Embed Size (px)
Citation preview

REVIEW
Premalignant conditions of gastric cancerKentaro Sugano
Department of Medicine, Division of Gastroenterology, Jichi Medical University, Tochigi, Japan
Key words
CDX1, CDX2, gastric cancer, Helicobacterpylori, intestinal metaplasia, premalignantcondition of the stomach.
Accepted for publication 21 March 2013.
Correspondence
Professor Kentaro Sugano, 3311-1 Yakushiji,Shimotsuke, Tochigi 329-0498, Japan.Email: [email protected]
AbstractPremalignant lesions of gastric cancer encompass a variety of conditions such as chronicgastritis, intestinal metaplasia and dysplasia, in which elevated risk of developing gastriccancer have been documented. Among them, intestinal metaplasia is frequently encoun-tered in our daily endoscopic examination, yet its clinical significance is often underesti-mated despite of a number of reports demonstrating genetic and epigenetic alterations inthe intestinal metaplastic mucosa. In this review, I will describe the molecular mechanismsof phenotypic changes from gastric mucosa to intestinal metaplasia based on our analysisof mouse model of intestinal metaplasia generated by ectopic expression of CDX2 inconjunction with the studies with human intestinal metaplasia.
IntroductionPremalignant condition of gastric cancer (GC) is an umbrella termfor high-risk states developing gastric cancer such as atrophiccorpus gastritis and intestinal metaplasia (IM). IM is not consid-ered to be a neoplastic lesion, but there is ample evidence thatintestinal metaplasia harbors a number of genetic and epigeneticchanges leading to gastric cancer.1 Moreover, most of the studiesdemonstrate that eradication therapy is generally ineffective inreversing the condition.2 Therefore, IM may be considered to be apre-neoplastic lesion that has crossed “a point of no-return.” In thisreview, I will focus on the molecular mechanisms that lead to theformation of IM; in particular, a critical role of caudal-relatedhomeobox transcriptional factor, CDX2, will be discussed basedon our experimental data obtained with transgenic CDX2 mice,a mouse model of IM.3
In the stomach with IM, hypochlorhydric gastric milieu allowsovergrowth of non-Helicobacter bacteria which is responsible forhigh nitrite contents. Our recent study indicates that oral micro-bacteria colonized in the hypochlorhydric stomach may be respon-sible for production of nitrosamines from nitrites.
I also discuss about diagnosis and management of premalignantconditions including “dysplastic lesion” for which there is aconsiderable disagreement between the West and Japan.
Molecular mechanisms leading to theintestinal metaplasiaIn a so-called Correa’s cascade, chronic gastric inflammation pre-disposes atrophic gastritis and IM. Now it is established that themost important cause of chronic gastritis is Helicobacter pylori(H. pylori) infection. However, the precise molecular mechanismsleading to IM had been unknown. To elucidate the mechanisms,we focused our research on the homeobox transcriptional factors,CDX1 and CDX2, which were reported to be critical in conferring
intestinal phenotype4 (Fig. 1). In humans, two homologous CDX1and CDX2 are known, and CDX1 had been reported to be ectopi-cally expressed in the Barrett’s esophagus and IM,5 but the role ofCDX2 was not known. Thus, we examined the temporal and topo-logical expression pattern of both CDX1 and CDX2 in patientswith chronic gastritis in conjunction of intestinal marker geneexpressions and found that the expression of CDX2, but notCDX1, occurred early in the mucosa without intestinal geneexpression. CDX1 expression was observed later in the mucosaexpressing intestinal marker genes.6 Therefore, we suspect thatectopic expression of CDX2 in the inflammatory gastric mucosamight trigger the molecular events leading to IM. To support thishypothesis, we generated CDX2-transgenic mice by expressing atransgene construct containing H+,K+-ATPase promoter attachedto CDX2 gene to guide its expression in the parietal cells.3
About one month after birth, foci of intestinal metaplastic glandsemerged in the corpus mucosa which spread to the entire corpusmucosa by 6 months after birth. In another mice model of IM usingFoxa3 promoter construct,7 however, the IM observed was limitedin the antrum and dissimilar to the human IM in terms of structuralorganization and was not extensive as shown in a patchy absorptivecells, indicating the importance of the selected promoter that couldinfluence the ectopic expression of CDX2 in a particular cell type.A detailed analysis of the sequence of molecular signature expres-sions in our CDX2-transgenic mice verified that CDX2 expressionemerged before apparent expression of intestinal marker genesthat shape intestinal phenotype, whereas CDX1 expression wasobserved concurrently with intestinal gene expressions.8 In thismouse model of IM, pseudopyloric metaplasia (spasmolyticpolypeptide-expressing metaplasia: SPEM) remained in thebottom of the metaplastic glands, indicating a hybrid nature of thegland architecture. Although CDX1-transgenic mice also showedIM, but the IM were not widespread and no cancerous lesions wereobserved.9 Therefore, CDX2 seemed to be more important ininducing IM. Indeed, CDX2 can activate endogenous CDX1 gene
doi:10.1111/jgh.12209
bs_bs_banner
906 Journal of Gastroenterology and Hepatology 28 (2013) 906–911
© 2013 Journal of Gastroenterology and Hepatology Foundation and Wiley Publishing Asia Pty Ltd

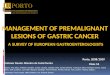
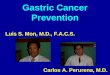
expression.10 Importantly, cancerous lesions developed in the IMin almost all the mice when kept for 2 years (Fig. 2). This processwas shortened when CDX2-transgenic mice were crossed withp53 deficient mice or APC (adenomatous polyposis coli) mutantMin mice.11 These experimental data indicate that IM may be adirect precursor of gastric cancer, but there are controversies thatthe majority of intestinal type of human gastric cancers developsfrom so-called gastric-intestinal mixed glands.12 However, thegastric-intestinal mixed glands have principally been defined bymucin histochemistry. As described above, CDX2 gene expressionoccurs before such phenotypic changes (including mucin expres-sion),6,8 and therefore CDX2 was also expressed in the so-calledgastric-intestinal mixed glands.9 Conversely, SOX2 [(Sex deter-mining region Y)-related high-mobility-group (HMG) box tran-scription factor 2 more simply known as SRY/HMG box 2transcriptional factor] gene expression whose expression is limitedin the normal stomach was simultaneously observed not only inour mice model,13 but also in human IM (Fig. 3). Thus, apparentintestinal glands showed mixed expression in terms of transcrip-tional factors SOX2 and CDX2 whose expressions in the normalcondition are limited to the stomach and intestine, respectively. Asproposed by McDonald and colleagues, multiple stem cells mayexist in a single gastric unit, and it may take a long time to have anentire gastric unit replaced by progenies from a single stem cell.14
Therefore, classification of gastric-intestinal mixed gland andintestinal gland based on expression of gastric mucins (MAC5Ac,MAC6) and intestinal mucin (MAC2), respectively seems to betoo simplistic. It would be more reasonable to assume that IM is ahybrid state where multiple progenitors are changing their cellfates in a differential manner. In support of this hypothesis,microRNA (miRNA) expression profile of the IM in the CDX2-transgenic mice was more closely related to the original gastricmucosa than intestinal mucosa (unpublished observation). Thus,IM may be better defined that it is not a true trans-differentiationbut a “disguised state” of gastric cells, as miRNA expressionprofile can be more informative in elucidating the developmentallineage.15
Figure 1 Caudal-related homeobox trans-criptional factor (CDX2) regulates multipleintestinal gene expressions. A number ofgene signatures for differentiated entero-cytes, including enteroendocrine cells, gobletcells, and absorptive cells are regulated byCDX2.
(a)
(b)
Figure 2 Gastric cancer developed in CDX2-transgenic mice. (a) In thestomach of CDX2-transgenic mice at 100 weeks after birth, differenti-ated type of gastric cancers developed.11 No tumors were seen in thecontrol mice at the same age. (b) Histological examination showed thetumor penetrated muscularis propria.
K Sugano Gastric precancerous conditions
907Journal of Gastroenterology and Hepatology 28 (2013) 906–911
© 2013 Journal of Gastroenterology and Hepatology Foundation and Wiley Publishing Asia Pty Ltd

Genetic and epigenetic changes in theIM and dysplasiaIt has been well-documented that considerable genetic and epige-netic changes occurred in IM including p53 mutations, methyla-tions of Runx3, CDH, and p16 that have been documented asimportant genetic/epigenetic alterations in gastric cancers.1,16
Among these changes, methylation of Runx3 seems important ininducing IM, because deficiency of Runx3 function was shown toinduce CDX2 expression.17 We have confirmed that micro-dissected human IM tissue contained a number of mutations in p53genes (Table 1). Additional genetic/epigenetic changes in the IMwould lead to neoplastic, dysplastic lesions as demonstrated by anelegant study by McDonald and colleagues, who showed thatdysplastic lesions contained the same genetic alterations with thesurrounding IM.18 Further genetic alterations occurring in the dys-plastic lesions give rise to cancerous foci within dysplastic area,so-called “cancer in adenoma” (Fig. 4a,b). As was shown in ourmice model, these human studies would support that at least insome cases, IM is directly connected to adenoma-carcinomasequence.
Hypochlorhydria and bacterialovergrowthHow can we explain the mechanisms of these genetic and epige-netic changes seen in IM or dysplasia? Some of the epigeneticchanges have been reported in chronic gastritis, and could bereversed by eradication. However, H. pylori may play only alimited role in the neoplastic progression from IM as it cannotcolonize in IM. In support of the role of other factors in thisprocess, continuous occurrence of gastric cancer long after suc-cessful eradication of H. pylori has been reported.19,20 What wouldbe the feasible mechanisms and factors to explain this process?We propose that bacterial overgrowth and resultant increased
Figure 3 Co-expression of SOX2 and CDX2 in the human intestinalmetaplasia. In human intestinal metaplasia, both SOX2 and CDX2 wereco-localized in the nuclei of the metaplastic glands. Antibodies used forSOX2 and CDX2 were obtained from Sigma and Biogenex, respectively.Second antibodies used for immunofluorescence were Alexa labeledantirabbit IgG from (Invitrogen) for SOX2 and Cy3-labeled antimouse IgG(immunoglobulin G) (Jackson) for CDX2, respectively.
(a)
(b)
Figure 4 Cancer in adenoma. (a) Cancer foci showing conspicuouscellular atypism and tissue disorganization compared with the surround-ing adenoma. Arrows show the site of submucosal invasion in thecancerous foci. (b) P53 positive cells were confined to a cancerouspart in the cancer in adenoma tissue. Left: HE staining, Right: P53immunostaining.
Table 1 P53 gene mutations in human IM. Human intestinal metaplastic glands were microdissected, and p53 mutations were analyzed with thehuman p53 Genechip (Affymetrix) that enables screen for mutations of coding region from exon 2 to 11 including introns of human p53 gene
Patient Age Sex Site of mutations Type of mutations Amino acid changes
1 54 M Exon 5 cgc →cac R→H2 48 M Intron 10 g→a —3 65 M — — —4 77 M — — —5 69 M Intron3, Exon 5 gtc→ggc V→G6 48 M Intron 10 g→a —7 68 M Exon 6 g→- V→Stop8 58 M Exon3, Intron 5,
Exon 6gtt→ttt, a→g, cga→ccagag→ggg, ccg→cgggag→cag
V→F, R→P,E→G, P→R,E→Q
9 69 F Exon 8 ggg→cag G→R10 49 F Exon 3, Intron 3 ctt→ttt, aaa→ccc,
ctg→cag, g→t, t→cL→F, N→P,L→Q
Gastric precancerous conditions K Sugano
908 Journal of Gastroenterology and Hepatology 28 (2013) 906–911
© 2013 Journal of Gastroenterology and Hepatology Foundation and Wiley Publishing Asia Pty Ltd

nitrosamine production in the stomach which was once the leadingtheory for gastric carcinogenesis should be reevaluated to explainthis process. In hypochlorhydric or achlorhydric stomach, abun-dant growth of bacteria, mainly from oral source, can be seen(Fig. 5). Since gastric juice is not acidic with low level of ascorbicacid in the stomach harboring the IM, nitrites from saliva can stayin the gastric juice and are converted to carcinogenic nitrosamines.It is also plausible that in other area of the stomach, H. pylori andother microbacteria may coexist, since IM distribution in thestomach is sporadic. Such coexistence of multiple organisms maybe more dangerous by aggravating the inflammation and atrophy.21
Moreover, other bacterial species can still reside in the atrophicstomach with low acid secretory state and exert harmful effects byproducing potentially chemical carcinogenic substance even aftereradication therapy. Thus, roles of other virulent bacterial speciesshould be further explored to explain the reasons why moreadvanced stages of atrophy have a higher risk for gastric cancerand to solve the so-called Asian or African enigma.
Diagnosis and management ofprecancerous conditionsValid diagnosis of IM can only be done by histological examina-tion of biopsied mucosa. Indeed, poor agreement between endo-scopic diagnosis and that of histology was documented. In aJapanese pilot study, endoscopic diagnosis of IM had a high speci-ficity (99%) but the sensitivity was surprisingly poor; only 12% ofhistologically confirmed IM was diagnosed by endoscopy.22
However, modern endoscopic imaging modalities, such as narrowband imaging (NBI), flexible intelligent color enhancement(FICE), and blue-laser imaging (BLI), can facilitate identificationof IM and dysplastic or cancerous lesions23–25 (Fig. 6a,b). Once IMis identified during endoscopic examinations, high levels of vigi-lance should be exerted to search for dysplastic or cancerouslesions, because patients with IM have a higher risk of harboringsuch neoplastic lesions (Fig. 6b). Also important is to eradicateH. pylori if positive. Eradication has dual benefits: reduction ofinflammation by H. pylori, a major culprit of inflammation andrestoration of acid secretion which can reduce bacterial over-growth in the majority of patients.26 Whether eradication ofH. pylori can revert IM is controversial. Most of the studies,however, could not demonstrate significant improvement of IM,2
which may be explained by the auto-regulatory mechanism ofCDX2.27 Thus, in the majority of cases, it is most likely that IMwith genetic derangements remains after eradication therapy. Asmentioned before, continuous development of gastric cancer longafter successful eradication therapy also support that patients withatrophy and/or IM are recommended to receive follow-up endo-scopic examinations.
If dysplastic lesions are detected during endoscopy, endoscopicmucosal resection should be considered if feasible. Even in Japan,where pathologists are well-experienced in the diagnosis of GC,biopsy-based diagnosis has to be corrected after entire lesionsbeing checked (Table 2). This is not because some of the lesionssatisfy the “invasion criteria,” but because distinct cellular and/orstructural disorganization or identification of cancerous foci inadenomas (cancer in adenoma, Fig. 4a,b) can only become evidentafter examination of whole resected materials.
Since in many Western countries, “invasive criterion” is neces-sary for the diagnosis of cancer; diagnosis based on biopsy alonetend to be insufficient, because it would be difficult to take biopsymaterials targeted to a locally invaded area even with modernimaging modalities as the invasive front resides in the submucosa
Figure 5 Bacterial overgrowth in the H. pylori infected stomach. Ingastric juice obtained from patients with atrophic gastritis, abundantgrowth of non-H. pylori species was observed both in aerobic (left) andanaerobic (right) conditions.
(a)
(b)
Figure 6 Endoscopic diagnosis of intestinal metaplasia. (a) Comparedwith conventional white light image (left), use of flexible-intelligentcolor enhancement (FICE) image facilitates detection of intestinalmetaplasia due to enhanced gain in color contrast (right, arrowheads).(b) Blue laser imaging (BLI) mode can facilitate diagnosis of intestinalmetaplasia and is useful in identifying the dysplastic area within theintestinal metaplasia. Left: Conventional white light image showingwhitish slightly elevated mucosa. The BLI image of the rectangulararea marked in the left photo was shown in the right. Intestinal meta-plasia appeared greenish due to so-called “light-blue crest sign.”23 Indysplastic mucosa, such coloration was lost, and it becomes easier tobe noted (right).
K Sugano Gastric precancerous conditions
909Journal of Gastroenterology and Hepatology 28 (2013) 906–911
© 2013 Journal of Gastroenterology and Hepatology Foundation and Wiley Publishing Asia Pty Ltd

(Fig. 4a,b). Furthermore, follow-up studies on gastric dysplasiaoutcome revealed a high rate of progression to advanced cancersin a short period of time quite similar to the natural course ofearly gastric cancer in Japan,28,29 urging therapeutic interventionfor patients with high-grade dysplasia diagnosed by Westernpathologists.
For this reason, it should be recommended to perform endo-scopic resection for high-grade dysplasia (early mucosal gastriccancer according to the Japanese criteria). To reconcile these dis-crepant diagnostic criteria between Japan and the West, the term“noninvasive high-grade neoplasia” was adopted in the Viennaclassification. Unfortunately, however, this term has not beenwidely used in either side. Moreover, the term, “intraepithelialneoplasia” was introduced in the recent World Health Organizationclassification. In the future, we definitely need a global consensushow to deal with such “neoplastic” lesions, for which recenttechnological advancement would be instrumental in promotingmutual understanding.
AcknowledgmentThis review article is the results of intensive clinical and researchefforts of colleagues in Jichi Medical University. Special thanksto Dr Hiroyuki Mutoh who contributed to the molecular mecha-nisms of IM and to Dr Kiichi Satoh for the histological analysis.I also thank Dr Yoshikazu Hayashi in our department and DrShunji Hayashi in the department of microbiology, Jichi MedicalUniversity who contributed to gastric microbiology. Endoscopicimages were kindly provided by Dr Hiroyuki Osawa in ourdepartment.
References1 Busuttil RA, Boussioutas A. Intestinal metaplasia: a premalignant
lesion involved in gastric carcinogenesis. J. Gastroenterol. Hepatol.2009; 24: 193–201.
2 Malfertheiner P, Megraud F, O’Morain CA et al.; The EuropeanHeicobacter Study Group. Management of Helicobacter pyloriinfection-the Maastricht IV/Florence Consensus Report. Gut 2012;61: 646–64.
3 Mutoh H, Hakamata Y, Sato K et al. Conversion of gastric mucosato intestinal metaplasia in Cdx2-expressing transgenic mice.Biochem. Biophys. Res. Commun. 2002; 294: 470–9.
4 Suh E, Chen I, Taylor J, Traber PG. A homeobox protein related tocaudal regulates intestine-specific gene transcription. Mol. Cell. Biol.1994; 14: 7340–51.
5 Silberg DG, Furth EE, Taylor JK, Schuck T, Chiou T, Traber PG.CDX1 protein expression in normal, metaplastic and neoplastichuman alimentary tract epithelium. Gastroenterology 1997; 113:478–86.
6 Eda A, Osawa H, Yanaka I et al. Expression of homeobox geneCDX2 precedes that of CDX1 during progression of intestinalmetaplasia. J. Gastroenterol. 2002; 37: 94–100.
7 Silberg DG, Sullivan J, Kang E et al. Cdx2 ectopic expressioninduces gastric intestinal metaplasia in transgenic mice.Gastroenterology 2012; 122: 689–96.
8 Sakamoto H, Mutoh H, Hayakawa H, Sashikawa M, Sugano K.Cell lineage dynamics in the process leading to intestinal metaplasia.J. Gastroenterol. 2011; 46: 620–8.
9 Mutoh H, Sakurai S, Satoh K et al. Cdx1 induced intestinalmetaplasia in the transgenic mouse stomach: comparative study withCdx2 transgenic mice. Gut 2004; 53: 1416–23.
10 Mutoh H, Hayakawa H, Sakamoto H, Sashikawa M, Sugano K.Transgenic Cdx2 induces endogenous Cdx1 in intestinal metaplasiaof Cdx2-transgenic mouse stomach. FEBS J. 2009; 276: 5821–31.
11 Mutoh H, Sakurai S, Satoh K et al. Development of gastriccarcinoma from intestinal metaplasia in Cdx2-transgenic mice.Cancer Res. 2004; 64: 7740–7.
12 Tsukamoto T, Mizoshita T, Tatematsu M. Gastric-and-intestinalmixed-type intestinal metaplasia: aberrant expression of transcriptionfactors and stem cell intestinalization. Gastric Cancer 2006; 9:156–66.
13 Mutoh H, Sashikawa M, Sugano K. Sox2 expression is maintainedwhile gastric phenotype is completely lost in Cdx2-induced intestinalmetaplasitic mucosa. Differentiation 2011; 81: 92–8.
14 McDonald SAC, Greaves LC, Gutierrez-Gonzalez L et al.Mechanisms of field cancerization in the huma; n stomach: theexpansion and spread of mutated gastric stem cells. Gastroenterology2008; 134: 500–10.
15 Lu J, Getz G, Miska EA et al. MicroRNA expression profilesclassify human cancers. Nature 2005; 435: 834–8.
16 Kang GH, Shim YH, Jung HY, Kim WH, Ro JY, Rhyu MG. CpGisland methylation in premalignant stages of gastric carcinoma.Cancer Res. 2001; 61: 2847–51.
17 Ito K, Chuang LS, Ito T et al. Loss of Runx3 is a key event ininducing precancerous state of the stomach. Gastroenterology 2011;140: 1536–46.
18 Guthirrez-Gonzalez L, Graham TA, Rodriguez-Justo M et al. Theclonal origins of dysplasia from intestinal metaplasia in the humanstomach. Gastroenterology 2011; 140: 1251–60.
19 Kamada T, Hata J, Sugiu K et al. Clinical features of gastric cancerdiscovered after successful eradication of Helicobacter pylori: resultsfrom a 9-year prospective follow-up study in Japan. Aliment.Pharmacol. Ther. 2005; 21: 1121–6.
20 Take S, Mizuno M, Ishiki K et al. The long-term risk of gastriccancer after the successful eradication of Helicobacter pylori.J. Gastroenterol. 2011; 46: 318–24.
21 Sanduleanu S, Jonkers D, De Bruine A, Hameeteman W,Stockbrugger RW. Double gastric infection with Helicobacter pyloriand non-Helicobacter pylori bacteria during acid-suppressivetherapy: increase of pro-inflammatory cytokines and development ofatrophic gastritis. Aliment. Pharmacol. Ther. 2001; 15: 1163–75.
22 Kaminishi M, Yamaguchi H, Nomura S et al. Endoscopicclassification of chronic gastritis based on a pilot study by
Table 2 Pathological diagnosis on biopsy samples and on endoscopi-cally resected tissues Jichi Medical University (2001–2004). About 20%of biopsy diagnose of adenoma were changed to adenocarcinomasbased on the entire tissue examinations obtained by endoscopicresections (ER). Conversely, about 6% of biopsy diagnose of well-differentiated adenocarcinomas were down-graded to adenomas afterexamination of endoscopically resected specimens.
Finaldiagnosisafter ER
Biopsy-baseddiagnosis
Adenoma Adenocarcinoma(tub1)
Adenocarcinoma(tub2)
Adenoma 59 14 1Adenocarcinoma
(tub1)9 102 11
Adenocarcinoma(tub2)
0 5 14
Gastric precancerous conditions K Sugano
910 Journal of Gastroenterology and Hepatology 28 (2013) 906–911
© 2013 Journal of Gastroenterology and Hepatology Foundation and Wiley Publishing Asia Pty Ltd

the research society for gastritis. Dig. Endosc. 2002; 14:138–51.
23 Uedo N, Ishihara R, Iishi H et al. A new method of diagnosinggastric intestinal metaplasia: narrow-band imaging with magnifyingendoscopy. Endoscopy 2006; 38: 819–24.
24 Osawa H, Yamamoto H, Miura Y et al. Diagnosis of extent of earlygastric cancer using flexible spectral imaging color enhancement.World J. Gastrointest. Endosc. 2012; 4: 356–61.
25 Osawa H, Miura Y, Ino Y, Satoh K, Yamamoto H, Sugano K. Bluelaser imaging as a new endoscopic system can produce an excellentimage of detailed microsctructure and microvasculare in superficialgastroduodenal neoplasm. Gut 2012; 61 (Suppl. 3): A240. (abstract).
26 Osawa H, Kita H, Ohnishi H et al. Helicobacter pylori eradicationinduces marked increase in H+/K+-adenosine triphosphataseexpression without altering parietal cell number in human gastricmucosa. Gut 2006; 55: 152–7.
27 Barros R, da Costa LT, Pinto-de-Sousa J et al. CDX2 autoregulationin human intestinal metaplasia of the stomach: impact on thestability of the phenotype. Gut 2011; 60: 290–8.
28 Rugge M, Cassaro M, Di Mario F et al. Interdisciplinary group ongastric epithelial dysplasia. Gut 2003; 52: 1111–16.
29 Tsukuma H, Oshima A, Narahara H, Morii T. Natural history ofearly gastric cancer: a non-concurrent, long-term, follow-up study.Gut 2000; 47: 618–23.
K Sugano Gastric precancerous conditions
911Journal of Gastroenterology and Hepatology 28 (2013) 906–911
© 2013 Journal of Gastroenterology and Hepatology Foundation and Wiley Publishing Asia Pty Ltd























![[Ghiduri][Cancer]Gastric Cancer](https://img.pdfslide.us/doc/110x75/55cf9399550346f57b9de771/ghiduricancergastric-cancer.jpg)
