Embed Size (px)
Citation preview

J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 9 , N O . 1 6 , 2 0 1 6
ª 2 0 1 6 B Y T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y F O UN DA T I O N I S S N 1 9 3 6 - 8 7 9 8 / $ 3 6 . 0 0
P U B L I S H E D B Y E L S E V I E R h t t p : / / d x . d o i . o r g / 1 0 . 1 0 1 6 / j . j c i n . 2 0 1 6 . 0 5 . 0 4 8
CLINICAL RESEARCH
CORONARY
Predictors, Trends, and Outcomes(AmongOlder Patients$65 Years of Age)AssociatedWithBeta-BlockerUseinPatientsWith Stable Angina Undergoing ElectivePercutaneous Coronary InterventionInsights From the NCDR Registry
Apurva A. Motivala, MD,a Valay Parikh, MD,b Matthew Roe, MD, MHS,c David Dai, PHD,c J. Dawn Abbott, MD,d
Abhiram Prasad, MD,e,f Debabrata Mukherjee, MD, MSg
ABSTRACT
OBJECTIVES This study sought to examine predictors, trends, and outcomes associated with b-blocker prescriptions at
discharge in patients with stable angina without prior history of myocardial infarction (MI) or systolic heart failure (HF)
undergoing elective percutaneous coronary intervention (PCI).
BACKGROUND The benefits of b-blockers in patients with MI and/or systolic HF are well established. However,
whether b-blockers affect outcomes in patients with stable angina, especially after PCI, remains uncertain.
METHODS We included patients with stable angina without prior history of MI, left ventricular systolic dysfunction (left
ventricular ejection fraction <40%) or systolic HF undergoing elective PCI between January 2005 and March 2013 from
the hospitals enrolled in the National Cardiovascular Data Registry (NCDR) CathPCI registry. These patients were
retrospectively analyzed for predictors and trends of b-blocker prescriptions at discharge. All-cause mortality (primary
endpoint), revascularization, or hospitalization related to MI, HF, or stroke at 30-day and 3-year follow-up were analyzed
among patients $65 years of age.
RESULTS A total of 755,215 patients from 1,443 sites were studied, and 71.4% population of our cohort was discharged
on b-blockers. At 3-year follow-up among patients $65 years of age with CMS data linkage (16.3% of the studied
population), there was no difference in adjusted mortality rate (14.0% vs. 13.3%; adjusted hazard ratio [HR]: 1.00; 95%
confidence interval [CI]: 0.96 to 1.03; p ¼ 0.84), MI (4.2% vs. 3.9%; adjusted HR: 1.00; 95% CI: 0.93 to 1.07; p ¼ 0.92),
stroke (2.3% vs. 2.0%; adjusted HR: 1.08; 95% CI: 0.98 to 1.18; p ¼ 0.14) or revascularization (18.2% vs. 17.8%; adjusted
HR: 0.97; 95% CI: 0.94 to 1.01; p ¼ 0.10) with b-blocker prescription. However, discharge on b-blockers was associated
with more HF readmissions at 3-year follow-up (8.0% vs. 6.1%; adjusted HR: 1.18; 95% CI: 1.12 to 1.25; p < 0.001).
Results at 30-day follow-up were broadly consistent as well. During the period between 2005 and 2013, there was a
gradual increase in prescription of b-blockers at the index discharge in our cohort (p < 0.001).
CONCLUSIONS Among patients $65 years of age with history of stable angina without prior MI, systolic HF or left
ventricular ejection fraction <40% undergoing elective PCI, b-blocker use at discharge was not associated with
any reduction in cardiovascular morbidity or mortality at 30-day and at 3-year follow-up. Over time, b-blockers
use at discharge in this population has continued to increase. (J Am Coll Cardiol Intv 2016;9:1639–48)
© 2016 by the American College of Cardiology Foundation.

ABBR EV I A T I ON S
AND ACRONYMS
ACC/AHA = American College
of Cardiology/American Heart
Association
CABG = coronary artery bypass
graft
CAD = coronary artery disease
CI = confidence interval
CMS = Centers for Medicare
and Medicaid Services
HF = heart failure
HR = hazard ratio
LV = left ventricular
LVEF = left ventricular ejection
fraction
NCDR = National
Cardiovascular Data Registry
PCI = percutaneous coronary
intervention
From the a
Staten Isla
Durham, NeDivision o
Kingdom;
research gr
Association
Amgen, Me
theyhaven
Manuscrip
Motivala et al. J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 9 , N O . 1 6 , 2 0 1 6
b-Blockers Following Elective PCI for Stable Angina A U G U S T 2 2 , 2 0 1 6 : 1 6 3 9 – 4 8
1640
Beta-blockers have consistently beenshown to improve cardiovascular out-comes, including survival, in coronary
artery disease (CAD) patients with myocar-dial infarction (MI) and in systolic heart fail-ure (HF) (1–4). Based on the strength ofevidence, use of b-blockers has a Class 1recommendation in the American College ofCardiology/American Heart Association(ACC/AHA) guidelines for these cardiovascu-lar conditions (5–7). b-blockers have beenshown to be effective in improving cardiacoutcomes in patients with CAD with stableangina without prior MI or systolic HF insome studies (8,9), but not in others (10–14).Nevertheless, b-blockers have consistentlybeen shown to provide an antianginal effect(15,16) and are considered a first line forantianginal therapy in this population (17). Inaddition, b-blockers are recommended as a
first line therapy for management of hypertension in
SEE PAGE 1649
patients with CAD (18) and have been used exten-sively for this indication (19,20). Because of thesereasons and findings of the landmark COURAGE(Clinical Outcomes Utilizing Revascularization andAggressive Drug Evaluation) trial (21–23), b-blockersremain an integral component of optimal medicaltherapy in patients with stable angina not undergoingrevascularization. However, whether b-blockersreduce morbidity and mortality in patients with sta-ble angina without prior MI and/or systolic HF, afterrevascularization with percutaneous coronary inter-vention (PCI) remains unclear.
Hence, using a very large contemporary databaserepresentative of U.S. population, we sought to: 1)evaluate the comparative effectiveness of the use ofb-blockers in patients with stable angina withoutprevious history of MI or systolic HF, who underwentan elective PCI; and 2) assess predictors and temporaltrends affecting prescription of b-blockers atdischarge in this population.
Division of Cardiology, Columbia University, New York, New Yor
nd University Hospital, Staten Island, New York; cDuke Clinical
orth Carolina; dDivision of Cardiology, Warren Alpert Medical S
f Cardiovascular Diseases, Mayo Clinic, Rochester, Minnesota; fS
and the gDivision of Cardiology, Texas Tech University Health S
ant support from Eli Lilly & Company, Sanofi, Daiichi-Sankyo, the
, and the Familial Hypercholesterolemia Foundation; and honorar
rck, and AstraZeneca. Dr. Abbott has received research grant supp
orelationships relevant to thecontentsof thispaper todisclose.Drs
t received February 11, 2016; revised manuscript received April 29
METHODS
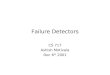
STUDY POPULATION. Our analysis included all pa-tients with stable angina undergoing elective PCI atany center participating in the NCDR CathPCI registrybetween January 1, 2005, and March 31, 2013(Figure 1). Each participating site within the registryhad institutional review board approval for waiver ofconsent for data entry. Patients with prior history ofMI, left ventricular (LV) systolic dysfunction (leftventricular ejection fraction [LVEF] <40%), or sys-tolic HF, prior coronary artery bypass graft (CABG),and documented contraindications to b-blockers wereexcluded. This whole cohort was used to evaluate thetrends and predictors of prescription of b-blockersat discharge. Outcomes following discharge wereanalyzed in a subset of this overall populationrestricted to patients $65 years of age using a link tothe Centers for Medicare and Medicaid Services (CMS)fee-for-service data (24,25).
CLINICAL OUTCOMES. Primary outcome was postdischarge all-cause mortality (at 30-day and 3-yearfollow-up) using CMS longitudinal claims data in asubgroup of patients $65 years of age. Secondaryoutcomes included the use of revascularization pro-cedures (PCI or CABG), and cause-specific read-mission for MI, HF, and stroke. Additionally, acomposite outcome of all-cause mortality, revascu-larization and cause-specific readmission for MI, HFor stroke was evaluated. The trends and predictorsassociated with prescription of b-blockers atdischarge were also evaluated. The InternationalClassification of Diseases-Ninth Revision codes usedto define these events based on primary admissiondiagnoses were hospitalization due to MI (410.x1),hospitalization due to stroke (434.x1, 436, or 433.x1)hospitalization due to HF (402.01, 402.11, 402.91,404.01, 404.03, 404.11, 404.13, 404.91, 404.93,428.xx), and revascularization (any of ICD-9 pro-cedures PX1, PX2, PX3, PX4, PX5, PX6) has thefollowing: (PCI: 00.66, 36.01-09; CABG: 36.10-19). Toevaluate long-term outcomes, CathPCI Registry stent
k; bDivision of Cardiology, Department of Medicine,
Research Institute/Duke University Medical Center,
chool, Brown University, Providence, Rhode Island;
t. George’s, University of London, London, United
ciences Center, El Paso, Texas. Dr. Roe has received
American College of Cardiology, the American Heart
ia from Elsevier Publishers, Janssen Pharmaceuticals,
ort from Gilead. All other authors have reported that
.ParikhandMotivalacontributedequally to thiswork.
, 2016, accepted May 19, 2016.

FIGURE 1 Study Population Flow Diagram
Flow diagram showing the process to define the study population. ACS ¼ acute coronary syndrome; CABG ¼ coronary artery bypass graft;
CMS ¼ Centers for Medicare and Medicaid Services; EF ¼ ejection fraction; HF ¼ heart failure; NCDR ¼ National Cardiovascular Data Registry;
MI ¼ myocardial infarction; PCI ¼ percutaneous coronary intervention.
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 9 , N O . 1 6 , 2 0 1 6 Motivala et al.A U G U S T 2 2 , 2 0 1 6 : 1 6 3 9 – 4 8 b-Blockers Following Elective PCI for Stable Angina
1641
procedures between January 1, 2005, and December31, 2009 were linked to Medicare’s 100% inpatientfee-for-service claims files using indirect identifiers(e.g., index PCI procedure site, patient date of birth orage, admission, discharge date, sex), as previouslydescribed (24). Sites that did not match to Medicarerecords were excluded, as were patients whose indexPCI procedure did not occur during a period of fee-for-service enrollment.
STATISTICAL ANALYSIS. Mean values, standarddeviations, and percentages are used to describe thebaseline characteristics. Differences in baselinecharacteristics between patients discharged withb-blockers and without b-blockers were compared byuse of Pearson chi-square test for categorical vari-ables and Wilcoxon rank sum test for continuousvariables.
Univariate and multivariate logistic regressionmodels containing various clinical and angiographicvariables were used to estimate the marginal effectsof each factor on prescriptions of b-blockers atdischarge (Online Table 1). The generalized esti-mating equation method with exchangeable workingcorrelation structure was used to account for within-hospital clustering. The cumulative incidence ratesfor time-to-event outcomes were estimated and dif-ferences were tested using Gray’s method (26). Thedifferences in unadjusted and adjusted analyses areexpressed as hazard ratio (HR) with 95% confidenceinterval (CI).
To assess whether the use of b-blocker at dischargein the overall cohort and pre-defined subgroupssignificantly changed over time, we used logisticregression with generalized estimating equations toaccount for within-hospital clustering. For thegeneralized estimating equation analysis we assumedthe exchangeable correlation structure.
In all calculations, the statistical tests were 2-sidedwith the significance defined as a p value <0.05. Allanalyses were performed at the Duke ClinicalResearch Institute with SAS statistical software(version 9.3, SAS Institute, Cary, North Carolina).
RESULTS
SAMPLE CHARACTERISTICS. The entire NCDR Cath-PCI registry population during the study periodincluded 4,523,488 patients from 1,443 sites. Ofthese, 3,132,750 (69.3%) patients were excluded dueto a presentation with acute coronary syndrome,276,418 (6.1%) patients due to prior history of CABGsurgery, 289,707 (6.4%) patients due to prior historyof MI, 46,208 (1%) patients due to prior history ofsystolic HF or LVEF <40% and 23,190 (0.5%) due todocumented contraindication to b-blockers. The finalstudy population included 755,215 patients (16.7% ofthe total NCDR CathPCI registry dataset during thestudy period). All 755,215 patients were used toidentify trends and predictors related to b-blockerusage as well as in-hospital outcomes. Post-discharge

TABLE 1 Baseline Clinical and Procedural Characteristics
DischargedWith
b-Blockers(n ¼ 539,521)
DischargedWithout
b-Blockers(n ¼ 215,694) p Value
Age, yrs 65.4 � 11.2 65.7 � 10.9 <0.001
Male 343,480 (63.7) 142,008 (65.8) <0.001
Body mass index, kg/m2 30.4 � 6.5 29.9 � 6.4 <0.001
Current/recent smoker 103,184 (19.1) 42,129 (19.5) <0.001
Hypertension 455,737 (84.5) 163,916 (76.0) <0.001
Diabetes 193,766 (35.9) 72,155 (33.5) <0.001
Peripheral vasculardisease
60,466 (11.2) 24,022 (11.1) 0.38
Cerebrovascular disease 56,415 (10.5) 21,673 (10.0) <0.001
Chronic lung disease 68,879 (12.8) 34,252 (15.9) <0.001
Dyslipidemia 430,948 (79.9) 165,024 (76.5) <0.001
Prior PCI 173,885 (32.2) 55,841 (25.9) <0.001
Prior CHF 39,608 (7.3) 10,402 (4.8) <0.001
FIGURE 2 Tempor
Patients With Stable
Elective PCI During
There was a significa
BB ¼ b-blocker; oth
Motivala et al. J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 9 , N O . 1 6 , 2 0 1 6
b-Blockers Following Elective PCI for Stable Angina A U G U S T 2 2 , 2 0 1 6 : 1 6 3 9 – 4 8
1642
outcomes with/without b-blocker usage were evalu-ated in patients $65 years of age using CMS-linkeddata containing 122,734 patients from 1,032 sites be-tween January 1, 2005, and December 31, 2009(Figure 1).
The baseline characteristics of the entire studycohort are shown in Table 1. A majority (71.4%) of ourpopulation cohort was discharged on b-blockers. Themean age of the overall population was 65.5 � 11.1years, 64.3% were male, 85.1% were Caucasian withmean body mass index of 30.3 � 6.5 kg/m2. Relatively,there were higher proportions of patients from thesouthern region (39.4%) and urban areas (58.7%).
Patients discharged on b-blockers were younger,more likely to be female and more likely to havehistory of hypertension, diabetes, dyslipidemia,smoking, dialysis, prior PCI, and prior and current HF.They were also more likely to have a higher bodymass index, higher New York Heart Associationfunctional class on presentation, ACC/AHA type Clesions on angiography, undergone multivessel PCI,acute PCI complications, and undergone urgent PCI.Patients discharged on b-blockers were less likely tohave chronic lung disease (Table 1).
TEMPORAL TRENDS OF PRESCRIPTION OF b-BLOCKERS
AT DISCHARGE. During the period between 2005 and2013, there was a gradual increase in prescription of
al Trends of BB Prescriptions at Discharge in Overall Cohort of
Angina Without Prior History of MI or Systolic HF Undergoing
the Period of 2005 to 2013
nt increase in the prescription rate over the time (p < 0.001).
er abbreviations as in Figure 1.
b-blockers at the index discharge in our cohort(Figure 2). This trend was similarly observed in allsubgroups. Despite the overall increase in the usagein all subgroups, there was a consistent difference inusage according to age, gender, history of diabetesmellitus, or multivessel PCI (p < 0.01) (Figure 3).
PREDICTORS AFFECTING PRESCRIPTIONS OF b-BLOCKERS
AT DISCHARGE. Certain patient and procedure specificfactors were associated with b-blocker prescription at
Current CHF 19,095 (6.6) 5,639 (4.7) <0.001
HF within 2 weeks 16,688 (6.7) 4,365 (4.6) <0.001
NYHA functional class <0.001
I 143,090 (49.2) 61,971 (51.1)
II 107,291 (36.9) 45,508 (37.5)
III 32,776 (11.3) 11,622 (9.6)
IV 7,833 (2.7) 2,114 (1.7)
EF 58.3 � 8.0 59.1 � 7.5 <0.001
Hospital region <0.001
Northeast 91,290 (16.9) 24,942 (11.6)
South 199,572 (37.0) 97,474 (45.2)
Midwest 165,317 (30.7) 57,780 (26.8)
West 82,964 (15.4) 35,280 (16.4)
Hospital setting <0.001
Rural 58,261 (10.8) 23,480 (10.9)
Suburban 162,973 (30.2) 67,097 (31.1)
Urban 318,287 (59.0) 125,117 (58.0)
Multivessel PCI 76,214 (14.1) 28,092 (13.0) <0.001
ACC/AHA type Clesions
203,159 (37.7) 75,357 (35.0) <0.001
Procedure success(excludingsame day death)
510,732 (96.1) 205,527 (96.5) <0.001
General complications(excludingsame day death)
11,584 (2.1) 2,949 (1.4) <0.001
Values are mean � SD or n (%).
ACC/AHA ¼ American College of Cardiology/American Heart Association; CHF ¼congestive heart failure; EF ¼ ejection fraction; MI ¼ myocardial infarction;NYHA ¼ New York Heart Association; PCI ¼ percutaneous coronary intervention.

FIGURE 3 Temporal Trends of BB Prescriptions at Discharge in Pre-Defined Subpopulation of Patients With Stable Angina Without Prior
History of MI or Systolic HF Undergoing Elective PCI During the Period of 2005 to 2013
There was a significant increase in the prescription rate over the time in all subgroups (p < 0.001 for all plots). BB ¼ b-blocker; other
abbreviations as in Figure 1.
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 9 , N O . 1 6 , 2 0 1 6 Motivala et al.A U G U S T 2 2 , 2 0 1 6 : 1 6 3 9 – 4 8 b-Blockers Following Elective PCI for Stable Angina
1643
discharge. The strongest predictors of b-blocker pre-scriptions at discharge were hypertension, prior PCI,lack of chronic lung disease, higher LVEF values, andprior congestive HF (Table 2).
SHORT-TERM (30-DAY) OUTCOMES. Among patients $65years of age with CMS linkage data available (16.3% ofthe studied population), the adjusted mortality ratewas similar between patients discharged with andwithout b-blockers (Figure 4A). There were no dif-ferences in adjusted rates of hospitalization related toMI, hospitalization related to stroke or revasculari-zation. Discharge on b-blockers was associated withmore post-discharge re-hospitalization related to HF(unadjusted: 0.9% vs. 0.4%; adjusted HR: 1.70; 95%
CI: 1.43 to 2.02; p < 0.001). A separate analysis per-formed including patients only with stable angina as apresenting symptom showed similar results except nodifferences in hospitalization related to HF (unad-justed: 0.6% vs. 0.4%; adjusted HR: 1.34; 95% CI:0.999 to 1.81; p < 0.051).
LONG-TERM (3-YEAR) OUTCOMES. At 3-year of follow-up among patients $65 years of age with CMS link-age data available (16.3% of the studied population),the unadjusted crude mortality rate was 13.8%. Therewas no difference in adjusted rates of mortality,hospitalization related to MI, and hospitalizationrelated to stroke or revascularization between pa-tients discharged with and without b-blockers

TABLE 2 Predictors Affecting b-Blocker Prescriptions at Discharge
Odds Ratio (95% CI) Chi-Square p Value
Hypertension 1.65 (1.62–1.68) 2375.02 <0.001
Prior PCI 1.39 (1.37–1.42) 1313.03 <0.001
Chronic lung disease 0.74 (0.73–0.76) 858.88 <0.001
HDEF (per 5-U when <60) 0.90 (0.9–0.91) 758.37 <0.001
Prior CHF 1.42 (1.38–1.46) 627.22 <0.001
PCI status
Urgent (vs. elective) 1.31 (1.28–1.35) 569.88 <0.001
Emergency (vs. elective) 1.91 (1.75–2.08)
4 (vs. elective) 1.47 (1–2.14)
Male 0.90 (0.88–0.9) 297.31 <0.001
GFR (per 5-U when <70 ml/min) 0.97 (0.97–0.97) 270.85 <0.001
Age (per 5-yr when <65 yrs) 0.96 (0.96–0.97) 245.79 <0.001
Pre-/in-procedure aspirin 1.19 (1.16–1.22) 212.03 <0.001
Hospital region
Northeast (vs. West) 1.50 (1.31–1.71) 144.21 <0.001
South (vs. West) 0.78 (0.71–0.85)
Midwest (vs. West) 1.09 (0.99–1.2)
BMI per 5-U (when <30 kg/m2) 1.06 (1.05–1.08) 139.36 <0.001
Any general complication 1.37 (1.3–1.45) 131.20 <0.001
Admission symptoms
Stable angina (vs. no symptoms/no angina) 1.11 (1.09–1.13) 120.62 <0.001
Atypical chest pain(vs. no symptoms/no angina)
1.04 (1.02–1.07)
Procedure year 1.04 (1.03–1.05) 103.76 <0.001
Race
Other (vs. White) 1.08 (1.05–1.12) 92.49 <0.001
African American (vs. White) 1.14 (1.1–1.17)
Hispanic (vs. White) 1.06 (1.01–1.12)
Pre-procedural TIMI flow 0.94 (0.92–0.95) 62.43 <0.001
Intervened vessels
CIRC (vs. RCA) 1.05 (1.04–1.07) 59.36 <0.001
LMA (vs. RCA) 1.13 (1.04–1.22)
BMI ¼ body mass index; CI ¼ confidence interval; CIRC ¼ left circumflex artery; GFR ¼ glomerular filtration rate;HDEF ¼ hemodynamic data ejection fraction; LMA ¼ left main artery; OR ¼ odds ratio; RCA ¼ right coronaryartery; Sx ¼ symptoms; TIMI ¼ Thrombolysis In Myocardial Infarction; other abbreviations as in Table 1.
Motivala et al. J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 9 , N O . 1 6 , 2 0 1 6
b-Blockers Following Elective PCI for Stable Angina A U G U S T 2 2 , 2 0 1 6 : 1 6 3 9 – 4 8
1644
(Figures 4B and 5). However, rates of hospitalizationrelated to HF were higher in patients dischargedon b-blockers. (Adjusted HR: 1.18; 95% CI: 1.12 to1.25; p < 0.001). Similar results were found whenpatients only with stable angina as a presentingsymptom were analyzed separately. These findingsremain essentially unchanged with/without adjustingfor discharge meds (antiplatelets, angiotensin-converting enzyme inhibitors/angiotensin receptorblockers, statins), with a slightly higher incidence(0.3%) of strokes on long-term follow-up of patients’discharged on b-blockers versus those withoutb-blockers.
DISCUSSION
The principal finding of this observational analysisfrom the NCDR CathPCI registry is that b-blocker use
at discharge among patients $65 years of age withCMS linkage data available (16.3% of the studiedpopulation) with stable angina without prior MI, LVsystolic dysfunction (LVEF <40%), or systolic HFundergoing elective PCI was not associated witha reduction in post-discharge mortality, revasculari-zation or re-hospitalization related to MI or strokeat 30-day and 3-year follow-up. Prescriptions ofb-blockers at discharge in this population were asso-ciated with specific patient and procedural charac-teristics, and have increased over the 8-year studyperiod.
The ACC/AHA guidelines strongly recommend b-blockers in patients with prior MI and/or systolic HFto decrease mortality and cardiovascular morbidity(7,27). Postulated mechanisms of the beneficial ef-fects of b-blockers include a decrease in oxygenrequirement and ischemia due to negative inotropicand chronotropic effects, decrease in LV wall stress,decrease in ventricular arrhythmias, and reduced LVremodeling (28–31). Based on these hypotheses, ithas been speculated that the prognostic benefits ofb-blockers would extend to the population of CADpatients with stable angina, even without priorhistory of MI or systolic HF. Due to findings fromCOURAGE trial and other studies, b-blockers remainan essential ingredient of optimal medical therapyfor patients with stable angina (3,8,9,21,32). How-ever, the evidence supporting the benefits of b-blockers in stable CAD patients without prior MI orsystolic HF undergoing elective PCI, especially inthe era of contemporary medical therapy, remainsscarce. There are no randomized control trialsaddressing this issue directly, and previous non-randomized observational studies are limited withsmaller size and/or varied inclusion criteria(10,13,14,33).
This lack of improvement in outcomes associatedwith b-blocker use at discharge among a small subsetof stable angina patients $65 years of age undergoingelective PCI are not surprising and remain broadlyconsistent with other recently reported analyses(10,13,14,33). To our knowledge, only 1 study hasinvestigated this particular question in this specificsubset of stable angina patients undergoing PCI. Inthe observational study done by Ozasa et al. (33),which included 5,288 Japanese patients with stableangina without prior MI or HF undergoing an electivePCI, higher incidence of adverse cardiac events wasnoted in b-blocker group (event rate: 4.9% vs. 3.4%;p ¼ 0.02). This difference may, in part, be explainedby a relatively large proportion of patients not onoptimal medical therapy, and relatively smallersample size of their study.

FIGURE 4 Adjusted HR of Cardiovascular Outcomes at 30-Day and 3-Year Interval
There was no significant difference in (A) short (30 days) and (B) long-term (3 years)
outcomes except HF-related hospitalization. HF-related hospitalization was significantly
higher in patients discharged with b-blocker. Confidence interval is 95%. BB ¼ b-blocker;
Ds ¼ discharge; HR ¼ hazard ratio; LCL ¼ lower confidence limit; UCL ¼ upper confidence
limit; other abbreviations as in Figure 1.
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 9 , N O . 1 6 , 2 0 1 6 Motivala et al.A U G U S T 2 2 , 2 0 1 6 : 1 6 3 9 – 4 8 b-Blockers Following Elective PCI for Stable Angina
1645
This apparent lack of efficacy of b-blockers in thisparticular subset of patients appears counter-intuitive, and may be attributable to multiple rea-sons. As previously demonstrated by the CAFÉ(Conduit Artery Functional End Point) trial in-vestigators, pharmacologically induced bradycardiawith b-blockers leads to increased central aorticpressure with consequently worse cardiovascularoutcomes (34). These agents are also poor atachieving optimal control of essential hypertension,resulting in a downgrade of their role as a first lineagent in current hypertension guidelines (35–37). Useof b-blockers has also been associated with worseninglipid profiles and new onset diabetes (38–40).Nonselective b-blockers inhibit adrenergically medi-ated coronary vasodilatation, potentially causingunstable angina due to coronary spasm (41).Furthermore, prolonged use of b-blockers is associ-ated with up-regulation of b-receptors and theirabrupt de-escalation or discontinuation, which mayresult from poor tolerability or lack of compliance;may potentially cause harm (42–46). Also, thefundamentally different pathophysiology of acutecoronary syndrome from stable angina may accountfor failure to replicate the beneficial prognostic out-comes of b-blockers in this population, especially af-ter revascularization (47). It should be noted thatmuch like b-blockers, PCI in stable angina also doesnot confer a survival benefit.
A possible counterview to this assessment is that b-blockers may have provided relative benefit to thesepatients. The patients prescribed with b-blockers hadhigher prevalence of traditional risk factors (Table 1)for atherosclerotic cardiac events and despite thatthere was no significant increase in mortality andmorbidity observed. There is a probability that thesepatients may have had higher event rates if they werenot prescribed b-blockers. It is possible that b-blockers provide beneficial effects, but the magnitudemay be less compared to following an acute coronarysyndrome.
Nevertheless, b-blockers have consistently beenshown to decrease angina frequency, increase exer-cise duration and reduce ischemic burden in patientswith stable angina who are partially revascularized(15,16). A reduction in residual ischemic burden inpartially revascularized patients has shown toimprove subsequent outcomes (48). Based on this, b-blockers are recommended as a first line agent todecrease angina frequency (17) and are considered anintegral component of optimal medical therapy forthese patients. Because the proportion of partiallyrevascularized patients in our cohort is unknown,whether b-blocker use in this subset improves
outcomes remains unclear. However, based on ourfindings along with others, among patients with sta-ble angina who are completely revascularized, long-term continuation of b-blocker therapy could have asignificant impact on their subsequent quality of life(e.g., fatigue, exercise intolerance, lethargy, impo-tence) and their routine use should be discouraged infuture guidelines.
We observed an increased incidence of HF read-missions among patients with b-blocker use in ourstudy. The mechanism of this association and po-tential for harm is unclear. While patients with sys-tolic HF, or LVEF <40%, were excluded from our

FIGURE 5 Unadjusted Incidence of Cardiovascular Outcomes Associated With BB
Prescriptions at Different Time Intervals
There was no difference in primary outcomes except HF-related admissions. HF-related
readmission were noted to be higher in patients discharged with BB (at 3-year follow-up,
unadjusted hazard ratio: 1.37; 95% confidence interval: 1.30 to 1.45; p < 0.001). BB ¼b-blocker; other abbreviations as in Figure 1.
Motivala et al. J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 9 , N O . 1 6 , 2 0 1 6
b-Blockers Following Elective PCI for Stable Angina A U G U S T 2 2 , 2 0 1 6 : 1 6 3 9 – 4 8
1646
analysis, patients with prior HF and LVEF >40%were likely to be included. Although we adjusted forprior HF, LVEF, and New York Heart Associationfunctional class using multivariate analysis, residualconfounding factors along with retrospective obser-vational nature of our study limits our ability tofurther explain the association between b-blockeruse and HF readmission. In the REACH (Reduction ofAtherothrombosis for Continued Health) registry, inpatients with CAD without prior MI, b-blocker usewas associated with an increased risk of hospitali-zation for atherothrombotic events or a revasculari-zation procedure (odds ratio: 1.17; 95% CI: 1.04 to 1.30;p ¼ 0.01) (10). HF, however, was not assessed in that
analysis. Due to the implications of these findings,randomized studies with adjudicated outcomes maybe warranted but would be difficult to perform dueto the highly selected nature of the population. Theuse of b-blockers at discharge has been steadilyincreasing overall in this population and in all pre-defined subgroups of patients with stable angina.This increased use may be related to physicians’belief, though not evidence based, that b-blockersare cardioprotective in CAD patients even in theabsence of prior MI. More likely, it is a marker of anincreasing emphasis on adherence to guidelinesbased therapies and requirement of optimal medicaltherapy prior to PCI in the appropriate use criteriaas well as b-blocker therapy at discharge beingregarded as an important quality metric among thispopulation by the Joint Commission, the NationalCommittee for Quality Assurance, and other organi-zations. In many cases, b-blocker use may be solelyfor antianginal benefit similar to nitrates andcalcium-channel blockers.
STUDY LIMITATIONS. Before considering applica-bility of the results of our study, certain importantlimitations should be kept in mind. First, our studypopulation comprised of 16.7 % of the overall NCDRpopulation and may be not representative of the allpatients enrolled in NCDR. However, it comprised of afairly large number of patients with stable anginaundergoing percutaneous revascularization and re-mains broadly representative of real world practiceand outcomes across a variety of hospitals within theUnited States. Second, our data only analyzedpatients $65 years of age with CMS linkage dataavailable (16.3% of the studied population), for post-discharge outcomes. Thus our outcomes data cannotbe extrapolated to younger patients, or the majorityof patients that did not have linkage to the CMSdatabase for post-discharge outcomes, based on thisstudy. Third, we did not have access to drug claimsdata and thus our data could not account for lackof compliance, use of suboptimal dosing, type ofb-blocker, and changes in b-blocker use pattern overtime (along with the use of other post-dischargeantianginals and other medications). This precludesus from ascertaining how actual treatment andcompliance may have influenced the results. Fourth,our dataset did not have information of anginafrequency and severity. However, to what extentb-blockers can continue to supplement antianginaleffects of PCI is not entirely clear. Last, despite of ourbest attempts to adjust for many confounding factors,we cannot control for residual confounding resultingfrom imperfectly collected or missing confounders.

PERSPECTIVES
WHAT IS KNOWN? b-blockers have consistently been shown
to improve outcomes in a variety of cardiovascular settings and
therefore remain widely used.
WHAT IS NEW? This nonrandomized, observational study re-
ports that b-blocker use at discharge among patients $65 years
of age with stable angina without prior MI, LV systolic dysfunc-
tion (LVEF <40%), or systolic HF undergoing elective PCI in
routine clinical practice was associated with no difference in
post-discharge mortality, revascularization, or rehospitalization
related to MI or stroke at 30-day and at 3-year follow-up. Their
prescriptions at discharge continue to trend upward with time.
WHAT IS NEXT? The use of b-blockers in this population
should be tailored based on other concomitant cardiovascular
conditions and completeness of revascularization.
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 9 , N O . 1 6 , 2 0 1 6 Motivala et al.A U G U S T 2 2 , 2 0 1 6 : 1 6 3 9 – 4 8 b-Blockers Following Elective PCI for Stable Angina
1647
However, it should be noted that a feature of theNCDR’s commitment to quality data is their NationalOn-Site Audit Program. Annually, participants arerandomly selected for an on-site audit. Followingthe audit, each site receives a detailed report oftheir audit findings to assist with data collectionimprovements.
CONCLUSIONS
This nonrandomized, observational study reportsthat b-blocker use at discharge among patients $65years of age with stable angina without prior MI, LVsystolic dysfunction (LVEF <40%), or systolic HFundergoing elective PCI in routine clinical practicewas associated with no difference in post-dischargemortality, revascularization, or rehospitalizationrelated to MI or stroke at 30-day and at 3-year follow-up. b-blocker use at discharge in these patientsincreased over time, and was preferentially used forpatients with prior/current HF and hypertension.These findings are in concordance with recent litera-ture and suggest no survival benefit with the use ofb-blockers in stable angina patients post PCI.
Notwithstanding the widespread use of b-blockersfor the treatment of hypertension and for anginacontrol among patients with stable angina, our resultsdemonstrate no difference in cardiovascular out-comes with the use of b-blocker after elective PCI inroutine clinical practice. These hypothesis-generatingfindings highlight patient features associated withthe use of b-blockers such as hypertension and
prior/current HF that often track with symptomaticcoronary artery disease that prompts elective PCI, andsuggest that the use of b-blockers in this popula-tion should be customized based on other concomi-tant cardiovascular conditions and completeness ofrevascularization.
REPRINT REQUESTS AND CORRESPONDENCE: Dr.Valay Parikh, Department of Cardiovascular Medi-cine, Staten Island University Hospital, Staten Island,New York 10305. E-mail: [email protected].
RE F E RENCE S
1. Teo KK, Yusuf S, Furberg CD. Effects of pro-phylactic antiarrhythmic drug therapy in acutemyocardial infarction. An overview of results fromrandomized controlled trials. JAMA 1993;270:1589–95.
2. Effect of metoprolol CR/XL in chronic heartfailure: Metoprolol CR/XL Randomised Interven-tion Trial in Congestive Heart Failure (MERIT-HF).Lancet 1999;353:2001–7.
3. Freemantle N, Cleland J, Young P, Mason J,Harrison J. beta Blockade after myocardial infarc-tion: systematic review and meta regressionanalysis. BMJ 1999;318:1730–7.
4. Silvet H, Spencer F, Yarzebski J, Lessard D,Gore JM, Goldberg RJ. Communitywide trends inthe use and outcomes associated with beta-blockers in patients with acute myocardial infarc-tion: the Worcester Heart Attack Study. ArchIntern Med 2003;163:2175–83.
5. Anderson JL, Adams CD, Antman EM, et al. 2012ACCF/AHA focused update incorporated into theACCF/AHA 2007 guidelines for the managementof patients with unstable angina/non-ST-elevation
myocardial infarction: a report of the AmericanCollege of Cardiology Foundation/American HeartAssociation Task Force on Practice Guidelines.J Am Coll Cardiol 2013;61:e179–347.
6. O’Gara PT, Kushner FG, Ascheim DD, et al. 2013ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of theAmerican College of Cardiology Foundation/American Heart Association Task Force on PracticeGuidelines. J Am Coll Cardiol 2013;61:e78–140.
7. Yancy CW, Jessup M, Bozkurt B, et al. 2013ACCF/AHA guideline for the management of heartfailure: executive summary: a report of theAmerican College of Cardiology Foundation/American Heart Association Task Force on practiceguidelines. Circulation 2013;128:1810–52.
8. Aronow WS, Ahn C, Kronzon I. Effect of propran-olol versus no propranolol on total mortality plusnonfatal myocardial infarction in older patients withprior myocardial infarction, congestive heart failure,and left ventricular ejection fraction > or ¼ 40%treated with diuretics plus angiotensin-convertingenzyme inhibitors. Am J Cardiol 1997;80:207–9.
9. Hippisley-Cox J, Coupland C. Effect of combi-nations of drugs on all cause mortality in patientswith ischaemic heart disease: nested case-controlanalysis. BMJ 2005;330:1059–63.
10. Bangalore S, Steg G, Deedwania P, et al. beta-Blocker use and clinical outcomes in stable out-patients with and without coronary artery disease.JAMA 2012;308:1340–9.
11. Huang HL, Fox KA. The impact of beta-blockerson mortality in stable angina: a meta-analysis.Scott Med J 2012;57:69–75.
12. Shu de F, Dong BR, Lin XF, Wu TX, Liu GJ.Long-term beta blockers for stable angina: sys-tematic review and meta-analysis. Eur J PrevCardiol 2012;19:330–41.
13. Andersson C, Shilane D, Go AS, et al. beta-blocker therapy and cardiac events amongpatients with newly diagnosed coronary heartdisease. J Am Coll Cardiol 2014;64:247–52.
14. Bangalore S, Bhatt DL, Steg PG, et al. Beta-blockers and cardiovascular events in patientswith and without myocardial infarction: post hoc

Motivala et al. J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 9 , N O . 1 6 , 2 0 1 6
b-Blockers Following Elective PCI for Stable Angina A U G U S T 2 2 , 2 0 1 6 : 1 6 3 9 – 4 8
1648
analysis from the CHARISMA trial. Circ CardiovascQual Outcomes 2014;7:872–81.
15. Savonitto S, Ardissiono D, Egstrup K, et al.Combination therapy with metoprolol and nifedi-pine versus monotherapy in patients with stableangina pectoris. Results of the InternationalMulticenter Angina Exercise (IMAGE) Study. J AmColl Cardiol 1996;27:311–6.
16. Weiss R, Ferry D, Pickering E, et al. Effective-ness of three different doses of carvedilol for ex-ertional angina. Carvedilol-Angina Study Group.Am J Cardiol 1998;82:927–31.
17. Fihn SD, Gardin JM, Abrams J, et al. 2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for thediagnosis and management of patients with stableischemic heart disease: a report of the AmericanCollege of Cardiology Foundation/American HeartAssociationTaskForceonPracticeGuidelines, and theAmericanCollegeof Physicians, AmericanAssociationfor Thoracic Surgery, Preventive CardiovascularNurses Association, Society for Cardiovascular Angi-ography and Interventions, and Society of ThoracicSurgeons. J Am Coll Cardiol 2012;60:e44–164.
18. Chobanian AV, Bakris GL, Black HR, et al. TheSeventh Report of the Joint National Committeeon Prevention, Detection, Evaluation, and Treat-ment of High Blood Pressure: the JNC 7 report.JAMA 2003;289:2560–72.
19. Gu Q, Paulose-Ram R, Dillon C, Burt V. Anti-hypertensive medication use among US adultswith hypertension. Circulation 2006;113:213–21.
20. MehtaSS,WilcoxCS, SchulmanKA.Treatmentofhypertension in patients with comorbidities: resultsfrom the study of hypertensive prescribing practices(SHyPP). Am J. Hypertens 1999;12:333–40.
21. Boden WE, O’Rourke RA, Teo KK, et al. Optimalmedical therapy with or without PCI for stablecoronary disease. N Engl J Med 2007;356:1503–16.
22. Frye RL, August P, Brooks MM, et al.A randomized trial of therapies for type 2 diabetesand coronary artery disease. N Engl J Med 2009;360:2503–15.
23. Sedlis SP, Hartigan PM, Teo KK, et al. Effect ofPCI on long-term survival in patients with stableischemic heart disease. N Engl J Med 2015;373:1937–46.
24. Douglas PS, Brennan JM, Anstrom KJ, et al.Clinical effectiveness of coronary stents in elderlypersons: results from 262,700 Medicare patientsin the American College of Cardiology-NationalCardiovascular Data Registry. J Am Coll Cardiol2009;53:1629–41.
25. Hammill BG, Hernandez AF, Peterson ED,Fonarow GC, Schulman KA, Curtis LH. Linkinginpatient clinical registry data to Medicare claimsdata using indirect identifiers. Am Heart J 2009;157:995–1000.
26. Gray RJ. A class of K-sample tests for com-paring the cumulative incidence of a competingrisk. Ann Stat 1988;16:1141–54.
27. Smith SC Jr., Benjamin EJ, Bonow RO, et al.AHA/ACCF Secondary Prevention and Risk Reduc-tion Therapy for Patients with Coronary and otherAtherosclerotic Vascular Disease: 2011 update: aguideline from the American Heart Association andAmerican College of Cardiology Foundation. Cir-culation 2011;124:2458–73.
28. Ryden L, Ariniego R, Arnman K, et al.A double-blind trial of metoprolol in acutemyocardial infarction. Effects on ventriculartachyarrhythmias. N Engl J Med 1983;308:614–8.
29. Friedman LM, Byington RP, Capone RJ,Furberg CD, Goldstein S, Lichstein E. Effect ofpropranolol in patients with myocardial infarctionand ventricular arrhythmia. J Am Coll Cardiol1986;7:1–8.
30. Nuttall SL, Toescu V, Kendall MJ. betaBlockade after myocardial infarction. Betablockers have key role in reducing morbidity andmortality after infarction. BMJ 2000;320:581.
31. Lopez-Sendon J, Swedberg K, McMurray J,et al. Expert consensus document on beta-adrenergic receptor blockers. Eur Heart J 2004;25:1341–62.
32. Yusuf S, Peto R, Lewis J, Collins R, Sleight P.Beta blockade during and after myocardialinfarction: an overview of the randomized trials.Prog Cardiovasc Dis 1985;27:335–71.
33. Ozasa N, Morimoto T, Bao B, et al. beta-blocker use in patients after percutaneouscoronary interventions: one size fits all? Worseoutcomes in patients without myocardial infarc-tion or heart failure. Int J Cardiol 2013;168:774–9.
34. Williams B, Lacy PS, Thom SM, et al. Differ-ential impact of blood pressure-lowering drugs oncentral aortic pressure and clinical outcomes:principal results of the Conduit Artery FunctionEvaluation (CAFE) study. Circulation 2006;113:1213–25.
35. Mancia G, Fagard R, Narkiewicz K, et al. 2013ESH/ESC Guidelines for the management of arte-rial hypertension: the Task Force for the man-agement of arterial hypertension of the EuropeanSociety of Hypertension (ESH) and of the Euro-pean Society of Cardiology (ESC). J Hypertens2013;31:1281–357.
36. James PA, Oparil S, Carter BL, Cushman WC,Dennison-Himmelfarb C, Handler J, et al. 2014evidence-based guideline for the management ofhigh blood pressure in adults: report from thepanel members appointed to the Eighth JointNational Committee (JNC 8). JAMA 2014;311:507–20.
37. Weber MA, Schiffrin EL, White WB, et al.Clinical practice guidelines for the management ofhypertension in the community a statement by theamerican society of hypertension and the inter-national society of hypertension. J Hypertens2014;32:3–15.
38. Weir MR, Moser M. Diuretics and beta-blockers: is there a risk for dyslipidemia? AmHeart J 2000;139:174–83.
39. Bangalore S, Parkar S, Grossman E,Messerli FH. A meta-analysis of 94,492 patientswith hypertension treated with beta blockers todetermine the risk of new-onset diabetes mellitus.Am J Cardiol 2007;100:1254–62.
40. Elliott WJ, Meyer PM. Incident diabetes inclinical trials of antihypertensive drugs: a networkmeta-analysis. Lancet 2007;369:201–7.
41. Japanese beta-Blockers and Calcium Antag-onists Myocardial Infarction (JBCMI) In-vestigators. Comparison of the effects of betablockers and calcium antagonists on cardiovas-cular events after acute myocardial infarction inJapanese subjects. Am J Cardiol 2004;93:969–73.
42. Miller RR, Olson HG, Amsterdam EA,Mason DT. Propranolol-withdrawal rebound phe-nomenon. Exacerbation of coronary events afterabrupt cessation of antianginal therapy. N Engl JMed 1975;293:416–8.
43. Houston MC. Abrupt cessation of treatment inhypertension: consideration of clinical features,mechanisms, prevention and management of thediscontinuation syndrome. Am Heart J 1981;102 3Pt 1:415–30.
44. Psaty BM, Koepsell TD, Wagner EH,LoGerfo JP, Inui TS. The relative risk of incidentcoronary heart disease associated with recentlystopping the use of beta-blockers. JAMA 1990;263:1653–7.
45. Bradley HA, Wiysonge CS, Volmink JA,Mayosi BM, Opie LH. How strong is the evidencefor use of beta-blockers as first-line therapy forhypertension? Systematic review and meta-anal-ysis. J Hypertens 2006;24:2131–41.
46. Heilbrunn SM, Shah P, Bristow MR,Valantine HA, Ginsburg R, Fowler MB. Increasedbeta-receptor density and improved hemodynamicresponse to catecholamine stimulation duringlong-term metoprolol therapy in heart failurefrom dilated cardiomyopathy. Circulation 1989;79:483–90.
47. Fuster V, Badimon L, Badimon JJ,Chesebro JH. The pathogenesis of coronary arterydisease and the acute coronary syndromes (1).N Engl J Med 1992;326:242–50.
48. Shaw LJ, Berman DS, Maron DJ, et al. Optimalmedical therapy with or without percutaneouscoronary intervention to reduce ischemic burden:results from the Clinical Outcomes UtilizingRevascularization and Aggressive Drug Evaluation(COURAGE) trial nuclear substudy. Circulation2008;117:1283–91.
KEY WORDS b-blockers, percutaneouscoronary intervention, stable angina
APPENDIX For a supplemental table, pleasesee the online version of this article.