Embed Size (px)
Citation preview

Spine Deformity 2 (2014) 70e75www.spine-deformity.org
Preoperative Pulmonary Function in Patients With OperativeScheuermann Kyphosis
Gaurav Abbi, MDa, Baron S. Lonner, MDa,*, Courtney S. Toombs, BAa,Paul D. Sponseller, MDb, Amer F. Samdani, MDc, Randal R. Betz, MDc, Suken A. Shah, MDd,
Peter O. Newton, MDe
aDepartment of Orthopaedics, New York University Hospital for Joint Diseases, 820 Second Avenue, New York, NY 10017, USAbDepartment of Orthopaedics, Johns Hopkins Hospital, 1800 Orleans St, Baltimore, MD, 21287, USA
cDepartment of Orthopaedics, Shriners Hospital for Children, 3551 N. Broad Street, Philadelphia, PA, 19140, USAdDepartment of Orthopaedics, Alfred I. duPont Hospital for Children, 1600 Rockland Road, Wilmington, DE, 19803, USAeDepartment of Orthopaedics, Rady Children’s Hospital San Diego, 3020 Children’s Way, San Diego, CA, 92123, USA
Received 10 April 2013; revised 31 July 2013; accepted 3 September 2013
Abstract
Study Design: A multicenter, prospective study of consecutively enrolled surgical patients with Scheuermann kyphosis (SK).Objectives: To evaluate the impact of SK on preoperative pulmonary function and to determine which radiographic criteria may helppredict pulmonary impairment.Summary of Background Data: Pulmonary function in SK is not well studied. Previous studies on adolescent idiopathic scoliosis re-vealed that certain factors, including the magnitude of the thoracic curve and the number of vertebrae involved, significantly affectpulmonary function.Methods: A total of 64 patients with SK were evaluated. Absolute and percent predicted forced vital capacity (FVC), forced expiratoryvolume in 1 second, and total lung capacity were collected preoperatively. Subjects were divided according to kyphosis apex (thoracic orthoracolumbar) and kyphosis magnitude groups, and compared. Correlation analysis was performed to evaluate the impact of gender, age,
Author disclosures: GA (grant to the Setting Scoliosis Straight Foun-
dation from DePuy Spine, Inc.); BSL (grants from DePuy Synthes Spine
to the Setting Scoliosis Straight Foundation, DePuy Spine, AOSpine,
OREF, The Jon and Marcella Fox Fund; board membership with Spine
Search; consultancy with DePuy; payment for lectures including service
on speakers bureaus for DePuy Spine Synthes and K2M; royalties from
DePuy Synthes Spine; stock/stock options from Spine Search, Paradigm
Spine); CST (grant to the Setting Scoliosis Straight Foundation from
DePuy Spine Inc.); PDS (grant from DePuy Synthes Spine to the Setting
Scoliosis Straight Foundation, DePuy Synthes Spine; consultancy for
DePuy Synthes Spine; royalties from DePuy Synthes Spine); AFS (grant
to the Setting Scoliosis Straight Foundation from DePuy Spine, Inc.;
consultancy for DePuy Synthes Spine, Zimmer Spine, SpineGuard,
Stryker; payment for manuscript preparation for DePuy Synthes Spine;
support for travel to meeting for the study or other purposes from grant
to the Setting Scoliosis Straight Foundation from DePuy Spine, Inc.);
RRB (grant from DePuy Synthes Spine to the Setting Scoliosis Straight
Foundation; board membership with Chest Wall and Spine Deformity
Study Group, Setting Scoliosis Straight Foundation; consultancy with
DePuy Spine, Synthes, Orthocon, SpineGuard, Medtronic; grants from
DePuy Spine, Synthes; payment for lectures including service on speakers
bureaus for DePuy Spine Synthes; royalties from DePuy Synthes Spine;
stock/stock options from SpineGuard, MiMedx, Orthocon, Orthobond);
SAS (grant from DePuy Synthes Spine to the Setting Scoliosis Straight
Foundation; board membership with grant from the Setting Scoliosis
Straight Foundation; consultancy for DePuy Synthes Spine and Ethicon
Endosurgery; grants from DePuy Synthes Spine; royalties from DePuy
Synthes Spine and Arthrex; payment for the development of educational
presentations from DePuy Synthes Spine; stock/stock options from
Globus Medical); PON (grant from the Setting Scoliosis Straight Founda-
tion; consulting fee/honorarium from DePuy Spine; support for travel to
meetings from DePuy Spine; board membership with POSNA, Harms
Study Group Foundation, Scoliosis Research Society, Children’s
Specialist Foundation; consultancy for DePuy Spine, Stanford University;
employment with Children’s Specialists of San Diego; expert testimony
for NorCal, law firm Carroll, Kelly, Trotter, Franzen, & McKenna, law
firm Smith, Haughey, Rice, & Roegge; grants from NIH, OREF, POSNA,
SRS, Harms Study Group Foundation, DePuy Synthes Spine, Axial
Biotech, Biospace/Med/EOS Imaging; payment for lectures including
service on speakers bureaus from DePuy Spine; patents from DePuy Syn-
thes Spine; royalties from DePuy Synthes Spine, Thieme Publishing;
payment for the development of educational presentations from DePuy
Synthes Spine; stock/stock options from Nuvasive).
This work was supported by a grant from DePuy Spine, Raynham,
MA, USA to the Setting Scoliosis Straight Foundation in support of the
Harms Study Group’s research.
*Corresponding author. Department of Orthopaedics, New York Univer-
sity Hospital for Joint Diseases, 820 Second Avenue, New York, NY 10017,
USA. Tel.: þ1 212-986-0140; fax: þ1 212-986-0160.
E-mail address: [email protected] (B.S. Lonner).
2212-134X/$ - see front matter � 2014 Scoliosis Research Society.
http://dx.doi.org/10.1016/j.jspd.2013.09.004

71G. Abbi et al. / Spine Deformity 2 (2014) 70e75
kyphosis magnitude, and apex on pulmonary function. American Thoracic Society guidelines were used to classify patients according to theseverity of pulmonary impairment.Results: Mean age was 16 years (range 13e24 years), with 42 males. The percent predicted forced vital capacity was 95.8%, percentforced expiratory volume in 1 second was 92.5%, and percent total lung capacity was 106.2%. The percent predicted FVC differedsignificantly between the 71�e80� and 81�e90� groups (105% vs. 83%, respectively; p 5 .016) and the 71�e80� and greater than 90�
groups (105% vs. 73%, respectively; p 5 .009). For percent predicted TLC, patients with greater than 90� had significantly lower averagevalues than those in the 71�e80� range (79% vs. 115%, respectively; p 5 .016). Greatest kyphosis showed a fairly weak (r 5 e.24;p ! .10) but significant correlation with percent predicted FVC. The percentage of patients with moderate to severe impairment (4%) waslowest in the 71�e80� range, which increased with increasing ranges of kyphosis magnitude: 81�e90� (11%) and greater than 90� (50%).� 2014 Scoliosis Research Society.
Keywords: Scheuermann kyphosis; Pulmonary function testing
Introduction
In 1920, Scheuermann [1] first described a spinaldeformity characterized by a rigid hyperkyphosis that hedistinguished from a flexible, correctable, postural hunch-back. This became known as Scheuermann kyphosis (SK),defined by fixed wedged vertebrae and end plate irregu-larities [2,3]. Operative management has been advocatedfor progressive kyphosis over 70�, intractable back pain,and unacceptable cosmetic deformity [4,5].
Pulmonary function in patients with adolescent idio-pathic scoliosis (AIS) is well studied. Adolescent idiopathicscoliosis is a more commonly occurring spinal deformitydiagnosis involving a similar adolescent population, andtherefore provides a reasonable comparison with SKpatients. Weinstein et al. [6] concluded that there is a directcorrelation between the severity of the thoracic curve inAIS and diminishment in pulmonary function. Newtonet al. [7] determined that the magnitude of the thoraciccurve, the number of vertebrae involved, thoracic hypo-kyphosis, and coronal imbalance all had a minimal butsignificant effect on preoperative pulmonary function tests(PFTs) in operative AIS patients. Numerous other studies inthis population have been performed [8-12], but mostaddress pulmonary function postoperatively with anteriorsurgery and/or thoracoplasty.
Unlike idiopathic scoliosis, there have been few reportson the impact of SK on pulmonary function. Murray et al.[13] reported decreased vital capacity and restrictive lungdisease in those with kyphosis greater than 100�. Dimin-ished pulmonary function was classically defined by Wengand Levison [14] as less than 80% of expected forced vitalcapacity (FVC) and/or forced expiratory volume in 1second (FEV1). Other natural history studies exist [15,16],but the study by Murray et al. is the only one to the authors’knowledge that addresses pulmonary function in Scheuer-mann disease.
The use of PFTs in the preoperative evaluation of SK hasnot been established. Some have stated that PFT is neces-sary in the preoperative evaluation of AIS to determinepreoperative risk [17,18]. The purposes of this study wereto assess the impact of operative SK on preoperativepulmonary function and to determine which radiographic
criteria, if any, may help predict pulmonary impairment inthis population.
Materials and Methods
A prospective, multicenter study of SK (ages 10e25years) involving 10 United States institutions where PFTsare performed for research purposes was conducted.Subjects included in this study were operative SK patientswho were diagnosed with either classical SK or idiopathicstructural kyphosis, and who were between the ages of 10and 25 years. Operative SK included patients who wereindicated for surgery for kyphosis associated with painunresponsive to exercise and physical therapy, or severedeformity, progressive deformity despite bracing, and largemagnitude rigid deformity greater than 70� for thoracicapex and greater than 45� for thoracolumbar apex. Anypatient with neuromuscular kyphosis or other seriouscomorbidities or a prior surgery was excluded. The studydatabase was queried for all SK patients who had completepreoperative PFT data and full-length posteroanterior andlateral radiographs available. Radiographs of the spine weretaken preoperatively with the patient standing (bendingradiographs were also obtained on all patients beforesurgery). Preoperative PFT was assessed in 64 patients.
Pulmonary function testing included absolute andpercent predicted FVC (%FVC), absolute and percentpredicted FEV1 (%FEV1), and absolute and percent pre-dicted total lung capacity (%TLC). Demographic data,T2eT12 and T5eT12 kyphosis, greatest sagittal Cobbkyphosis, and apex of kyphosis were determined for eachpatient. Patients were divided into 2 groups based onkyphosis apex: thoracic (T), apex proximal to or at T10,and thoracolumbar (TL), apex distal to T10/T11. Patientswere also stratified by greatest Cobb kyphosis to determinethe relationship between the magnitude of deformityand PFTs.
Spearman rho nonparametric correlations were calculatedto evaluate the impact of gender and kyphosis apex onpulmonary function. Pearson’s correlation coefficients werecalculated to compare PFTs depending on age, T2eT12kyphosis, T5eT12 kyphosis, and greatest sagittal Cobb angle.

Table 1
Pulmonary function test data (overall and stratified by greatest Cobb deformity).
N Forced vital capacity Forced expiratory volume in 1
second
Total lung capacity
Liters % predicted Liters % predicted Liters % predicted
<60 � 6 4.69�0.86 91�13 3.99�0.78 89�12 6.70�1.5 100�21
61 �e70 � 20 4.05�0.71 97�17 3.33�0.69 92�21 5.60�1.05 108�18
71 �e80 � 24 4.34�0.86 105�14 3.68�0.77 100�15 5.98�1.05 115�20
81 �e90 � 9 4.12�1.38 83�25 3.52�1.02 83�21 5.98�1.25 97�16
O90 � 5 4.23�0.84 73�14 3.35�0.96 78�16 5.02�1.66 79�17
All 64 4.25�0.89 96�19 3.56�0.80 93�19 5.89�1.20 106�21
p .598 .002* .477 .053** .293 .016***
All reported p values are for comparison between all 5 curve magnitude groups using analysis of variance. Post hoc tests revealed individual differences
between specific curve magnitude groups and their accompanying p values, cited below, which are the source of the total significance.
* Overall significant difference is the result of differences between 71 �e80 � versus 81 �e90 � (p 5 .016) and 71 �e80 � and greater than 90 � (p 5 .009);
** overall significant difference is the result of the difference between 71 �e80 � versus greater than 90 � (p5 .014); *** post hoc tests showed no p values! .10.
72 G. Abbi et al. / Spine Deformity 2 (2014) 70e75
Patients were also categorized based on AmericanThoracic Society (ATS) guidelines for normal/mild andmoderate/severe pulmonary function impairment, to deter-mine clinically meaningful pulmonary function status [19].This method of analysis has been previously applied toclassifying pulmonary function in operative AIS patients[7]. These definitions are based on age-, gender-, andheight-matched standards used to generate a percentage ofthe predicted value for each parameter. Pulmonary functionwas considered to be normal when TLC, FVC, and FEV1were greater than 80% of the predicted values. Mildpulmonary impairment was defined as when those param-eters were greater than 65% but 80% or less of the pre-dicted values. Moderate impairment was defined as whenthe parameters were 50% or more but 65% or less of thepredicted values, and severe impairment when they wereless than 50% of the predicted values. An analysis ofvariance was performed to determine the differences inATS guidelines classification by curve magnitude.
Results
The 64 patients included 22 females and 42 males, witha mean age of 16 years (range, 13e25 years). The averageabsolute FVC/%FVC was 4.25/95.8%, average absoluteFEV1/%FEV1 was 3.6/92.5%, and average absolute TLC/%TLC was 5.9/106.2% (Table 1). The mean greatestSagittal Cobb kyphosis angle was 74� (range 49�e102�;49� thoracolumbar kyphosis) (Table 2). The apex ofkyphosis was T10 and cephalad (T) for 57 patients (89%)and caudal to T10/T11 (TL) for 7 patients (11%) (Table 2).
Table 2
Cohort characteristics (overall and by apex group).
N Sagittal T2eT12
All patients 64 68 ��10 �
Apex group
>T10 57 68 ��10 �
<T10/11 7 70 ��10 �
Significance .627
Radiographic variables (T2eT5 kyphosis, T5eT12kyphosis, and greatest sagittal Cobb angle) were alsoanalyzed based on kyphosis apex groups (Tor TL) (Table 2).Subjects with a kyphosis apex T10 and cephalad hada significantly smaller greatest sagittal Cobb angle thanpatients with a kyphosis apex T10e11 and caudad (72� vs.84�; p5 .006). T2eT12 kyphosis and T5eT12 kyphosis didnot differ significantly between the 2 kyphosis apex groups(T vs. TL).
The PFT values were also analyzed based on greatestCobb kyphosis values (Table 1). For %FVC, patients withkyphosis from 81� to 90� and greater than 90� had a signif-icantly lower average percent predicted value than those inthe 71�e80� range: %FVC differed significantly betweenthe 71�e80� group and the 81�e90� group (105% vs. 83%;p 5 .016) and the 71�e80� and greater than 90� groups(105% vs. 73%; p5 .009). Whereas a similar pattern of thisdecrease in average percent predicted existed for FEV1(decline once kyphosis exceeded 80�), this did not reachstatistical significance (p 5 .053). However, the smallnumber of these larger curve groups should be noted. For %TLC, patients with greater than 90� had significantly loweraverage values than those in the 71�e80� range; however,there was a reduced number value for this group (79% vs.115%; p 5 .016). Absolute values of lung volumes and%FEV1 were not affected by the magnitude of kyphosis.
In looking at variables correlated with percent predictedvalues, gender (r 5 .32; p ! .05) and greatest kyphosis(r 5 e.24; p ! .10) showed a weak but significant corre-lation with %FVC (Table 3). Female patients showeda greater average %FVC than male patients (104.6% vs.
Sagittal T5eT12 Greatest sagittal Cobb
63 ��11 � 74 ��11 �
63 ��11 � 72 ��10 �
66 ��7 � 84 ��12 �
.475 .006

Table 3
Correlation magnitude between patient characteristics/radiographic
deformity and pulmonary function testing.
Percent
predicted
for forced
vital
capacity
Percent predicted
for forced
expiratory
volume in 1
second
Percent
predicted
for total lung
capacity
Age �0.07 �0.07 0.05
Gendera 0.32* 0.19 0.07
Apex groupa �0.09 �0.09 �0.09
Sagittal T2eT12 �0.14 �0.05 �0.02
Sagittal T5eT12 �0.06 0.05 �0.03
Greatest sagittal
Cobb
�0.24y �0.12 �0.26
* p ! .05; y p ! .10.a Spearman rho nonparametric correlation was used; all others used
Pearson correlation.
73G. Abbi et al. / Spine Deformity 2 (2014) 70e75
91.5%; p 5 .01). No variable was significantly correlatedwith %FEV1.
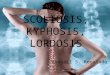
When percent predicted values were broken down into theATS guidelines for impairment, the percentage of patientswith moderate to severe impairment (4%) was lowest in the71�e80� range and increased with increasing ranges ofkyphosis magnitude: 81�e90� (11%) and greater than 90�
(50%; FEV1 and FVC were not available for 1 patient in thegreater than 90� group). There were no statistically significantdifferences between the numbers of patients in each ATSclassification group based on curve magnitude; however,therewere a small number of patients in the groupswith largercurve sizes (Fig. 1).
Fig. 1. American Thoracic Society classification guidelines based on kyphosis
patients in the American Thoracic Society classification groups when the cohort
more pulmonary function test results that were less than 65% of the predicted v
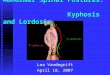
Examples of 2 patients included in this study, 1 witha curve size at the mean and 1 with an increased curve size,are shown in Figure 2, along with their respective preop-erative pulmonary function data.
Discussion
Numerous studies exist on SK, but more information isrequired [1-5,13,15,16,20-22]. Some researchers suggestedthat the progressive condition could eventually lead tocardiopulmonary failure [5], although the study by Murrayet al. [13] is the only one to the authors’ knowledge thataddressed pulmonary function for this entity. Following thenatural history of 67 patients with SK over an average of 32years, they found normal to above-normal averages forpulmonary function in kyphosis less than 100�. Impairedlung function in those with kyphosis greater than 100� wasobserved. Similarly, the current authors found no correla-tion with apex of the kyphosis or other radiographicparameters to impaired pulmonary function until a kyphosismagnitude of 90� was reached. At this critical angle, morethan 50% of patients had clinically decreased PFTs or lessthan 80% of predicted values. The case examples inFigure 2 illustrate the effect of increased curve magnitudeon PFTs, and show a patient with a 102� curve whosepulmonary function was much more impaired than that inthe patient with a significantly smaller curve magnitude.Although PFTs are not performed at all institutions for SKpatients, these data suggest that patients with more severekyphotic curves should be monitored for pulmonary func-tion preoperatively, and perhaps after surgery.
magnitude. No significant differences were found between the number of
was divided into curve magnitude categories. Moderate to severe 5 1 or
alue.

Fig. 2. Case examples of radiographic and pulmonary function for operative Scheuermann kyphosis (SK). Two case examples of operative SK patients with
accompanying forced vital capacity (FVC), forced expiratory volume in 1 second (FEV1), and total lung capacity (TLC) data. One patient has a curve magni-
tude at the smaller end of the cohort’s range; the other patient has the largest curve magnitude in the cohort. Increase curve magnitude can be seen here
affecting pulmonary function values in a negative manner.
74 G. Abbi et al. / Spine Deformity 2 (2014) 70e75
Many researchers consider pulmonary function testing tobe a routine or important aspect of preoperative evaluation inthe surgical treatment of patients with AIS [17,18]. Thecurrent authors know from a previous retrospective study onAIS in 631 patients recommended for surgery that preoper-ative pulmonary function is affected by large thoracic curvesgreater than 70�, as well as increased number of vertebraeinvolved, thoracic hypokyphosis, and coronal imbalance [7].Clinically significant pulmonary decline was also found inuntreated AIS patients with thoracic curve magnitudebeyond 100� [6]. Multiple studies have evaluated thesepatients postoperatively, as well [8-12]. Overall, chest walldisruption as a result of a thoracoplasty procedure or openanterior release and fusion has the largest effects on post-operative pulmonary function [10,11,13]. Posterior-onlyfusion may result in significant improvement in PFTs at 2years postoperatively [10,12]. In the current prospectivestudy of operative SK, the authors continue to follow thepatient population postoperatively to determine the impact ofsurgery on pulmonary function.
The variability of measuring pulmonary functionaccurately is known and is a limitation of this studybecause of the likely variability among 10 hospital insti-tutions, even though similar spirometers were used andguidelines for their use were provided [7,23,24]. In addi-tion, there are concerns regarding the use of data based onheight to predict values for pulmonary function witha condition such as Scheuermann disease, which affectsthe height of the test subject [23]. This may lead to anunderestimation of the effect of the curvature on PFTs.Arm span measurements have been used as a surrogate
for height in other studies [25]. Unmeasured confoun-ding factors also may affect pulmonary function values,including preexisting comorbidities such as asthma,smoking, and diminished activity levels of SK patientscompared with the normal population [24].
This study was also limited by the small number ofpatients with larger curves (greater than 90�). This caveatrequires that results be considered preliminary evaluationsof PFTs in this segment of the population, and thereforea greater number of patients with large curve magnitudesare necessary for analysis to definitively determine the roleof PFTs in the range of this population. The current studyindicated that pulmonary function declines steadily inpatients with curves over 80� from both the comparison ofmean PFT values and the comparison of patients based ondisease severity using the ATS guidelines. Despite the smallnumber of patients in these groups, 2 sets of analysis dis-played the same trends, which provides more support tothese findings. Few studies have evaluated operativeScheuermann disease patients with larger curves, and nonehave evaluated PFTs in this population; therefore the dataare valuable in filling this void in the literature.
Overall, the data confirm the hypothesis that more severekyphosis magnitude negatively affects the pulmonary func-tion of patients with operative SK. Specifically, a significantnumber of patients with kyphotic curves greater than 80� inmagnitude had signs of mild pulmonary impairment, whichbecame more significant for kyphosis greater than 90�. Otherradiographic criteria were not significant, including thelocation of the apex of the kyphosis. Further evaluation ofthese patients to observe the impact of surgery on pulmonary

75G. Abbi et al. / Spine Deformity 2 (2014) 70e75
function is planned. Pulmonary function tests should bemeasured in select patients (those with severe curves witha magnitude of kyphosis greater than 90�) because this mayaffect a patient’s postoperative course.
References
[1] Scheuermann H. Kyphosis dorsalis juvenilis. Ugeskr kaeger 1920;82:
385e93.
[2] Bradford DS. Juvenile kyphosis. Clin Orthop 1977;128:45e55.
[3] Bradford DS. Vertebral osteochondrosis (Scheuermann’s kyphosis).
Clin Orthop 1981;158:83e90.[4] Lowe TG. Current concepts review: Scheuermann disease. J Bone
Joint Surg Am 1990;72:940e5.
[5] Bradford DS, Ahmed KB, Moe JH, et al. The surgical management of
patients with Scheuermann’s disease: a review of twenty-four cases
managed by combined anterior and posterior spine fusion. J Bone
Joint Surg Am 1980;62:705e12.
[6] Weinstein SL, Zavala DC, Ponseti IV. Idiopathic scoliosis: long-term
follow-up and prognosis in untreated patients. J Bone Joint Surg Am
1981;63:702e12.
[7] Newton PO, Faro FD, Gollogly S, et al. Results of preoperative
pulmonary function testing of adolescents with idiopathic scoliosis.
J Bone Joint Surg Am 2005;87:1937e46.
[8] Lenke LG, Newton PO, Marks MC, et al. Prospective pulmonary
function comparison of open versus endoscopic anterior fusion
combined with posterior fusion in adolescent idiopathic scoliosis.
Spine (Phila Pa 1976) 2004;29:2055e60.
[9] Newton PO, Perry A, Bastrom TP, et al. Predictors of change in post-
operative pulmonary function in adolescent idiopathic scoliosis.
Spine (Phila Pa 1976) 2007;32:1875e82.
[10] Vedantam R, Lenke LG, Bridwell KH, et al. A prospective evaluation
of pulmonary function in patients with adolescent idiopathic scoliosis
relative to the surgical approach used for spinal arthrodesis. Spine
(Phila Pa 1976) 2000;25:82e90.
[11] Verma K, Lonner BS, Kean KA, et al. Maximal pulmonary recovery
after spinal fusion for adolescent idiopathic scoliosis. Spine (Phila Pa
1976) 2011;36:1086e95.
[12] Gitelman Y, Lenke LG, Bridwell KH, et al. Pulmonary function in
adolescent idiopathic scoliosis relative to the surgical procedure.
Spine (Phila Pa 1976) 2011;36:1665e72.[13] Murray PM, Weinstein SL, Spratt KF. The natural history and long-
term follow-up of Scheuermann kyphosis. J Bone Joint Surg Am
1993;75:236e48.
[14] Weng TR, Levison H. Standards of pulmonary function in children.
Am Rev Respir Dis 1969;99:879e94.
[15] Soo CL, Noble PC, Esses SI. Scheuermann kyphosis: long-term
follow up. Spine (Phila Pa 1976) 2002;2:149e56.
[16] Ristolainen L, Kettunen JA, Heliovaara M, et al. Untreated Scheuer-
mann’s disease: a 37- year follow-up study. Eur Spine J 2012;21:
819e24.
[17] Bowen RM. Respiratory management in scoliosis. In: Lonstein JE,
Winter RB, Bradford DS, Ogilvie JW, editors. Moe’s textbook of
scoliosis and other deformities. 3rd ed. Philadelphia: WB Saunders
Co; 1995. p. 572e81.
[18] Lonstein J. Scoliosis. In: Morrissy RT, Weinstein SL, editors. Scoli-
osis in Lovell and Winter’s pediatric orthopaedics. vol. 2. 1996. p.
925e87.
[19] Murray J, Nadel J, editors. Textbook of respiratory medicine. 3rd ed.
Philadelphia: Saunders; 2000.
[20] Lonner BS, Newton P, Betz R, et al. Operative management of
Scheuermann’s kyphosis in 78 patients. Spine (Phila Pa 1976)
2007;32:2644e52.
[21] Coe JD, Smith JS, Berven S, et al. Complications of spinal fusion
for Scheuermann’s kyphosis. Spine (Phila Pa 1976) 2010;35:
99e103.
[22] Tsirikos AI, Jain AK. Scheuermann’s kyphosis: current controversies.
J Bone Joint Surg Br 2011;93:857e64.
[23] Baur X, Degens P, Heitmann R, et al. Lung function testing: the
dilemma of predicted values in relation to the individual variability.
Respiration 1996;63:123e30.
[24] Hruby J, Butler J. Variability of routine pulmonary function tests.
Thorax 1975;30:548e53.
[25] Reeves SL, Varakamin C, Henry CJ. The relationship between arm-
span measurement and height with special reference to gender and
ethnicity. Eur J Clin Nutr 1996;50:398e400.