Embed Size (px)
Citation preview

Preparedness for Acts of Nuclear, Biological, and Chemical TerrorismRussell E. Berger, MDMichele Burns Ewald, MD, FAAP
chapter 21
Introduction
Background
Major Biological Agents: Class 1A Biologic Agents Inhalational Anthrax Botulism Plague Smallpox Tularemia Viral Hemorrhagic Fevers
Chemical Agents Cyanide Nerve Agents (Sarin Gas)Vesicants
Nuclear AgentsRadiation Exposure
Conclusions
Chapter Outline
1 Distinguish signs and symptoms of common childhood illnesses from those caused by biological agents.
2 Formulate a treatment plan for children exposed to chemical agents.
3 Discuss short-term and long-term effects of radiation exposure in children.
Objectives
Copyright © 2012 by the American Academy of Pediatrics and the American College of Emergency Physicians

21-3
IntroductionOn September 11, 2001, our world changed forever. The attacks on the World Trade Center complex and the Pentagon killed thousands of innocent men, women, and children. In the immediate wake of those tragedies, attention turned to protecting our citizens against new threats. Emerging threats in-clude attacks that use chemical, biologic, and nuclear weapons designed to create mass casualties and hysteria. Emergency physicians are
on the frontlines of treating and triaging critically ill and injured children and therefore must be prepared to act if faced with any of these threats. This chapter addresses the major manifestations, pathogenesis, and natural history of the agents most likely to be encountered in a terrorist attack. Special attention is paid to the Centers for Disease Control and Prevention (CDC) class 1A biologic weapons, common chemical and nerve agents, and finally nuclear threats.
CASE
SCE
NARI
O 1 You are working the medical control telephone at Children’s Hospital and receive a
call from paramedics, who are bringing in schoolchildren exposed to a downtown gas attack. The hazardous materials team has yet to identify the agent but tells you that many people are dead on the scene. Those who are not dead are in extremis secondary to respiratory distress. Seizures are noted in some patients. Others have a strange reddish hue. Emergency medical services (EMS) officials report that the first patient they are bringing to you is hypotensive.
1. What agent is most likely to cause this presentation?2. What type of decontamination or treatment is needed?
Copyright © 2012 by the American Academy of Pediatrics and the American College of Emergency Physicians

21-4 Preparedness for Acts of Nuclear, Biological, and Chemical Terrorism
BackgroundDespite the increased attention to and recogni-tion of the complications of attack, most health care professionals feel ill prepared and poorly trained to deal with the unique challenges of disaster-stricken children. In a survey of 1,396 pediatricians, 86% believed that their medical training had not adequately prepared them to deal with the aftermath of the 9/11 attacks.1
In addition to training gaps among practi-tioners, in many places, the infrastructure for crisis management has not been established. In a survey of 3,670 school superintendents, only 42.8% had ever met with local EMS officials to discuss emergency planning at their schools.2
Although most hospitals have mass casualty protocols, only 64% include pediatric patients in their disaster drills.3 Most potential antidotes for exposures have not been tested in children, and there is a lack of weight-appropriate anti-dotes and treatment for exposures.4
Major Biological Agents: Class 1A Biologic WeaponsThe CDC has classified six biological agents as those posing the greatest threat in an attack: anthrax, botulism, plague, smallpox, tularemia, and viral hemorrhagic fevers.
The natural diseases caused by these agents have characteristic incubation times and natural histories. For frontline health care professionals, it is essential to be able to rapidly distinguish these entities (see Table 21-1).
Inhalational Anthrax
Clinical FeaturesInhalational anthrax is caused by the gram-pos-itive, rod-shaped, spore-forming bacteria Bacil-lus anthracis.5 Spores enter the body through inhalation and are taken up by macrophages in the lung. Macrophages transport the spores to lymph nodes, where the spores germinate into bacteria and escape into the bloodstream.5
Anthrax spores are resistant to drying, heat, UV radiation, and gamma radiation. Reports indicate that anthrax spores can remain biologi-cally active for a period of up to 200 years. Large
stores of weaponized anthrax are still believed to exist despite efforts to destroy stockpiles.6
Anthrax has a long and well-documented history of causing disease in patients. Early re-ports of disease date back thousands of years. Despite this long history, the number of pedi-atric patients documented in the literature is incredibly small. Thus, little is known about the natural history of this disease in children.
Most experts believe that anthrax infections are markedly underreported. Respiratory infec-tions are a leading cause of death in the developing world; thus, childhood death due to anthrax can be attributed to other, more common, pathogens. In addition, confirmatory pathology reports are rarely available to make postmortem diagnoses.7
Signs and SymptomsIn the few cases that are documented in the literature, some patterns have emerged. First, and this is true for the adult patients as well, children affected by fulminant anthrax have a mortality rate approaching 100%.8 Second, there are strong parallels between the prodro-mal phase of anthrax and influenza. With the 2009 outbreak of the H1N1 virus, we as physi-cians must remain vigilant for underlying and
Y O U R F I R S T C L U E
Signs and Symptoms of Inhalational Anthrax
• Nonfebrileillnessassociatedwithrapidonset of severe respiratory distress and shock.
T H E C L A S S I C S
Radiographic Findings of Inhalational Anthrax
• Pleuraleffusions
• Infiltrates
• Mediastinalwidening(Figure 21.1)
Copyright © 2012 by the American Academy of Pediatrics and the American College of Emergency Physicians

Major Biological Agents: Class 1A Biologic Weapons 21-5
TAB
LE 2
1-1
Cri
tica
l Bio
log
ical
Ag
ents
of T
erro
rism
Dis
ease
Ori
gin
Cli
nic
al F
ind
ings
aIn
cub
atio
n
Peri
od, d
Dia
gnos
tic
Sam
ple
sD
iagn
osti
c A
ssay
Isol
atio
n
Prec
auti
onsb
Init
ial
Trea
tmen
tPr
oph
ylax
is
An
thra
xB
acill
us
anth
raci
sIn
hal
atio
n: f
ebri
le
pro
dro
me
wit
h
rap
id p
rogr
essi
on
to m
edia
stin
al
lym
ph
aden
itis
, m
edia
stin
itis
(c
hes
t ra
dio
grap
h:
wit
h o
r w
ith
out
infi
ltra
tes,
wid
ened
m
edia
stin
um
, ple
ura
l ef
fusi
ons)
; sep
sis;
sh
ock;
men
ingi
tis
1–5
Blo
od
CSF
Pleu
ral fl
uid
Cu
ltu
re
Gra
m s
tain
ELIS
A
PCR
Stan
dar
dC
ipro
flox
acin
, 15
mg/
kg
(max
imu
m,
500
mg)
IV
ev
ery
12 h
, or
dox
ycyc
lin
e,
2.2
mg/
kg
(max
imu
m,
100
mg)
IV
ev
ery
12 h
c
Cip
rofl
oxac
in,
15 m
g/kg
(m
axim
um
, 500
m
g) o
rall
y ev
ery
12 h
3 6
0d,d
or
dox
ycyc
lin
e,
2.2
mg/
kg
(max
imu
m, 1
00
mg)
ora
lly
ever
y 12
hc 3
60d
d
Plag
ue
Yers
inia
pe
stis
Febr
ile
pro
dro
me
wit
h r
apid
p
rogr
essi
on
to f
ulm
inan
t p
neu
mon
ia w
ith
bl
ood
y sp
utu
m,
sep
sis,
DIC
2–4
Blo
od
Spu
tum
Lym
ph
nod
eas
pir
ate
Cu
ltu
re
Gra
m o
rW
righ
tG
iem
sa s
tain
ELIS
A, I
FA
Ag-
ELIS
A
Pneu
mon
ic:
dro
ple
t u
nti
l p
atie
nt
trea
ted
fo
r 3
day
s
Gen
tam
icin
, 2.
5 m
g/kg
IV
ev
ery
8h,e
or
dox
ycyc
lin
e,
2.2
mg/
kg I
V
(max
imu
m,
100
mg)
IV
ev
ery
12h
, or
ci
pro
flox
acin
, 15
mg/
kg
(max
imu
m,
500
mg)
IV
ev
ery
12 h
, or
chlo
ram
ph
en-
icol
, 15
mg/
kg
(max
imu
m, 1
g)
eve
ry 6
h
Dox
ycyc
lin
e,
2.2
mg/
kg
(max
imu
m, 1
00
mg)
ora
lly
ever
y 12
h ×
10
d, o
r ci
pro
flox
acin
, 20
mg/
kg
(max
imu
m,
500
mg)
ora
lly
ever
y 12
h ×
10
d, o
r ch
lora
-m
ph
enic
ol,
15 m
g/kg
(m
axim
um
, 1 g
) or
ally
eve
ry
6 h
× 7
d
Smal
lpox
Var
iola
vir
us
Febr
ile
pro
dro
me
Syn
chro
nou
s ve
sico
pu
stu
lar
eru
pti
on,
pre
dom
inan
t on
fac
e an
d e
xtre
mit
ies
7–17
Ph
aryn
geal
s
wab
Scab
mat
eria
l
ELIS
A, P
CR
Vir
us
is
olat
ion
Air
born
e,
dro
ple
t,
con
tact
Sup
por
tive
ca
reV
acci
nat
ion
w
ith
in 4
d
(con
sid
er
Vac
cini
a im
mu
n-
oglo
buli
n, 0
.6
mL/
kg, I
M
wit
hin
3 d
of
exp
osu
re
for
vacc
ine
com
pli
cati
ons,
im
mu
no-
com
pro
mis
ed
per
son
s) (con
tin
ues
)
Copyright © 2012 by the American Academy of Pediatrics and the American College of Emergency Physicians

21-6 Preparedness for Acts of Nuclear, Biological, and Chemical Terrorism
TAB
LE 2
1-1
Cri
tica
l Bio
log
ical
Ag
ents
of T
erro
rism
, con
tin
ued
Dis
ease
Ori
gin
Cli
nic
al F
ind
ings
aIn
cub
atio
n
Peri
od, d
Dia
gnos
tic
Sam
ple
sD
iagn
osti
c A
ssay
Isol
a-
tion
Pre
- ca
uti
onsb
Init
ial T
reat
men
tPr
oph
ylax
is
Tula
rem
iaFr
anci
sella
tu
lare
nsis
Pneu
mon
ic: a
bru
pt-
onse
t fe
ver,
fu
lmin
ant
pn
eum
onia
(c
hes
t ra
dio
grap
h:
pro
min
ent
hil
ar
aden
opat
hy)
Typ
hoi
dal
: fev
er,
mal
aise
, abd
omin
al
pai
n
2–10
B
lood
Spu
tum
Seru
m
Tis
sue
Cu
ltu
ref
sero
logy
: ag
glu
tin
atio
n
EM
Stan
dar
dG
enta
mic
in, 2
.5 m
g/kg
IM
or
IV e
very
8h
,e or
dox
ycyc
lin
e, 2
.2 m
g/kg
(max
imu
m, 1
00
mg)
IV
eve
ry 1
2 h
, or
cip
rofl
oxac
in, 1
5 m
g/kg
(max
imu
m, 5
00
mg)
IV
eve
ry 1
2 h
, or
cip
rofl
oxac
in, 1
5 m
g/kg
(max
imu
m, 5
00
mg)
UV
eve
ry 1
2 h
, or
chlo
ram
ph
enic
ol, 1
5 m
g/kg
(max
imu
m,
1 g)
IV
eve
ry 6
h
Dox
ycyc
lin
e,
2.2
mg/
kg
(max
imu
m, 1
00
mg)
ora
lly
ever
y 12
h ×
14
d, o
r ci
pro
flox
acin
, 15
mg/
kg
(max
imu
m, 5
00
mg)
ora
lly
ever
y 12
h ×
14
d
Bot
uli
smC
lost
ridi
um
bo
tulin
um
to
xin
Afe
bril
e
Des
cen
din
g fl
acci
d
par
alys
is
Cra
nia
l ner
ve p
alsi
es
Sen
sati
on a
nd
m
enta
tion
inta
ct
1–5
Nas
al s
wab
Mou
se
bioa
ssay
Ag-
ELIS
A
Stan
dar
dC
DC
hep
tava
len
t an
tito
xin
(ser
otyp
es
A-G
), 1
vial
(20
mL)
IV
Non
e
Vir
al
hem
or-
rhag
ic
feve
rs
Filo
viri
dae
(E
bola
, M
arbu
rg)
Febr
ile
pro
dro
me;
ra
pid
pro
gres
sion
to
sh
ock,
pu
rpu
ra,
blee
din
g d
iath
esis
4–21
Se
rum
Blo
od
Vir
al is
olat
ion
Ag-
ELIS
A
RT-
PCR
Sero
logy
:
Ab-
ELIS
A
Con
tact
, d
rop
let;
co
nsi
der
ai
rbor
ne
if m
assi
ve
hem
or-
rhag
e
Sup
por
tive
car
eN
one
Hen
reti
g FM
, Cie
slak
TJ,
Eitz
en Jr
EE.
Bio
logi
cal a
nd
ch
emic
al t
erro
rism
. Jou
rnal
of
Ped
iatr
ics.
200
2; 1
41(3
):311
–326
. Ad
apte
d w
ith
per
mis
sion
.
Abb
revi
atio
ns:
Ab,
an
tibo
dy;
Ag,
an
tige
n; C
DC
, Cen
ters
for
Dis
ease
Con
trol
an
d P
reve
nti
on; C
SF, c
ereb
rosp
inal
flu
id; D
IC, d
isse
min
ated
intr
avas
cula
r co
agu
lati
on; E
LISA
, en
zym
e-li
nke
d im
mu
nos
orbe
nt
assa
y; E
M,
elec
tron
mic
rosc
opy;
IFA
, im
mu
nofl
uor
esce
nt
assa
y; I
M, i
ntr
amu
scu
larl
y; I
V, in
trav
enou
sly;
PC
R, p
olym
eras
e ch
ain
rea
ctio
n; R
T, r
ever
se t
ran
scri
pta
se.
a Syn
dro
me
exp
ecte
d a
fter
aer
osol
exp
osu
re.
b Bri
ef d
efin
itio
n o
f is
olat
ion
pre
cau
tion
s: S
tan
dar
d—
han
dw
ash
ing;
glo
ves,
mas
ks, e
ye p
rote
ctio
n, f
ace
shie
lds,
an
d n
onst
eril
e, fl
uid
-res
ista
nt
gow
ns
for
bloo
d, b
ody
flu
id e
xpos
ure
; ap
pro
pri
ate
han
dli
ng
of p
atie
nt
care
eq
uip
men
t, li
nen
s, e
tc; a
void
ance
of
nee
dle
-sti
ck, s
har
ps
inju
ry. A
irbo
rne—
stan
dar
d, p
lus
pri
vate
, neg
ativ
e-p
ress
ure
roo
m w
ith
ext
ern
al e
xhau
st o
r H
EPA
filt
ered
rec
ircu
late
d a
ir; s
pec
ial “
fitt
ed”
and
“se
alin
g” r
esp
irat
or
mas
ks (e
g, N
95).
Dro
ple
t—st
and
ard
, plu
s p
riva
te r
oom
, “ro
uti
ne”
mas
k w
ith
in91
cm
(3 f
t) o
f p
atie
nt.
Con
tact
—st
and
ard
, plu
s p
riva
te r
oom
; glo
ves
at a
ll t
imes
; han
d-w
ash
ing
afte
r gl
ove
rem
oval
; gow
ns
at a
ll t
imes
, re
mov
ed p
rior
to
leav
ing
pat
ien
t’s r
oom
. Ad
apte
d f
rom
: Am
eric
an A
cad
emy
of P
edia
tric
s. I
nfe
ctio
n c
ontr
ol f
or h
osp
ital
ized
ch
ild
ren
. In
: Pic
keri
ng
LK, e
d. 2
000
Red
book
: Rep
ort
of t
he C
omm
itte
e on
Inf
ecti
ous
Dis
ease
s. 2
5th
ed
. Elk
Gro
ve V
illa
ge, I
L: A
mer
ican
Aca
dem
y of
Ped
iatr
ics;
200
0:12
7–13
7.c T
he
CD
C r
ecom
men
ded
on
e or
tw
o ad
dit
ion
al a
nti
biot
ics
for
inh
alat
ion
al a
nth
rax
in t
he
fall
200
1 ou
tbre
ak: r
ifam
pin
, van
com
ycin
, pen
icil
lin
or
amp
icil
lin
, cli
nd
amyc
in, i
mip
enem
, or
clar
ith
rom
ycin
. Rec
omm
end
atio
ns
in f
utu
re o
utb
reak
s m
igh
t ev
olve
rap
idly
, an
d f
req
uen
t co
nsu
ltat
ion
wit
h lo
cal h
ealt
h d
epar
tmen
ts a
nd
th
e C
DC
(ww
w.b
t.cd
c.go
v) is
en
cou
rage
d.
d A
mox
icil
lin
, 80
mg/
kg p
er d
ay d
ivid
ed e
very
8 h
ours
, can
be
subs
titu
ted
if s
trai
n p
rove
s su
scep
tibl
e.e S
trep
tom
ycin
, 15
mg/
kg I
M e
very
12
hou
rs, c
an b
e su
bsti
tute
d if
ava
ilab
le.
f Lab
orat
ory
mu
st b
e n
otifi
ed t
hat
tu
lare
mia
is s
usp
ecte
d.
Copyright © 2012 by the American Academy of Pediatrics and the American College of Emergency Physicians

Major Biological Agents: Class 1A Biologic Weapons 21-7
insidious attacks that can be superimposed over a background of natural disease.
In the pediatric anthrax literature, some patterns of disease have been identified. In the prodromal phase of anthrax, dizziness, visual changes, and syncope are key symptoms to help distinguish between an acute viral syndrome and anthrax.7 Pediatric patients presenting with sore throat or rhinorrhea are much more likely to have a common viral illness than anthrax.7
Diagnostic Studies and ManagementAntibiotic treatment for inhalation anthrax is ef-fective in preventing mortality when begun with-in the first day or two. However, index cases are notoriously difficult to recognize. Early detection could prevent excess morbidity and mortality.
Botulism
Clinical FeaturesBotulism is one of the most potent toxins. A single gram of aerosolized toxin could kill at least 1.5 million people. Botulism is caused by a gram-positive, rod-shaped, spore-forming, ob-ligate anaerobe. Its spores are hearty, resistant to
gastric acidity, and survive temperatures higher than 100°C (>212°F).9 Botulism causes irrevers-ible damage to the neuromuscular junction.
Signs and SymptomsPatients with botulism are afebrile and experi-ence a descending symmetric paralysis. Patients have no fevers or chills, have normal blood pres-sure and heart rate, but can experience blurring of their vision.9 Symptoms begin after a latency of approximately 24 hours.10 Despite their paral-ysis, these patients have preserved sensation and mental status. Botulism is not contagious.9,10
Diagnostic Studies and ManagementThe diagnosis of botulism is made via enzyme-linked immunosorbent assay (ELISA) testing. A new equine-derived heptavalent (toxin types A-G) botulinum antitoxin (called HBAT) is available for the treatment of noninfantile bot-ulism from the CDC. Although it can help in-terrupt disease progression, it does not reverse damage to already paralyzed muscles.11 Death
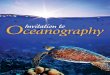
Figure 21.1 Chest radiograph demonstrating mediastinal widening and pleural effusion associated with inhalational anthrax.
Y O U R F I R S T C L U E
Signs and Symptoms of Botulism
• Afebrile
• Symmetric,descendingflaccidparalysis(poor tone in infants)
• Cranialnervepalsiesandbulbarfindings(decreased suck in infants)
• Normalmentalstatusassociatedwithother profound neurologic findings
W H AT E L S E
Differential Diagnosis of Botulism
• Polio:asymmetricparalysis
• Guillain-Barrésyndrome:symmetric,ascending paralysis
• Myastheniagravis:ophthalmoplegia,positive Tensilon test result
• Transversemyelitis:ascendingparalysis
Copyright © 2012 by the American Academy of Pediatrics and the American College of Emergency Physicians

21-8 Preparedness for Acts of Nuclear, Biological, and Chemical Terrorism
from botulism is primarily secondary to respirato-ry failure. Thus, prompt intubation and support-ive care are necessary.10 Serum, feces, or gastric aspirates can be obtained to confirm the diagnosis. Differential diagnosis includes myasthenia gravis, tick paralysis, Guillain-Barré syndrome, polio, stroke, and heavy metal intoxication.9
Plague
Clinical FeaturesPlague is caused by Yersinia pestis, a gram-neg-ative, nonmotile, pleomorphic, nonsporulat-ing bacterium.12 Plague has a storied history of killing as many as 75 million people during the black death of the late 1300s, fully one-third of the population of Europe. Because of this devas-tation, plague has been identified as a potential bioweapon.13
During World War II, a secret branch of the Japanese Army dropped plague-infected fleas over populated areas of China.13 Since then, both the US government and the former Soviet govern-ment have worked to create aerosols of this agent.
Airborne exposure via aerosol would pro-duce the most devastating effects on a popula-tion. If 50 kg of Y. pestis was aerosolized in a city of 5 million people, 150,000 cases of plague would result, and approximately 36,000 people would die.13 Once a population was infected, pneumon-ic plague could spread from person to person.14 Untreated pneumonic plague carries a mortality rate of 100%, whereas treated pneumonic plague is fatal approximately 50% of the time.12
Signs and SymptomsThe disease begins with rapid onset of severe flulike illness, including fever, headache, myal-gias, and exhaustion and weakness after a 1- to 6-day incubation period. The disease rapidly turns into hemorrhagic pneumonia character-ized by hemoptysis and respiratory failure.13
Diagnostic Studies and ManagementLaboratory work can reveal leukocytosis with toxic granulations, liver function test (LFT) de-rangements, coagulopathy, and other signs of multiorgan failure. Yersinia is difficult to isolate; growth can take up to 48 hours.14
Streptomycin is the drug of choice based on nonrandomized studies performed in the 1940s
and 1950s. Doxycycline is indicated for post-exposure prophylaxis when these individuals encounter patients with untreated pneumonic plague. This therapy should continue for a mini-mum of 7 days. Although a vaccine has been developed for Y. pestis, it was discontinued in 1999 and is no longer available, though it does exist in the military sector.13
Smallpox
Clinical FeaturesSmallpox (Variola virus) is a deadly viral infec-tion that has been considered eradicated world-wide. However, it is feared that there remain large stockpiles of weaponized smallpox that have not yet been destroyed. If these stockpiles truly remain, they could produce a devastating outbreak if they fell into the wrong hands.15
Y O U R F I R S T C L U E
Signs and Symptoms of Smallpox
• Distinguishingsmallpoxfromchickenpoxinfections
• Featuresofsmallpox
• Vesicularlesionsinsimilarstageofdevelopment
• Beginonfaceandextremitiesthenspreadto trunk and abdomen
• Hightemperature
• Exhaustionandweakness
T H E C L A S S I C S
Diagnostic Findings of Plague
• Chestradiographrevealspatchyorconsolidated pneumonia.
• Pneumonicplaguesareassociatedwithsignificant hemoptysis and progression to respiratory failure.
• Mortalityisalmostuniversalinpatientspresenting with advanced pneumonic plague.
Copyright © 2012 by the American Academy of Pediatrics and the American College of Emergency Physicians

Major Biological Agents: Class 1A Biologic Weapons 21-9
Y O U R F I R S T C L U E
Findings of Tularemia
• LFTresultsaretheonlycommonlaboratory test abnormalities.
• Nodularinfiltratesandapleuraleffusionon chest radiograph are suggestive of the diagnosis.
Figure 21.2 Smallpox lesions in a child.
Signs and SymptomsSmallpox is highly contagious and rapidly fatal, with a mortality rate of approximately 30%. It begins with a febrile prodrome, and then the characteristic exanthem of the infection emerg-es. In contrast to Varicella infection, smallpox lesions, which are small fluid-filled vesicles, all appear at the same stage of development. These lesions tend to concentrate on the face and cen-trifugally migrate from the head out15,16 (Figure 21.2). The lesions tend to concentrate on ventral surfaces and spare the axillae, palms, soles, and antecubital areas.15
Diagnostic Studies and ManagementThe diagnosis of smallpox requires a 1- to 4-day febrile prodrome followed by the classic smallpox lesions, all at the same stage of development.15
An outbreak of smallpox requires airborne, droplet, and contact precautions to be strictly maintained. Unvaccinated caregivers are at sig-nificant risk of contracting the disease. How-ever, exposed individuals, vaccinated within 3 to 4 days of exposure, can be protected from contracting the disease or can have a less ful-minant course.15,16
Vaccination for smallpox is with a live but attenuated virus. Thus, immunocompromised patients should not be vaccinated. In addition, vaccination is category D for pregnant women, and thus benefits must be carefully weighed against fetal risk. Treatment is otherwise sup-portive care.15,16
Tularemia
Clinical FeaturesTularemia is caused by Francisella tularensis, a gram-negative, intracellular, nonmotile, coc-cobacillus.17,18 It is a hardy organism that can remain alive for weeks to years. Mortality linked to tularemia infection ranges from 2% to 4% after exposure. A 50-kg aerosol dispersal in a population of 5 million would kill approxi-mately 19,000 people and lead to approximately 250,000 hospitalizations.19
Tularemia is not contagious but is highly infectious.18 As few as 10 organisms can pre-cipitate fulminant disease.
Signs and SymptomsThe most common signs and symptoms of tu-laremia are fever, lymphadenopathy, pharyngi-tis, nausea, and vomiting.17 Given these signs, a high index of suspicion for this disease must be maintained.
Diagnostic Studies and ManagementBasic blood work is frequently normal, although 50% of patients with tularemia will have LFT re-sult abnormalities.17,18 Complete blood cell counts might not demonstrate leukocytosis or left shift. Chest radiograph might reveal only peribronchial infiltrates. The presence of nodular infiltrates and a pleural effusion is suggestive of the diagnosis, al-though nonspecific.17 Tularemia, thus, represents a significant diagnostic challenge.
Streptomycin combined with gentamicin are the preferred treatments once the diagnosis has been made. Doxycycline and ciprofloxacin might be acceptable alternative treatments. In other countries, tularemia vaccines have been developed, but these are not commercially avail-able in the United States.17,18
Copyright © 2012 by the American Academy of Pediatrics and the American College of Emergency Physicians

21-10 Preparedness for Acts of Nuclear, Biological, and Chemical Terrorism
Viral Hemorrhagic Fevers
Clinical FeaturesViral hemorrhagic fevers due to Ebola and Mar-burg fever are highly lethal and contagious. These viruses are nonsegmented, negative-sense, single-stranded RNA viruses that belong to the Filovirus class.20 Their high infectivity and lethality make them potential bioweapons.
To date, all natural cases of these infections have begun in sub-Saharan Africa. A laboratory incident in Germany exposed German scientists to a swift but deadly outbreak in the 1970s. The natural reservoir for Marburg virus was recently discovered in the African fruit bat. The animal host for the Ebola virus has not yet been identified.20
Signs and SymptomsBoth Marburg and Ebola begin with a viral pro-drome and rapidly lead to a fatal multisystem organ failure, with a case fatality rate of 20% to 25%.21 These viruses turn on a potent cy-tokine storm, releasing tumor necrosis factor αinterleukin 1, interleukin 6, nitric oxide, and macrophage chemotactic protein. The result is a disseminated vascular leak syndrome, produc-ing hypotension and ultimately death.20
Diagnosis and ManagementELISA testing and polymerase chain reaction can be used to confirm the diagnosis. For patients exposed to Ebola, they can have a dark red, discolored soft palate and conjunctival injection along with hypotension and mucous membrane hemorrhage.20,21 It is believed that that these viruses can spread in the blood, vomit, urine, feces, and even sweat.19 Thus, use of protec-tive gowns, gloves, and masks must be used by
health care professionals. In addition, affected patients must be strictly isolated. Equipment must be sterilized before use. No effective treat-ment has been identified for these diseases.
Chemical AgentsThe infamous Tokyo subway sarin attack of 1995 brought the terrifying prospect of gas attacks again into the forefront of international atten-tion. This attack led to thoughtful consideration of other chemical agents that could be used as ter-rorist tools; mustard gas, cyanide, and vesicants were identified. Chemical agents would cause relatively rapid onset of clinical effects ranging from minutes to hours (see Table 21-2).
Cyanide
Clinical FeaturesCyanide uncouples aerobic respiration by disrupt-ing cytochrome oxidase and blocking the final step in oxidative phosphorylation.22 Cyanide lev-els higher than 0.5 mg/dL are considered toxic.23
Signs and SymptomsClinical manifestations of cyanide poisoning are nonspecific and reflect deprivation of oxygen to the heart and to the brain.24 Early manifes-tations include headaches, anxiety, dyspnea, tachycardia, and hypertension. Later manifesta-tions include coma, seizures, hypotension, and ventricular arrhythmias.23
The physical findings include cherry red discoloration of the skin and notably reddened retinal veins, reflecting the cell’s inability to ex-tract oxygen from the blood. Exposed patients might have a bitter almond odor on their breath.24
Y O U R F I R S T C L U E
Signs and Symptoms of Cyanide Exposure
• Rapidlyproducesrespiratoryarrest
• Produceslaboratorytestresultsthatsuggestprofoundandrefractorymetabolicacidosis
Y O U R F I R S T C L U E
Signs and Symptoms of Viral Hemorrhagic Fever
• Conjunctivalinjection
• Discolorationofthesoftpalate
• Hypotension
• Multiorganfailure
Copyright © 2012 by the American Academy of Pediatrics and the American College of Emergency Physicians

Chemical Agents 21-11
TAB
LE 2
1-2
Prim
ary
Ch
emic
al A
gen
ts o
f Ter
rori
sm
Age
nt
Tox
ic E
ffec
tsC
lin
ical
Fin
din
gsO
nse
tD
econ
tam
inat
ion
aM
anag
emen
t
Ner
ve a
gen
ts:
tabu
n, s
arin
, so
man
, VX
An
tich
olin
este
rase
: m
usc
arin
ic,
nic
otin
ic a
nd
CN
S ef
fect
s
Vap
or: m
iosi
s,
rhin
orrh
ea, d
ysp
nea
Liq
uid
: Dia
ph
ores
is,
vom
itin
g
Bot
h: c
oma,
par
alys
is,
seiz
ure
s, a
pn
ea
Seco
nd
s: v
apor
Min
ute
s-h
ours
: li
qu
id
Vap
or: f
resh
air
, rem
ove
clot
hes
, w
ash
hai
r
Liq
uid
: rem
ove
clot
hes
, cop
iou
s w
ash
ing
skin
, hai
r w
ith
soa
p a
nd
w
ater
, ocu
lar
irri
gati
on
AB
Cs
Atr
opin
e: 0
.05
mg/
kg I
Vb
or I
Mc
(min
imu
m, 0
.1 m
g; m
axim
um
, 5
mg)
, rep
eat
ever
y 2–
5 m
in
prn
for
mar
ked
sec
reti
ons,
br
onch
osp
asm
Pral
idox
ime:
25
mg/
kg I
V o
r IM
d (m
axim
um
, 1 g
IV
; 2 g
IM
), ca
n r
epea
t w
ith
in 3
0–60
min
p
rn, t
hen
aga
in e
very
1 h
for
1
or 2
dos
es p
rn f
or p
ersi
sten
t w
eakn
ess,
hig
h a
trop
ine
req
uir
emen
t
Dia
zep
am: 0
.3 m
g/kg
(m
axim
um
, 10
mg)
IV
; Lo
raze
pam
: 0.1
mg/
kg I
V o
r IM
(m
axim
um
, 4 m
g); M
idaz
olam
: 0.
2 m
g/kg
(max
imu
m, 1
0 m
g)
IM p
rn f
or s
eizu
res
or s
ever
e ex
pos
ure
Ves
ican
t:
mu
star
dA
lkyl
atio
nSk
in: e
ryth
ema,
ve
sicl
es
Eye:
infl
amm
atio
n
Res
pir
ator
y tr
act:
in
flam
mat
ion
Hou
rs
Skin
: soa
p a
nd
wat
er
Eyes
: wat
er (o
nly
eff
ecti
ve if
don
e w
ith
in m
inu
tes
of e
xpos
ure
)
Sym
pto
mat
ic c
are
(con
tin
ues
)
Copyright © 2012 by the American Academy of Pediatrics and the American College of Emergency Physicians

21-12 Preparedness for Acts of Nuclear, Biological, and Chemical Terrorism
TAB
LE 2
1-2
Prim
ary
Ch
emic
al A
gen
ts o
f Ter
rori
sm, c
onti
nue
d
Age
nt
Tox
ic E
ffec
tsC
lin
ical
Fin
din
gsO
nse
tD
econ
tam
inat
ion
aM
anag
emen
t
Cya
nid
eC
ytoc
hro
me
oxid
ase
inh
ibit
ion
: ce
llu
lar
anox
ia,
lact
ic a
cid
osis
Tach
ypn
ea, c
oma,
se
izu
res,
ap
nea
Seco
nd
sFr
esh
air
Skin
: soa
p a
nd
wat
er
AB
Cs,
100
% o
xyge
n
Sod
ium
bic
arbo
nat
e p
rn f
or
met
abol
ic a
cid
osis
Sod
ium
nit
rite
(3%
)
Esti
mat
ed
Dos
e (m
L/k
g)
Hgb
(g/d
L)
0.
27
10
0.
33
12
0.
39
14
(max
10/
mL)
Sod
ium
th
iosu
lfat
e (2
5%):
1.65
m
L/kg
(max
imu
m, 5
0 m
L)
Hyd
roxo
coba
lam
in (7
0 m
g/kg
u
p t
o 5
g (a
du
lt d
ose)
Hen
reti
g FM
, Cie
slak
TJ,
Eitz
en Jr
EE.
Bio
logi
cal a
nd
ch
emic
al t
erro
rism
. Jou
rnal
of
Pedi
atri
cs. 2
002;
141
(3):3
11–3
26. R
epri
nte
d w
ith
per
mis
sion
.
Abb
revi
atio
ns:
AB
Cs,
air
way
, bre
ath
ing,
an
d c
ircu
lato
ry s
up
por
t; C
NS,
cen
tral
ner
vou
s sy
stem
; Hgb
, hem
oglo
bin
; IM
, in
tram
usc
ula
rly;
IV,
intr
aven
ousl
y; p
rn, a
s n
eed
ed.
a Dec
onta
min
atio
n, e
spec
iall
y fo
r p
atie
nts
wit
h s
ign
ifica
nt
ner
ve a
gen
t or
ves
ican
t ex
pos
ure
, sh
ould
be
per
form
ed b
y h
ealt
h c
are
pro
fess
ion
als
garb
ed in
ad
equ
ate
per
son
al p
rote
ctiv
e eq
uip
men
t. F
or e
mer
gen
cy
dep
artm
ent
staf
f, t
his
con
sist
s of
non
enca
psu
late
d, c
hem
ical
ly r
esis
tan
t bo
dy
suit
, boo
ts, a
nd
glo
ves
wit
h a
fu
ll-f
ace
air
pu
rifi
er m
ask/
hoo
d.
b In
trao
sseo
us
rou
te is
like
ly e
qu
ival
ent
to t
he
IV r
oute
.c A
trop
ine
mig
ht
hav
e so
me
ben
efit
via
end
otra
chea
l tu
be o
r in
hal
atio
n, a
s m
igh
t ae
roso
lize
d ip
ratr
opiu
m.
dPr
alid
oxim
e is
rec
onst
itu
ted
to
50 m
g/m
L (1
g in
20
mL
of w
ater
) for
IV
ad
min
istr
atio
n, a
nd
th
e to
tal d
ose
infu
sed
for
30
min
, or
can
be
give
n b
y co
nti
nu
ous
infu
sion
(loa
din
g d
ose
of 2
5 m
g/kg
for
30
min
, th
en 1
0 m
g/kg
per
hou
r). F
or I
M u
se, i
t m
igh
t be
dil
ute
d t
o a
con
cen
trat
ion
of
300
mg/
mL
(1 g
ad
ded
to
3 m
L of
wat
er—
by a
nal
ogy
to t
he
US
Arm
y’s
Mar
k 1
auto
inje
ctor
con
cen
trat
ion
) to
effe
ct a
rea
son
able
vol
um
e fo
r in
ject
ion
. Ea
ch M
ark
1 ki
t h
old
s tw
o au
toin
ject
ors,
on
e ea
ch o
f at
rop
ine,
2 m
g (0
.7 m
L), a
nd
pra
lid
oxim
e, 6
00 m
g (2
mL)
; alt
hou
gh n
ot a
pp
rove
d f
or p
edia
tric
use
, th
ey m
igh
t be
con
sid
ered
as
init
ial t
reat
men
t in
dir
e (e
spec
iall
y ou
t-of
-hos
pit
al) c
ircu
mst
ance
s fo
r ch
ild
ren
wit
h s
ever
e, li
fe-t
hre
aten
ing
ner
ve a
gen
t to
xic
effe
cts
wh
o la
ck I
V a
cces
s an
d f
or w
hom
mor
e p
reci
se I
M d
osin
g w
ould
be
logi
stic
ally
imp
ossi
ble.
Su
gges
ted
dos
ing
guid
elin
es a
re o
ffer
ed; n
ote
pot
enti
al e
xces
s of
init
ial a
trop
ine
and
pra
lid
oxim
e d
ose
for
age
and
wei
ght,
alt
hou
gh w
ith
in g
ener
al g
uid
elin
es f
or r
ecom
men
ded
tot
al d
uri
ng
the
firs
t 60
to
90 m
inu
tes
of t
her
apy
of
seve
re e
xpos
ure
s:
Ap
pro
xim
ate
Age
, yA
pp
rox
imat
e W
eigh
t, k
gN
o. o
f A
uto
inje
ctor
s (E
ach
Typ
e)
Atr
opin
e D
ose
Ran
ge,
mg/
kg
Pral
idox
ime
dos
e ra
nge
(m
g/k
g)
3–7
13–2
5 1
0.08
–0.1
324
-46
8–14
6–
50
20.
08–0
.13
24-4
6
>14
>
51
3≤0
.11
35 o
r le
ss
Copyright © 2012 by the American Academy of Pediatrics and the American College of Emergency Physicians

Chemical Agents 21-13
Nerve Agents (Sarin Gas)
Clinical FeaturesNerve agents are organophosphate analogues that lead to overstimulation of cholinergic receptors. The organophosphorus compounds have been known since the early 1800s and are synthesized by combining alcohols with phosphoric acid.27
Signs and SymptomsAt low exposure levels, pupils constrict and vi-sion is interrupted for several days.27,28 For higher doses, acetylcholinesterase activity is inhibited.27
Acetylcholinesterase is the enzyme responsi-ble for breakdown of acetylcholine in the synapse. As this enzyme’s activity is compromised, toxic levels of acetylcholine build at the synapse, result-ing in cholinergic toxicity. Salivation, lacrimation, urinary incontinence, defecation, and vomiting result. Severe nerve agent exposure produces se-vere bronchorrhea, resulting in respiratory com-promise, hypoxia, coma, and ultimately death.29
Long-term effects of sarin exposure among survivors include neurobehavioral syndromes, personality changes, new-onset headaches, and memory deficits.29
Diagnostic Studies and ManagementThe early and ultimate goal of treatment for nerve agent exposure is to restore cholinester-ase activity. After sarin exposure, the half-life for “aging” (irreversible cholinesterase inhibition) is approximately 5 hours. Once aging occurs, acetylcholinesterase is not able to metabolize acetylcholine again.30,31
Treatment first involves decontamination of patients. For most agents, soap and water will suf-fice, but for liquid formulations of nerve agents, methodical cleaning with thorough scrubbing must be undertaken. The patient should be taken to a well-ventilated area. Clothing that is removed should be double-bagged to protect patients and caretakers from exposure. Physicians must be wary of direct contact with patients because they can still be subject to exhaled poison.31
Patients exposed to cholinergic toxins should receive appropriate supportive care. If they expe-rience isolated eye symptoms (miosis, conjunc-tival injection, or ocular pain), atropine is not indicated and will not work.31 These patients can be treated with tropicamide ophthalmic drops.30
The differential diagnosis for cyanide poi-soning includes drug intoxication, hypogly-cemia, electrolyte disturbances, and postictal state. A hallmark of cyanide poisoning is the presence of a profound and refractory metabolic acidosis and increased anion gap.22
Children might be particularly vulnerable to the effects of cyanide, although there have not been many studies documenting this. Children’s vulnerability seems to reflect their higher re-spiratory rate, their lower body mass, and their immature metabolic mechanisms.24
Long-term effects of cyanide exposure in-clude parkinsonism, dysarthria, ataxia, and overall intellectual decline.
Diagnostic Studies and ManagementManagement of cyanide poisoning begins with removal of the patient from the source, car-diopulmonary resuscitation, and provision of 100% oxygen via nonrebreather mask or en-dotracheal tube. One treatment option is the use of the cyanide antidote kit, which contains amyl nitrite, sodium nitrite, and sodium thiosul-fate.24,25 Amyl nitrite ampules are crushed and the contents inhaled. This is followed by the use of intravenous (IV) sodium nitrite to induce methemoglobinemia.24 Methemoglobinemia is desirable in this clinical context because cyanide has a higher affinity for methemoglobin than it does for cytochrome oxidase. Once cyanide combines with methemoglobin, sodium thio-sulfate is added. The sodium thiosulfate acts as a sulfur atom donor, forming thiocyanate, a compound readily excreted in the urine.22,24,26
The induction of methemoglobinemia can be risky. High concentrations of methemoglo-bin reduce the oxygen-carrying capacity of the blood and can be dangerous and even fatal.22,24 A new agent, hydroxycobalamin (Cyanokit), is gaining favor as the antidote of choice for acute cyanide intoxication. Hydroxycobalamin directly combines with cyanide to form cyano-cobalamin (vitamin B
12), which is excreted in
the urine. The compound produces a reddish discoloration of the skin, mucous membranes, and urine and can induce self-limited hyperten-sion.25 The current adult treatment is 5 g of IV hydroxycobalamin.24,25 A pediatric dose of 70 mg/kg has been used in France.24
Copyright © 2012 by the American Academy of Pediatrics and the American College of Emergency Physicians

21-14 Preparedness for Acts of Nuclear, Biological, and Chemical Terrorism
If patients have signs of systemic cholinergic toxic effects, they should receive initial therapy with atropine right away. They should immedi-ately receive 2 or 4 mg of atropine with retreat-ment every 5 to 10 minutes with persistent signs of respiratory distress.31 If the patient requires rapid sequence intubation, succinylcholine should be avoided because it is metabolized by plasma cholinesterases.30
Patients will benefit from atropine, which will serve to block the activity of synaptic ace-tylcholine and, in particular, benefit from early administration of pralidoxime. Pralidoxime restores acetylcholinesterase activity if rapidly administered before “aging.”
Sarin has been demonstrated to inhibit the release of central nervous system g-aminobu-tyric acid supplies, resulting in a lowered sei-zure threshold. Benzodiazepines, particularly valium, have been shown to prevent seizures from developing and therefore should be ad-ministered with atropine and pralidoxime.31
As patients recover from their exposures, erythrocyte acetylcholinesterase activity can be measured as an index of poisoning.30
Vesicant
Clinical FeaturesMustard is a vesicant sought by terrorist orga-nizations. Mustard gas was invented in 1886 by Meyer and was first used in 1917 in Belgium. There it killed 5,000 soldiers immediately and created 10,000 additional casualties.32
Mustard is an oily liquid that smells faintly like garlic and is capable of penetrating cloth-ing.33 The gas is highly lipophilic and concen-trates in the skin, eyes, gastrointestinal tract, and respiratory tract.34 Mustard gas alkylates DNA, inhibits mitosis, decreases tissue respiration, and ultimately leads to cell death.32
Signs and SymptomsThe mortality rate after exposure is approxi-mately 3%.33 When death occurs, it is usually secondary to overwhelming infection. The most susceptible areas for gas exposures are the warm and moist areas of the groin and axillae.33 In these areas, deep and painful burns can develop.
Long-term effects include the development of tracheobronchial stenosis, bronchiectasis,
and, most notably, chronic bronchitis.34 Bron-chiolitis obliterans has also been documented.35 Chronic respiratory disease ultimately leads to right heart strain and cor pulmonale.32
Patients exposed to mustard will also experi-ence desquamation of their skin after the develop-ment of flaccid blisters that are prone to infection. These patients will require careful wound care, debridement, burn treatment, and antibiotics.36
Diagnosis and TreatmentTherapy for vesicant gas exposure consists of rapid decontamination and supportive care. The patients, although frequently able to survive the initial attack, will represent a significant and continued source of disease and strain on the affected population.
Nuclear Agents
Radiation Exposure
Clinical FeaturesRadiation exposure is one of the most feared and potentially devastating of all terrorist ac-tions. Any radiation release, unintentional or deliberate, would produce significant panic and psychological stress among those affected, even with a minimal, non–life-threatening exposure.
Signs and SymptomsRadiation exposure damages tissue directly through imparting high-energy particles and indirectly via the generation of oxygen free radi-cals. If enough tissue is disturbed, organ failure results. The tissues most at risk include rapidly dividing cells. Thus, the intestinal mucosa and the bone marrow are at particular risk.37
Damage to progenitor cells in the bone mar-row sets the stage for hematopoietic malignant tumors, beginning as early as 2 years after ex-posure.38 Solid organ malignant tumors tend to lag behind and on average begin 10 years after initial exposures.38 In the wake of the Chernobyl meltdown, childhood thyroid cancer peaked 4 years after the initial exposure.38
Children are a particularly vulnerable group because of their greater minute ventilation (in-haled gases) and because they are closer to the ground (radioactive fallout).38 Infants rely on
Copyright © 2012 by the American Academy of Pediatrics and the American College of Emergency Physicians

Conclusions 21-15
their mother’s milk for nutrition. Radioactive io-dine concentrates in maternal mammary glands, making this an unsafe source of nutrition.38
Pediatric gonads experience a dose-de-pendent reduction in fertility after radiation exposure.39 The eyes, too, are a particularly vulnerable site. Doses as little as 0.2 Gy can cause cataracts.39 Fetal radiation exposure produces growth retardation, congenital malformations, carcinogenesis, and fetal death.39
Whole-body exposure to penetrating ra-diation or internal absorption will result in acute radiation syndrome. The symptoms vary with individual radiation sensitivity, type of ra-diation, and dose absorbed.39 Within 6 to 12 hours of a significant exposure, the syndrome typically begins with a prodromal phase. This is manifested by rapid onset of nausea, vomiting, diarrhea, headache, and, in more severe cases, fever.37,39 In fact, the time to emesis decreases with increasing radiation dose.37 The gastroin-testinal manifestations last 24 to 48 hours and are followed by a latent phase, during which the patient is relatively asymptomatic. The latent phase typically lasts up to 2 weeks, although it can be absent in very severe exposures.37,39 The overt or critical illness phase follows and is dose dependent. At doses exceeding 2 Gy, the bone marrow is injured, with the resulting hemato-poietic syndrome. Many patients will have lym-phopenia within 48 hours of exposure, which can predict the occurrence of this syndrome.37–39 These patients usually have maximal neutro-penia and thrombocytopenia at 3 to 4 weeks, when infection and hemorrhage are the primary challenges to medical care.37,39
Without treatment, the midlevel lethal ra-diation is 3.5 Gy (the dose that will kill 50% of the population within 30 days).37 Casualties whose radiation exposure range from 2 to 6 Gy are most amenable to treatment. Nearly every-one who receives more than 6 Gy is unlikely to survive.37
Nuclear power plant incidents and atomic or nuclear weapon detonation result in high-level radiation exposure with multiple types of radioactive isotopes and particles that persist in the environment. The more likely terror-ism scenario is a single isotope (eg, cesium)
dispersed either manually or in the water system or detonated with a conventional explosive to disperse the radioactive material (known as a “dirty bomb”). The degree and amount of radio-activity are much smaller and can be limited to a specific isotope that can have a specific antidote or protection measure.
Diagnosis and TreatmentEarly treatment means removing patients from the source of radiation and, in particular, re-moving all of their clothing and shoes. Removal of outer clothing reduces contamination by ap-proximately 90%.37,38 Decontamination includes assessment of contamination with a radiation detector, washing the skin and hair with warm water and soap, and gentle brushing to dislodge particles on the skin, followed by repeat radia-tion assessment.37,38,40 For patients who have in-ternal contamination with radioactive materials, biologic fluids, including saliva, blood, urine, and stool, must be handled carefully.38
Initial management includes assessment of the ABCs. Patients with exposures should un-dergo blood work, including a complete blood cell count with differential every 4 to 6 hours to check for decreasing lymphocyte and neu-trophil counts.37 Potassium iodide should be rapidly administered after a radiation disaster but not after a “dirty bomb”38 (see Table 21-3). Potassium iodide floods the thyroid with iodine, blocking the uptake of inhaled or ingested ra-dionuclides. Potassium iodide is generally well tolerated but should be avoided in patients with dermatitis herpetiformis and hypocomplement-emic vasculitis. Adverse effects include rash and gastric upset.38 Recommendations for repeated dosing depend on environmental evaluation by federal or state authorities.38
Treatment for internal contamination with other potential radioactive elements is listed in Table 21-4, but expert consultation is advised be-fore treatment because experience in pediatric patients is limited.
ConclusionsThe world we live in has changed forever, and we need to be prepared to react. Children are
Copyright © 2012 by the American Academy of Pediatrics and the American College of Emergency Physicians

21-16 Preparedness for Acts of Nuclear, Biological, and Chemical Terrorism
of fear and contagion. We must work to build robust response capabilities into our pharma-ceutical companies and pressure international leaders to destroy stores of nuclear, chemical, and biological weapons. These combined steps will translate into our own safety and the safety of generations to come.
both vulnerable and innocent and should be
protected from the violence of war and terror. As
health care professionals, we have an obligation
to help protect the public health.
When faced with disaster, we must work as
coordinated teams to help prevent the spread
TABLE 21-3 Threshold Thyroid Radioactive Exposures and Recommended Doses of Potassium Iodide for Different Risk Groups
Patient Age Predicted Thyroid Exposure, Gy (rad)
Potassium Iodide Dose, mg
No. of 130-mg Tablets
No. of 65-mg Tablets
>40 ya >5 (500) 130 1 2
>18–40 y >0.1 (10) 130 1 2
Pregnant or lactating
≥0.05 (5) 130 1 2
>12–18 yb ≥0.05 (5) 65 ½ 1
>3–12 ≥0.05 (5) 65 ½ 1
>1 mo to 3 yc ≥0.05 (5) 32 ¼ ½
Birth to 1 moc,d ≥0.05 (5) 16 / ¼
Adapted from: American Academy of Pediatrics Committee on Environmental Health. Policy Statement: Radiation Disasters and Children. Pediatrics. 2003;111:1455–1466.aOlder patients are more likely to experience adverse effects from potassium iodide, including iodine-induced thyrotoxicosis, goiter, and hypothyroidism in iodide-deficient areas.bAdolescents approaching 70 kg or more in weight should be given the full adult dose (130 mg).cInfants and young children can be given potassium iodide as a fresh saturated solution diluted in milk, formula, syrup (raspberry disguises the taste best), or flat cola soda.dNeonates should have their thyrotropin and free thyroxine monitored with free thyroxine (levothyroxine) replacement therapy as needed. Adverse effects can also include gastrointestinal distress, rash, and sialadenitis.
81
Copyright © 2012 by the American Academy of Pediatrics and the American College of Emergency Physicians

Conclusions 21-17
TABLE 21-4 Radioactive Elements and Treatment Modalities
Radioactive Element Absorption Therapeutic Approach
Treatment
Americium 241 Wounds, GI or non-GI Chelation Ca-DTPA then Zn-DTPA if in first 24–48 h
Cesium 134,137 Inhalation, GI, wound Reduction of GI absorption
Prussian blue
Cobalt 60 Inhalation, <5% GI Reduction of GI absorption chelation if severe
Gastric lavage, purgatives; severe cases use penicillamine
Iodine 125, 131,132,134,135
Primarily thyroid Blockage mobilization Potassium iodide; alternatives are propylthiouracil or methimazole
Phosphorus 32 All sites Lavage, aluminum hydroxide, oral phosphates
Plutonium 239,238 Inhalation, GI or non-GI wounds variable
Reduction of GI absorption chelation
Ca-DTPA within 24 h followed by Zn-DTPA
Radium 226 GI Reduction of GI absorption
Mobilization
10% Magnesium sulfate lavage followed by saline and magnesium purgatives, ammonium chloride can increase stool elimination
Strontium 89,90 Inhalation, GI Reduction of GI absorption blockage, displacement, mobilization
Aluminum phosphate orally stable strontium can competitively inhibit metabolism; increase urinary excretion by acidification with ammonium chloride and large doses of calcium
Tritium (hydrogen 3) Inhalation, GI Dilution Hydration with caution to avoid iatrogenic water intoxication
Uranium 238,235, 239 Inhalation Mobilization Sodium bicarbonate and tubular diuretics to decrease renal toxic effects
Abbreviations: Ca-DTPA, pentetate calcium trisodium; GI, gastrointestinal; Zn-DTPA, pentetate zinc trisodium.
Adapted from: Koenig KL, Goans RE, Hatchett RJ, et al. Medical treatment of radiologic casualties. Ann Emerg Med. 2005;45:643–65237 and Allen JY, Endom EE. Management of radiation injury in children. In: Wiley JF, ed. UpToDate. Waltham, MA: UpToDate; 2010.
Copyright © 2012 by the American Academy of Pediatrics and the American College of Emergency Physicians

21-18 Preparedness for Acts of Nuclear, Biological, and Chemical Terrorism
Check Your Knowledge1. An afebrile patient with mediastinal
widening and pleural effusions is most likely to have:A. tularemia.B. anthrax.C. botulism.D. pneumococcal pneumonia.E. viral hemorrhagic fever.
2. Which of the following is FALSE regarding botulism?A. Patients experience an ascending
paralysisB. A single gram of aerosolized toxin
could kill 1.5 million peopleC. There can be a latency of up to 24
hours before patients are symptomaticD. Botulism can resist gastric acidityE. Death is secondary to respiratory
failure3. Which of the following is FALSE
regarding smallpox?A. Lesions begin on the torso and spread
out from thereB. Strict precautions must be maintained
when ministering to smallpox patients C. Mortality rate is approximately 30%D. Postexposure vaccination can
reduce severity of disease in affected individuals
E. It is widely believed that stores of weaponized smallpox still exist
4. The following are long-term effects of sarin exposure EXCEPT:A. personality change.B. new-onset headaches.C. memory deficits.D. neurobehavioral syndromes.E. hypersalivation.
5. The following are anatomical sites that are particularly vulnerable to radiation exposure EXCEPT:A. the heart.B. the small intestine.C. the bone marrow.D. the eyes.E. the gonads.
6. All of the following are early manifestations of cyanide exposure EXCEPT:A. headaches.B. anxiety.C. dyspnea.D. bradycardia.E. hypertension.
References1. Hu YY, Adams RE, Boscarino JA, et al. Training needs of
pediatricians facing the environmental health and bioterrorism consequences of September 11th. Mt Sinai J Med. 2006;73:1156–1164.
2. Graham J, Shirm S, Liggin R, Aitken ME, et al. Mass casualty events at schools: a national preparedness survey. Pediatrics. 2006;117:e8–e15.
3. Thompson T, Lyle K, Mullins SH, et al. A state survey of emergency department preparedness for the care of children in a mass casualty event. Am J Disaster Med. 2009;4:227–232.
4. Markenson D, Reynolds S. The pediatrician and disaster preparedness. Pediatrics. 2006;117:e340–e362.
5. Lewerin, et al. Anthrax outbreak in a Swedish beef cattle herd-first case in 27 years: case report. Acta Veterinaria Scandinavica. 2010;52:7.
6. Swartz MN. Recognition and management of anthrax—an update. N Engl J Med. 2001;345:1621–1626.
7. Bravata DM, Wang E, Holty JE, et al. Pediatric Anthrax: Implications For Bioterrorism Preparedness: Evidence Report/Technology Assessment, Agency for Health Care Research and Quality. Washington, DC: US Dept of Health and Human Services; 2006:141.
8. Wilson, KH. Clinical manifestations and diagnosis of anthrax. In: Sexton DJ, ed. UpToDate. Waltham, MA: UpToDate; 2009.
9. Pegram PS, Stone SM. Botulism. In: Bartlett JG, ed. UpToDate. Waltham, MA: UpToDate; 2009.
10. Patt HA, Feigin RD. Diagnosis and management of suspected cases of bioterrorism: a pediatric perspective. Pediatrics. 2002;109:685–692.
11. Zhang JC, Sun L, Nie QH. Botulism, where are we now? Clin Toxicol. 2010;48:867-879.
12. Wayangankar S, Jackson R, Bronze MS, et al. Plague. Emedicine. October 2009.
13. Inglesby TV, Dennis DT, Henderson DA, et al. Plague as a biological weapon: medical and public health management. JAMA. 2000;283:2281–2290.
14. Margolis DA, Burns J, Reed Sl, et al. Case report: septicemic plague in a community hospital in California. Am J Trop Med Hyg. 2008;78:868–871.
15. Hogan CJ, Harchelroad F. Smallpox. Emedicine. 2009.16. Friedman HM, Isaacs SN. Smallpox. In: Hirsch MS, ed.
UpToDate. Waltham, MA: UpToDate; 2010.17. Everett ED. Clinical manifestations, diagnosis, and treatment
of tularemia. In: Calderwood SB, Edwards MS, eds. UpToDate. Waltham, MA: UpToDate; 2010.
18. Bossi P, Tegnell A, Baka A, et al. Bichat guidelines for the clinical management of tularemia and bioterrorism related tularemia. Eurosurveillance. 2004;9:e9–e10.
19. Obrien KK, Higdon ML, Halverson JJ. Recognition and management of bioterrorism infections. Am Fam Physician. 2003;67:1927–1934.
20. Bray M. Diagnosis and treatment of Ebola and Marburg hemorrhagic fever. In: Hirsch MS, ed. UpToDate. Waltham, MA: UpToDate; 2010.
C H A P T E R R E V I E W
Copyright © 2012 by the American Academy of Pediatrics and the American College of Emergency Physicians

Chapter Review 21-19
21. Centers for Disease Control and Prevention. http://www.emergency.cdc.gov/agent/vhf/. Accessed June 15, 2011.
22. Riordan M, Rylance G, Berry K. Poisoning in children 5: rare and dangerous poisons. Arch Dis Child. 2002;87:407–410.
23. Mokhlesi B, Leikin JB, Murray P, et al. Adult toxicology in critical care: part II: specific poisonings. Chest. 2003;123:897–922.
24. Geller RJ, Barthold C, Saiers JA, Hall AH. Pediatric cyanide poisoning: causes, manifestations, management, and unmet needs. Pediatrics. 2006;118:2146–2158.
25. Hall AH, Dart R, Bogdan G. Sodium thiosulfate or hydroxycobalamin for the empiric treatment of cyanide poisoning? Ann Emerg Med. 2007;49:806–813.
26. Martin CO, Adams HP Jr. Neurological aspects of biological and chemical terrorism: a review for neurologists. Arch Neurol. 2003;60:21–25.
27. Khurana D, Prabhakar S. Organophosphorus intoxication. Arc Neurol. 2000;57:600–602.
28. Kato T, Hamanaka T. Ocular signs and symptoms caused by exposure to sarin gas. Am J Emerg Med. 2000;18:113–114.
29. Newmark J. Therapy for nerve agent poisoning. Arch Neurol. 2004;61:649–652.
30. Lee EC. Clinical manifestations of sarin nerve gas exposure. JAMA. 2003;290:659–662.
31. Leikin JB, Thomas RG, Walter FG, Klein R, Meislin HW. A review of nerve agent exposure for the critical care physician. Crit Care Med. 2002;30:2346–2354.
32. Freitag L, Firusian N, Stamatis G, Greschuchna D. The role of bronchoscopy in pulmonary complications due to mustard gas inhalation. Chest. 199;100:1436–1441.
33. Evison D, Hinsley D, Rice P. Chemical Weapons. BMJ. 2002;324:332–335.
34. Emad A, Rezaian GR. The diversity of the effects of sulfur mustard gas inhalation on respiratory system 10 years after a single heavy exposure: analysis of 197 cases. Chest. 1997;112:734–738.
35. Thomason JW, Rice TW, Milstone AP. Bronchiolitis obliterans in a survivor of a chemical weapons attack. JAMA. 2003;290:598–599.
36. Momeni AZ, Enshaeih S, Meghdadi M, Amindjavaheri M. Skin manifestations of mustard gas: a clinical study of 535 patients exposed to mustard gas. Arch Dermatol. 1992;128:775–780.
37. Koenig KL, Goans RE, Hatchett RJ, et al. Medical treatment of radiological casualties: current concepts. Ann Emerg Med. 2005;45:643–652.
38. American Academy of Pediatrics Committee on Environmental Health. Radiation disasters and children. Pediatrics. 2003;111(6 pt 1):1455–1466.
39. Allen JY, Endom EE. Clinical features of radiation injury in children. In: Wiley JF, ed. UpToDate. Waltham, MA: UpToDate; 2010.
40. Allen JY, Endom EE. Management of radiation injury in children. In: Wiley JF, ed. UpToDate. Waltham, MA: UpToDate; 2010.
CASE
SUM
MAR
Y 1 YouareworkingthemedicalcontroltelephoneatChildren’sHospitalandreceivea
callfromparamedics,whoarebringinginschoolchildrenexposedtoadowntowngasattack.Thehazardousmaterialsteamhasyettoidentifytheagentbuttellsyouthatmanypeoplearedeadonthescene.Thosewhoarenotdeadareinextremissecondarytorespiratorydistress.Seizuresarenotedinsomepatients.Othershaveastrangereddishhue.Theemergencymedicalservicesofficialsreportthatthefirstpatienttheyarebringingtoyouishypotensive.
1. What agent is most likely to cause this presentation?2. What type of decontamination or treatment is needed?
Basedonknockoutpresentationandreddenedappearanceofpatientsandseizureactivityandhypotension,cyanidepoisoningisthemostlikelyexplanationforthepatient’ssymptoms.Patientsshouldbeundressed,cardiopulmonaryresuscitationbegunasneeded,100%oxygenbynonrebreathermaskprovided,intubationperformedifneeded,andemergentadministrationofhydroxycobalaminundertaken.
Photo Credits
Opener © Asianet-Pakistan/Alamy Images; 21-1 Courtesy CDC/Dr. P.S. Brachman; 21-2 Courtesy CDC/Dr. John Noble, Jr
Unless otherwise indicated, all photographs and illustrations are under copyright of Jones & Bartlett Learning, courtesy of Maryland Institute for Emergency Medical Services Systems, or the American Academy of Pediatrics.
Some images in this book feature models. These models do not necessarily endorse, represent, orparticipate in the activities represented in the images.
C H A P T E R R E V I E W
Copyright © 2012 by the American Academy of Pediatrics and the American College of Emergency Physicians