Trautwein
C,
et al. Structural organization of the hepatitis B virus
minichromo-
some. J Mol Biol 2001;307:183-196.19. Pollicino T, Belloni L,
Raffa G, Pediconi N, Squadrito G, Raimondo
G, et al. Hepatitis B virus replication is regulated by the
acetylation
status of hepatitis B virus cccDNA-bound H3 and H4 histones.
Gas-
troenterology 2006;130:823-837.
20. Belloni L, Pollicino T, De Nicola F, Guerrieri F, Raffa G,
FanciulliM, et al. Nuclear HBx binds the HBV minichromosome and
modifies
the epigenetic regulation of cccDNA function. Proc Natl Acad
Sci
USA 2009;106:19975-19979.
21. Lucifora J, Arzberger S, Durantel D, Belloni L,
Strubin M, Levrero
M, et al. Hepatitis B virus X protein is essential to initiate
and main-
tain virus replication after infection. J Hepatol
2011;55:996-1003.
22. Watanabe T, Sorensen EM, Naito A, Schott M, Kim S, Ahlquist
P.
Involvement of host cellular multivesicular body functions in
hepatitis
B virus budding. Proc Natl Acad Sci USA 2007;104:10205-10210.23.
Lentz TB, Loeb DD. Roles of the envelope proteins in the
amplifica-
tion of covalently closed circular DNA and completion of
synthesis of
the plus-strand DNA in hepatitis B virus. J Virol
2011;85:11916-
11927.
24. Werle-Lapostolle B, Bowden S, Locarnini S, Wursthorn K,
Petersen J,
Lau G, et al. Persistence of cccDNA during the natural history
of
chronic hepatitis B and decline during adefovir dipivoxil
therapy. Gas-
troenterology 2004;126:1750-1758.
25. Lok AS, McMahon BJ. Chronic hepatitis B: update 2009.
HEPATO-
LOGY 2009;50:661-662.
26. European Association for the Study of the Liver. EASL
clinical prac-
tice guidelines: management of hepatitis C virus infection. J
Hepatol2011;55:245-264.
27. Liaw YF, Leung N, Kao JH, Piratvisuth T, Gane E, Han KH, et
al.
Asian-Pacific consensus statement on the management of
chronic hep-
atitis B: a 2008 update. Hepatol Int 2008;2:263-283.
28. Xu C, Guo H, Pan XB, Mao R, Yu W, Xu X, et al. Interferons
accel-
erate decay of replication-competent nucleocapsids of hepatitis
B
virus. J Virol 2010;84:9332-9340.
29. Hao J, Jin W, Li X, Wang S, Zhang X, Fan H, et al.
Inhibition of
alpha interferon (IFN-alpha)-induced microRNA-122
negatively
affects the anti-hepatitis B virus efficiency of IFN-alpha. J
Virol 2013;
87:137-147.
30. Micco L, Peppa D, Loggi E, Schurich A, Jefferson L, Cursaro
C,
et al. Differential boosting of innate and adaptive antiviral
responses
during pegylated-interferon-alpha therapy of chronic hepatitis
B.
J Hepatol 2013;58:225-233.31. ter Borg MJ, Hansen BE,
Herrmann E, Zeuzem S, Cakaloglu Y,
Karayalcin S, et al. Modelling of early viral kinetics and
pegylated
interferon-alpha2b pharmacokinetics in patients with
HBeAg-positive
chronic hepatitis B. Antivir Ther 2007;12:1285-1294.
32. Sadler AJ, Williams BR. Interferon-inducible antiviral
effectors. Nat
Rev Immunol 2008;8:559-568.
33. Belloni L, Allweiss L, Guerrieri F, Pediconi N, Volz T,
Pollicino T,
et al. IFN-alpha inhibits HBV transcription and replication in
cell
culture and in humanized mice by targeting the epigenetic
regulation
of the nuclear cccDNA minichromosome. J Clin Invest
2012;122:
529-537.
34. Gripon P, Rumin S, Urban S, Le Seyec J, Glaise D, Cannie I,
et al.
Infection of a human hepatoma cell line by hepatitis B virus.
Proc
Natl Acad Sci USA 2002;99:15655-15660.
35. Lucifora J, Xia Y , Reisinger F, Zhang K,
Stadler D, Cheng X, et al.Specific and nonhepatotoxic degradation
of nuclear hepatitis B virus
cccDNA. Science 2014;343:1221-1228.
36. Stenglein MD, Burns MB, Li M, Lengyel J, Harris RS.
APOBEC3
proteins mediate the clearance of foreign DNA from human
cells.
Nat Struct Mol Biol 2010;17:222-229.
37. Liang G, Kitamura K, Wang Z, Liu G, Chowdhury S, Fu W, et
al.
RNA editing of hepatitis B virus transcripts by
activation-induced cyt-
idine deaminase. Proc Natl Acad Sci USA 2013;110:2246-2251.
38. Noguchi C, Hiraga N, Mori N, Tsuge M, Imamura M, Takahashi
S,
et al. Dual effect of APOBEC3G on Hepatitis B virus. J Gen
Virol
2007;88:432-440.
39. Renard M, Henry M, Guetard D, Vartanian JP, Wain-Hobson
S.
APOBEC1 and APOBEC3 cytidine deaminases as restriction
factors
for hepadnaviral genomes in non-humans in vivo. J Mol Biol
2010;
400:323-334.40. Turelli P, Mangeat B, Jost S,
Vianin S, Trono D. Inhibition of hepa-
titis B virus replication by APOBEC3G. Science
2004;303:1829.
41. Guidotti LG, Chisari FV. Immunobiology and pathogenesis of
viral
hepatitis. Annu Rev Pathol 2006;1:23-61.
42. Yapali S, Talaat N, Lok AS. Management of hepatitis B: our
practice
and how it relates to the guidelines. Clin Gastroenterol
Hepatol
2014;12:16-26.
43. Marcellin P, Ahn SA, Ma X, Caruntu FA, Tak WY, Elkashab
M,
et al. HBsAg loss with tenofovir disoproxil fumarate plus
peginter-
feron alfa-2a in chronic hepatitis B: results of a global
randomized
controlled trial. HEPATOLOGY 2014;60:294A.
44. Marcellin P, Gane E, Buti M, Afdhal N, Sievert W, Jacobson
IM,
et al. Regression of cirrhosis during treatment with
tenofovir
HEPATOLOGY, Vol. 62, No. 6, 2015 LIANG ET AL. 1905
-
8/18/2019 Present and Future Therapies of Hepatitis B From
Discovery to Cure
14/16
disoproxil fumarate for chronic hepatitis B: a 5-year
open-label
follow-up study. Lancet 2013;381:468-475.
45. Chotiyaputta W, Peterson C, Ditah FA, Goodwin D, Lok AS.
Persist-
ence and adherence to nucleos(t)ide analogue treatment for
chronic
hepatitis B. J Hepatol 2011;54:12-18.
46. Liaw YF, Sung JJ, Chow WC, Farrell G, Lee CZ, Yuen H, et al.
Lam-
ivudine for patients with chronic hepatitis B and advanced liver
dis-
ease. N Engl J Med 2004;351:1521-1531.47. Menendez-Arias L,
Alvarez M, Pacheco B. Nucleoside/nucleotide ana-
log inhibitors of hepatitis B virus polymerase: mechanism of
action
and resistance. Curr Opin Virol 2014;8:1-9.
48. Zoulim F, Mason WS. Reasons to consider earlier treatment
of
chronic HBV infections. Gut 2012;61:333-336.
49. Chan HL, Chan CK, Hui AJ, Chan S, Poordad F, Chang TT, et
al.
Effects of tenofovir disoproxil fumarate in hepatitis B e
antigen-
positive patients with normal levels of alanine aminotransferase
and
high levels of hepatitis B virus DNA. Gastroenterology
2014;146:
1240-1248.
50. Lok AS, Trinh H, Carosi G, Akarca US, Gadano A, Habersetzer
F,
et al. Efficacy of entecavir with or without tenofovir
disoproxil fuma-
rate for nucleos(t)ide-naive patients with chronic hepatitis B.
Gastro-
enterology 2012;143:619-628.
51. Lau GK, Piratvisuth T, Luo KX, Marcellin P, Thongsawat
S,Cooksley G, et al. Peginterferon alfa-2a, lamivudine, and the
combi-
nation for HBeAg-positive chronic hepatitis B. N Engl J Med
2005;
352:2682-2695.
52. Marcellin P, Lau GK, Bonino F, Farci P, Hadziyannis S, Jin
R, et al.
Peginterferon alfa-2a alone, lamivudine alone, and the two in
combi-
nation in patients with HBeAg-negative chronic hepatitis B. N
Engl J
Med 2004;351:1206-1217.
53. Su W-W, Hsu C-W, Lee C-M, Peng C-Y, Chuang W-L, Kao J-H,
et al. Combination therapy with peginterferon alfa-2a and a
nucleos(-
t)ide analogue for HBeAg-positive chronic hepatitis B patients:
results
of a large, randomised, multicentre, double-blind,
placebo-controlled
study. J Hepatol 2014;60:S47.
54. Ning Q, Han M, Sun Y, Jiang J, Tan D, Hou J, et al.
Switching
from entecavir to PegIFN alfa-2a in patients with
HBeAg-positive
chronic hepatitis B: a randomised open-label trial (OSST
trial). J Hepatol 2014;61:777-784.
55. Chan HL, Leung NW, Hui AY, Wong VW, Liew CT, Chim AM,
et al. A randomized, controlled trial of combination therapy
for
chronic hepatitis B: comparing pegylated interferon-alpha2b and
lami-
vudine with lamivudine alone. Ann Intern Med
2005;142:240-250.
56. Thimme R, Dandri M. Dissecting the divergent effects of
interferon-
alpha on immune cells: time to rethink combination therapy
in
chronic hepatitis B? J Hepatol 2013;58:205-209.
57. Brouwer WP, Xie Q, Sonneveld MJ, Zhang N, Zhang Q, Tabak
F,
et al. Adding peginterferon to entecavir for HBeAg-positive
chronic
hepatitis B: a multicentre randomized trial (ARES study).
HEPATOLOGY
2015;61:1512-1522.
58. Seto WK, Chan TS, Hwang YY, Wong DK, Fung J, Liu KS, et
al.
Hepatitis B reactivation in patients with previous hepatitis B
virus
exposure undergoing rituximab-containing chemotherapy for
lym-phoma: a prospective study. J Clin Oncol 2014;32:3736-3743.
59. Bourliere M, Rabiega P, Ganne-Carrie N, Serfaty L, Marcellin
P,
Pouget N, et al. HBsAg clearance after addition of 48 weeks
of
PEGIFN in HBeAg negative CHB patients on nucleos(t)ide with
undetactable HBV DNA for at leat one year: a multicenter
random-
ized controlled phase III trial ANRS-HB06 PEGAN study:
prelimi-
nary findings. HEPATOLOGY 2014;60:1094A.
60. Xie Q, Zhou H, Bai X, Wu S, Chen JJ, Sheng J, et al. A
randomized,
open-label clinical study of combined pegylated interferon
alfa-2a
(40KD) and entecavir treatment for hepatitis B “e”
antigen-positive
chronic hepatitis B. Clin Infect Dis 2014;59:1714-1723.
61. Vanderlinden E, Naesens L. Emerging antiviral strategies to
interfere
with influenza virus entry. Med Res Rev
2014;34:301-339.
62. Haqqani AA, Tilton JC. Entry inhibitors and their use in the
treat-
ment of HIV-1 infection. Antiviral Res 2013;98:158-170.
63. Petersen J, Dandri M, Mier W, Lutgehetmann M, Volz T,
von
Weizsacker F, et al. Prevention of hepatitis B virus
infection in vivo
by entry inhibitors derived from the large envelope protein. Nat
Bio-
technol 2008;26:335-341.
64. Aspinall EJ, Hawkins G, Fraser A, Hutchinson SJ, Goldberg D.
Hep-
atitis B prevention, diagnosis, treatment and care: a review.
OccupMed (Lond) 2011;61:531-540.
65. Galun E, Eren R, Safadi R, Ashour Y, Terrault N, Keeffe EB,
et al.
Clinical evaluation (phase I) of a combination of two human
mono-
clonal antibodies to HBV: safety and antiviral properties.
HEPATOLOGY
2002;35:673-679.
66. Mason WS, Xu C, Low HC, Saputelli J, Aldrich CE, Scougall
C,
et al. The amount of hepatocyte turnover that occurred during
resolu-
tion of transient hepadnavirus infections was lower when virus
replica-
tion was inhibited with entecavir. J Virol 2009;83:1778-1789.67.
Blanchet M, Sureau C. Infectivity determinants of the hepatitis
B
virus pre-S domain are confined to the N-terminal 75 amino acid
res-
idues. J Virol 2007;81:5841-5849.
68. Gripon P, Le Seyec J, Rumin S, Guguen-Guillouzo C.
Myristylation
of the hepatitis B virus large surface protein is essential for
viral infec-
tivity. Virology 1995;213:292-299.69. Blank A, Markert C,
Hohmann N, Carls A, Mikus G, Lehr T, et al.
Myrcludex B: successful first-in-human administration of a first
in
class hepatitis B and hepatitis D virus entry inhibitor. J
Hepatol. Sub-
mitted for publication.
70. Lucifora J, Esser K, Protzer U. Ezetimibe blocks hepatitis B
virus
infection after virus uptake into hepatocytes. Antiviral Res
2013;97:
195-197.
71. Nkongolo S, Ni Y, Lempp FA, Kaufman C, Lindner T,
Esser-Nobis
K, et al. Cyclosporin A inhibits hepatitis B and hepatitis D
virus entry
by cyclophilin-independent interference with the NTCP
receptor.
J Hepatol 2014;60:723-731.
72. Watashi K, Sluder A, Daito T, Matsunaga S, Ryo A, Nagamori
S,
et al. Cyclosporin A and its analogs inhibit hepatitis B virus
entry
into cultured hepatocytes through targeting a membrane
transporter,
sodium taurocholate cotransporting polypeptide (NTCP).
HEPATOLOGY
2014;59:1726-1737.
73. Vaz FM, Paulusma CC, Huidekoper H, de Ru M, Lim C, Koster
J,
et al. Sodium taurocholate cotransporting polypeptide
(SLC10A1)
deficiency: conjugated hypercholanemia without a clear clinical
pheno-
type. HEPATOLOGY 2015;61:260-267.74. Slijepcevic D,
Kaufman C, Wichers CG, Gilglioni EH, Lempp FA,
Duijst S, et al. Impaired uptake of conjugated bile acids and
hepatitis
B virus preS1-binding in Na-taurocholate cotransporting
polypeptide
knockout mice. HEPATOLOGY 2015;62:207-219.75.
Bogomolov P, Voronkova N, Allweiss L, Dandri M, Schwab M,
Lempp FA, et al. A proof-of-concept phase 2a clinical trial
with
HBV/HDV entry inhibitor Myrcludex B. HEPATOLOGY
2014;60:
1279A-1280A.76. King RW, Ladner SK, Miller TJ, Zaifert K, Perni
RB, Conway SC,
et al. Inhibition of human hepatitis B virus replication by
AT-61, a
phenylpropenamide derivative, alone and in combination with
(–)beta-L-2’,3’-dideoxy-3’-thiacytidine. Antimicrob Agents
Chemother 1998;
42:3179-3186.
77. Feld JJ, Colledge D, Sozzi V, Edwards R, Littlejohn M,
Locarnini SA.
The phenylpropenamide derivative AT-130 blocks HBV replication
at
the level of viral RNA packaging. Antiviral Res
2007;76:168-177.
78. Delaney WE, Edwards R, Colledge D, Shaw T, Furman P, Painter
G,
et al. Phenylpropenamide derivatives AT-61 and AT-130 inhibit
repli-
cation of wild-type and lamivudine-resistant strains of
hepatitis B
virus in vitro. Antimicrob Agents Chemother
2002;46:3057-3060.
79. Billioud G, Pichoud C, Puerstinger G, Neyts J, Zoulim F. The
main
hepatitis B virus (HBV) mutants resistant to nucleoside analogs
are
susceptible in vitro to non-nucleoside inhibitors of HBV
replication.
Antiviral Res 2011;92:271-276.
1906 LIANG ET AL. HEPATOLOGY, December 2015
-
8/18/2019 Present and Future Therapies of Hepatitis B From
Discovery to Cure
15/16
80. Katen SP, Tan Z, Chirapu SR, Finn MG, Zlotnick A.
Assembly-
directed antivirals differentially bind quasiequivalent pockets
to mod-
ify hepatitis B virus capsid tertiary and quaternary structure.
Structure
2013;21:1406-1416.
81. Deres K, Schroder CH, Paessens A, Goldmann S, Hacker HJ,
Weber
O, et al. Inhibition of hepatitis B virus replication by
drug-induced
depletion of nucleocapsids. Science 2003;299:893-896.
82. Stray SJ, Bourne CR, Punna S, Lewis WG, Finn MG, Zlotnick A.
A heteroaryldihydropyrimidine activates and can misdirect
hepatitis B
virus capsid assembly. Proc Natl Acad Sci USA
2005;102:8138-8143.
83. Stray SJ, Zlotnick A. BAY 41-4109 has multiple effects on
hepatitis B
virus capsid assembly. J Mol Recognit 2006;19:542-548.
84. Gane E, Schwabe C, Walker K, Flores L, Hartman G, Klumpp
K,
et al. Phase 1a safety and pharmacokinetics of NVR 3-778, a
poten-
tial first-in-class HBV core inhibitor. HEPATOLOGY
2014;60:1267A-
1290A.
85. Prange R. Host factors involved in hepatitis B virus
maturation,
assembly, and egress. Med Microbiol Immunol
2012;201:449-461.
86. Heermann KH, Goldmann U, Schwartz W, Seyffarth T,
Baumgarten
H, Gerlich WH. Large surface proteins of hepatitis B virus
containing
the pre-S sequence. J Virol 1984;52:396-402.
87. Xu Y, Hu Y, Shi B, Zhang X, Wang J, Zhang Z, et al. HBsAg
inhib-
its TLR9-mediated activation and IFN-alpha production in
plasmacy-toid dendritic cells. Mol Immunol 2009;46:2640-2646.
88. Gehring AJ, Ann D’Angelo J. Dissecting the dendritic cell
controversy
in chronic hepatitis B virus infection. Cell Mol Immunol
2015;12:
283-291.
89. Kapoor R, Kottilil S. Strategies to eliminate HBV infection.
Future
Virol 2014;9:565-585.
90. Blazquez LC, Fortes P. Harnessing RNAi for the treatment of
viral
infections. In: Arbuthnot P, Weinberg MS, eds. Applied RNAi.
Cais-
ter Academic Press, Norfolk, UK; 2014:151-180.
91. Chen Y, Cheng G, Mahato RI. RNAi for treating hepatitis B
viral
infection. Pharm Res 2008;25:72-86.
92. Klein C, Bock CT, Wedemeyer H, Wustefeld T, Locarnini S,
Dienes
HP, et al. Inhibition of hepatitis B virus replication in vivo
by nucleo-
side analogues and siRNA. Gastroenterology 2003;125:9-18.
93. McCaffrey AP, Nakai H, Pandey K, Huang Z, Salazar FH, Xu
H,et al. Inhibition of hepatitis B virus in mice by RNA
interference.
Nat Biotechnol 2003;21:639-644.
94. Lanford R, Wooddell CI, Chavez D, Oropeza CE, Chu Q,
Hamilton
HL, et al. ARC-520 RNAi therapeutic reduces hepatitis B
virus
DNA, S antigen and e antigen in a chimpanzee with a very high
viral
titer. HEPATOLOGY 2013;58(Suppl. 1):705A-730A.
95. Yuen M-F, Chan HL-Y, Given B, Hamilton J, Schluep T, Lewis
DL,
et al. Phase II, dose ranging study of ARC-520, a siRNA-based
thera-
peutic, in patients with chronic hepatitis B virus infection. H
EPATO-
LOGY 2014;60:1267A-1290A.
96. Alnylam announces new RNAi therapeutic program for the
treatment
of HBV infection and reports an up to 2.3 log10 reduction of
HBsAg
in chronically infected chimpanzees [press release]. Cambridge,
MA:
Alnylam; February 12, 2014.
97. Sung JJ, Wong ML, Bowden S, Liew CT, Hui AY, Wong VW, et
al.Intrahepatic hepatitis B virus covalently closed circular DNA
can be a
predictor of sustained response to therapy. Gastroenterology
2005;
128:1890-1897.
98. Zhu Y, Yamamoto T, Cullen J, Saputelli J, Aldrich CE, Miller
DS,
et al. Kinetics of hepadnavirus loss from the liver during
inhibition of
viral DNA synthesis. J Virol 2001;75:311-322.
99. Zoulim F, Durantel D, Deny P. Management and prevention of
drug
resistance in chronic hepatitis B. Liver Int 2009;29(Suppl.
1):108-
115.
100. Moraleda G, Saputelli J, Aldrich CE, Averett D, Condreay L,
Mason
WS. Lack of effect of antiviral therapy in nondividing
hepatocyte cul-
tures on the closed circular DNA of woodchuck hepatitis
virus.
J Virol 1997;71:9392-9399.
101. MacDonald RA. “Lifespan” of liver cells. Autoradiographic
study
using tritiated thymidine in normal, cirrhotic, and partially
hepatec-
tomized rats. Arch Intern Med 1961;107:335-343.102. Magami Y,
Azuma T, Inokuchi H, Kokuno S, Moriyasu F, Kawai K,
et al. Cell proliferation and renewal of normal hepatocytes and
bile
duct cells in adult mouse liver. Liver 2002;22:419-425.
103. Chen J, Zhang W, Lin J, Wang F, Wu M, Chen C, et al. An
efficient
antiviral strategy for targeting hepatitis B virus genome using
tran-scription activator-like effector nucleases. Mol Ther
2014;22:303-311.
104. Weber ND, Stone D, Sedlak RH, De Silva Feelixge HS,
Roychoudhury P, Schiffer JT, et al. AAV-mediated delivery of
zinc fin-
ger nucleases targeting hepatitis B virus inhibits active
replication.
PLoS One 2014;9:e97579.
105. Tavis JE, Cheng X, Hu Y, Totten M, Cao F, Michailidis E, et
al. The
hepatitis B virus ribonuclease H is sensitive to inhibitors of
the
human immunodeficiency virus ribonuclease H and integrase
enzymes. PLoS Pathog 2013;9:e1003125.
106. Liu F, Campagna M, Qi Y, Zhao X, Guo F, Xu C, et al.
Alpha-inter-
feron suppresses hepadnavirus transcription by altering
epigenetic
modification of cccDNA minichromosomes. PLoS Pathog 2013;9:
e1003613.
107. Cai D, Mills C, Yu W, Yan R, Aldrich CE, Saputelli JR, et
al. Identi-
fication of disubstituted sulfonamide compounds as specific
inhibitorsof hepatitis B virus covalently closed circular DNA
formation. Anti-
microb Agents Chemother 2012;56:4277-4288.108. Protzer U, Maini
MK, Knolle PA. Living in the liver: hepatic infec-
tions. Nat Rev Immunol 2012;12:201-213.
109. Bertoletti A, Ferrari C. Innate and adaptive immune
responses in
chronic hepatitis B virus infections: towards restoration of
immune
control of viral infection. Gut 2012;61:1754-1764.110. Lau JY,
Bird GL, Alexander GJ, Williams R. Effects of immunosup-
pressive therapy on hepatic expression of hepatitis B viral
genome and
gene products. Clin Invest Med 1993;16:226-236.111. Das A, Hoare
M, Davies N, Lopes AR, Dunn C, Kennedy PT, et al.
Functional skewing of the global CD8 T cell population in
chronic
hepatitis B virus infection. J Exp Med 2008;205:2111-2124.
112. Lopes AR, Kellam P, Das A, Dunn C, Kwan A, Turner J, et al.
Bim-
mediated deletion of antigen-specific CD8 T cells in patients
unable
to control HBV infection. J Clin Invest 2008;118:1835-1845.
113. Chang KM. Hepatitis B immunology for clinicians. Clin Liver
Dis
2010;14:409-424.
114. Bertoletti A, Maini MK, Ferrari C. The host–pathogen
interaction
during HBV infection: immunological controversies. Antivir
Ther
2010;15(Suppl. 3):15-24.115. Xu D, Fu J, Jin L, Zhang H, Zhou C,
Zou Z, et al. Circulating and
liver resident CD41CD251 regulatory T cells actively influence
the
antiviral immune response and disease progression in patients
with
hepatitis B. J Immunol 2006;177:739-747.
116. Boni C, Fisicaro P, Valdatta C, Amadei B, Di Vincenzo P,
Giuberti T,
et al. Characterization of hepatitis B virus (HBV)-specific
T-cell dys-
function in chronic HBV infection. J Virol
2007;81:4215-4225.
117. Nakamoto N, Cho H, Shaked A, Olthoff K, Valiga ME,
Kaminski
M, et al. Synergistic reversal of intrahepatic HCV-specific CD8
T cell
exhaustion by combined PD-1/CTLA-4 blockade. PLoS Pathog
2009;5:e1000313.
118. Baxevanis CN, Voutsas IF, Tsitsilonis OE. Toll-like
receptor agonists:
current status and future perspective on their utility as
adjuvants in
improving anticancer vaccination strategies. Immunotherapy
2013;5:
497-511.119. Zoulim F, Luangsay S, Durantel D. Targeting innate
immunity: a
new step in the development of combination therapy for chronic
hep-
atitis B. Gastroenterology 2013;144:1342-1344.
120. Hirsch I, Caux C, Hasan U, Bendriss-Vermare N, Olive D.
Impaired
Toll-like receptor 7 and 9 signaling: from chronic viral
infections to
cancer. Trends Immunol 2010;31:391-397.121. Lanford RE, Guerra
B, Chavez D, Giavedoni L, Hodara VL, Brasky
KM, et al. GS-9620, an oral agonist of Toll-like receptor-7,
induces
HEPATOLOGY, Vol. 62, No. 6, 2015 LIANG ET AL. 1907
-
8/18/2019 Present and Future Therapies of Hepatitis B From
Discovery to Cure
16/16
prolonged suppression of hepatitis B virus in chronically
infected
chimpanzees. Gastroenterology 2013;144:1508-1517.
122. Gane EJ, Lim YS, Gordon SC, Visvanathan K, Sicard E,
Fedorak RN, et al. The oral toll-like receptor-7 agonist
GS-9620 in patients
with chronic hepatitis B virus infection. J Hepatol
2015;63:320-328.
123. Bertoletti A, Gehring AJ. Immune therapeutic strategies in
chronichepatitis B virus infection: virus or inflammation control?
PLoS
Pathog 2013;9:e1003784.124. Topalian SL, Hodi FS, Brahmer JR,
Gettinger SN, Smith DC,
McDermott DF, et al. Safety, activity, and immune correlates of
anti-PD-1 antibody in cancer. N Engl J Med 2012;366:2443-2454.
125. Kosinska AD, Zhang E, Johrden L, Liu J, Seiz PL, Zhang X,
et al.
Combination of DNA prime–adenovirus boost immunization
withentecavir elicits sustained control of chronic hepatitis B in
the wood-
chuck model. PLoS Pathog 2013;9:e1003391.
126. Koh S, Shimasaki N, Suwanarusk R, Ho ZZ, Chia A, Banu N, et
al. A practical approach to immunotherapy of hepatocellular
carcinoma
using T cells redirected against hepatitis B virus. Mol Ther
Nucleic
Acids 2013;2:e114.
127. Qasim W, Brunetto M, Gehring AJ, Xue SA, Schurich A,
Khakpoor A, et al. Immunotherapy of HCC metastases with
autologous T cell
receptor redirected T cells, targeting HBsAg in a liver
transplant
patient. J Hepatol 2015;62:486-491.128. Gill S, June CH. Going
viral: chimeric antigen receptor T-cell therapy
for hematological malignancies. Immunol Rev 2015;263:68-89.
129. Bohne F, Chmielewski M, Ebert G, Wiegmann K, Kurschner
T,Schulze A, et al. T cells redirected against hepatitis B virus
surface
proteins eliminate infected hepatocytes. Gastroenterology
2008;134:
239-247.130. Krebs K, Bottinger N, Huang LR, Chmielewski M,
Arzberger S,
Gasteiger G, et al. T cells expressing a chimeric antigen
receptor that
binds hepatitis B virus envelope proteins control virus
replication in
mice. Gastroenterology 2013;145:456-465.131. Gehring AJ, Haniffa
M, Kennedy PT, Ho ZZ, Boni C, Shin A, et al.
Mobilizing monocytes to cross-present circulating viral antigen
in
chronic infection. J Clin Invest 2013;123:3766-3776.132.
Dienstag JL, Stevens CE, Bhan AK, Szmuness W. Hepatitis B
vaccine
administered to chronic carriers of hepatitis b surface antigen.
Ann
Intern Med 1982;96:575-579.133. Pol S, Driss F, Michel ML,
Nalpas B, Berthelot P, Brechot C. Specific
vaccine therapy in chronic hepatitis B infection. Lancet
1994;344:
342.
134. Horiike N, Fazle Akbar SM, Michitaka K, Joukou K, Yamamoto
K,Kojima N, et al. In vivo immunization by vaccine
therapy following
virus suppression by lamivudine: a novel approach for
treating
patients with chronic hepatitis B. J Clin Virol
2005;32:156-161.135. Vandepapeliere P, Lau GK, Leroux-Roels G,
Horsmans Y, Gane E,
Tawandee T, et al. Therapeutic vaccination of chronic hepatitis
B
patients with virus suppression by antiviral therapy: a
randomized,controlled study of co-administration of HBsAg/AS02
candidate vac-
cine and lamivudine. Vaccine 2007;25:8585-8597.
136. Xu DZ, Zhao K, Guo LM, Li LJ, Xie Q, Ren H, et al. A
randomizedcontrolled phase IIb trial of antigen-antibody
immunogenic complex
therapeutic vaccine in chronic hepatitis B patients. PLoS One
2008;3:e2565.
137. Xu DZ, Wang XY, Shen XL, Gong GZ, Ren H, Guo LM, et
al.Results of a phase III clinical trial with an HBsAg-HBIG
immuno-
genic complex therapeutic vaccine for chronic hepatitis B
patients:
experiences and findings. J Hepatol 2013;59:450-456.138.
Heathcote J, McHutchison J, Lee S, Tong M, Benner K, Minuk G,
et al. A pilot study of the CY-1899 T-cell vaccine in subjects
chroni-
cally infected with hepatitis B