Embed Size (px)
Citation preview
Obstetric Physiology for the Non-Obstetrician
Nicole Smith, M.D., M.P.H. Assistant Professor, Harvard Medical School Medical Director, Maternal Fetal Medicine Division of Maternal-Fetal Medicine, Brigham & Women’s Hospital
Disclosures
I have no disclosures (aside from an enjoyment of art and history)

Physiology vs pathology

Martha Jefferson
Overview • Review of physiology of pregnancy, by system
• Common disorders of pregnancy and postnatal counseling
• Hypertensive disorders
• Diabetes
• Maternal hematologic disorders
Pregnancy Physiology
Cardiovascular
Blood Pressure
• BP= CO x SVR • BP decreases ~10% by the 7th week of
pregnancy • Decreased BP due to lower SVR in pregnancy • Progesterone mediated vasodilation • Increased blood volume • Leads to a resultant increased cardiac output
• Heart Rate • Increases as early as 7th week • By term, increases by ~10-20%
Fluids • Hypervolemia from Na+ and water retention
• Accumulation of 6-8 L total body water content • TBW= 2/3 intracellular (ICF), 1/3 extracellular (ECF) • ECF=3:1 ratio interstitial to intravascular
• Maternal plasma volume increases by 10% as early as 7 weeks of pregnancy • Increase by ~50% at 32 weeks • Hemodilution is maximal at 30-32 weeks
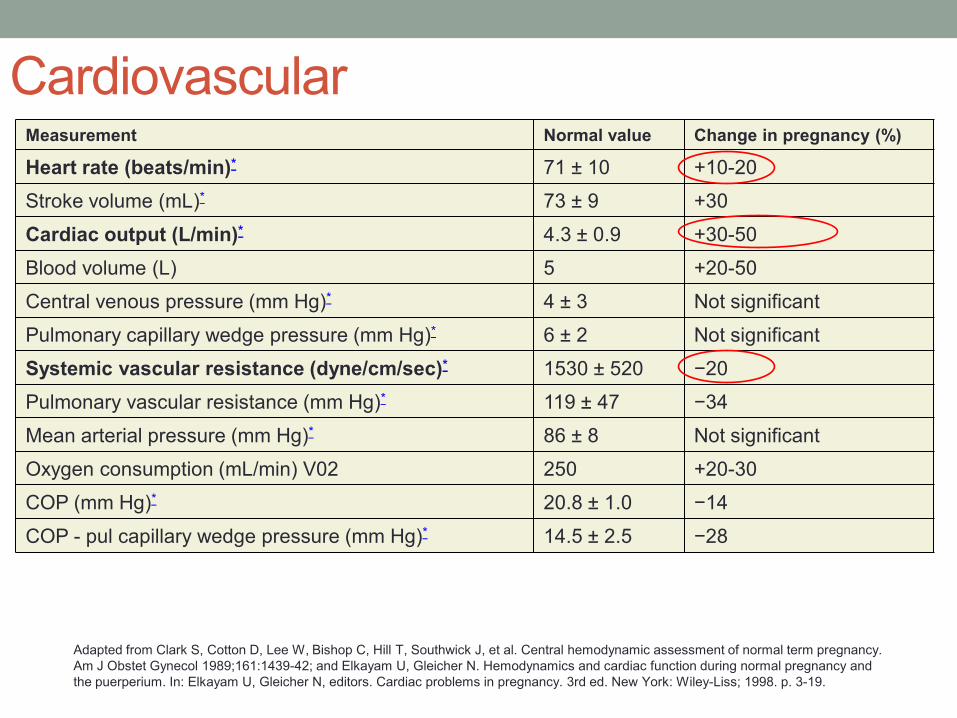
Cardiovascular Measurement Normal value Change in pregnancy (%)
Heart rate (beats/min)* 71 ± 10 +10-20 Stroke volume (mL)* 73 ± 9 +30 Cardiac output (L/min)* 4.3 ± 0.9 +30-50 Blood volume (L) 5 +20-50 Central venous pressure (mm Hg)* 4 ± 3 Not significant Pulmonary capillary wedge pressure (mm Hg)* 6 ± 2 Not significant Systemic vascular resistance (dyne/cm/sec)* 1530 ± 520 −20 Pulmonary vascular resistance (mm Hg)* 119 ± 47 −34 Mean arterial pressure (mm Hg)* 86 ± 8 Not significant Oxygen consumption (mL/min) V02 250 +20-30 COP (mm Hg)* 20.8 ± 1.0 −14 COP - pul capillary wedge pressure (mm Hg)* 14.5 ± 2.5 −28
Adapted from Clark S, Cotton D, Lee W, Bishop C, Hill T, Southwick J, et al. Central hemodynamic assessment of normal term pregnancy. Am J Obstet Gynecol 1989;161:1439-42; and Elkayam U, Gleicher N. Hemodynamics and cardiac function during normal pregnancy and the puerperium. In: Elkayam U, Gleicher N, editors. Cardiac problems in pregnancy. 3rd ed. New York: Wiley-Liss; 1998. p. 3-19.
Blood loss in Birth • A healthy pregnant woman can lose up
to 30% of her blood volume with little/no change in hemodynamics • Average blood loss with vaginal birth
~300cc • Average blood loss with Cesarean
~1000 cc • Typical medications given to reduce
bleeding include: • Methergine (methylergonavine) • Hemabate (carboprost) • Pitocin (oxytocin) • TXA (tranexamic acid) • and an intrauterine balloon device
(“Bakri”)
Hemodynamic Changes Post-Partum • Most of the volume loss following SVD is
due to diuresis • Diuresis normally occurs 2-5 days postpartum • Allows for loss of excess ECF accumulated in
pregnancy • Average ~6lb weight loss • Failure to diurese may lead to higher
intravascular volume and pulmonary edema • Postpartum diuresis
• Hct difference PP w VD: +5.2% on day 3 • Hct difference PP w C-sec: -5.8 % on day 5
Pulmonary Physiology
Dyspnea • Common symptom in pregnancy
• Up to 70% of women experience this sensation in a normal pregnancy
• The obstetric patient presenting with an acute onset of shortness of breath deserves a careful evaluation
• Cardiovascular diseases as a cause of dyspnea complicate 1–4% of pregnancies. • Peripartum cardiomyopathy is an uncommon but life
threatening complication of pregnancy • Women with underlying valvular disease may poorly tolerate
plasma volume expansion
Soubra, S, Gunupalli, K. Critical illness in pregnancy: an overview. Critical Care Medicine. Volume 33, (10) Supplement. S248-55. October 2005
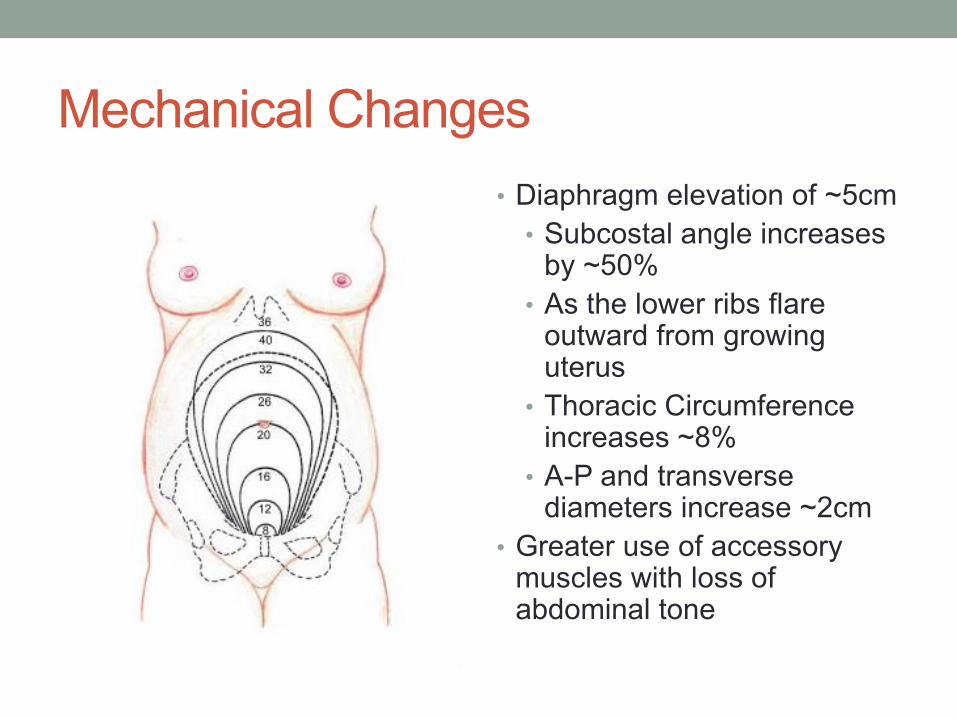
Mechanical Changes • Diaphragm elevation of ~5cm
• Subcostal angle increases by ~50%
• As the lower ribs flare outward from growing uterus
• Thoracic Circumference increases ~8%
• A-P and transverse diameters increase ~2cm
• Greater use of accessory muscles with loss of abdominal tone
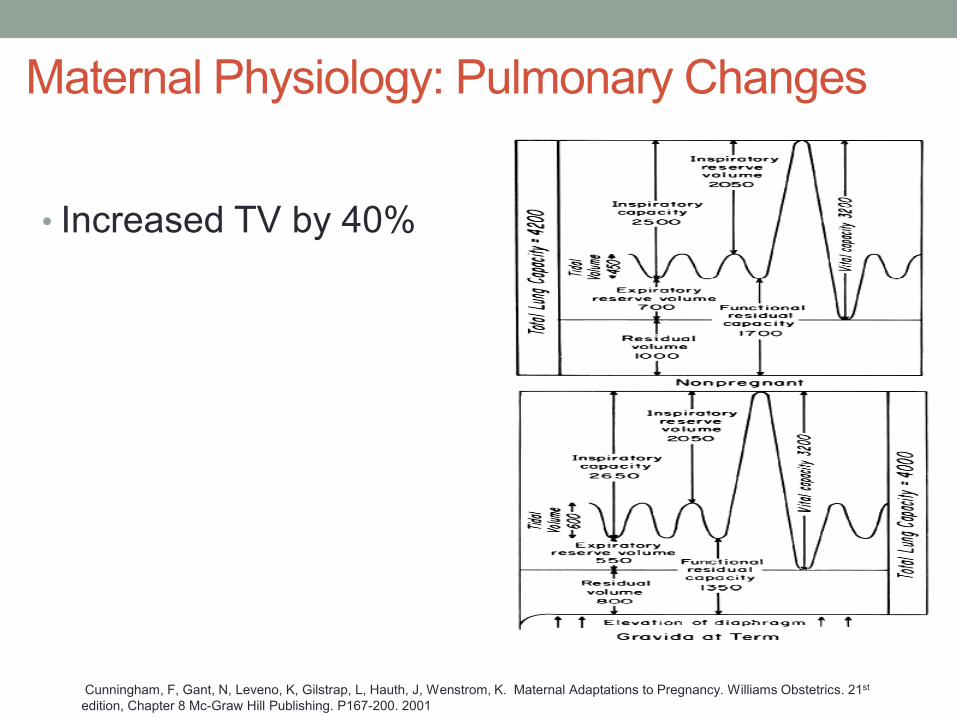
Maternal Physiology: Pulmonary Changes
• Increased TV by 40%
Cunningham, F, Gant, N, Leveno, K, Gilstrap, L, Hauth, J, Wenstrom, K. Maternal Adaptations to Pregnancy. Williams Obstetrics. 21st edition, Chapter 8 Mc-Graw Hill Publishing. P167-200. 2001
Renal and GI
Urinary System • Renal plasma flow and GFR both increase
early in pregnancy. • Increased GFR up to 50% reduces the upper limit
of normal for serum creatinine to 0.8 mg/dL • Creatinine of 1 is never normal in pregnancy!
• Pregnancy does not alter daily urine output • Urinary protein excretion in pregnant patients
over 24 hrs 95th %tile is 260 mg/day • Adds validity to proteinuria >300 mg/day as a
criterion for the diagnosis of preeclampsia
Yeomans, E, Gilstrap, L. Physiologic changes in pregnancy and their impact on critical care. Critical Care Medicine. Volume 33(10) Supplement. pp S256-S258. October 2005
Gastrointestinal System • Few changes in the gastrointestinal tract during
pregnancy have critical care significance • Decreased LES tone • Slowed gastric motility • Alkaline phosphatase elevated because of placental
production • Does not indicate hepatic obstruction.
• Gallbladder stasis may result in stone formation • Aminotransferases and coagulation times are not altered
• Elevation or prolongation of these values suggests underlying pathology
Yeomans, E, Gilstrap, L. Physiologic changes in pregnancy and their impact on critical care. Critical Care Medicine. Volume 33(10) Supplement. pp S256-S258. October 2005
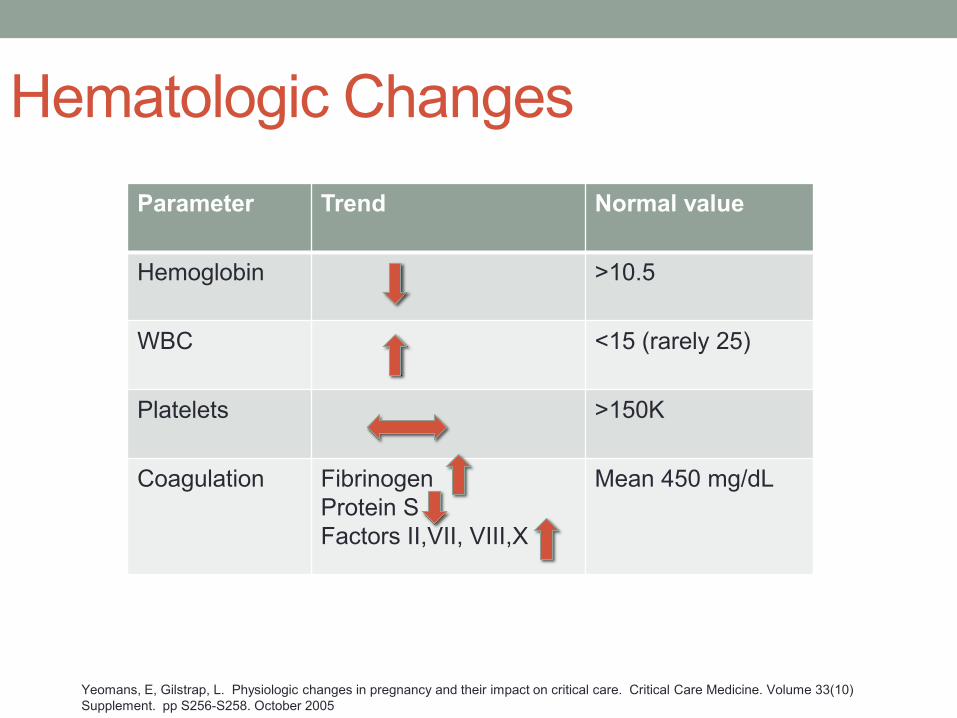
Hematologic Changes
Yeomans, E, Gilstrap, L. Physiologic changes in pregnancy and their impact on critical care. Critical Care Medicine. Volume 33(10) Supplement. pp S256-S258. October 2005
Parameter Trend Normal value
Hemoglobin >10.5
WBC <15 (rarely 25)
Platelets >150K
Coagulation Fibrinogen Protein S Factors II,VII, VIII,X
Mean 450 mg/dL
Select Pregnancy Disorders and Postnatal Counseling
Hypertensive Disorders of Pregnancy 1) Chronic Hypertension 2) Preeclampsia 3) Superimposed Preeclampsia 4) Gestational Hypertension 5) Eclampsia 6) HELLP Syndrome
2013 Guidelines
Classic presentation • C.M., a 32 year old prima gravida • First prenatal care visit: 16 weeks GA
• BP 106/70 mmHg, no proteinuria • Weight 102 pounds
• Pregnancy proceed unremarkably • At 36 weeks:
• Edema of the hands and face • BP 160/115 mmHg • Urine contained 6g of albumin in a 24 hour sample • 30 pound weight gain, 11 in last 4 weeks
• Admitted to Boston Lying In Hospital in 1862
2,400 years of preeclampsia
Bossier du Sauvages (1710-1795)
First to use the Greek term “eclampsia”
Hippocrates (400 BC)
Scipione Riva-Rocci’s sphygmomanometer: 1896
Preeclampsia
BP≥160/110 Elevated creatinine Thrombocytopenia Doubled LFTs Neurological changes
BP≥140/90 (Proteinuria) >300 mg/day Prot:Creat > 0.3 >1+ dip
Preeclampsia with Severe Features
John Lever (1811-1859)
Preeclampsia Epidemiology • Nulliparity (RR 2.91) • Past history of preeclampsia (RR 7.19) • Preeclampsia in first degree relative (RR 2.90) • Advanced maternal age (RR 1.96) • Medical conditions
• Chronic hypertension – 25% incidence • Maternal obesity – 15-24% • Pregestational diabetes • APS • Lupus • Chronic kidney disease
• Multiple gestation • Twins 12% • Triplet 20% • Quad 19%
Preeclampsia Risks
Fetal • Prematurity: 20% • Growth restriction • Placental abruption • Stillbirth
Maternal
• Stroke, seizure, liver rupture • 2-3x increase in lifelong cardiovascular disease
Management Goals Healthy mother, healthy baby (ies) Most at presentation have no permanent deficit Gestational age is critical in decision making and
outcome
Antihypertensives
Hydralazine to control severe hypertension 5-10 mg doses at 15-20 minute intervals Labetalol 20 mg IV 40 mg given in 10 minutes 80 mg given in 10 minutes Not to exceed 220 mg per episode Nifedipine
10 mg oral repeat in 30 minutes Idiosyncratic hypotension when used sublingual
Seizures
Eclampsia
• Eclampsia: the development of generalized tonic clonic seizures in a pregnant patient without history of a seizure disorder
Bossier du Sauvages (1710-1795) First to use the Greek term
“eclampsia”
Eclampsia epidemiology & symptomatology Ranges from 1/2000-3448 pregnancies
Incidence higher in: • Tertiary Care Centers • Multifetal pregnancy • No prenatal care
May occur before or after convulsions • Persistent occipital or frontal HA • Blurred vision • Photophobia • Epigastric or RUQ pain • Altered mental status
Symptoms:
Onset and Prevention
Timing of onset
• Antepartum (38-53%) • Postpartum (11-44%) • Reported 23 days PP • Comprehensive
evaluation for other sources should be undertaken for late occurrence
Prevention: Magnesium Sulfate
• Randomized controlled trials comparing magnesium vs. other agents (diazepam, phenytoin) for eclampsia prevention
• Recurrent seizures • 9.4% vs. 23.1%
• Maternal death • 3.0% vs. 4.8%
Magnesium • Intramuscular magnesium was introduced in the 1900s • Intravenous injection in the 1920s • 1990s brought RCTs demonstrating superiority over other
methods.
Chronic Hypertension
• Hypertension prior to pregnancy • Hypertension prior to 20 wks GA • Hypertension first seen after 20 weeks but persisting >12
weeks PP • Medication optimization
Gestational Hypertension
• Not preeclampsia • BP≥140/90 • May be associated with adverse outcomes • 10% of eclamptics seize without proteinuria
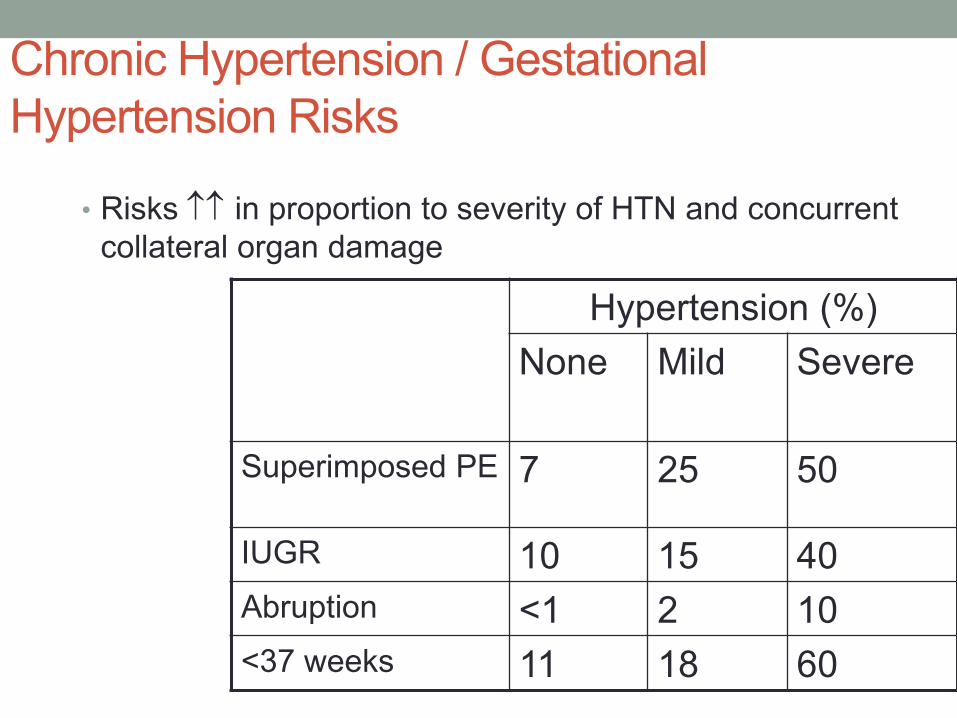
Chronic Hypertension / Gestational Hypertension Risks
• Risks ↑↑ in proportion to severity of HTN and concurrent collateral organ damage Hypertension (%)
None
Mild Severe
Superimposed PE 7 25 50
IUGR 10 15 40 Abruption <1 2 10 <37 weeks 11 18 60
Chronic Hypertension / Gestational Hypertension Management
• Medicate • Labetalol, nifedipine, methyldopa • Other agents can be used thoughtfully:
• Beta blockers • Diuretics (HCTZ, lasix)
• Goal: 150/100 mmHg… approximately
• Delivery • HTN but no medication: 38 to 39+6… maybe • HTN well controlled on med: 37 to 39+6
ACOG
Superimposed Preeclampsia
New proteinuria in chronic hypertensive after 20 weeks Sudden increase in protein, pressures, other findings in
patients with nephrotic syndrome and hypertension prior to 20 weeks
HELLP Syndrome
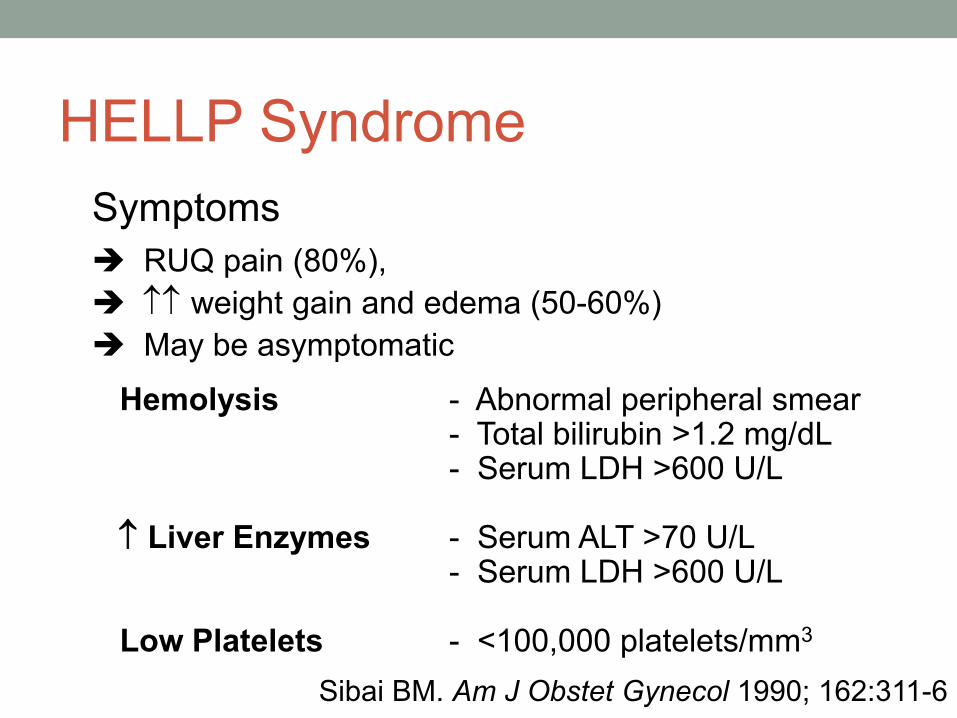
Hemolysis - Abnormal peripheral smear - Total bilirubin >1.2 mg/dL - Serum LDH >600 U/L ↑ Liver Enzymes - Serum ALT >70 U/L - Serum LDH >600 U/L Low Platelets - <100,000 platelets/mm3
Symptoms RUQ pain (80%), ↑↑ weight gain and edema (50-60%) May be asymptomatic
Sibai BM. Am J Obstet Gynecol 1990; 162:311-6
Postnatal counseling- Preeclampsia
• Preeclampsia and gestational hypertension are major risk factors for development of CV disease (AHA)
• Morbidity is related to • Severity of disease • GA at delivery • Number of disease recurrences
Schwartz Am J Med 2010
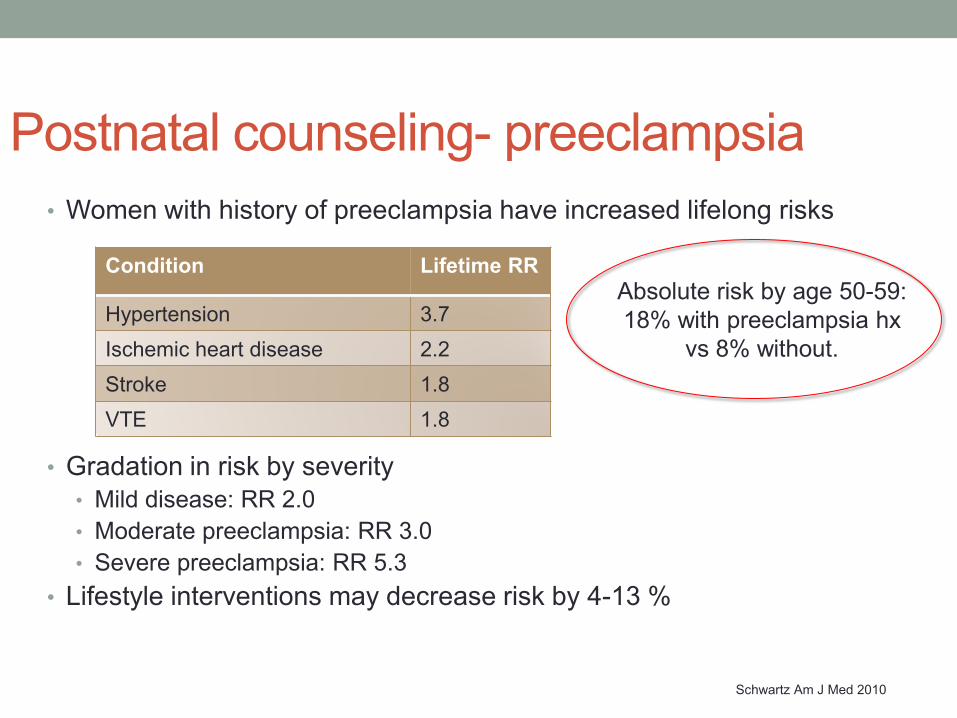
Postnatal counseling- preeclampsia • Women with history of preeclampsia have increased lifelong risks
• Gradation in risk by severity • Mild disease: RR 2.0 • Moderate preeclampsia: RR 3.0 • Severe preeclampsia: RR 5.3
• Lifestyle interventions may decrease risk by 4-13 %
Schwartz Am J Med 2010
Condition Lifetime RR
Hypertension 3.7 Ischemic heart disease 2.2 Stroke 1.8 VTE 1.8
Absolute risk by age 50-59: 18% with preeclampsia hx
vs 8% without.
Diabetes in Pregnancy
Pregestational Diabetes • Pregestational has been diagnosed prior to second trimester
pregnancy • Type 1 – insulin dependent • Type 2 – insulin resistant • Glucose intolerance in 1st trimester
• Approximately 2% of pregnancies • Depends on population characteristics • Increasing
• 0.8% in 1999
Gestational Diabetes • First documentation in 1824, of
hyperglycemia and stillbirth of a macrosomic infant at 22 weeks
• “Of pregnancy and progeny:” 1980
• Carbohydrate intolerance of variable severity with onset or first recognition during pregnancy
• May not depend on treatment with insulin
• Complicates 7% of pregnancies
Diagnosis of Gestational DM
• Usually screen 24-28 weeks gestation • Two step endorsed by ACOG
• (6-7%) • One step endorsed by ADA and IADPSG
• (15-20%) • NIH consensus recommend two step continue
(Vandorsten et al, NIH Concens State Sci 2013;29(1):1)
ACOG=American College of Obstetrics and Gynecology ADA= American Diabetes Association IADPSG= International Association Diabetes and Pregnancy Groups
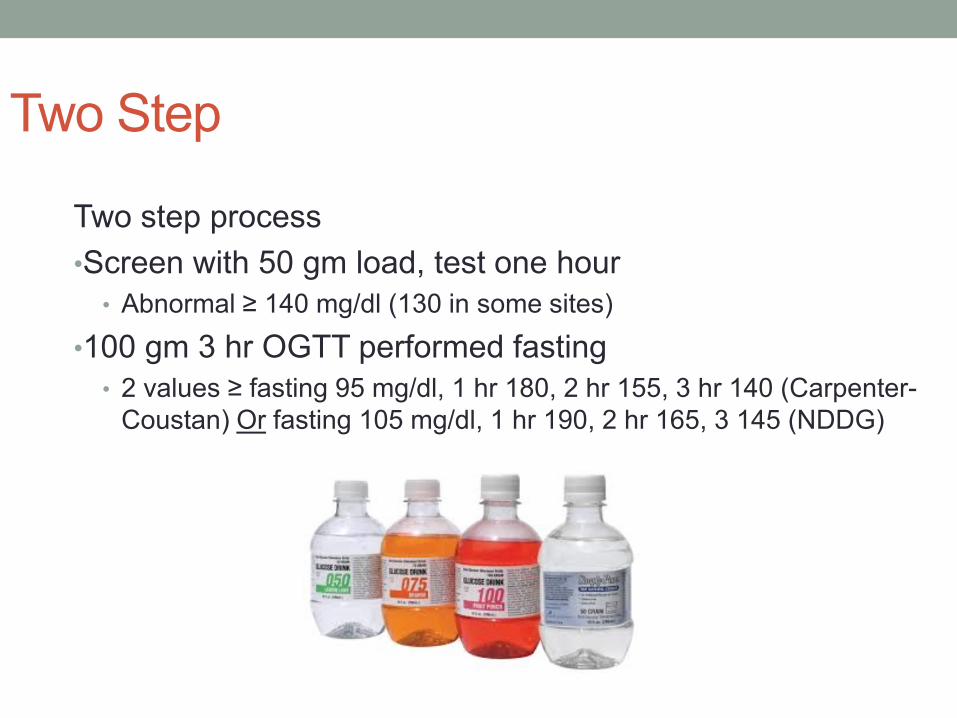
Two Step
Two step process •Screen with 50 gm load, test one hour
• Abnormal ≥ 140 mg/dl (130 in some sites) •100 gm 3 hr OGTT performed fasting
• 2 values ≥ fasting 95 mg/dl, 1 hr 180, 2 hr 155, 3 hr 140 (Carpenter-Coustan) Or fasting 105 mg/dl, 1 hr 190, 2 hr 165, 3 145 (NDDG)
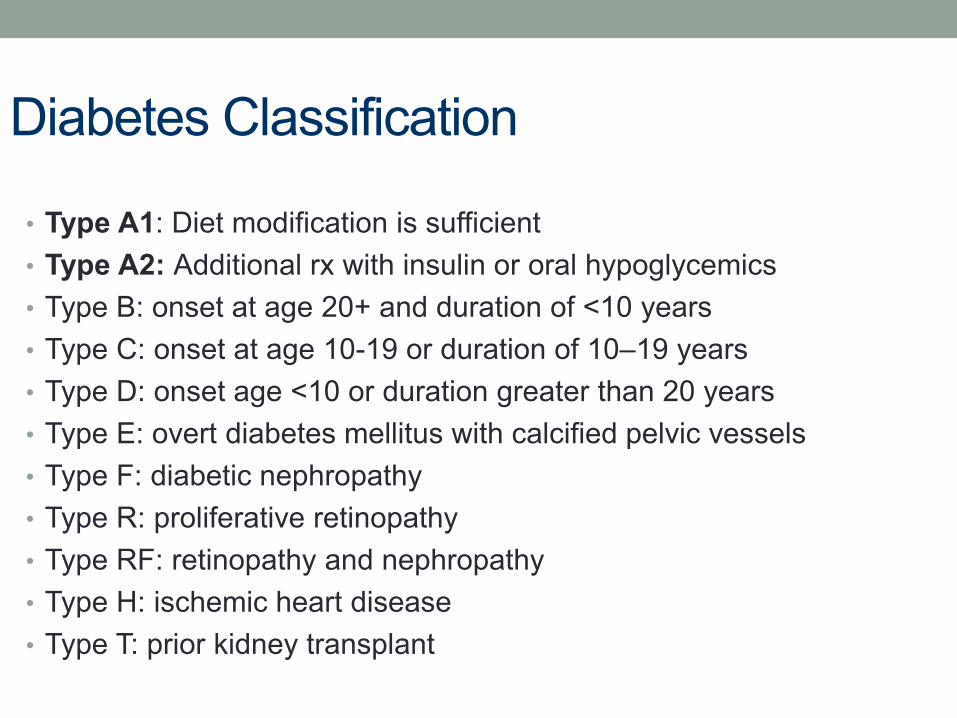
Diabetes Classification
• Type A1: Diet modification is sufficient • Type A2: Additional rx with insulin or oral hypoglycemics • Type B: onset at age 20+ and duration of <10 years • Type C: onset at age 10-19 or duration of 10–19 years • Type D: onset age <10 or duration greater than 20 years • Type E: overt diabetes mellitus with calcified pelvic vessels • Type F: diabetic nephropathy • Type R: proliferative retinopathy • Type RF: retinopathy and nephropathy • Type H: ischemic heart disease • Type T: prior kidney transplant
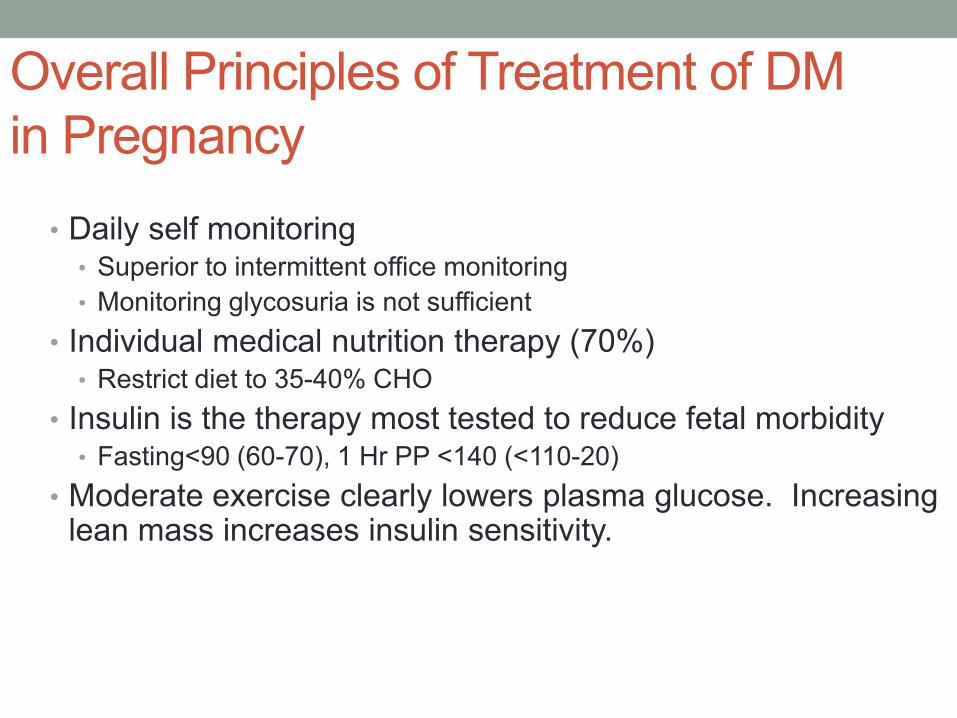
Overall Principles of Treatment of DM in Pregnancy
• Daily self monitoring • Superior to intermittent office monitoring • Monitoring glycosuria is not sufficient
• Individual medical nutrition therapy (70%) • Restrict diet to 35-40% CHO
• Insulin is the therapy most tested to reduce fetal morbidity • Fasting<90 (60-70), 1 Hr PP <140 (<110-20)
• Moderate exercise clearly lowers plasma glucose. Increasing lean mass increases insulin sensitivity.
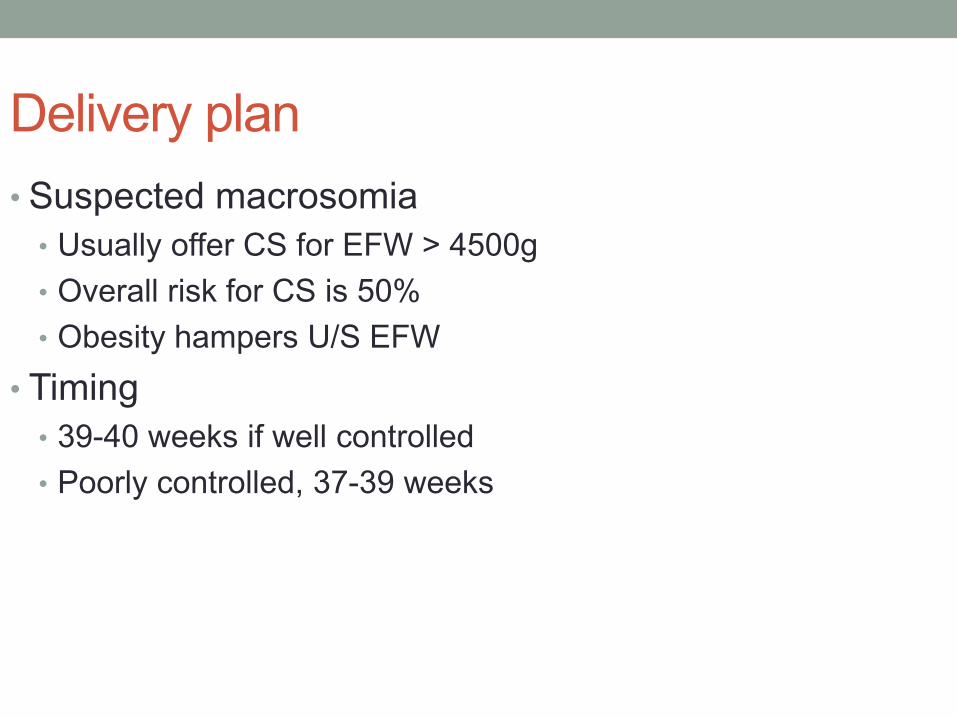
Delivery plan • Suspected macrosomia
• Usually offer CS for EFW > 4500g • Overall risk for CS is 50% • Obesity hampers U/S EFW
• Timing • 39-40 weeks if well controlled • Poorly controlled, 37-39 weeks
Postnatal counseling- Diabetes
• 50% risk of Type 2 diabetes in women with gestational diabetes • Encourage 75 g testing at 6 weeks postpartum
Schwartz Am J Med 2010
Mitigating risk • Optimize maternal conditions prior to pregnancy • Screen postpartum for T2DM in patients with GDM
• Early GDM screen in patients with risk factors (HbA1c <5.7, GLT <130)
• ASA for those with risk factors for preeclampsia • MFM consultation for medications rather than abrupt discontinuation
Select Maternal Hematologic Conditions
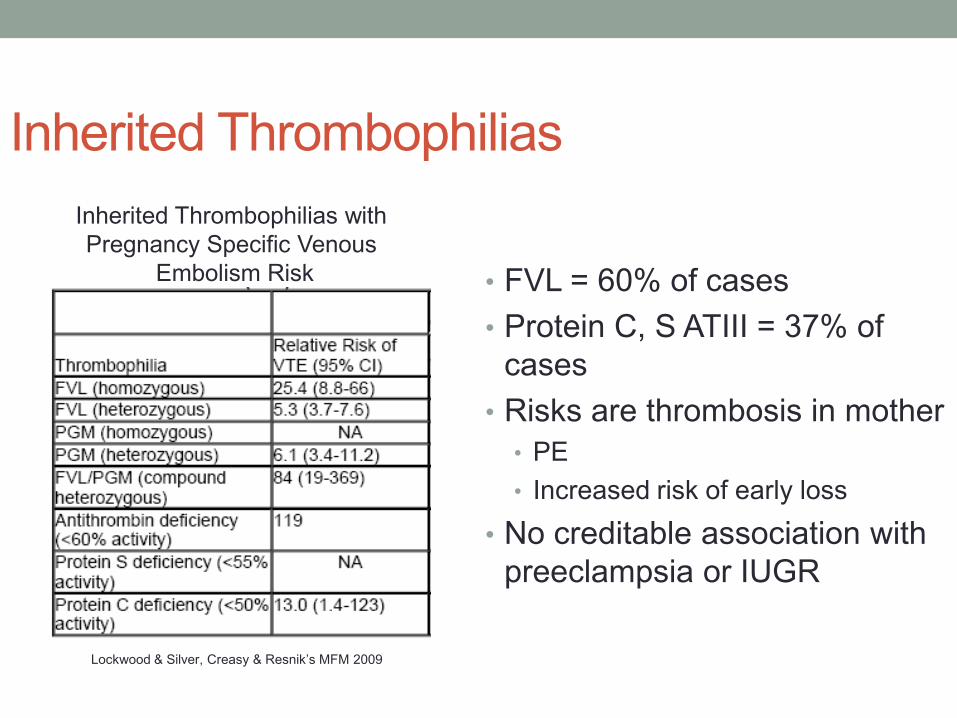
Inherited Thrombophilias
• FVL = 60% of cases • Protein C, S ATIII = 37% of
cases • Risks are thrombosis in mother
• PE • Increased risk of early loss
• No creditable association with preeclampsia or IUGR
Inherited Thrombophilias with Pregnancy Specific Venous
Embolism Risk
Lockwood & Silver, Creasy & Resnik’s MFM 2009
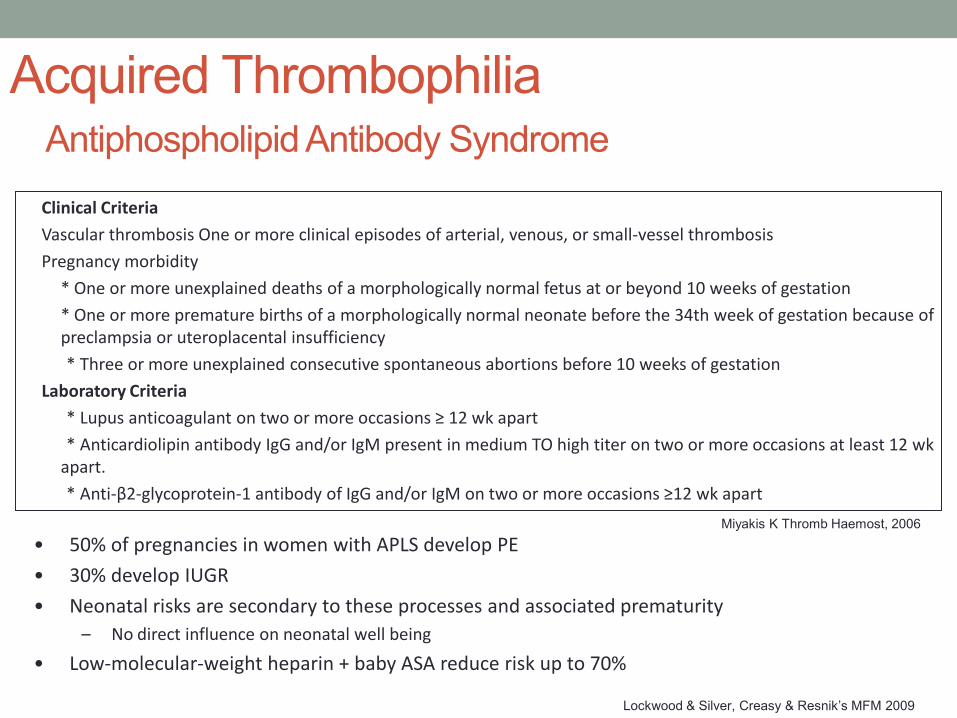
Acquired Thrombophilia Antiphospholipid Antibody Syndrome
Clinical Criteria Vascular thrombosis One or more clinical episodes of arterial, venous, or small-vessel thrombosis Pregnancy morbidity * One or more unexplained deaths of a morphologically normal fetus at or beyond 10 weeks of gestation * One or more premature births of a morphologically normal neonate before the 34th week of gestation because of
preclampsia or uteroplacental insufficiency * Three or more unexplained consecutive spontaneous abortions before 10 weeks of gestation Laboratory Criteria * Lupus anticoagulant on two or more occasions ≥ 12 wk apart * Anticardiolipin antibody IgG and/or IgM present in medium TO high titer on two or more occasions at least 12 wk
apart. * Anti-β2-glycoprotein-1 antibody of IgG and/or IgM on two or more occasions ≥12 wk apart
Miyakis K Thromb Haemost, 2006
• 50% of pregnancies in women with APLS develop PE • 30% develop IUGR • Neonatal risks are secondary to these processes and associated prematurity
– No direct influence on neonatal well being
• Low-molecular-weight heparin + baby ASA reduce risk up to 70%
Lockwood & Silver, Creasy & Resnik’s MFM 2009
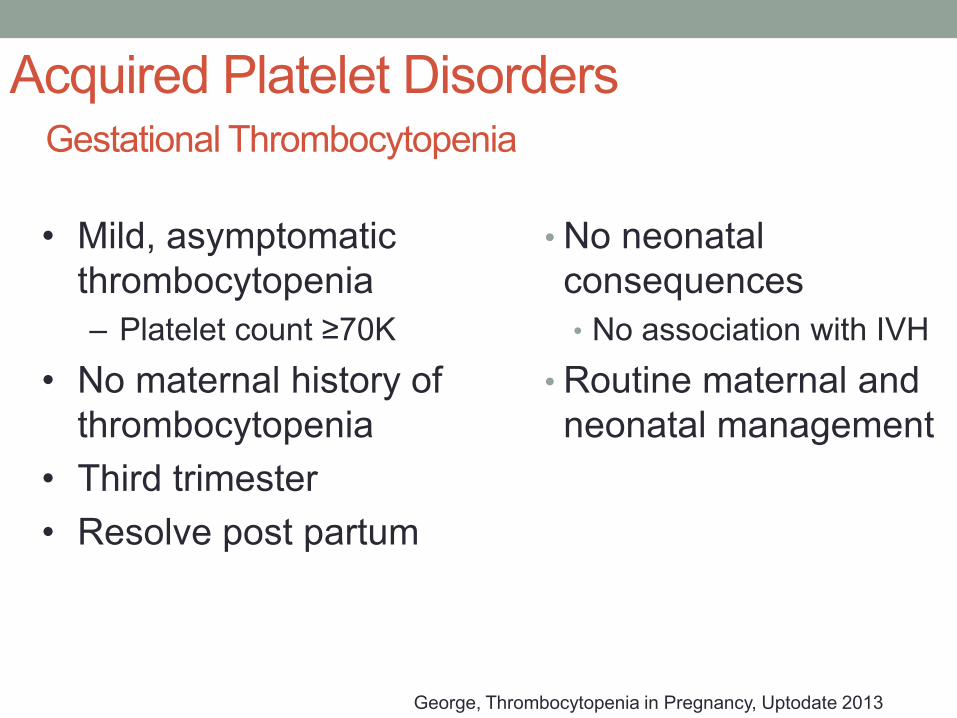
Acquired Platelet Disorders Gestational Thrombocytopenia
• No neonatal consequences • No association with IVH
• Routine maternal and neonatal management
• Mild, asymptomatic thrombocytopenia – Platelet count ≥70K
• No maternal history of thrombocytopenia
• Third trimester • Resolve post partum
George, Thrombocytopenia in Pregnancy, Uptodate 2013
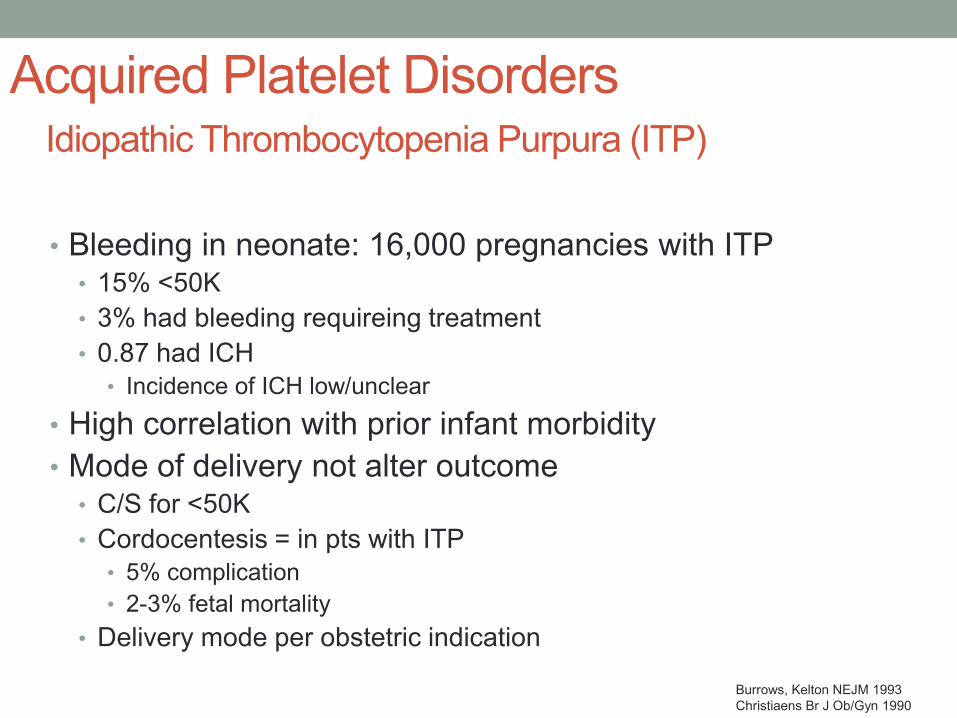
Acquired Platelet Disorders Idiopathic Thrombocytopenia Purpura (ITP)
• Bleeding in neonate: 16,000 pregnancies with ITP • 15% <50K • 3% had bleeding requireing treatment • 0.87 had ICH
• Incidence of ICH low/unclear • High correlation with prior infant morbidity • Mode of delivery not alter outcome
• C/S for <50K • Cordocentesis = in pts with ITP
• 5% complication • 2-3% fetal mortality
• Delivery mode per obstetric indication
Burrows, Kelton NEJM 1993 Christiaens Br J Ob/Gyn 1990
Breastfeeding
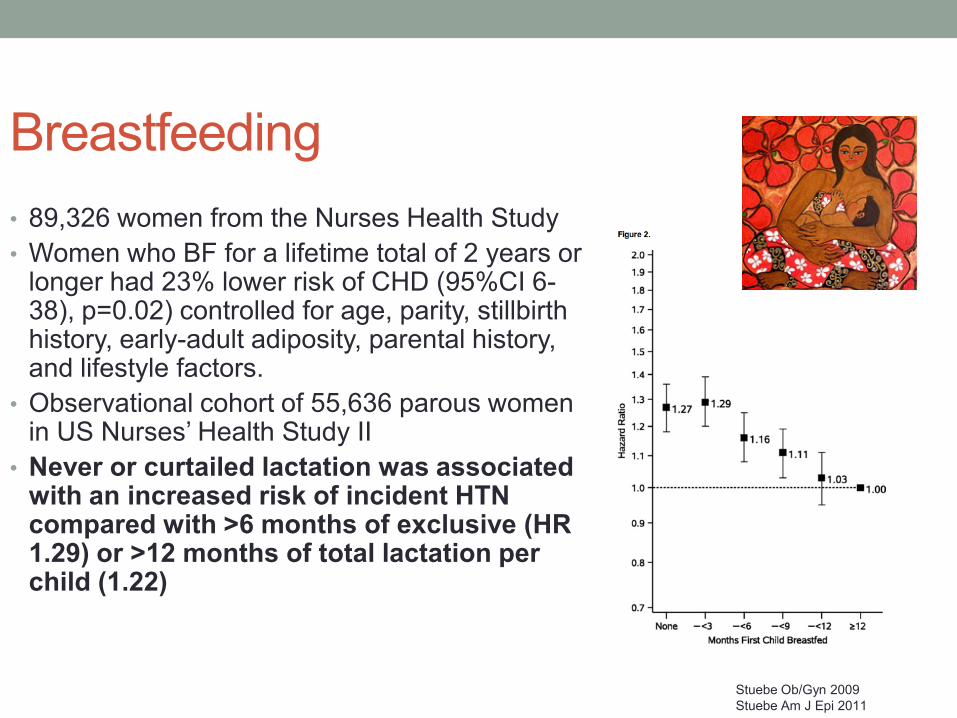
Breastfeeding • 89,326 women from the Nurses Health Study • Women who BF for a lifetime total of 2 years or
longer had 23% lower risk of CHD (95%CI 6-38), p=0.02) controlled for age, parity, stillbirth history, early-adult adiposity, parental history, and lifestyle factors.
• Observational cohort of 55,636 parous women in US Nurses’ Health Study II
• Never or curtailed lactation was associated with an increased risk of incident HTN compared with >6 months of exclusive (HR 1.29) or >12 months of total lactation per child (1.22)
Stuebe Ob/Gyn 2009 Stuebe Am J Epi 2011
Breastfeeding
• 2233 women in California (Kaiser) • 56% BF for >1 month • BF>1 mo had similar rates of T2DM as nulliparas
• (OR 1.01 95%CI 0.56-1.81)
• No BF were more likely to develop T2DM than nulliparas • (OR 1.93 95%CI 1.14-3.27)
• No BF were more likely to develop T2DM than BF 1-3 months • (OR 1.52 95% CI 1.11-2.1)
• Risk of type 2 diabetes increases when term pregnancy is followed
by <1 month of BF, independent of physical activity and BMI later in life
Schwartz Am J Med 2010
Breastfeeding
• Many medications are compatible with breastfeeding
• Lactmed when unsure • Advising “pump and dump” or
interrupting BF for therapy can significantly impact BF success

Acknowledgements- historical references
Thank you





























