Embed Size (px)
Citation preview
Neo-adjuvant Therapies for Gastric Cancer: An Alternative Approach to an Old Problem
Eduardo A. Guzman MD

Introduction
• Gastric cancer is the second leading cause of cancer death
worldwide
• US
– 22,280 new case
– 11,430 deaths
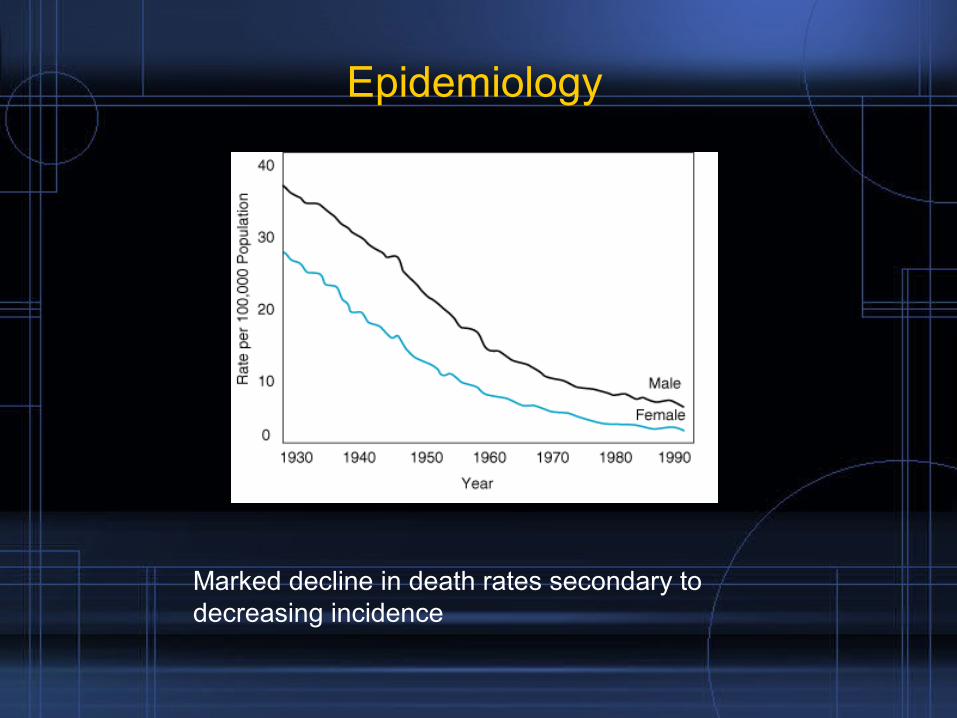
Epidemiology
Marked decline in death rates secondary to decreasing incidence
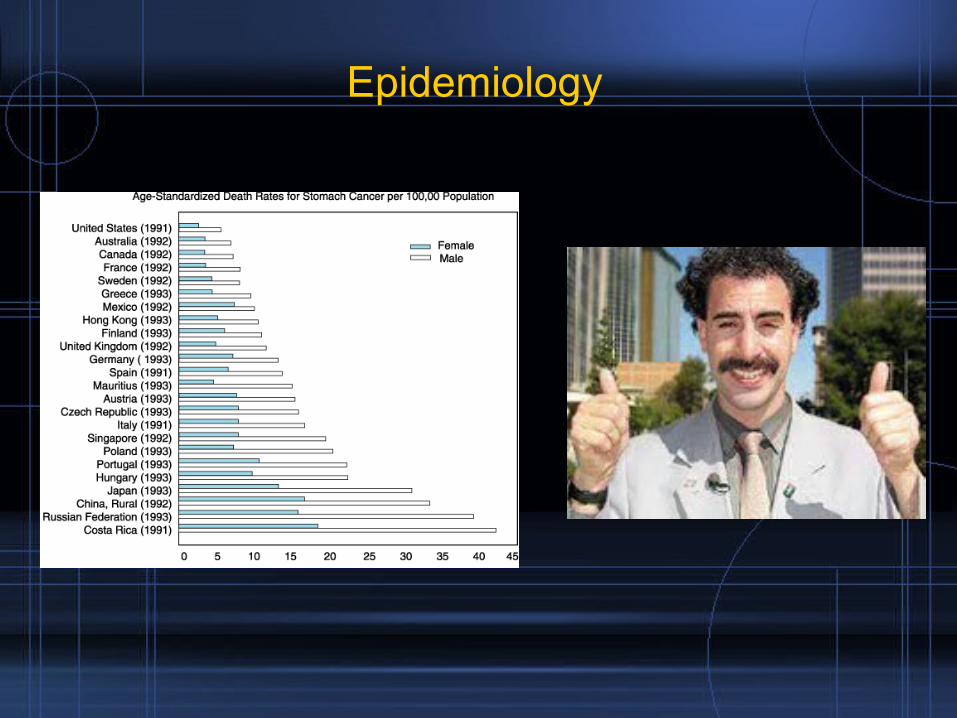
Epidemiology
Etiology
• Low fruits and vegetables
• High salts and nitrates
• Salted fish
• Smoked meats
• H pylori
• Hypochlorhydria
• Polyps
• Genetics (p 53 mutations, microastellite instability gene MSI., e-cadherin gene)
• Previous radiation
• Post gastrectomy
• Pernicious anemia
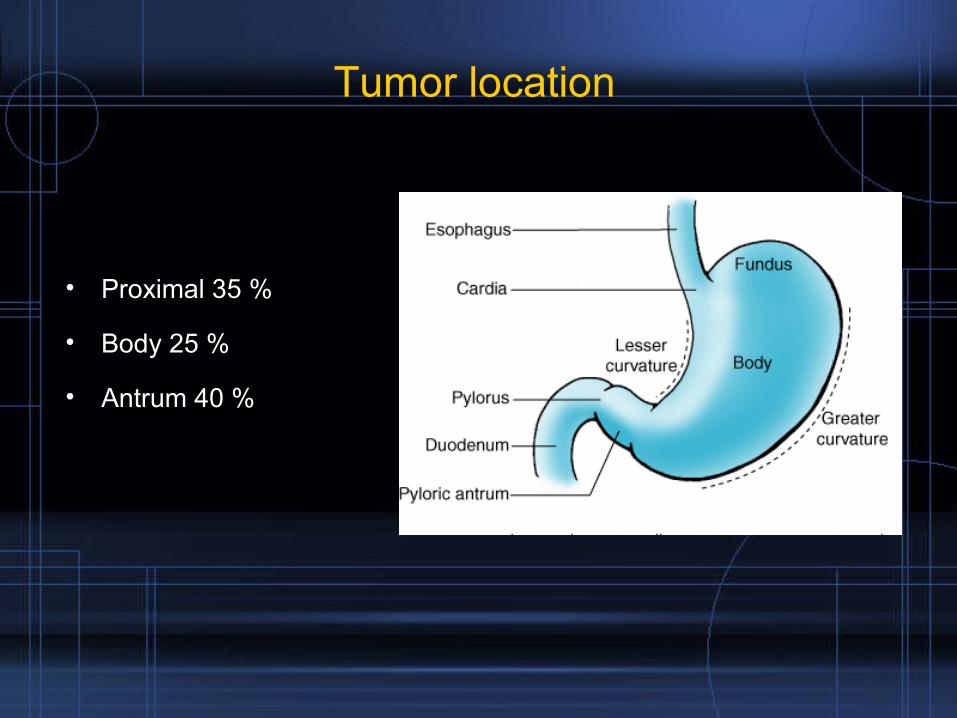
Tumor location
• Proximal 35 %
• Body 25 %
• Antrum 40 %
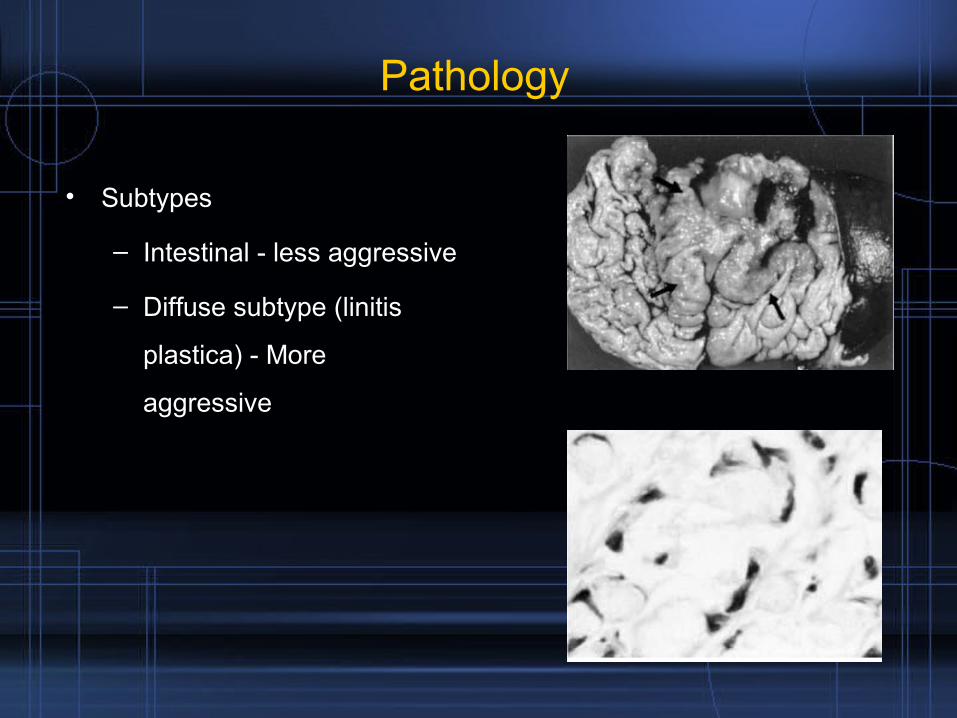
Pathology
• Subtypes
– Intestinal - less aggressive
– Diffuse subtype (linitis
plastica) - More
aggressive
Lexicon
• Krukenberg tumor – Ovarian metastasis
• Sister Mary Joseph node – Periumbilical node
• Virchow’s node – Left supraclavicular node
• Irish’s node – Axillary lymphadenopathy
• Blummer’s shelf – Tumor in the pelvic cul de sac
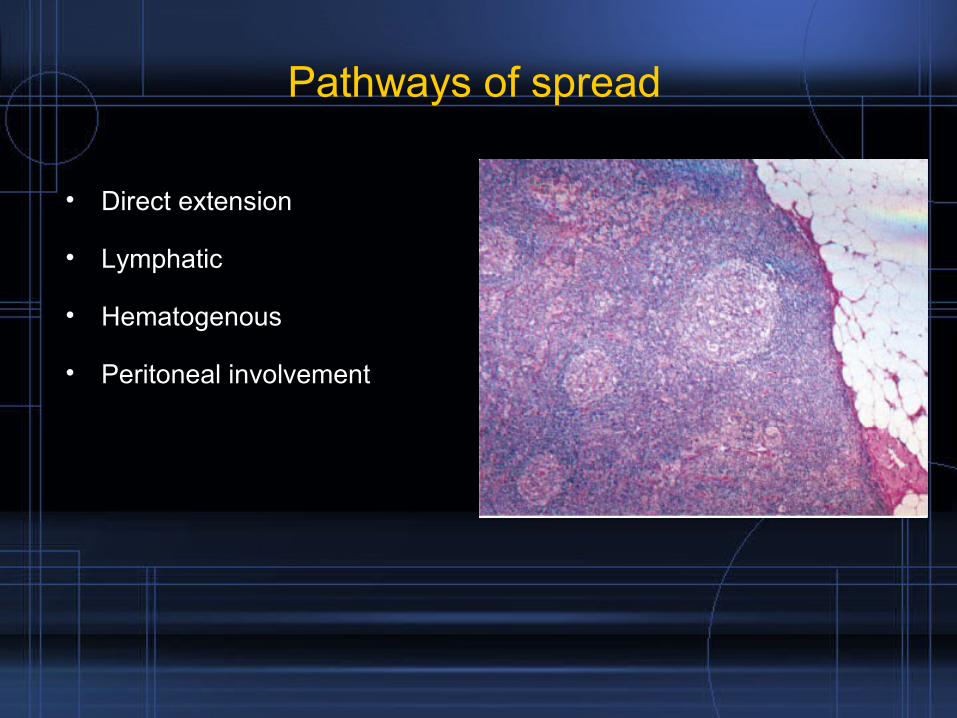
Pathways of spread
• Direct extension
• Lymphatic
• Hematogenous
• Peritoneal involvement
Clinical findings
• Dysphagia• Indigestion• Early satiety• Loss of appetite• Nausea• Abdominal pain• Weight loss• Gastric outlet obstruction• Anemia• Hematemesis• Melena• Lymphadenopathy
Diagnosis
• Often confused with benign
pathology
– GERD
– Ulcer
• Often diagnosed at an
advance stage
• Endoscopy
• Biopsy
Staging
• Upper endoscopy
• Chest x ray
• CT scan abdomen and pelvis
• EUS
• Laparoscopy
• Peritoneal cytology
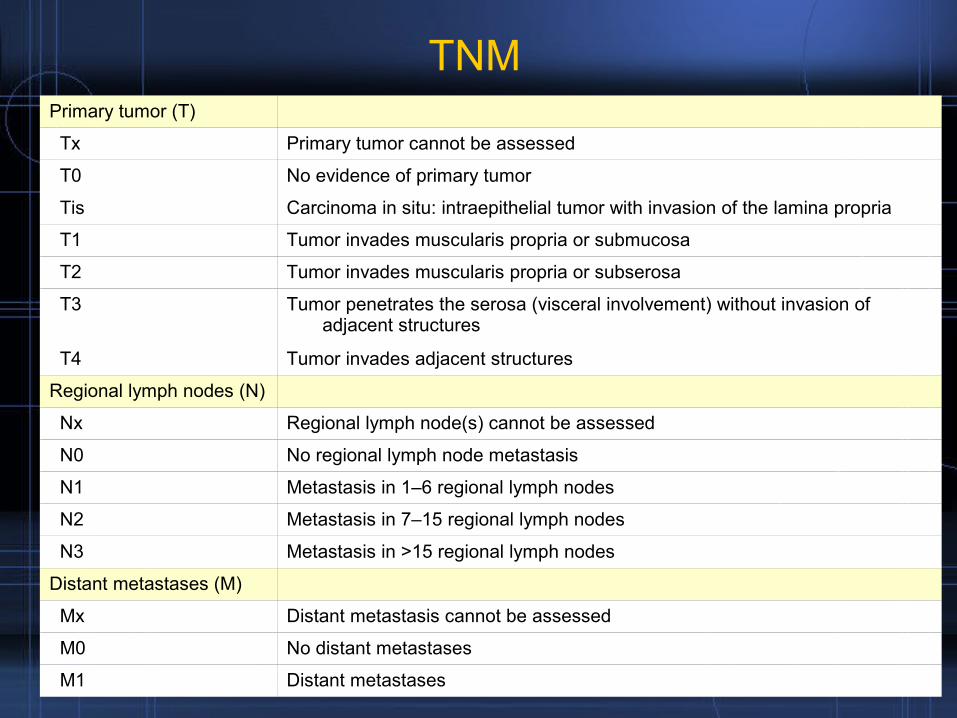
Primary tumor (T)
Tx Primary tumor cannot be assessed
T0 No evidence of primary tumor
Tis Carcinoma in situ: intraepithelial tumor with invasion of the lamina propria
T1 Tumor invades muscularis propria or submucosa
T2 Tumor invades muscularis propria or subserosa
T3 Tumor penetrates the serosa (visceral involvement) without invasion of adjacent structures
T4 Tumor invades adjacent structures
Regional lymph nodes (N)
Nx Regional lymph node(s) cannot be assessed
N0 No regional lymph node metastasis
N1 Metastasis in 1–6 regional lymph nodes
N2 Metastasis in 7–15 regional lymph nodes
N3 Metastasis in >15 regional lymph nodes
Distant metastases (M)
Mx Distant metastasis cannot be assessed
M0 No distant metastases
M1 Distant metastases
TNM
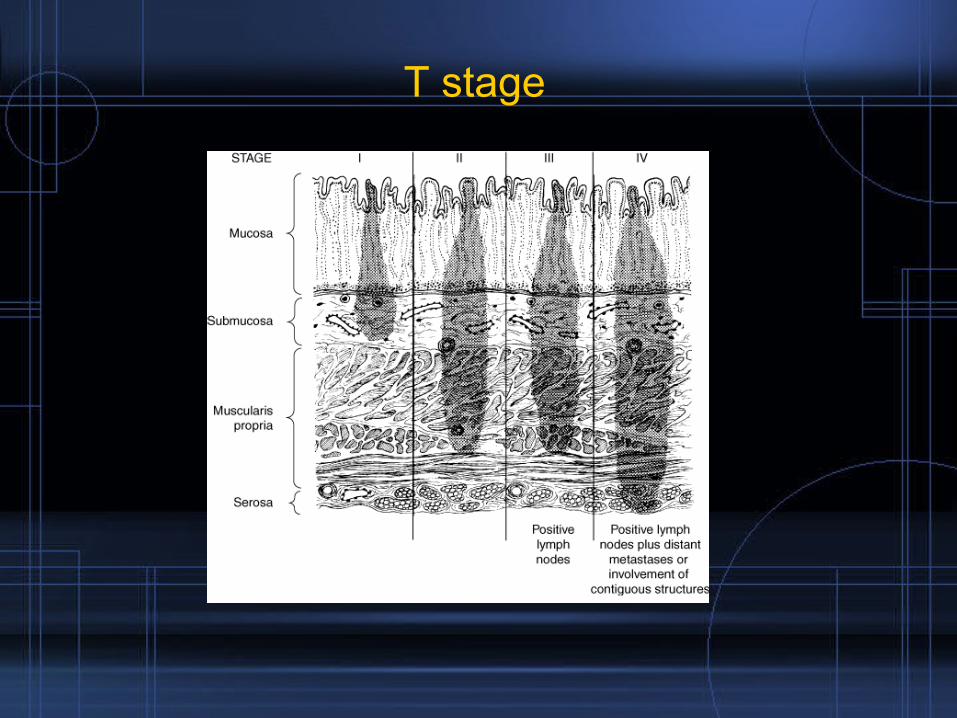
T stage
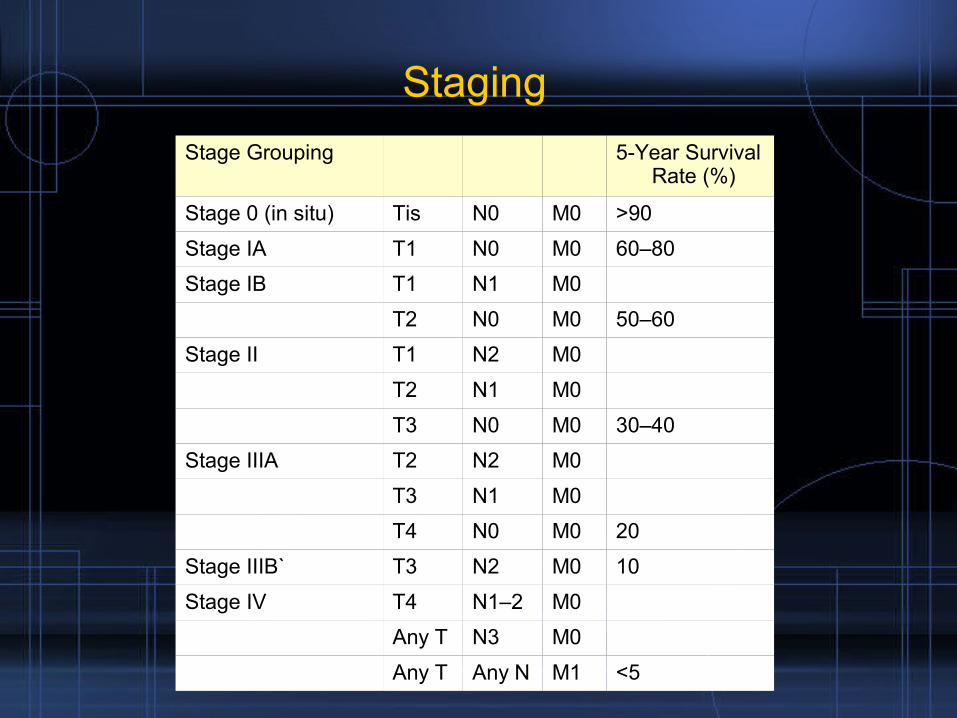
Stage Grouping 5-Year Survival Rate (%)
Stage 0 (in situ) Tis N0 M0 >90
Stage IA T1 N0 M0 60–80
Stage IB T1 N1 M0
T2 N0 M0 50–60
Stage II T1 N2 M0
T2 N1 M0
T3 N0 M0 30–40
Stage IIIA T2 N2 M0
T3 N1 M0
T4 N0 M0 20
Stage IIIB` T3 N2 M0 10
Stage IV T4 N1–2 M0
Any T N3 M0
Any T Any N M1 <5
Staging
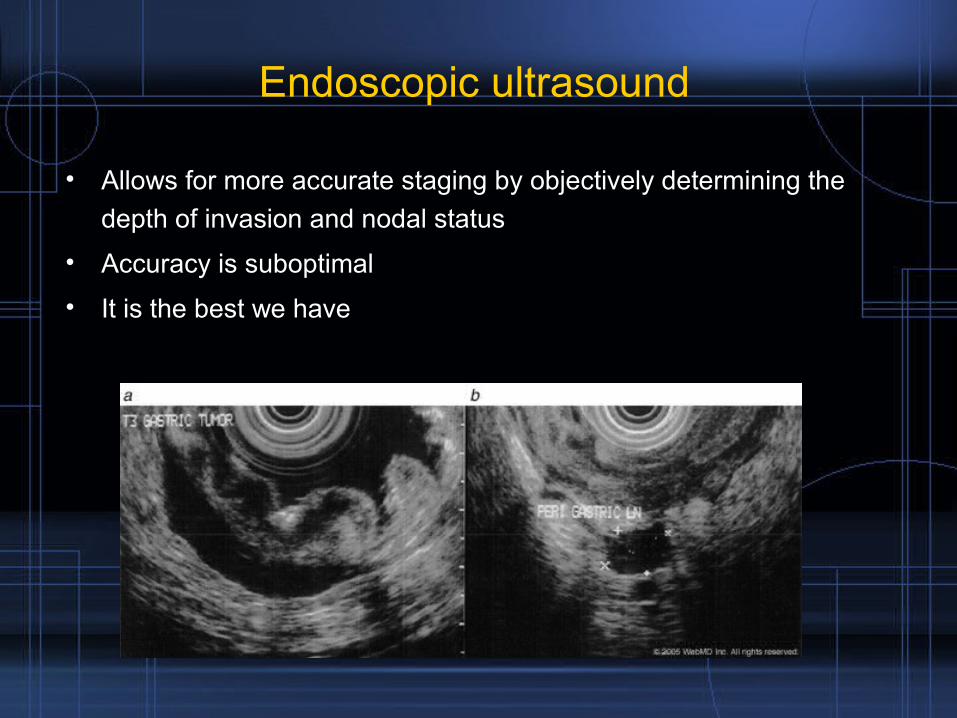
Endoscopic ultrasound
• Allows for more accurate staging by objectively determining the
depth of invasion and nodal status
• Accuracy is suboptimal
• It is the best we have
Clinical correlation of endoscopic ultrasonography with pathologic stage and outcome in patients undergoing curative resection for gastric cancer
D Bentrem et al. Ann Surg Onc 2006
• Retrospective review MSKCC• 225 patients with gastric CA• Preoperative EUS followed by R0 gastric resection• Exclusion of patients who received neoadjuvant therapies• EUS compared with anatomic pathology• Accuracy
– T stage 57 %– N stage 50 %
• Conclusion– Concordance was “lower than expected”– Difficult to differentiate between T2 and T3– EUS can identify high risk group of patients. Those with
serosal invasion and positive nodes
Laparoscopy
• Preoperative laparoscopy is occasionally done as part of the
staging efforts
• Goal is to evaluate for resectability and evidence of peritoneal or
liver metastasis prior to initiation of chemotherapy
• Allows for biopsy of suspicious lesions and peritoneal lavage
• Used in clinical trials
• Not standard of care
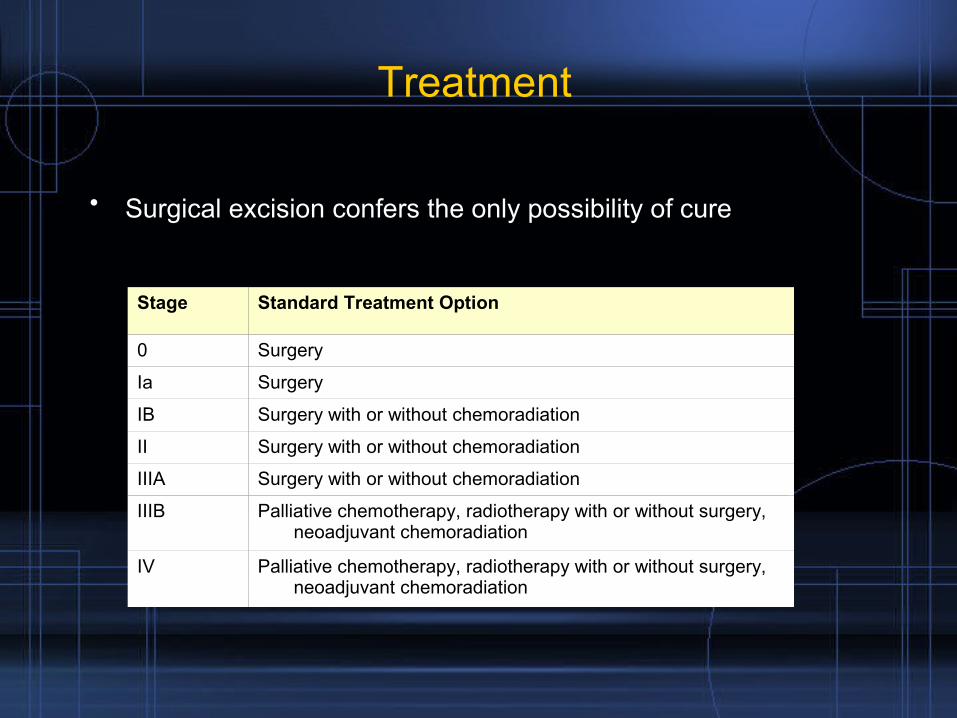
Treatment
• Surgical excision confers the only possibility of cure
Stage Standard Treatment Option
0 Surgery
Ia Surgery
IB Surgery with or without chemoradiation
II Surgery with or without chemoradiation
IIIA Surgery with or without chemoradiation
IIIB Palliative chemotherapy, radiotherapy with or without surgery, neoadjuvant chemoradiation
IV Palliative chemotherapy, radiotherapy with or without surgery, neoadjuvant chemoradiation
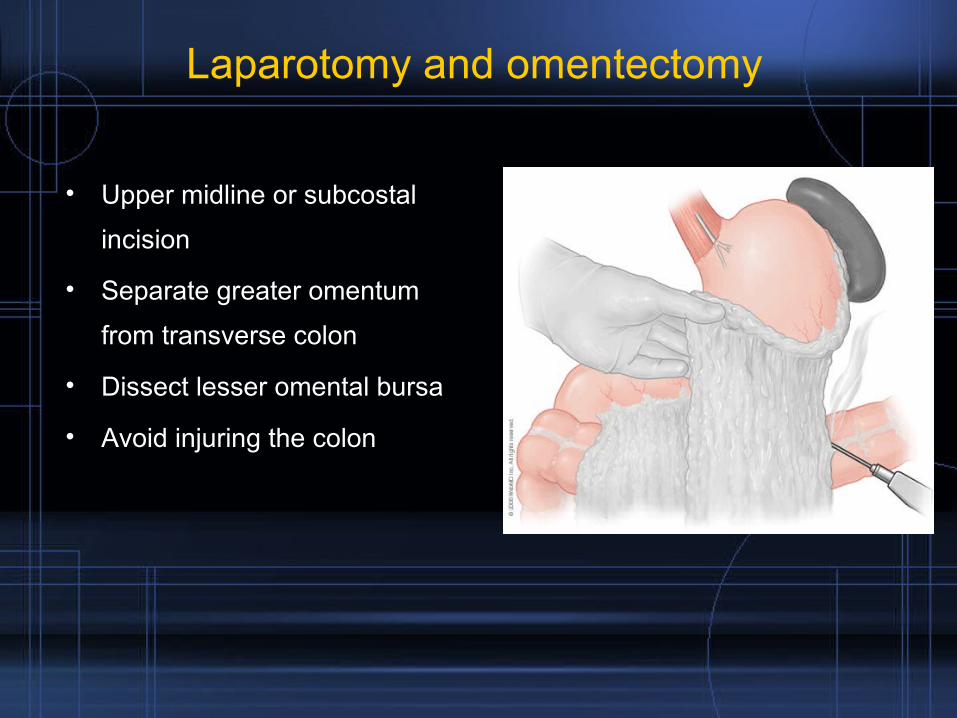
Laparotomy and omentectomy
• Upper midline or subcostal
incision
• Separate greater omentum
from transverse colon
• Dissect lesser omental bursa
• Avoid injuring the colon
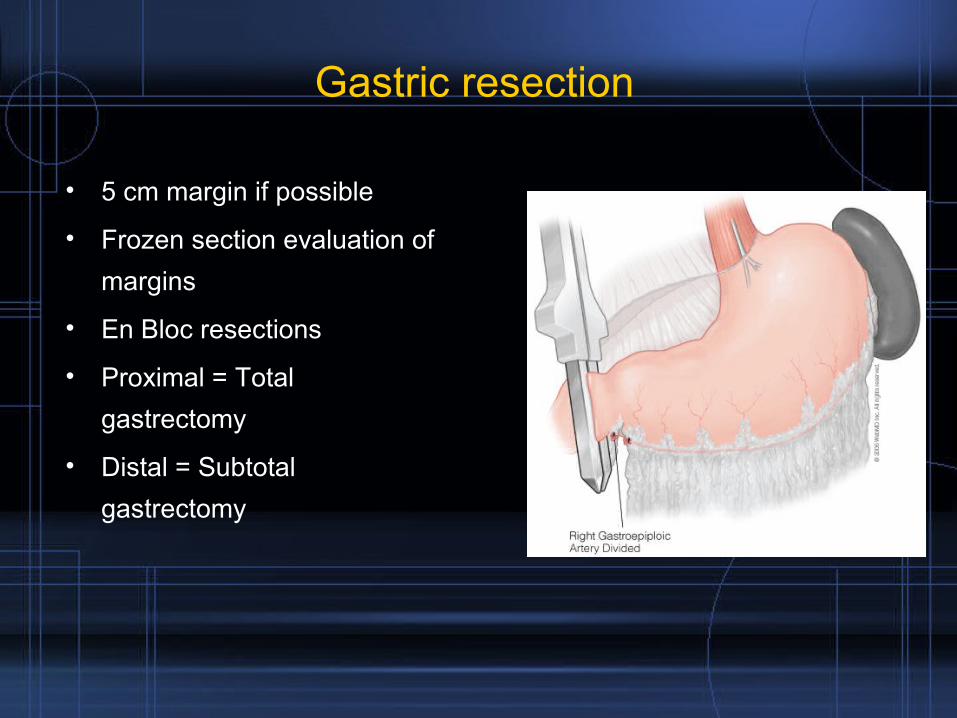
Gastric resection
• 5 cm margin if possible
• Frozen section evaluation of
margins
• En Bloc resections
• Proximal = Total
gastrectomy
• Distal = Subtotal
gastrectomy
Extent of resection
• Gastrectomy
– Subtotal gastrectomy has been shown to have an equivalent
oncologic result with significantly fewer complications
– For proximal tumors total gastrectomy is preferred over
proximal gastrectomy
• Splenectomy
– Routine performance of splenectomy has been associated
with increased morbidity without improvement in long term
survival
– Indicated if involved lymph nodes in splenic hylum
• En bloc resection
– should be done for local invasion into other organs
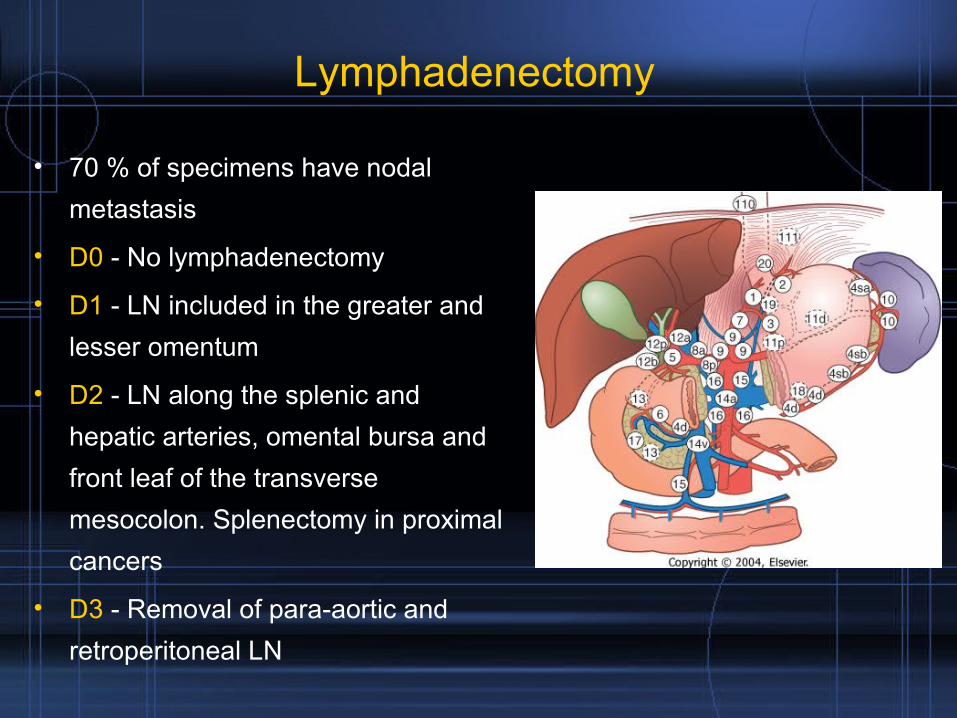
Lymphadenectomy
• 70 % of specimens have nodal
metastasis
• D0 - No lymphadenectomy
• D1 - LN included in the greater and
lesser omentum
• D2 - LN along the splenic and
hepatic arteries, omental bursa and
front leaf of the transverse
mesocolon. Splenectomy in proximal
cancers
• D3 - Removal of para-aortic and
retroperitoneal LN
Randomized comparison of morbidity after D1 and D2 disection for gastric cancer in 996 Dutch patientsJJ Bonenkamp et al, Lancet 1995
• Dutch gastric cancer study
• Randomized controlled trial
• Resectable gastric cancer
• 711 patients who underwent curative resection
• D1 380 D2 331
• Supervising surgeons were proctored by expert Japanese
surgeon experienced in gastric CA surgery
• Supervising surgeons attended every D2 dissection
• Significantly higher morbidity and mortality in D2
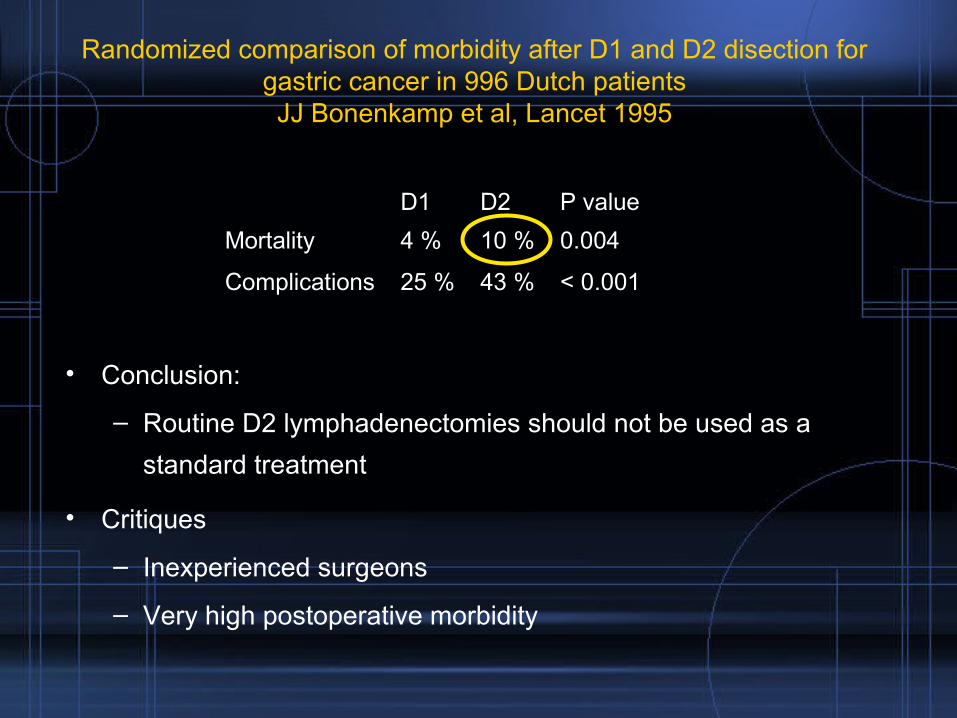
Randomized comparison of morbidity after D1 and D2 disection for gastric cancer in 996 Dutch patientsJJ Bonenkamp et al, Lancet 1995
• Conclusion:
– Routine D2 lymphadenectomies should not be used as a
standard treatment
• Critiques
– Inexperienced surgeons
– Very high postoperative morbidity
D1 D2 P value
Mortality 4 % 10 % 0.004
Complications 25 % 43 % < 0.001
D1 Vs D2 lymphadenectomy
• Similar trial from England (Medical research council trial) showed
equivalent results
• Due to this trials the routine performance of a distal
pancreatectomy and splenectomy has been eliminated
• A D2 lymphadenectomy is viewed as a superior oncologic
operation and it should continue to be performed by experienced
oncologic surgeons with minimal morbidity
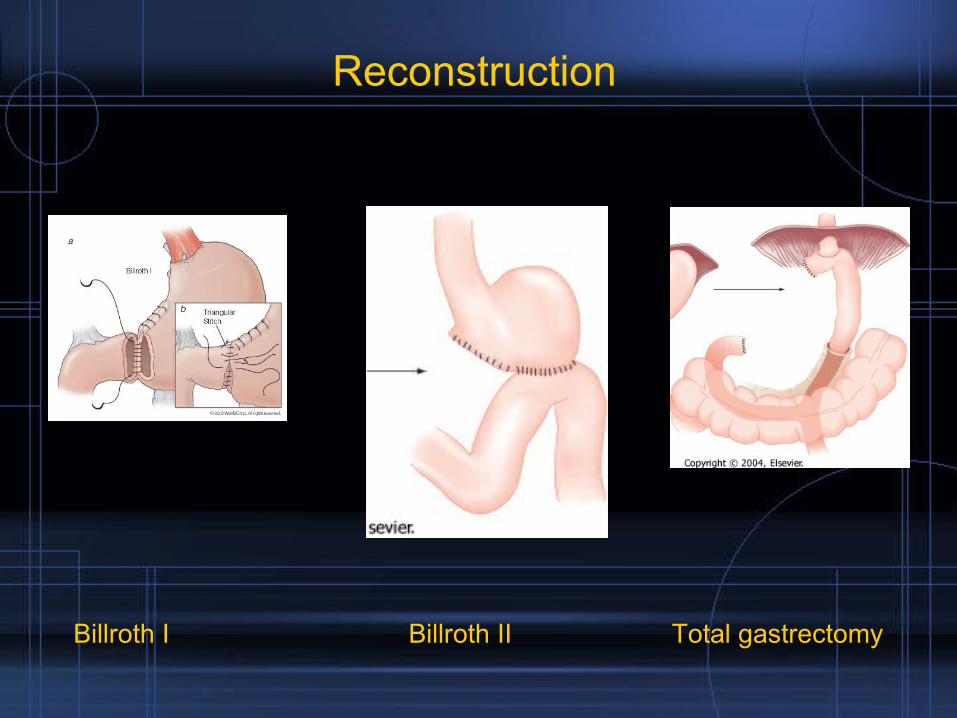
Reconstruction
Billroth I Billroth II Total gastrectomy
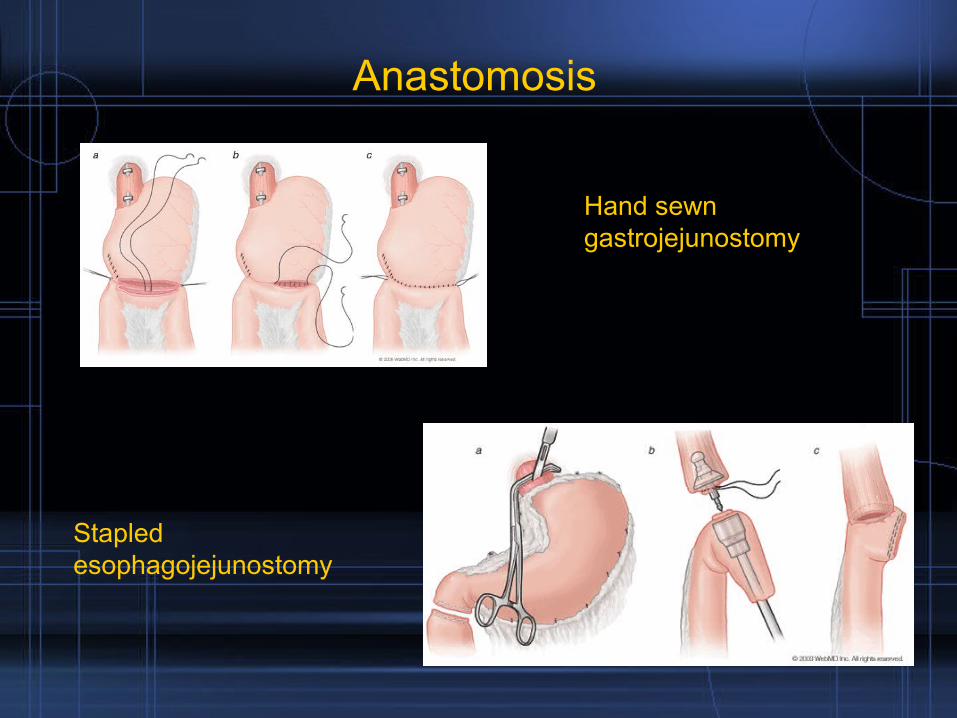
Anastomosis
Hand sewn gastrojejunostomy
Stapled esophagojejunostomy
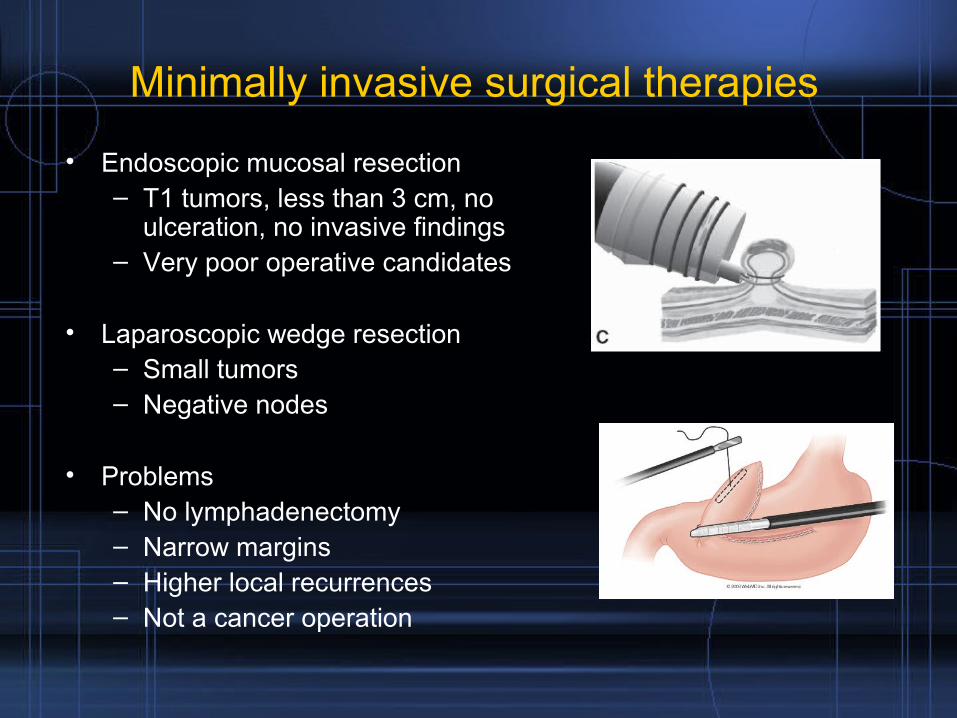
Minimally invasive surgical therapies
• Endoscopic mucosal resection– T1 tumors, less than 3 cm, no
ulceration, no invasive findings– Very poor operative candidates
• Laparoscopic wedge resection– Small tumors– Negative nodes
• Problems– No lymphadenectomy– Narrow margins– Higher local recurrences– Not a cancer operation
“R” status
• R0: No macroscopic or microscopic cancer at
resection margin ( - margins)
• R1: Microscopic residual cancer (+ margin)
• R2: Gross residual cancer
Nutrition
• Feeding catheher jejunostomy
• Aggressive nutritional supplementation
• Vitamin deficits
• Postgastrectomy diet
Post-gastrectomy syndromes
• Dumping
– Very common
– Due to absence of pylorus and rapid entry of hyperosmolar solutions into the small bowel
– Early - 20 min
• GI symptoms nausea, vomiting, fullness
• Cardiovascular symptoms, palpitations, tachycardia, diaphorsesis
• Secondary to the release of hormones (bradykinin, serotonin)
– Late 2 hours• Caused by rapid delivery of carbohydrates into the small intestine
• Hyperinsulinemia with resultant hypoglycemia
• Recommendation is to eat frequent small meals
Post-gastrectomy syndromes
• Metabolic disturbances– Worse with Billroth 2
– Megaloblastic anemia• B12 deficiency – Due to lack of intrinsic factor
– Steatorrhea
Post-gastrectomy syndromes
• Afferent loop syndrome
– Caused by partial obstruction of the afferent limb
– Kinking , adhesions, stenosis
– Limb distention > Cramping > Bilious vomiting
– Acute or chronic
– Blind loop syndrome
Post-gastrectomy syndromes
• Efferent loop obstruction– Limb obstruction caused by retroanastomotic herniation
• Alkaline reflux gastritis– Epigastric pain, bilious vomiting– More common with B2
• Retained antral syndrome– Retained antrum in duodenal side – Hypergastrinemia > Increased gastric acid– Document duodenal mucosa on frozen section
Neo-adjuvant Therapies for Gastric Cancer: An Alternative Approach to an Old Problem
Eduardo A. Guzman MD
Status quo
• Gastric cancer still has a high mortality
– Overall 5 yr survival 10 % to 20 %
– Overall 5 yr survival after curative resection 24 % to 57 %
• High rates of recurrences– 40 to 80 %– Locoregional failure
• 38 – 45%– Peritoneal metastasis
• 54 %• Low rates of R0 resection < 50 % of patients
• Significant delays in initiation of adjuvant therapy
– 1/3 of patients do not recover quickly enough
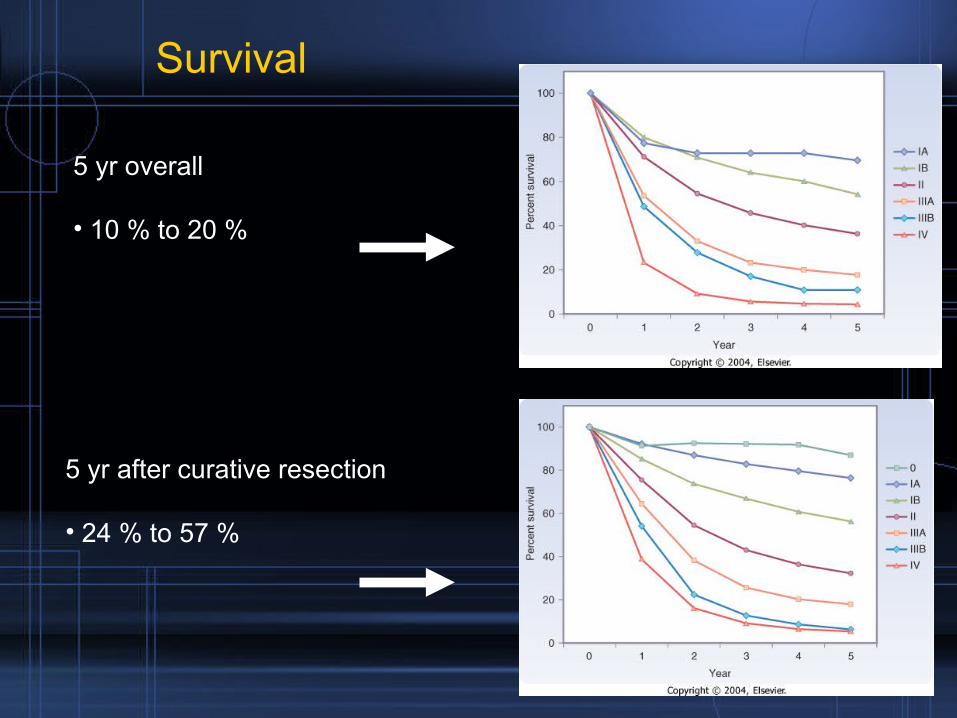
Survival
5 yr after curative resection
• 24 % to 57 %
5 yr overall
• 10 % to 20 %
Is there anything we can do about it?
Adjuvant therapies
Adjuvant radiation
• Not much data
• RCT by British stomach cancer group 1989
• 436 patients randomized
– Surgery
– Surgery + radiation
• No survival difference
• Depressed locoregional failure rates
– Surgery 27 %
– Surgery + radiation 10 %
• Radiation is helpful in improving local control rates
Adjuvant chemotherapy
• Multiple studies
• Phase III RCT by EORTC - Lise M et al JCO 1995
• 314 patients with resected gastric CA
• FAM2 regimen = 5 Fu + doxorubicin + mitomycin
• Randomized
– Surgery
– Surgery + FAM2
• No difference in overall survival
• Highly toxic regimen
• Adjuvant chemotherapy alone has failed to demonstrate significant improvements in survival
• HR Rosen JCO 1998
• Phase III multicentric trial
• 91 patients 1994 1997
• Gastric adenocarcinoma s/p R0 resection
• Randomized intraoperatively
– Intraperitoneal mitomycin C
– No further tx
• Median follow up 597 days
Adjuvant intraperitoneal chemotherapy
• Complications
– Mitomycin C 35 %
– Control 16 %
• Mortality
– Mitomycin C 11 %
– Control 2 %
• Conclusion
– Adjuvant Mitomycin C is associated with an increased rate of postoperative complications without improvements in long term survival
• Currently there is no role for IP chemotherapy outside of a clinical trial
• John S. MacDonald NEJM 2001
• To investigate the effect of surgery + adjuvant chemoradiotherapy on survival
• 556 selected patients with resected gastric cancer
• 66 %T3 T4 85 % nodal metastasis
• Postoperative randomization
– Surgery alone
– Surgery > 5 FU + Leucovorin > 4500 cGy > 5 FU + Leucovorin
• R0 resection
• D2 lymphadenectomy 10 % pts
• Median follow up 5 years
Adjuvant chemoradiation
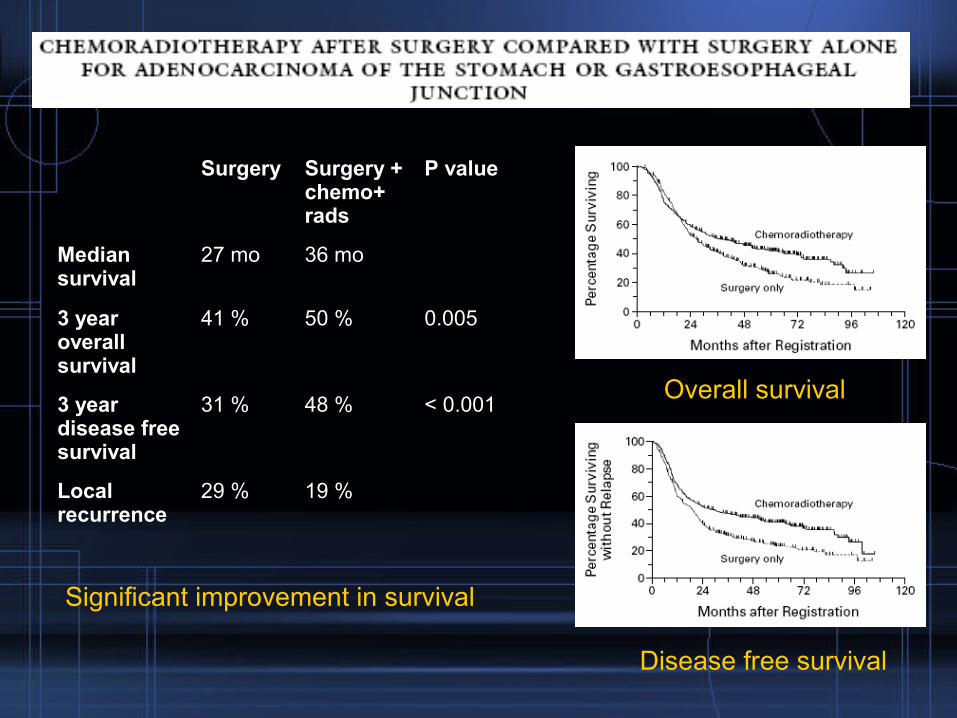
Surgery Surgery + chemo+ rads
P value
Median survival
27 mo 36 mo
3 year overall survival
41 % 50 % 0.005
3 year disease free survival
31 % 48 % < 0.001
Local recurrence
29 % 19 %
Significant improvement in survival
Overall survival
Disease free survival
• Conclusion: – Adjuvant chemoradiotherapy should be considered in all
patients at high risk of recurrence of gastric cancer who have undergone a curative resection
• Critiques– Considerable toxicity (41 % grade 3, 32 % grade 4)– Incomplete lymphadenectomies (D2 10 %)– These findings suggest that the main effect of chemoradiation
was to compensate for inadequate surgery
• Based on this trial, adjuvant chemoradiation has become “standard of care” on patients with completely resected gastric cancer other than T1
Can we do any better?
Neoadjuvant therapies
Benefits of preoperative therapies
• Increased patient compliance
• Specially postgastrectomy patients who suffer from long
postoperative recovery periods
• Avoidance of curative surgery in patients who rapidly develop
metastatic disease (10 – 15 % of T3 pts)
• Selection of patients with not so aggressive disease
• Tumor downstaging – Improved resectability
• Early initiation of systemic therapy
• Better tissue oxygenation
• Easier to define radiation fields ( removal of surgeon effect
• H Hartgrink European Journal of Surgical Oncology 2004
• To evaluate the effect of preoperative chemotherapy on resectability and survival
• FAMTX = 5-flouroracil + doxorubicin + methotrexate
• 59 patients 1993 -1996
• Randomization
– 4 cycles FAMTX >> Surgey
– Surgery alone
Neoadjuvant chemotherapy
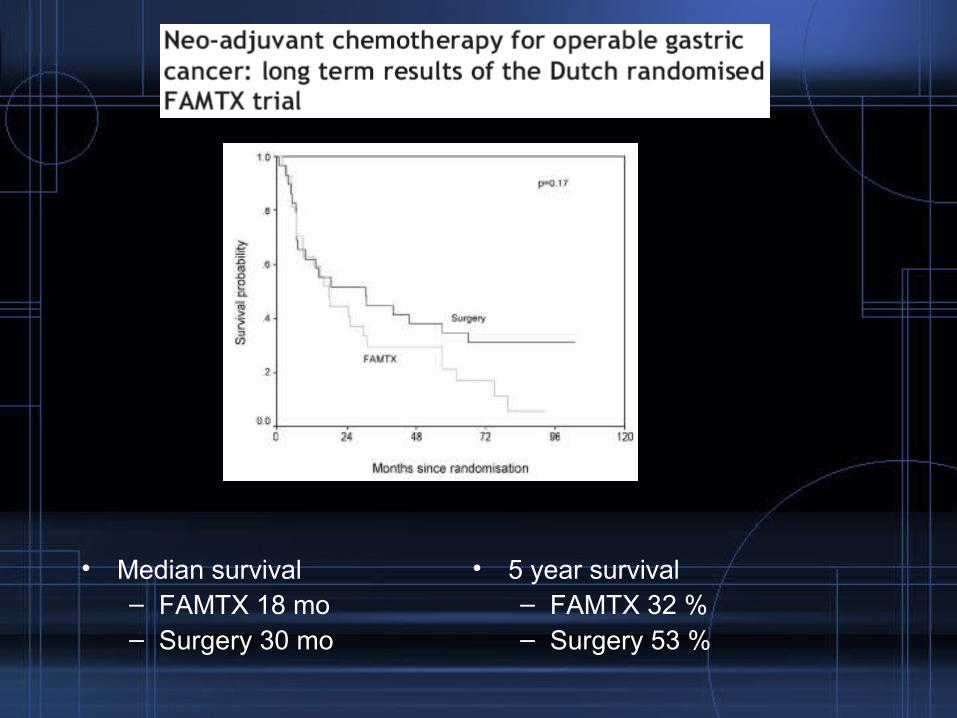
• Median survival– FAMTX 18 mo– Surgery 30 mo
• 5 year survival – FAMTX 32 %– Surgery 53 %
• Conclusion– No beneficial effect of preoperative FAMTX chemotherapy
• Critiques– Trial was closed prematurely due to lack of tumor downstaging
combined with no survival diference.– Poor trial
• MAGIC trial D Cunningham NEJM 2006
• Regimen of epirubicin, cisplatin and infused fluorouracil has been shown to improve survival in patients with locally advanced and metastatic gastric adenocarcinoma
• Evaluate whether the addition of this regimen to surgery improves outcomes
• Prospective Randomized multi-center
• 453 patients were randomized
– ECF > Surgery > ECF
– Surgery
• Median follow up 4 years
• Perioperative morbidity and mortality were similar between groups
Neoadjuvant chemotherapy

Overall survival Disease free survival
•5 year overall survival
–Surgery 23 %
–Chemotherapy + surgery 36 %
• Conclusion: Perioperative ECF decreases tumor size and stage and improves both overall and disease free survival
• Critiques– Tumor heterogeneity
• 25 % of patients had esophageal and GE junction tumors
– Treatment toxicity• Only 42 % of the patients in the perioperative group completed all
protocol treatments• 34 % of the patients who completed preoperative chemotx + surgery did
not undergo postop chemotx
– Inadequate staging• Only 70 % of the patients had their tumor size recorded prior to surgery• No EUS, no laparoscopy
– No radiation, older generation drugs
• Despite the impressive results of the trial, neoadjuvant chemotherapy with an ECF regimen has not been adopted as standard of care
What else is coming down the pipeline?
Phase II trials
Investigational treatments
• Phase II clinical trial J Ajani JCO 2006
• Primary aim: Achievement of a 20 % pathologic complete response in a multinstitutional setting
• Rigorous staging: EUS, laparoscopy, peritoneal lavage
• 20 institutions 43 patients
• 5FU + Cisplatin >>> 4500 cGY + 5fu >>> Surgery
• 50 % had a D2 Lymphadenectomy• Median follow up 21.6 months• Path Cr 26 % • R0 resection 77 % • Grade 4 toxicity 21%
Neoadjuvant chemoradiation
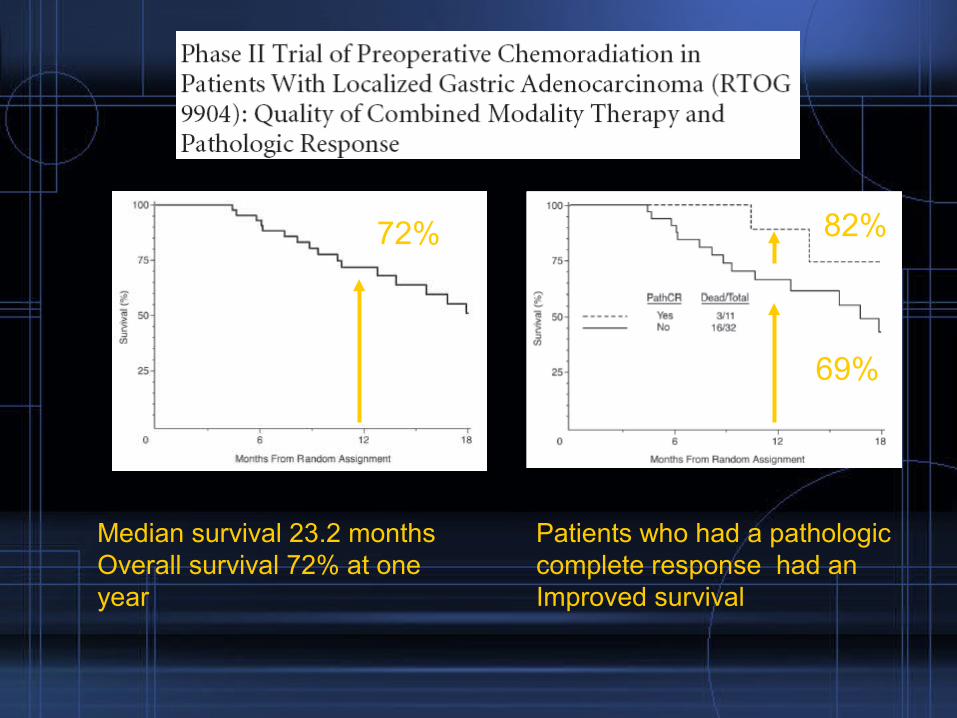
Median survival 23.2 monthsOverall survival 72% at one year
72% 82%
69%
Patients who had a pathologic complete response had an Improved survival
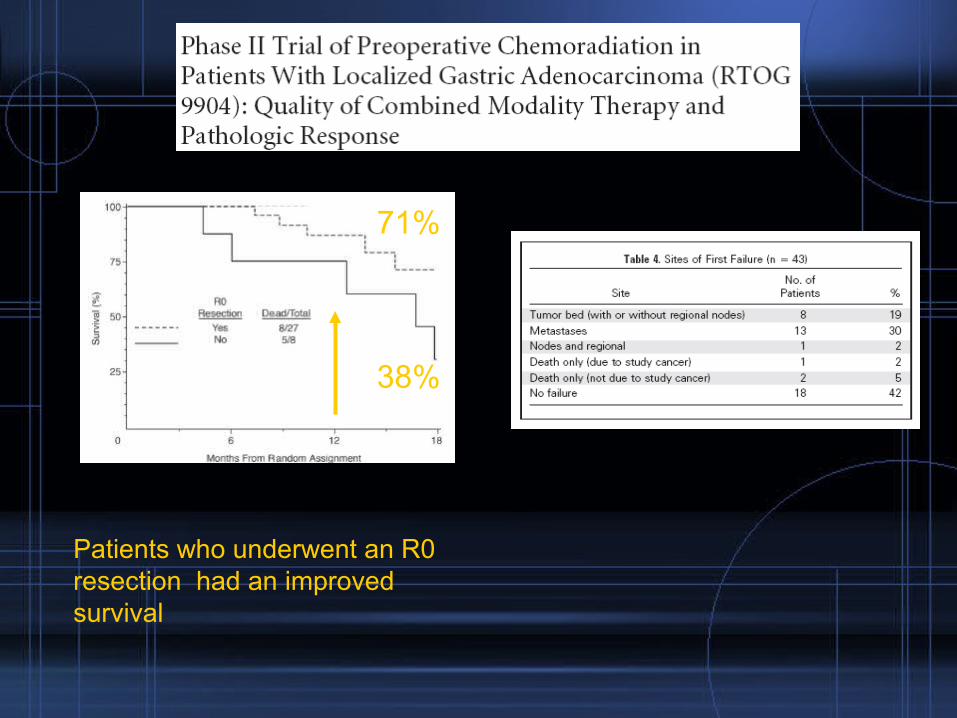
71%
38%
Patients who underwent an R0 resection had an improved survival
• Conclusion– A preoperative chemoradiotherapy strategy proved to be
succesful in a cooperative group setting with acheivement of a pathological complete response rate of over 20 %
• Critiques– Small number of patients– Phase II trial – No comparison arm
• Based on this results, a preoperative chemoradiation strategy is to be compared with adjuvant chemoradiation in a phase III clinical trial
What is the future?
• Neoadjuvant therapies vs adjuvant chemoradiation
• Trial CALGB (Cancer and Leukemia Group B) 80101
– Assessing the role of a potentially more active postoperative
chemoradiation regimen
• Magic B study
– Examine the role of adding bevacizumab to perioperative
chemotherapy
• CRITICS
– Evaluate the role of postoperative chemoradiation in combination with
preoperative chemotherapy
• Immunotherapy
Summary
• Gastric cancer remains a challenging disease to treat
– High mortality
– High rates of locoregional recurrences
– Low R0 resection
• Extended lymphadenectomies have not proven beneficial,
although still being performed by advanced centers
• Adjuvant chemoradiotherapy remains standard of care
• Neoadjuvant therapy approaches have not been proven to be
superior to adjuvant chemoradiation
• Neoadjuvant chemoradiation awaits it evaluation under a
randomized clinical trial
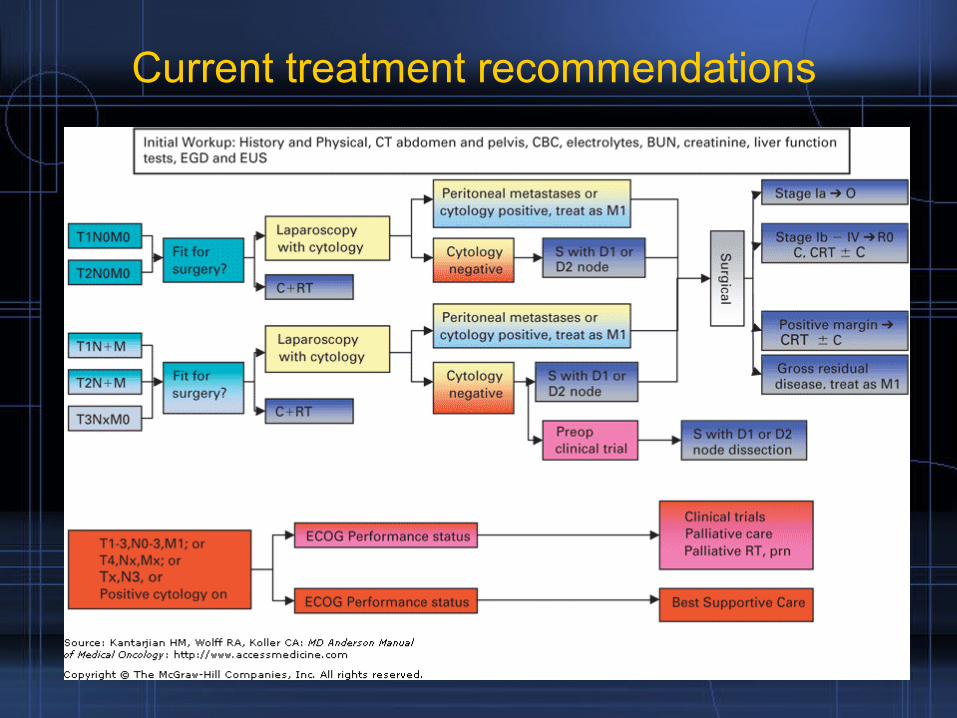
Current treatment recommendations
Conclusion
• The introduction of neoadjuvant therapy protocols appears likely
to favorably impact tumor resectability, local control and overall
survival
• Phase III randomized controlled trials are required to prove its
efficacy









![[Ghiduri][Cancer]Gastric Cancer](https://img.pdfslide.us/doc/110x75/55cf9399550346f57b9de771/ghiduricancergastric-cancer.jpg)