Embed Size (px)
Citation preview

Preparing for CNST Maternity Levels 1, 2 and 3:
Experience of the Liverpool Women’s Hospital
Helen Scholefield
Consultant Obstetrician & Lead for Clinical Risk Management

• Where are trusts now?
• Why separate maternity standards?
• Why aim higher
• Team approach
• The standards– Difficult level 1 criteria
– Level 2 & 3 criteria
– How we covered them
– Feedback from assessors where we could improve
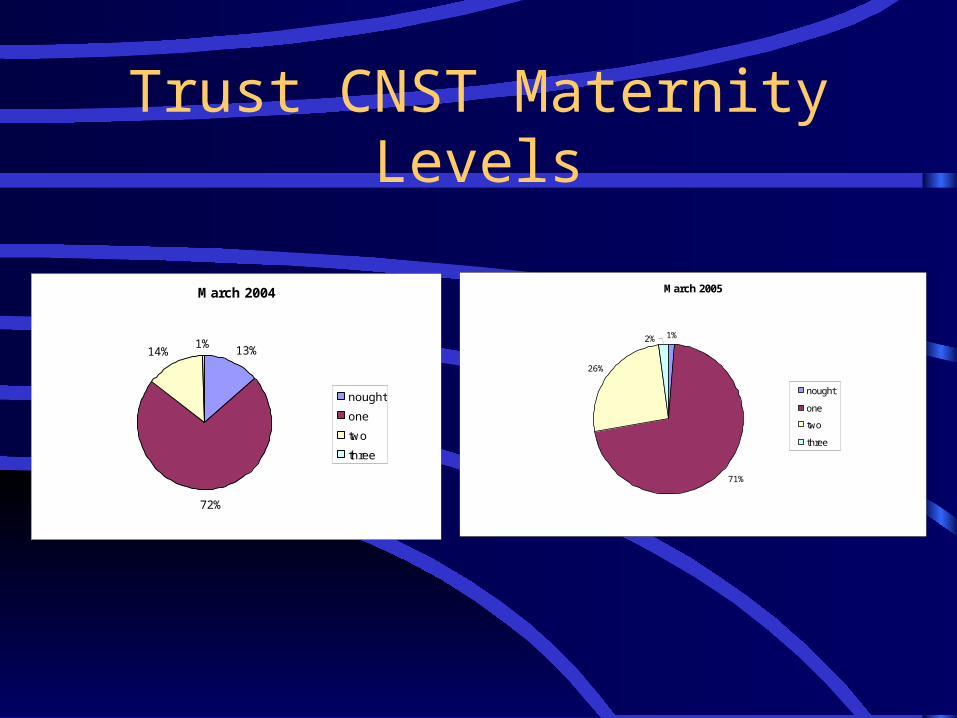
Trust CNST Maternity Levels
March 2005
1%
71%
26%
2%
nought
one
two
three
March 2004
13%
72%
14%1%
nought
one
two
three
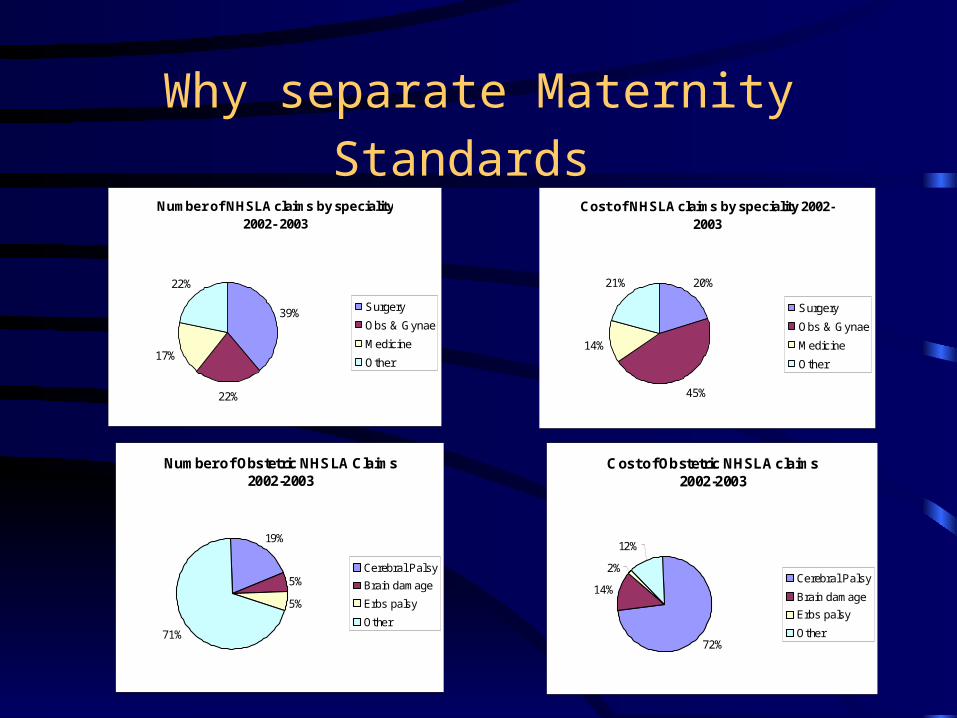
Why separate Maternity Standards
Number of Obstetric NHSLA Claims 2002-2003
19%
5%
5%
71%
Cerebral Palsy
Brain damage
Erbs palsy
Other
Cost of Obstetric NHSLA claims2002-2003
72%
14%
2%
12%
Cerebral Palsy
Brain damage
Erbs palsy
Other
Number of NHSLA claims by speciality 2002- 2003
39%
22%
17%
22%
Surgery
Obs & Gynae
Medicine
Other
Cost of NHSLA claims by speciality 2002-2003
20%
45%
14%
21%
Surgery
Obs & Gynae
Medicine
Other

Organisation with a Memory 2000
• Reduce risk in Obstetrics by 25% by 2005

8 standards
• Organisation• Learning from experience• Communication• Clinical Care• Induction, Training and competence• Health records• Implementation of CRM• Staffing levels

Incentives for achieving higher levels
• Improve safety for patients
• Staff ,ownership of CRM through training, teamwork, avoid being second victim of error, sense of shared achievement
• Financial- 1.7 million saving in achieving Level 3 for LWH
• Trust performance indicators
• Use as lever with Trust to gain resources for maternity services

CNST Planning Group
• Develop action plan including all criteria.• Designated persons and time scales for
required action- takes longer than you think• Use scoring in ‘Summary of Standards’ to
check on progress and areas of difficulty• Don’t overlook criteria from lower levels as
need 90% in those• Regularly reassess.

Think Evidence
• Use the guidance in the manual
• Make sure every thing in each criterion is covered
• Have evidence for each item of verification
• Keep in separate file for each standard
• Keep it up to date & review regularly

Key People
• Training and postgraduate education leads• Audit department• Midwifery and directorate management • Clinical Risk Management MW• LW, clinic and ward managers• Complaints manager• Someone from neonatology and anaesthetics• Clerical help with minutes

Engagement- up ad down the organisation
• Directorate management
• Executives
• Board
• Consultants
• All staff

Big ‘things’ at Level 2& 3
• Implement risk strategy• Lessons from incidents• Confidential enquiry lessons• Robust system for all test results• Antenatal risk assessment documented• Annual Skills Drills – all staff• Full risk assessment• Appropriate clinical staffing ( consultants and
midwives)• Audit

Standard 1- Organisation
• Risk management strategy – Philosophy, objectives, responsibility, coordination, accountability,
implementation, author, review date.– Board minute that approved it.
• Job descriptions of nominated lead(s) – Risk management (1.1.2) – Delivery Suite (1.1.4)– Use consultant job plans

Organisation
• Risk management strategy distributed to all professional staff (1.2.1)
• Evidence of implementation and annual review (1.2.2)– Original and revised strategies– Action plans– Minutes of meetings

S Standard 2 Learning from Experience
: Learning from experience• Incident reporting (2.1.1).
– Use list of triggers in manual.
– Make sure all staff reporting.
• Analysis, review, and actions (2.1.2)– Need to show for each area
– Numbers and trends
– Actions taken, changes needed.

Learning from experience
• Strategic approach to incidents that might lead to a claim (2.2.1)– Use guidance in manual for guideline– Start early after incident– File of evidence, update regularly
• Evidence of lessons learned and action arising from adverse incident reporting (2.2.2 )
• Changes in practice in response to complaints (2.2.3)

Standard 3 - Learning from experience
• Considers and applies the recommendations made in the National Confidential Enquiries (2.2.4 ). Audit of service against these (2.3.1)– Action plans for each one (Don’t forget CISH &
NCEPOD)– Audit showing changes in practice or rationale
for not implementing recommendations– New policies– Minutes of meetings where discussed

Standard 3- Communication
Patient information ( 3.1.1 & 3.2.1)– Alternatives, risks and benefits , consequences– Different formats and languages– P.I.G terms of reference and minutes
• Labour Ward forum (3.1.5 )– Terms of reference– Group members - 50% attendance
• anaesthetist, neonatologist, junior MW & medical staff, consumer.
– Minutes

Communication
• System for test results( 3.2.2 & 3.3.1) – Guideline to cover this. – Patient information on screening.– System for ensuring tests done, reported ,
relayed and acted on.– Training– Uptake and detection rates (don’t forget
neonatal screening)

Communication
• At risk women (3.2.3)– Mental health guideline and screening process– Domestic violence– Documentation of these risks– Availability of interpreters– Follow up of non attendees

Communication
• Emergency Caesarean Section (3.2.4) – Unit standard – Annual audit recommendations and action plan– Review of audit and remedial actions
• System for early referral where fetal abnormalities have been identified (3.2.5)– Guideline/pathways

Standard 4 - Clinical Care
• 27 clinical guidelines (4.1.1) – evidence based, dated, minutes of meeting where
approved
• Systematic approach to guideline development (4.2.1)– Policy, minutes of meetings, distribution & archiving
old versions
• Audit of guidelines at least 14/27 within 3 years (4.3.1)

Clinical Care
• High Dependency care (4.1.3)– Guideline including lines of communication
• Recovery (4.1.4) – Post op/recovery guideline
– Training in monitoring, airway and resuscitation for MWs

Standard 5 - Induction training and competence
• CTG training (5.1.3)– Need evidence of 6 monthly attendance
– Formal study day
– Informal- computer package, video, consultant DS sessions • Annual skills drill (5.2.1, 5.3.1)
– Obstetric Emergency day covers:
– CTG, CPR, Neonatal resuscitation, cord prolapse, breech, shoulder dystocia, massive haemorrhage
– Ran at least monthly
•

Induction training and competence
• Junior doctors competency (5.2.2)– Skills checklist based on RCOG log book.– Educational supervisors go through this at
induction– Log book of supervised procedures

Standard 6- Health Records
• Record keeping audits (6.1.2, 6.2.1, 6.3.1)– Audit tool– Must cover electronic records as well as paper– check reports and results and action plans are
available.– Level 3 need to show improvement– Need evidence of changes cited in action plans

Health Records
• These were previously level 2 now level 1
• Medical and midwifery records (6.1.3).– chronological order
– all professional notes are filed together
• Designated place for recording (6.1.4).– of hyper-sensitivity reactions
– other information relevant to all healthcare professionals

Standard 7: Implementation of Clinical Risk Management
• All clinical risk management systems are in place and operational (7.2.1).– Evidence of nominated lead playing an active
role– Staff awareness of systems– Staff feed back, news letters, notice boards– Collaboration with audit, claims and complaints– Involvement of service users

Implementation of Clinical Risk Management
• Multidisciplinary clinical risk assessment (7.2.2, 7.3.1)– Check tool covers guidance in manual for
breadth, content, depth and action– Prioritisation of risk– Action plan, responsible persons– Board acceptance- need minutes– Progress on action points

Standard 8 - Staffing levels
• Dedicated anaesthetic (8.1.2) and ODA cover (8.1.3)– check recommended levels are reflected in the rota, and
the rota is clear.
• Labour ward medical cover (8.2.1)– 40 hours dedicated consultant cover- job plans and timetables
– Available out of hours within 30 minutes
– Resident SpR

Staffing levels
• Midwifery staffing (8.2.2, 8.3.1)– 1:1– Birthrate plus – Contingency plans etc
• Supervision of midwives(8.1.1, 8.2.3)– Action plan on LSA report– Evidence of monitoring of annual reviews

Summary
• Good reasons for aiming high
• Team approach especially with training
• Attention to detail
• Evidence is crucial- training and induction records
• Keep reviewing your position
• Don’t forget lower level criteria
• Good luck