Embed Size (px)
Citation preview

VOL. 7 NO. 2 FEBRUARY 2005 THE JOURNAL OF CLINICAL HYPERTENSION 81
Recent literature suggests that most hypertensives will require two or more drugs to achieve target blood pressure. Our objective was to estimate the proportion of patients receiving diuretics, includ-ing thiazides, for blood pressure control among those receiving two or more drugs. We studied 25,052 hypertensives in a tertiary care Veterans Affairs facility and identified individuals tak-ing any thiazide or loop diuretic among patients receiving two, three, four, or more drugs. Rates of any diuretic use were 50%, 73%, and 89%, and decreased to 39.0%, 59.0%, and 72.5% for thiazide use, respectively. Rates of thiazide use were statistically significantly higher among African Americans compared with the general study population, but did not differ significantly in the elderly. Though overall diuretic use seems to be increasing as compared with previous stud-ies, there is room for improvement in the use of thiazides in multi-drug hypertension regimens. (J Clin Hypertens. 2005;7:81–89) ©2005 Le Jacq Ltd.
Hypertension treatment is the most common rea-son for office visits to physicians and for use
of prescription drugs in adults in the United States.1 Hypertension affects about 50 million people in the United States and about 1 billion worldwide.2 In the Department of Veterans Affairs (VA) health care system, it has a prevalence of 37%, being the most common chronic condition, and affecting more than a million patients.3 Studies have persistently shown that many patients have inadequate blood pressure (BP) control, suggesting a gap between hypertension practice guide-lines and achieved BP control.4–6 Since BP control is often inadequate even in patients who receive regular care, it has been emphasized that control of hypertension can be better achieved if the processes of care are improved. This includes aggressiveness with use and appropriate-ness of antihypertensive medication regimens.2,5 The Seventh Report of the Joint National Committee on the Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7)2 serves an important function to issue guidelines and advisories designed to increase treatment and control of hypertension. Even before the recent findings of the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT)7 and release of JNC 7 guidelines, diuretics were recommended by previous reports of the JNC as one of the first-choice medications in the management of hypertension, in the absence of contraindications and compelling indications for other drugs.8 Recent hyperten-sion guidelines and the ALLHAT results acknowledge that most patients with hypertension will require two or more drugs to achieve target BP. JNC strongly suggests using diuretics in such regimens. In fact, inadequate use of diuretics is a known factor for “resistance” in control-ling BP.9 Under-utilization of diuretics as first-line therapy and as an overall percentage of prescriptions dispensed as antihypertensives is well documented.10–16 However, pat-terns of diuretic use specifically in regimens using multiple
O r i g i n a l P a p e r • C M E
Prescribing Patterns of Diuretics in Multi-Drug Antihypertensive Regimens
Hardeep Singh, MD, MPH;1,2 Michael L. Johnson, PhD1,3
From the Michael E. DeBakey Veterans Affairs Medical Center, Houston, TX;1 and Department of Medicine, Baylor College of Medicine, Houston, TX;2 Houston Center for Quality of Care and Utilization Studies, Section of Health Services Research, Baylor College of Medicine, Houston, TX3
Address for correspondence:Hardeep Singh, MD, MPH, VA Medical Center (111PC), 2002 Holcombe Boulevard, Houston, TX 77030E-mail: [email protected] Manuscript received November 8, 2004; revised December 2, 2004; accepted December 7, 2004
www.lejacq.com ID: 3922
The Journal of Clinical Hypertension (ISSN 1524-6175) is published monthly by Le Jacq Ltd., Three Parklands Drive, Darien, CT 06820-3652. Copyright ©2005 by Le Jacq Ltd., All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recording, or any information storage and retrieval system, without permission in writing from the publishers. The opinions and ideas expressed in this publication are those of the authors and do not necessarily reflect those of the Editors or Publisher. For copies in excess of 25 or for commercial purposes, please contact Sarah Howell at [email protected] or 203.656.1711 x106.

THE JOURNAL OF CLINICAL HYPERTENSION VOL. 7 NO. 2 FEBRUARY 200582
drugs have not been well studied. We undertook a study to determine utilization of diuretics, including thiazides, in patients receiving multiple drugs for hypertension, and to examine patterns of utilization of these drugs in sub-sets of special populations (elderly and African-American patients). We further tested the association of diuretic use with BP control.
METHODSStudy DesignA cross-sectional retrospective design was employed to estimate the patterns of use of antihypertensive agents in a cohort of hypertensive patients as of March 1, 2001.
Data SourcesComputerized demographic and clinical data were obtained from one of the largest medical centers of the Department of Veterans Affairs (VA). All data were transferred over the VA intranet from the regional net-work data warehouse computer system to the study team for analysis. All aspects of the study protocol, including access and use of the computerized patient clinical infor-mation, were authorized by the local Institutional Review Board and Michael E. DeBakey, VA Medical Center Research and Development review committee.
Inclusion and Exclusion CriteriaPatients were identified as having hypertension based on previous research, described in detail elsewhere.17,18 Briefly, all inpatients and outpatients seen from October 1, 1998 to March 1, 2001 were screened and classified as having hypertension based on diagnostic information in the form of International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes, pre-scription drug use from pharmacy dispensing records, and diagnostic information or elevated BP readings.
Patients were classified as having hypertension if they met any of the following definitions: 1) At least two out-patient diagnoses of hypertension; 2) at least one prescrip-tion of antihypertensive drug plus at least one outpatient diagnosis of hypertension; 3) at least one prescription of antihypertensive drug plus at least one elevated BP; 4) at least one elevated BP measurement plus one outpatient diagnosis of hypertension; or 5) at least two elevated BP measurements. We excluded patients with chronic heart failure (CHF), since many of these patients were receiving loop diuretics and the focus of our study was the thiazide diuretics. Additionally, the presence of compelling indica-tions to use other drugs such as angiotensin-converting enzyme (ACE) inhibitors and β blockers in the setting of CHF would have complicated our analysis and may have made it less meaningful. We also excluded diabetics for a separate analysis since JNC VI guidelines included several agents in addition to diuretics.8 Inclusion of these
two conditions, where other medications might have been preferred could allow for lower rates of thiazide utilization. Our focus was mostly on “diuretic eligible” patients, where the practitioners had compelling reasons to include diuretics (especially thiazides) in prescribing regimens and where preferred use of other agents could not be easily justified. Thus, patients with any record of an inpatient or outpatient diagnosis of diabetes or CHF were excluded.
Treatment PatternsPrescription fills of any antihypertensive drugs between the November 1, 2000 and March 1, 2001 were iden-tified from the computerized pharmacy records. We used a 4-month period to ensure capture of 90-day fills before March 1, 2001. The number of antihypertensive drugs being prescribed was tabulated. Patients with any thiazide, loop diuretic, or other diuretic use (diuretics in combination with other drugs) were classified as hav-ing any diuretic use. The proportion of patients with any diuretic use, and use of the other antihypertensive drug classes, among patients with two, three, four, or more drugs was cross-tabulated. Included were α and β blockers, calcium channel blockers, ACE inhibitors, angiotensin receptor blockers, combination drugs, and a category of other antihypertensives (methyldopa, reserpine, clonidine, hydralazine, and minoxidil). We determined the specific diuretic agents and dose levels prescribed. We also tabulated the proportions of sepa-rate diuretic categories for African-American patients, patients ≥65 years of age, and among all patients based on the most recent serum creatinine level recorded.
BP ControlWe determined whether patients were at controlled BP lev-els at the most recent measurement recorded. Controlled BP was defined as <140/90 mm Hg, or <130/85 mm Hg in patients with certain comorbid conditions.18
AnalysisWe present the patterns of use of antihypertensive drugs, especially diuretics among all patients and in subgroups of patients on two, three, four, or more drugs. We compared the rates of diuretic use among African-American patients and elderly patients (≥65 years) with the overall population, and compared rates of diuretic use separately among patients with creatinine <2.0 mg/dL compared with patients with creatinine ≥2.0 mg/dL. To specifically assess the use of thiazide diuretics, which was one of the main goals of the study, we used a creatinine level ≥2.0 mg/dL to exclude patients who may not benefit from these class-es of drugs based on the ALLHAT exclusion criteria.19 Proportions were tested by the normal approximation
The Journal of Clinical Hypertension (ISSN 1524-6175) is published monthly by Le Jacq Ltd., Three Parklands Drive, Darien, CT 06820-3652. Copyright ©2005 by Le Jacq Ltd., All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recording, or any information storage and retrieval system, without permission in writing from the publishers. The opinions and ideas expressed in this publication are those of the authors and do not necessarily reflect those of the Editors or Publisher. For copies in excess of 25 or for commercial purposes, please contact Sarah Howell at [email protected] or 203.656.1711 x106.
VOL. 7 NO. 2 FEBRUARY 2005 THE JOURNAL OF CLINICAL HYPERTENSION 83
to the binomial. Finally, we tested the association of diuretic use with controlled BP by the chi-square test.
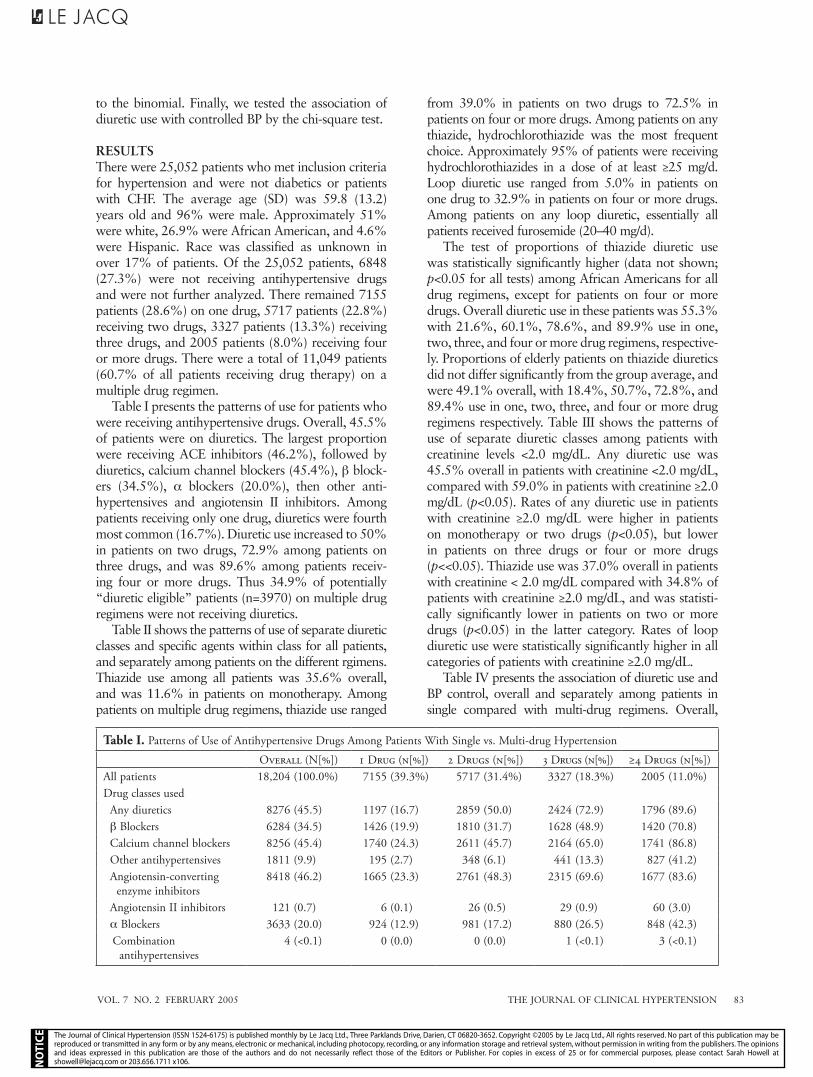
RESULTSThere were 25,052 patients who met inclusion criteria for hypertension and were not diabetics or patients with CHF. The average age (SD) was 59.8 (13.2) years old and 96% were male. Approximately 51% were white, 26.9% were African American, and 4.6% were Hispanic. Race was classified as unknown in over 17% of patients. Of the 25,052 patients, 6848 (27.3%) were not receiving antihypertensive drugs and were not further analyzed. There remained 7155 patients (28.6%) on one drug, 5717 patients (22.8%) receiving two drugs, 3327 patients (13.3%) receiving three drugs, and 2005 patients (8.0%) receiving four or more drugs. There were a total of 11,049 patients (60.7% of all patients receiving drug therapy) on a multiple drug regimen.
Table I presents the patterns of use for patients who were receiving antihypertensive drugs. Overall, 45.5% of patients were on diuretics. The largest proportion were receiving ACE inhibitors (46.2%), followed by diuretics, calcium channel blockers (45.4%), β block-ers (34.5%), α blockers (20.0%), then other anti-hypertensives and angiotensin II inhibitors. Among patients receiving only one drug, diuretics were fourth most common (16.7%). Diuretic use increased to 50% in patients on two drugs, 72.9% among patients on three drugs, and was 89.6% among patients receiv-ing four or more drugs. Thus 34.9% of potentially “diuretic eligible” patients (n=3970) on multiple drug regimens were not receiving diuretics.
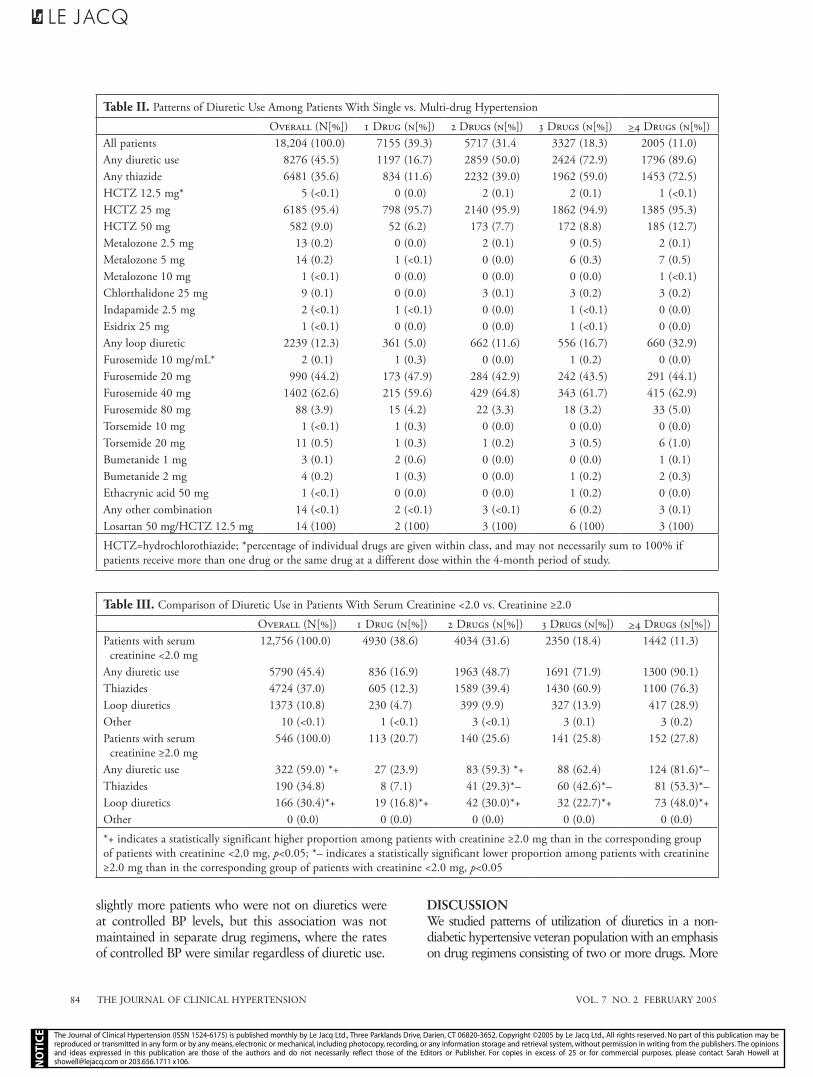
Table II shows the patterns of use of separate diuretic classes and specific agents within class for all patients, and separately among patients on the different rgimens. Thiazide use among all patients was 35.6% overall, and was 11.6% in patients on monotherapy. Among patients on multiple drug regimens, thiazide use ranged
from 39.0% in patients on two drugs to 72.5% in patients on four or more drugs. Among patients on any thiazide, hydrochlorothiazide was the most frequent choice. Approximately 95% of patients were receiving hydrochlorothiazides in a dose of at least ≥25 mg/d. Loop diuretic use ranged from 5.0% in patients on one drug to 32.9% in patients on four or more drugs. Among patients on any loop diuretic, essentially all patients received furosemide (20–40 mg/d).
The test of proportions of thiazide diuretic use was statistically significantly higher (data not shown; p<0.05 for all tests) among African Americans for all drug regimens, except for patients on four or more drugs. Overall diuretic use in these patients was 55.3% with 21.6%, 60.1%, 78.6%, and 89.9% use in one, two, three, and four or more drug regimens, respective-ly. Proportions of elderly patients on thiazide diuretics did not differ significantly from the group average, and were 49.1% overall, with 18.4%, 50.7%, 72.8%, and 89.4% use in one, two, three, and four or more drug regimens respectively. Table III shows the patterns of use of separate diuretic classes among patients with creatinine levels <2.0 mg/dL. Any diuretic use was 45.5% overall in patients with creatinine <2.0 mg/dL, compared with 59.0% in patients with creatinine ≥2.0 mg/dL (p<0.05). Rates of any diuretic use in patients with creatinine ≥2.0 mg/dL were higher in patients on monotherapy or two drugs (p<0.05), but lower in patients on three drugs or four or more drugs (p<<0.05). Thiazide use was 37.0% overall in patients with creatinine < 2.0 mg/dL compared with 34.8% of patients with creatinine ≥2.0 mg/dL, and was statisti-cally significantly lower in patients on two or more drugs (p<0.05) in the latter category. Rates of loop diuretic use were statistically significantly higher in all categories of patients with creatinine ≥2.0 mg/dL.
Table IV presents the association of diuretic use and BP control, overall and separately among patients in single compared with multi-drug regimens. Overall,
Table I. Patterns of Use of Antihypertensive Drugs Among Patients With Single vs. Multi-drug Hypertension
OVERALL (N[%]) 1 DRUG (N[%]) 2 DRUGS (N[%]) 3 DRUGS (N[%]) ≥4 DRUGS (N[%])All patients 18,204 (100.0%) 7155 (39.3%) 5717 (31.4%) 3327 (18.3%) 2005 (11.0%)Drug classes used
Any diuretics 8276 (45.5) 1197 (16.7) 2859 (50.0) 2424 (72.9) 1796 (89.6)β Blockers 6284 (34.5) 1426 (19.9) 1810 (31.7) 1628 (48.9) 1420 (70.8)Calcium channel blockers 8256 (45.4) 1740 (24.3) 2611 (45.7) 2164 (65.0) 1741 (86.8)Other antihypertensives 1811 (9.9) 195 (2.7) 348 (6.1) 441 (13.3) 827 (41.2)Angiotensin-converting
enzyme inhibitors8418 (46.2) 1665 (23.3) 2761 (48.3) 2315 (69.6) 1677 (83.6)
Angiotensin II inhibitors 121 (0.7) 6 (0.1) 26 (0.5) 29 (0.9) 60 (3.0)α Blockers 3633 (20.0) 924 (12.9) 981 (17.2) 880 (26.5) 848 (42.3)Combination
antihypertensives4 (<0.1) 0 (0.0) 0 (0.0) 1 (<0.1) 3 (<0.1)
The Journal of Clinical Hypertension (ISSN 1524-6175) is published monthly by Le Jacq Ltd., Three Parklands Drive, Darien, CT 06820-3652. Copyright ©2005 by Le Jacq Ltd., All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recording, or any information storage and retrieval system, without permission in writing from the publishers. The opinions and ideas expressed in this publication are those of the authors and do not necessarily reflect those of the Editors or Publisher. For copies in excess of 25 or for commercial purposes, please contact Sarah Howell at [email protected] or 203.656.1711 x106.
THE JOURNAL OF CLINICAL HYPERTENSION VOL. 7 NO. 2 FEBRUARY 200584
slightly more patients who were not on diuretics were at controlled BP levels, but this association was not maintained in separate drug regimens, where the rates of controlled BP were similar regardless of diuretic use.
DISCUSSIONWe studied patterns of utilization of diuretics in a non-diabetic hypertensive veteran population with an emphasis on drug regimens consisting of two or more drugs. More
Table II. Patterns of Diuretic Use Among Patients With Single vs. Multi-drug Hypertension
OVERALL (N[%]) 1 DRUG (N[%]) 2 DRUGS (N[%]) 3 DRUGS (N[%]) >4 DRUGS (N[%])All patients 18,204 (100.0) 7155 (39.3) 5717 (31.4 3327 (18.3) 2005 (11.0)Any diuretic use 8276 (45.5) 1197 (16.7) 2859 (50.0) 2424 (72.9) 1796 (89.6)Any thiazide 6481 (35.6) 834 (11.6) 2232 (39.0) 1962 (59.0) 1453 (72.5)HCTZ 12.5 mg* 5 (<0.1) 0 (0.0) 2 (0.1) 2 (0.1) 1 (<0.1)HCTZ 25 mg 6185 (95.4) 798 (95.7) 2140 (95.9) 1862 (94.9) 1385 (95.3)HCTZ 50 mg 582 (9.0) 52 (6.2) 173 (7.7) 172 (8.8) 185 (12.7)Metalozone 2.5 mg 13 (0.2) 0 (0.0) 2 (0.1) 9 (0.5) 2 (0.1)Metalozone 5 mg 14 (0.2) 1 (<0.1) 0 (0.0) 6 (0.3) 7 (0.5)Metalozone 10 mg 1 (<0.1) 0 (0.0) 0 (0.0) 0 (0.0) 1 (<0.1)Chlorthalidone 25 mg 9 (0.1) 0 (0.0) 3 (0.1) 3 (0.2) 3 (0.2)Indapamide 2.5 mg 2 (<0.1) 1 (<0.1) 0 (0.0) 1 (<0.1) 0 (0.0)Esidrix 25 mg 1 (<0.1) 0 (0.0) 0 (0.0) 1 (<0.1) 0 (0.0)Any loop diuretic 2239 (12.3) 361 (5.0) 662 (11.6) 556 (16.7) 660 (32.9)Furosemide 10 mg/mL* 2 (0.1) 1 (0.3) 0 (0.0) 1 (0.2) 0 (0.0)Furosemide 20 mg 990 (44.2) 173 (47.9) 284 (42.9) 242 (43.5) 291 (44.1)Furosemide 40 mg 1402 (62.6) 215 (59.6) 429 (64.8) 343 (61.7) 415 (62.9)Furosemide 80 mg 88 (3.9) 15 (4.2) 22 (3.3) 18 (3.2) 33 (5.0)Torsemide 10 mg 1 (<0.1) 1 (0.3) 0 (0.0) 0 (0.0) 0 (0.0)Torsemide 20 mg 11 (0.5) 1 (0.3) 1 (0.2) 3 (0.5) 6 (1.0)Bumetanide 1 mg 3 (0.1) 2 (0.6) 0 (0.0) 0 (0.0) 1 (0.1)Bumetanide 2 mg 4 (0.2) 1 (0.3) 0 (0.0) 1 (0.2) 2 (0.3)Ethacrynic acid 50 mg 1 (<0.1) 0 (0.0) 0 (0.0) 1 (0.2) 0 (0.0)Any other combination 14 (<0.1) 2 (<0.1) 3 (<0.1) 6 (0.2) 3 (0.1)Losartan 50 mg/HCTZ 12.5 mg 14 (100) 2 (100) 3 (100) 6 (100) 3 (100)
HCTZ=hydrochlorothiazide; *percentage of individual drugs are given within class, and may not necessarily sum to 100% if patients receive more than one drug or the same drug at a different dose within the 4-month period of study.
Table III. Comparison of Diuretic Use in Patients With Serum Creatinine <2.0 vs. Creatinine ≥2.0
OVERALL (N[%]) 1 DRUG (N[%]) 2 DRUGS (N[%]) 3 DRUGS (N[%]) >4 DRUGS (N[%])Patients with serum
creatinine <2.0 mg12,756 (100.0) 4930 (38.6) 4034 (31.6) 2350 (18.4) 1442 (11.3)
Any diuretic use 5790 (45.4) 836 (16.9) 1963 (48.7) 1691 (71.9) 1300 (90.1)Thiazides 4724 (37.0) 605 (12.3) 1589 (39.4) 1430 (60.9) 1100 (76.3)Loop diuretics 1373 (10.8) 230 (4.7) 399 (9.9) 327 (13.9) 417 (28.9)Other 10 (<0.1) 1 (<0.1) 3 (<0.1) 3 (0.1) 3 (0.2)Patients with serum
creatinine ≥2.0 mg546 (100.0) 113 (20.7) 140 (25.6) 141 (25.8) 152 (27.8)
Any diuretic use 322 (59.0) *+ 27 (23.9) 83 (59.3) *+ 88 (62.4) 124 (81.6)*–Thiazides 190 (34.8) 8 (7.1) 41 (29.3)*– 60 (42.6)*– 81 (53.3)*–Loop diuretics 166 (30.4)*+ 19 (16.8)*+ 42 (30.0)*+ 32 (22.7)*+ 73 (48.0)*+Other 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0)
*+ indicates a statistically significant higher proportion among patients with creatinine ≥2.0 mg than in the corresponding group of patients with creatinine <2.0 mg, p<0.05; *– indicates a statistically significant lower proportion among patients with creatinine ≥2.0 mg than in the corresponding group of patients with creatinine <2.0 mg, p<0.05
The Journal of Clinical Hypertension (ISSN 1524-6175) is published monthly by Le Jacq Ltd., Three Parklands Drive, Darien, CT 06820-3652. Copyright ©2005 by Le Jacq Ltd., All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recording, or any information storage and retrieval system, without permission in writing from the publishers. The opinions and ideas expressed in this publication are those of the authors and do not necessarily reflect those of the Editors or Publisher. For copies in excess of 25 or for commercial purposes, please contact Sarah Howell at [email protected] or 203.656.1711 x106.

VOL. 7 NO. 2 FEBRUARY 2005 THE JOURNAL OF CLINICAL HYPERTENSION 85
than one third of all patients on multi-drug regimens (34.9%) were not receiving any diuretics, although they were potentially eligible for them based on our criteria. Overall, thiazide diuretics remained underused in multi-drug regimens despite good evidence for their use and tolerability. Furthermore, in a subgroup analysis of patients >65 years of age (elderly population), diuretic use did not differ. Diuretic use was higher in African Americans, although overall use was still relatively low, especially in one- and two-drug regimens. These data suggest more emphasis on diuretic use in the more vulnerable elderly and African-American populations. In our limited analysis, diuretic-based regimens had similar levels of BP control as other regimens. Nevertheless, due to many reasons includ-ing a well-demonstrated reduction in both cerebrovascular and cardiovascular morbidity in numerous trials, low cost, and a synergistic effect on BP reduction when used in combination with most drugs, the inclusion of diuretics in multi-drug regimens should be strongly advocated.
Current hypertension guidelines and randomized clini-cal trials have identified the need for multi-drug regimens to control BP to target levels.20,21 In the recent ALLHAT trial, 63% of patients were receiving two or more drugs after 5 years of follow-up. The use of diuretics in multi-drug regimens has been increasingly recognized as essen-tial for BP control in many patients with hypertension, due to their ability to decrease blood volume and reduce vascular resistance.22 The JNC VI and JNC 7 reports note that volume overload due to inadequate diuretic therapy is one of the most common reasons for resistance to hypertension treatment.2,8 More than one half of these “resistant” patients can be controlled by either adjust-ment of the antihypertensive regimen or the addition of a diuretic.23 Data from several clinical trials have demon-strated that the use of low-dose diuretics has a synergistic effect on BP reduction when used in combination with most drugs.2,24 Using our exclusion criteria in this study population, a majority of the patients were considered eligible for a diuretic, at least as add-on therapy, if not an initial choice. There was more than an expected utiliza-tion of loop diuretics as compared with thiazides to treat hypertension regardless of renal function. We could not fully explain this pattern; we expected patients without evidence of CHF and a normal or mildly elevated creati-nine level (<2 mg/dL based on the ALLHAT criteria) to be on thiazides rather than loop diuretics because of the
better antihypertensive effects of thiazides. Perhaps con-comitant edema or other thiazide contraindications might account for this pattern, but further analysis of these fac-tors was beyond the scope of our study. Most patients who were on thiazides were on an appropriate dose. A significant proportion of people on loop diuretics were only on 20 mg/d. Thus, loop diuretics seem to be utilized for antihypertensive treatment with possibly ineffective doses. Another observation was that of low utilization of combination diuretic regimens (n=18), which may be partly explained by local formulary restrictions on some of these drugs at that time. At the present time, β blocker/ or ACE inhibitor/diuretic combination drugs are easily available on the local formulary. The use of angiotensin receptor blockers was minimal at the time of the analysis, since they were not on the VA drug formulary. The obser-vation of frequent use of α blockers was explained by the high prevalence of benign prostatic hyperplasia in our population (this was before the results of the ALLHAT study). Notably, about 20% of patients were on β block-ers as recommended by JNC VI for monotherapy.
We believe that our study is one of few to highlight under-utilization of diuretics, specifically thiazides, in multi-drug regimens. A number of previous studies have noted the trends in antihypertensive drug therapy during the 1990s and concluded that prescriptions of diuretics were inadequate as compared with other agents; physicians’ prescribing patterns did not con-form to the JNC guidelines.11–15 However, two recent VA studies showed an increase in the use of thiazide diuretics in the late 1990s.25,26 These studies assessed aggregate proportions of prescriptions or percentages of patients receiving each class of drugs over time and not specifically diuretic use in multi-drug regimens, which was the main objective of our study. In addition to the prescription volume for various antihypertensive drug classes, our data characterize specific prescribing for patients; for example, percentage of patients on three drugs who are taking a diuretic. Our data actually suggest an increase in diuretic use as monotherapy and overall utilization rates of diuretics as compared with a previous VA study.26 This could imply that practitioners are more adherent to guidelines than before and have, in fact, increased their use of diuretics over the years. With this continued upward trend, we may be able to see further improved utilization rates in the future.
Table IV. Diuretic Use and Blood Pressure (BP) Control
OVERALL 1 DRUG 2 DRUGS 3 DRUGS >4 DRUGSAmong patients on diuretics at BP control (%) 34.6 42.3 36.9 33.0 28.3Among patients not on diuretics at BP control (%) 39.3* 41.5 36.9 34.5 30.6
*statistically significantly higher proportion of overall patients not on thiazides at BP control compared with overall patients on diuretics at BP control; p<0.001
The Journal of Clinical Hypertension (ISSN 1524-6175) is published monthly by Le Jacq Ltd., Three Parklands Drive, Darien, CT 06820-3652. Copyright ©2005 by Le Jacq Ltd., All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recording, or any information storage and retrieval system, without permission in writing from the publishers. The opinions and ideas expressed in this publication are those of the authors and do not necessarily reflect those of the Editors or Publisher. For copies in excess of 25 or for commercial purposes, please contact Sarah Howell at [email protected] or 203.656.1711 x106.

THE JOURNAL OF CLINICAL HYPERTENSION VOL. 7 NO. 2 FEBRUARY 200586
Previous VA cooperative studies have shown that thia-zide diuretics were more effective in older patients and had a greater effect on systolic BP reduction than other agents, i.e., β blockers, etc.27,28 Although studies have shown under-utilization of diuretics in the elderly, no study to our knowledge specifically examined multi-drug regimens in this population.13,29,30 African-American patients have a higher prevalence of stage 3 hyperten-sion and many require multi-drug therapy. According to JNC VI and 7, diuretics should be either used as first line therapy or combined with other agents to improve response. Previous studies have reported nonadherence to JNC guidelines for initial monotherapy and in combina-tion regimens in the treatment of African Americans.29,31 However, both the studies were limited by a small sample size. A more recent study also found that African Americans were less likely to use diuretics, but did not analyze their use in multi-drug regimens separately.11
Possible Reasons for Underutilization of DiureticsCould the inadequate use of diuretics be explained by high rates of intolerance to these drugs? JNC recom-mendations were based on the demonstration of a high level of patient tolerability on diuretics with a majority of patients remaining free of symptoms or adverse effects; this fact was corroborated by other studies.32–34 Although their metabolic side effects are significantly reduced when used in lower doses, practitioners may still hesitate to use diuretics.24,28 Although we did not have exact laboratory values and allergy information, we assessed our study sample for ICD-9 codes for hypokalemia, hyponatremia, electro-lyte imbalance, orthostatic hypotension, sulfonamide allergy, and adverse therapeutic effect of diuretics. On this limited analysis, these factors in combination were present in a total of 554 patients (3.0%); 228 patients of the 9928 patients not on diuretics (2.3%) had these conditions. Rates of discontinuation of thiazide diuret-ics in the Systolic Hypertension of the Elderly (SHEP)33 trial were only about 15%−20% at 1 year. Allowing for about a 15%−20% discontinuation rate due to adverse effects, we still could not account for some of the thiazide utilization rates seen in two- and three-drug regimens. This is unlikely to be due to lack of knowledge because previous studies have shown that there is a high awareness of JNC guidelines among practitioners.35 Some of the reasons given by Moser24 that apply to our setting may include the widespread overemphasis on the possible, but unproven, problems with diuretics. With increasing recognition of the need for multi-drug combinations to reach goal BP and the findings from ALLHAT, there should be a rigorous assessment of prescribing patterns in these regimens.
Although we found that BP control was actually higher overall among patients who were not on diuret-ics, this finding should be interpreted with caution. The finding did not hold up in separate categories of patients in single vs. multi-drug regimens, where the rates of BP control were similar. The statistical significance was most likely due to the large sample size affecting the chi-square test. The association was also unadjusted for an array of potential confounding factors, and more research would be necessary to determine the unique affect of diuretic use on BP control.
Limitations of the StudyInterpretation of our results must be considered along with recognition of several limitations. First, our study is cross-sectional and cannot provide information on changing patterns of use reflecting the indications for prevalent vs. incident cases of hypertension. In addi-tion, because of the predominantly male population, the results cannot be generalized to women. We also did not analyze individual medical records to look for contraindications to the initiation or continuation of diuretics. Because our database required prescriptions to be filled within the VA system, prescriptions filled in the private sector would not be accounted for. However, because the medication co-pay was only $2 in the VA at the time of our study, we do not believe this to be a sig-nificant potential bias. In addition, we do not have any concomitant comparisons with the private sector, which could be revealing for better or worse utilization rates. Hence, our findings underscore the need for larger stud-ies addressing use of diuretics in multi-drug regimens in more diverse health care settings. Such studies should also aim to understand complexities of prescribing behavior and address why thiazides did not find their place as therapeutic agents in some of these regimens.
Our study suggests a room for improvement in the utilization of diuretics, especially thiazides, in multi-drug regimens for hypertension.. In light of recent guidelines and trials suggesting the need for multiple drugs to achieve goal BP, new strategies to maximize thiazide diuretic use in such regimens along with appli-cation of recommendations to avoid clinical inertia in this setting may lead to better hypertension control.36
Disclosure and Acknowledgment: This project was supported in part by a grant from Pfizer, Inc., and by the Department of Veterans Affairs Health Services Research and Development Service. The views expressed in this article are those of the authors and do not necessarily represent the views of the Department of Veterans Affairs. The authors wish to acknowledge the support of the Veterans Integrated Service Network (VISN 16) data ware-house team, Susan Pendergrass, DrPH (Deputy Director, VISN 16) and Jack Bates (Data warehouse administrator). The authors also thank Raji Sundaravaradan and Louise Henderson for computer analysis assistance and Donna Espadas for editorial assistance in the preparation of this manuscript. Dr. Johnson is a VA career development awardee (Merit Review Entry Program).
The Journal of Clinical Hypertension (ISSN 1524-6175) is published monthly by Le Jacq Ltd., Three Parklands Drive, Darien, CT 06820-3652. Copyright ©2005 by Le Jacq Ltd., All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recording, or any information storage and retrieval system, without permission in writing from the publishers. The opinions and ideas expressed in this publication are those of the authors and do not necessarily reflect those of the Editors or Publisher. For copies in excess of 25 or for commercial purposes, please contact Sarah Howell at [email protected] or 203.656.1711 x106.
VOL. 7 NO. 2 FEBRUARY 2005 THE JOURNAL OF CLINICAL HYPERTENSION 87
REFERENCES 1 Cherry DK, Burt CW, Woodwell DA. National Ambulatory
Medical Care Survey: 2001 summary. Adv Data. 2003;1–44. 2 The Seventh Report of the Joint National Committee on
Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA. 2003;289:2560–2572.
3 Yu W, Ravelo AL. The cost of common chronic diseases in the VA health care system. Abstract presented at VA Research and Development Service annual meeting Feb.13–15, 2002.
4 Alexander M, Tekawa I, Hunkeler E, et al. Evaluating hypertension control in a managed care setting. Arch Intern Med. 1999;159:2673–2677.
5 Berlowitz DR, Ash AS, Hickey EC, et al. Inadequate man-agement of blood pressure in a hypertensive population. N Engl J Med. 1998;339:1957–1963.
6 Borzecki AM, Wong AT, Hickey EC, et al. Hypertension control: how well are we doing? Arch Intern Med. 2003;163:2705–2711.
7 Major outcomes in high-risk hypertensive patients random-ized to angiotensin-converting enzyme inhibitor or calcium channel blocker vs diuretic: The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT). JAMA. 2002;288:2981–2997.
8 The sixth report of the Joint National Committee on pre-vention, detection, evaluation, and treatment of high blood pressure. Arch Intern Med. 1997;157:2413–2446.
9 Setaro JF, Black HR. Refractory hypertension. N Engl J Med. 1992;327:543–547.
10 Clause SL, Hamilton RA. Medicaid prescriber compliance with Joint National Committee VI Hypertension Treatment Guidelines. Ann Pharmacother. 2002;36:1505–1511.
11 Guo JD, Liu GG, Christensen DB, et al. How well have practices followed guidelines in prescribing antihyper-tensive drugs: the role of health insurance. Value Health. 2003;6:18–28.
12 Manolio TA, Cutler JA, Furberg CD, et al. Trends in pharmacologic management of hypertension in the United States. Arch Intern Med. 1995;155:829–837.
13 Psaty BM, Manolio TA, Smith NL, et al. Time trends in high blood pressure control and the use of antihypertensive medications in older adults: the Cardiovascular Health Study. Arch Intern Med. 2002;162:2325–2332.
14 Schulman KA, Mehta SS, Gersh BJ, et al. Study of Hypertensive Prescribing Practices (SHyPP): A National Survey of Primary Care Physicians. J Clin Hypertens. (Greenwich) 1999;2:106–114.
15 Siegel D, Lopez J. Trends in antihypertensive drug use in the United States: do the JNC V recommendations affect prescribing? Fifth Joint National Commission on the Detection, Evaluation, and Treatment of High Blood Pressure. JAMA. 1997;278:24:1745–1748.
16 Weiss R, Buckley K, Clifford T. Changing patterns of initial drug therapy for the treatment of hypertension in a Medicaid population, 1997–2000. Clin Ther. 2002;1451–1462.
17 Johnson ML, Pietz K, Battleman DS, et al. Prevalence of comorbid hypertension and dyslipidemia and associated cardiovascular disease in the Veterans Affairs healthcare system, provisionally accepted. Am J Manag Care. 2004; 10:1926–1932.
18 Selby JV, Peng T, Karter AJ, et al. High rates of co-occur-rence of hypertension, elevated low-density lipoprotein cholesterol, and diabetes mellitus in a large managed care
population. Am J Manag Care. 2004;10(part 2):163–170. 19 Davis BR, Cutler JA, Gordon DJ. et al. Rationale and design
for the Antihypertensive and Lipid Lowering Treatment to Prevent Heart Attack Trial (ALLHAT). ALLHAT Research Group. Am J Hypertens. 1996;4:342–360.
20 Hansson L, Zanchetti A, Carruthers SG, et al. Effects of intensive blood-pressure lowering and low-dose aspirin in patients with hypertension: principal results of the Hypertension Optimal Treatment (HOT) randomised trial. HOT Study Group. Lancet. 1998;351:1755–1762,
21 Pool JL. Is it time to move to multidrug combinations? Am J Hypertens. 2003;16:36–40.
22 Kaplan NM. Diuretics as a basis of antihypertensive thera-py. An overview. Drugs. 2000;59(suppl 2):21–25.
23 Giles TD, Sander GE. Beyond the usual strategies for blood pressure reduction: therapeutic considerations and combination therapies. J Clin Hypertens. (Greenwich) 2001;3:346–53.
24 Moser M. Why are physicians not prescribing diuret-ics more frequently in the management of hypertension? JAMA. 1998;279:1813–1816.
25 Carter BL, Malone DC, Ellis SL, et al. Antihypertensive drug utilization in hypertensive veterans with complex medication profiles. J Clin Hypertens. (Greenwich) 2000;172–180.
26 Siegel D, Lopez J, Meier J, et al. Changes in the phar-macologic treatment of hypertension in the Department of Veterans Affairs 1997–1999: decreased use of calcium antagonists and increased use of beta-blockers and thiazide diuretics. Am J Hypertens. 2001;957–962.
27 Freis ED. Age and antihypertensive drugs (hydrochloro-thiazide, bendroflumethiazide, nadolol and captopril). Am J Cardiol. 1988;61:117–21.
28 Flack JM, Cushman WC. Evidence for the efficacy of low-dose diuretic monotherapy. Am J Med. 1996;101:53S–60S.
29 Mehta SS, Wilcox CS, Schulman KA. Treatment of hyper-tension in patients with comorbidities: results from the study of hypertensive prescribing practices (SHyPP). Am J Hypertens. 1999;12:333–340.
30 Knight EL, Glynn RJ, Levin R, et al. Failure of evidence-based medicine in the treatment of hypertension in older patients. J Gen Intern Med. 2000;10:702–709.
31 Henderson SO, Bretsky P, DeQuattro V, et al. Treatment of hypertension in African Americans and Latinos: the effect of JNC VI on urban prescribing practices. J Clin Hypertens (Greenwich). 2003;5:107–112.
32 Neaton JD, Grimm RH Jr, Prineas RJ, et al. Treatment of Mild Hypertension Study. Final results. Treatment of Mild Hypertension Study Research Group. JAMA. 1993;270:713–724.
33 Prevention of stroke by antihypertensive drug treatment in older persons with isolated systolic hypertension. Final results of the Systolic Hypertension in the Elderly Program (SHEP). SHEP Cooperative Research Group. JAMA. 1991;265:3255–64.
34 Materson BJ, Reda DJ, Cushman WC, et al. Single-drug therapy for hypertension in men. A comparison of six antihy-pertensive agents with placebo. The Department of Veterans Affairs Cooperative Study Group on Antihypertensive Agents. N Engl J Med. 1993;330:914–21.
35 Oliveria SA, Lapuerta P, McCarthy BD, et al. Physician-related barriers to the effective management of uncon-trolled hypertension. Arch Intern Med. 2002;413–420.
36 Phillips LS, Branch WT, Cook CB, et al. Clinical inertia. Ann Intern Med. 2001;135:825–834.
The Journal of Clinical Hypertension (ISSN 1524-6175) is published monthly by Le Jacq Ltd., Three Parklands Drive, Darien, CT 06820-3652. Copyright ©2005 by Le Jacq Ltd., All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recording, or any information storage and retrieval system, without permission in writing from the publishers. The opinions and ideas expressed in this publication are those of the authors and do not necessarily reflect those of the Editors or Publisher. For copies in excess of 25 or for commercial purposes, please contact Sarah Howell at [email protected] or 203.656.1711 x106.

THE JOURNAL OF CLINICAL HYPERTENSION VOL. 7 NO. 2 FEBRUARY 200588
INSTRUCTIONS FOR COMPLETING THIS FORM: Read the selected paper and answer all the questions that follow. After each question there is a series of possibly correct answers. Please select the one best answer for each and place your selection on the answer grid. YOU MUST ALSO COMPLETE THE CME EVALUATION SECTION and return the form within 6 months of the paper’s publication to receive credit. Letters of credit will be mailed to participants biannually.
ACCREDITATION STATEMENT: Winthrop-University Hospital (WUH) is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to sponsor continuing medical education for physicians. WUH designates this Continuing Medical Education activity for a maximum of (1) credit hour in Category 1 credit towards the AMA Physicians’ Recognition Award. Each physi-cian should claim only those hours of credit that he/she actually spent on the educational activity. WUH relies upon faculty participants in its CME programs to provide educational information that is objective and as free of bias as possible. In this spirit, and in accordance with the guidelines of the program sponsor, faculty participants are expected to indicate any commercial relationship that might be per-ceived as a real or apparent conflict of interest.
OBJECTIVE AND TARGET AUDIENCE: All primary care physicians and cardiologists are eligible to receive credit. At the conclusion of this activity, participants should be able to: 1) summarize the important points discussed in the paper reviewed; 2) identify patients to whom the paper is relevant; 3) modify management practices as new information is learned; and 4) identify deficiencies in their knowledge base.
1. Which one of the following was not a goal of this study?A __To determine the utilization of diuretics in
antihypertensive regimensB __To examine the use of diuretics specifically
in the elderly and African-American popu-lations
C __To examine the financial implications of diuretic-based antihypertensive regimens
D __To test the association of diuretic use with blood pressure control
2. Which of the following statements regarding the study design is false?A __The study population was recruited from
multiple types of health care facilitiesB __Patients with congestive heart failure were
excludedC __Patients taking α blockers were includedD __Patients with diabetes were excluded
3. Which of the following statements regarding the results of the study is false?A __Approximately one half of the patients
were African AmericanB __Approximately 60% of the patients were
treated with two or more antihypertensive drugs
C __Overall, approximately 45% of the patients were receiving a diuretic
D __Diuretic use increased with the number of antihypertensive drugs the patients were taking
4. Which of the following statements regarding diuretic use in this study is false?A __The use of diuretics in African Americans
was generally higher than the general study population
B __Thiazide was the most common type of diuretic used
C __The use of diuretics in the elderly was sig-nificantly higher than in the general study population
D __Overall, more patients not on a diuretic achieved blood pressure control
5. Which of the following statements regarding the authors’ conclusions is false?A __Thiazide diuretics were underusedB __Diuretics were underused in the African-
American populationC __The results of this study cannot be gener-
alized to women or patients outside of the Department of Veterans Affairs system
D __The use of diuretics resulted in superior blood pressure control
CME QuestionsTodd C. Kerwin, MD, Section Editor, Winthrop Cardiology Associates, Mineola, NY
Please Select the One Best Answer for Each Question and Place Your Selection on the Answer Grid.
The Journal of Clinical Hypertension (ISSN 1524-6175) is published monthly by Le Jacq Ltd., Three Parklands Drive, Darien, CT 06820-3652. Copyright ©2005 by Le Jacq Ltd., All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recording, or any information storage and retrieval system, without permission in writing from the publishers. The opinions and ideas expressed in this publication are those of the authors and do not necessarily reflect those of the Editors or Publisher. For copies in excess of 25 or for commercial purposes, please contact Sarah Howell at [email protected] or 203.656.1711 x106.
VOL. 7 NO. 2 FEBRUARY 2005 THE JOURNAL OF CLINICAL HYPERTENSION 89
Answer the questions from the previous page by selecting the best choice of A, B, C, or D.
Questions: 1.__ 2.__ 3.__ 4.__ 5.__
Agree Disagree
1. My knowledge was enhanced by this activity. 1.__ 2.__ 3.__ 4.__ 5.__
2. The activity helped to clarify issues specific to hypertension patients. 1.__ 2.__ 3.__ 4.__ 5.__
3. The information obtained from this exercise will have an impact on my care of patients. 1.__ 2.__ 3.__ 4.__ 5.__
4. The format of the exercise was useful. 1.__ 2.__ 3.__ 4.__ 5.__
5. Suggestions for future topics:
CME Answer Grid
CME Evaluation
Please print all information. Please submit a $5 administrative fee in the form of a check
made out to the Office of Academic Affairs-WUH.
SEND TO:Office of Academic AffairsWinthrop-University Hospital259 First StreetMineola, NY 11501
Re: Singh H, Johnson ML. Prescribing patterns of diuretics in multi-drug antihypertensive regimens. J Clin Hypertens (Greenwich). 2005;7:81–89.
Name: ___________________________________________________________________________
Address: _________________________________________________________________________
________________________________________________________________________________
________________________________________________________________________________
Where To Send The Completed CME Form
The Journal of Clinical Hypertension (ISSN 1524-6175) is published monthly by Le Jacq Ltd., Three Parklands Drive, Darien, CT 06820-3652. Copyright ©2005 by Le Jacq Ltd., All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recording, or any information storage and retrieval system, without permission in writing from the publishers. The opinions and ideas expressed in this publication are those of the authors and do not necessarily reflect those of the Editors or Publisher. For copies in excess of 25 or for commercial purposes, please contact Sarah Howell at [email protected] or 203.656.1711 x106.