Embed Size (px)
Citation preview

Listen to this manuscript’s
audio summary by
Editor-in-Chief
Dr. Valentin Fuster on
JACC.org.
J O U R N A L O F T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y V O L . 7 2 , N O . 2 4 , 2 0 1 8
ª 2 0 1 8 B Y T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y F O UN DA T I O N
P U B L I S H E D B Y E L S E V I E R
JACC STATE-OF-THE-ART REVIEW
Idiopathic/IatrogenicLeft Bundle Branch Block–InducedReversible Left Ventricle Dysfunction
JACC State-of-the-Art ReviewVincent Auffret, MD,a,b,c Raphaël P. Martins, MD, PHD,a,b,c Claude Daubert, MD,b,c Christophe Leclercq, MD, PHD,a,b
Hervé Le Breton, MD,a,b,c Philippe Mabo, MD,a,b,c Erwan Donal, MD, PHDa,b,c
ABSTRACT
ISS
Fro
Re
the
Ma
Idiopathic or iatrogenic left bundle branch block (LBBB) is a unique model of electro-mechanical ventricular dyssynchrony
with concordant changes in electrical activation sequence and mechanical ventricle synchronization. In chronic animal
models, isolated LBBB induces structural remodeling with progressive left ventricular (LV) dysfunction. Most abnor-
malities can be reverted after cardiac resynchronization therapy (CRT). In humans, 2 principal models of LBBB dys-
synchronopathy can be observed: the chronic model of isolated LBBB and an acute iatrogenic model of new-onset LBBB
after aortic valve interventions. Although epidemiological evidence and clinical data need to be strengthened, there is a
strong presumption that they may lead to LBBB-induced cardiomyopathy and benefit from CRT to prevent progression to
heart failure. A large cohort study with prospective follow-up would be required to better define actual incidence,
evolution over time, and predisposing factors. Parallel randomized CRT clinical trials should be conducted in
selected at-risk populations: namely, patients with persistent LBBB after transcatheter aortic valve replacement.
(J Am Coll Cardiol 2018;72:3177–88) © 2018 by the American College of Cardiology Foundation.
A lthough rare in the general population(<1%), left bundle branch block (LBBB) hasalways aroused a keen interest among cardi-
ologists (1). Being a unique model of ventricularelectromechanical dyssynchrony, LBBB was sus-pected to generate structural remodeling, leftventricular (LV) dysfunction, and—eventually—heartfailure (HF) and to associate with worse prognosis.Data from animal models (2,3) and clinical observa-tions in humans (4,5) support the existence ofLBBB-induced cardiomyopathy (LBBB-CM), poten-tially reversible by cardiac resynchronization ther-apy (CRT), leading to discuss preventive CRTindications in some categories of patients withLBBB. Two clinical situations can reproduce theexperimental model of LBBB-dyssynchronopathy
N 0735-1097/$36.00
m the aUniversité de Rennes1-Faculté de Médecine, Rennes, France; bSer
nnes, France; and cLTSI-INSERM U1099, Rennes, France. All authors have
contents of this paper to disclose.
nuscript received June 16, 2018; revised manuscript received August 22,
and be potential indications for preventive CRT:the chronic situation of isolated LBBB on presumedhealthy hearts and the acute iatrogenic situation ofnew LBBB, mainly after aortic valve interventions.In this paper, we discuss recent controversies inLBBB definition, the electromechanical substratefor LBBB dyssynchronopathy, the animal and humanmodels and their clinical consequences, and, finally,the potential role of CRT to prevent development of“true” LBBB-CM.
DEFINITION OF LBBB
Diagnostic criteria of LBBB have been previouslypublished in a recent expert consensus and thereforewill not be thoroughly discussed here (6).
https://doi.org/10.1016/j.jacc.2018.09.069
vice de Cardiologie, Centre Hospitalier Universitaire,
reported that they have no relationships relevant to
2018, accepted September 10, 2018.

ABBR EVA T I ON S
AND ACRONYMS
BVP = biventricular pacing
CMR = cardiac magnetic
resonance
CRT = cardiac
resynchronization therapy
ECG = electrocardiogram
HAVB = high degree
atrioventricular block
HF = heart failure
LBBB = left bundle branch
block
LBBB-CM = LBBB-induced
cardiomyopathy
LV = left ventricle
LVEF = left ventricular ejection
fraction
PPI = permanent pacemaker
implantation
RBBB = right bundle branch
block
RV = right ventricle
SAVR = surgical aortic valve
replacement
SHD = structural heart disease
TAVR = transcatheter aortic
valve replacement
Auffret et al. J A C C V O L . 7 2 , N O . 2 4 , 2 0 1 8
LBBB-Induced Left Ventricular Dysfunction D E C E M B E R 1 8 , 2 0 1 8 : 3 1 7 7 – 8 8
3178
Figure 1 depicts typical and atypical patternsof LBBB according to these criteria.
More recently, based on additional in-sights from computer simulations, Strausset al. (7) introduced stricter criteria fortypical LBBB, which remain of uncertainvalue in routine clinical practice, especiallyto refine selection of candidates for CRT.
LBBB: A UNIQUE MODEL OF
VENTRICULAR ELECTROMECHANICAL
DYSSYNCHRONY
ELECTRICAL DYSSYNCHRONY. LBBB-inducedchanges in the ventricular activationsequence have been extensively studied byendocardial catheter mapping (8–10) or morerecently by body surface electrocardiogram(ECG) mapping (11). Studies included patientswith isolated LBBB (8) or, more often, pa-tients with LBBB and structural heart disease(8). The most recent studies focused onpatients with HF who were candidates forCRT (9–11).
Contradictory results have been publishedregarding LV activation in patients withLBBB. Indeed, Auricchio et al. (9), usingendocardial 3-dimensional (3D) contact and
noncontact mapping, demonstrated a complex andheterogeneous LV activation pattern, with a U-sha-ped activation wavefront imposed on the LV activa-tion sequence by a transmural functional line of blocklocated between the LV septum and the lateral wallwith a prolonged activation time (LVAT). On thecontrary, using detailed 3D endocardial mapping andnoninvasive body surface electrocardiographic map-ping, Derval et al. (10) and Ploux et al. (11), respec-tively, demonstrated a more uniform pattern ofactivation with a delayed and homogeneous wave-front spreading in the LV from the septal to the lateralbasal region, without areas of conduction block(Figure 2). The inherent limitations of each mappingtechnique, in addition to the underlying myocardialsubstrate, may account for such discrepancies.
The activation pattern appears more homogeneousin patients with LBBB and without structural heartdisease (SHD) than in patients with myocardial pa-thology (9). Ventricular activation begins in the rightventricle (RV), usually in the septum. RV endocardialbreakthrough occurs a few milliseconds after surfaceQRS complex onset. The total RV activation time isshort: approximately 35 m. Transseptal LV activationlasts on average 30 to 40 ms. Most patients have only1 site of LV endocardial breakthrough, located in the
LV mid-septum. When multiple sites are identified, 1is located at the mid or lower LV septum. In mostcases, the latest activation site is the basal LV freewall in inferior, posterior, or lateral part (9). In iso-lated LBBB patients, the latest activation occurson average 125 ms after surface QRS complex onsetwith a mean LVAT of 80 ms. The intervals are muchlonger in patients with LBBB and SHD especially incase of coronary artery disease (CAD) with infarctscar. Briefly, LBBB is characterized by a significantprolongation of LVAT and a marked delay in theactivation of the basal LV free wall. From thebeginning to end, the LV activation sequence seemsto be quite homogeneous in patients with isolatedLBBB but much more heterogeneous in patients withLBBB and SHD.
MECHANICAL DYSSYNCHRONY, MYOCARDIAL FUNCTION,
PERFUSION. Abnormal septa l mot ion . In 1974, Dil-lon et al. (12) described by M-mode echocardiogra-phy a “specific abnormality characterized by ahighly dynamic posterior interventricular septalmovement occurring within 0.04 s of the onset ofQRS and preceding anterior movement of the pos-terior LV wall during ventricular ejection.” Thisleftward septal pre-ejectional shift, followed by aparadoxical movement to the right, differs widelyfrom the normal heart where the septum has mini-mal movement during pre-ejection and moves to theleft and toward the LV cavity center during ejection(13). The specific value of this abnormality wasdemonstrated in patients with intermittent LBBBwho all had normal wall motion and normal LVEFduring normal conduction but developed asynchro-nous LV deformation and abrupt decrease in LVEFat onset of LBBB (14).
Variants of the Dillon’s abnormality have beenlater described using new imaging technologies.Septal flash is an early septal thickening/thinningduring the isovolumic contraction period (Figure 3,Online Video 1) due to the septal contraction against areduced load, resulting in faster shortening thannormal (15). Apical rocking is a back-and-forth motionof the LV apex related to the mutual stretching ofopposing walls (16). These 2 simple approachesdescribe with great specificity the mechanical conse-quences of true LBBB. In some cases, the apicalrocking and/or the septal flash can be absent despitebroad QRS and typical LBBB: for instance, when theRV function is severely impaired.
To be more sensitive, longitudinal 2D-speckletracking echocardiography has been proposed fordescribing patterns of deformation and/or for quan-tifying these abnormalities (17). Recently, the

FIGURE 1 ECG Patterns of Left Bundle Branch Block
(A) Typical left bundle branch block with QRS duration ¼170 ms, broad notched or slurred R-wave in leads I; aVL; V5–V6; absent q waves in
leads I, aVL, V5–V6; and R peak time ¼ 80 ms in lead V6. (B) Atypical pattern with QS aspect in leads V1–V3, presence of deep S-wave in leads
V5–V6, and q wave in lead aVL. These signs are possibly related to QRS left-axis deviation (–60�)
J A C C V O L . 7 2 , N O . 2 4 , 2 0 1 8 Auffret et al.D E C E M B E R 1 8 , 2 0 1 8 : 3 1 7 7 – 8 8 LBBB-Induced Left Ventricular Dysfunction
3179
relevance of using the myocardial work to describeand quantify LBBB consequences has been demon-strated (18,19). A typical deformation pattern defining“true LBBB” was also described, combining 3 criteria:1) early shortening of $1 basal or mid-ventricularsegment in the septal wall and early stretching in$1 basal or midventricular segment in the lateralwall; 2) early septal peak shortening (within thefirst 70% of the ejection phase); and 3) lateral wallpeak shortening after aortic valve closure (20)(Figure 3).
Dyssynchrony cannot be limited to a systolicproblem. The delayed deformation of the lateral wallhas consequences on papillary muscles and mitralvalve apparatus kinetics (diastolic mitral regurgita-tion and increased tethering effect of mitral valveleaflets). It also affects diastole and LV filling (21).Most patients with the true LBBB pattern have afusion of E and A waves of the mitral inflow(Figure 3). This shortening of LV diastolic filling canhave severe hemodynamic consequences. Also, it
has been nicely demonstrated that in the presence ofa true LBBB, there is a thinning of the septum and athickening of the LV-lateral wall. The changes inregional function lead to changes in regional wallstress and consequently modify the LV regionalthickness (22).Myocard ia l perfus ion . Septal or anteroseptalperfusion defects are present on stress thalium-201SPECT in 70% to 100% of patients with LBBB andnormal coronary angiography (23,24). Cardiac posi-tron emission tomography (PET) studies have shownreverse mismatch in the septum, sometimesextended to the anterior and inferior walls, withmarkedly reduced glucose uptake but without corre-lating reduction in perfusion (25). Experimental datasuggest that this effect is primarily due to reducedoxygen demand, caused by the underlying electricalsubstrate, but also perfusion is impaired by theabnormal contraction, which augments intra-myocardial pressure and shortens the diastolic periodof coronary perfusion (24). Reduced coronary flow

FIGURE 2 Electrical Ventricular Dyssynchrony in Typical Left Bundle Branch Block
Epicardial ventricular activation sequence analyzed by body surface electrocardiogram mapping. Three views are shown: anteroposterior (AP),
left anterior oblique (LAO), and left lateral (LL). The wave front spreads from the right ventricle to the left with 2 lines of slow conduction:
the first oriented from the base to the apex at the septal level and the second limited to the first two-thirds of the anterolateral area. The
latest left ventricular activation site is at the lateral base. Adapted with permission from Ploux et al. (11).
Auffret et al. J A C C V O L . 7 2 , N O . 2 4 , 2 0 1 8
LBBB-Induced Left Ventricular Dysfunction D E C E M B E R 1 8 , 2 0 1 8 : 3 1 7 7 – 8 8
3180
reserve, suggesting microvascular dysfunction, wasalso observed (24). Anyway, patients with LBBBappear to have functional myocardial ischemia,which is likely to be involved in septal hypokinesia inaddition to the interstitial fibrosis.
ANIMAL MODELS OF
LBBB-INDUCED DYSSYNCHRONOPATHY
Most experiments were done on normal (2,26–28) orfailing (29) dog hearts with LBBB induced by radio-frequency ablation of the left bundle branch. No an-imal model of a chronic increase in afterload has beentested for the impact of LBBB.
In normal hearts, the main acute effects of newLBBB were doubling of QRS duration (28), markedinterventricular mechanical dyssynchrony, and pro-found hemodynamic changes: in particular, elevationof LV end-diastolic pressure and decrease in cardiacoutput (2,28).
This model was later used in chronic (16 weeks)experiments to investigate whether isolated LBBBmay cause ventricular remodeling and loss of LVpump function and whether abnormal septal
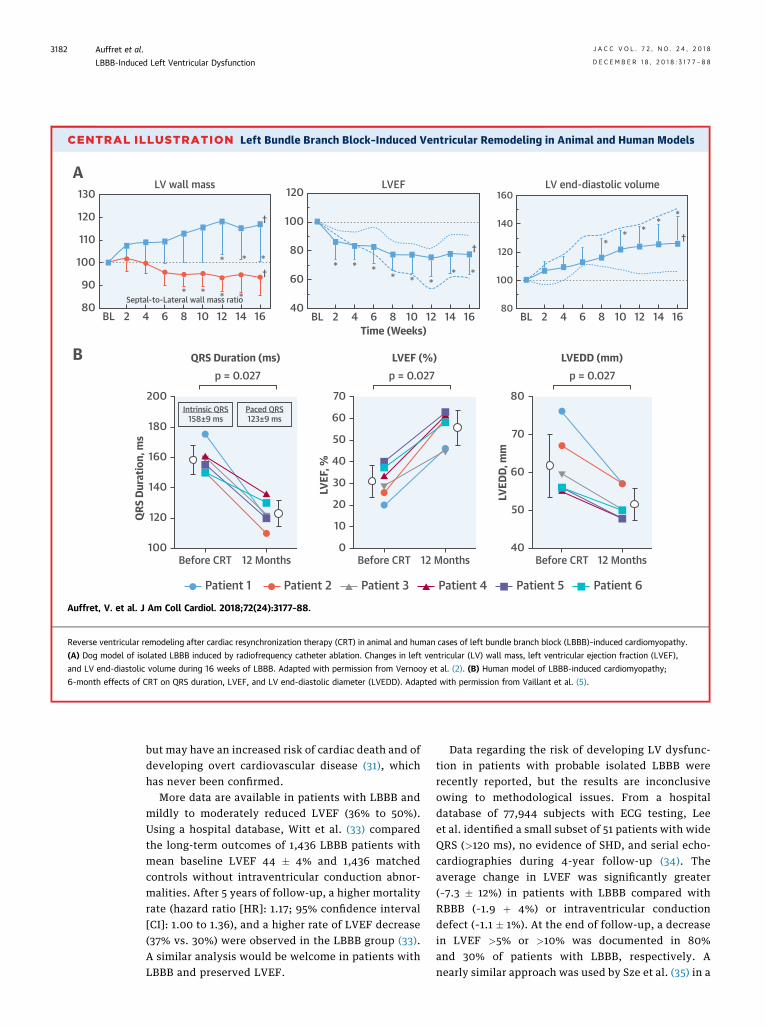
perfusion may contribute to these changes (2). LBBBinduced, both acutely and chronically, marked intra-LV dyssynchrony, with changes in the ventricularcontraction sequence very similar to those reportedin humans (20). During acute and chronic LBBB,myocardial blood flow was consistently lower in theseptum than in the LV lateral wall. Progressivestructural remodeling was evidenced by 2D echo.After 16 weeks of LBBB, mean 25% increase in LVend-diastolic volume, 23% decrease in LVEF, and 17%increase in LV wall mass were documented (CentralIllustration). Decrease in the septal-to-lateral wallmass index indicated asymmetric hypertrophy. Theauthors concluded that “asynchronous ventricularactivation during LBBB leads to redistribution ofcircumferential shortening and myocardial blood flowand, in the long run, LV remodeling. Septal hypo-perfusion appears to be primarily determined byreduced septal workload.”
In a complementary study, the authors showedthat most abnormalities could be reverted by biven-tricular pacing (BVP) (3). BVP reduced duration ofQRS, restored normal septal-to-lateral wall-motiondelay, and normalized the redistribution of regional

FIGURE 3 Mechanical Ventricular Dyssynchrony in Typical Left Bundle Branch Block
(A) Two-dimensional gray scale images in M-mode showing a typical aspect of septal flash (SF) with early thickening/thinning within the
isovolumic contraction period. (B) Longitudinal strain curves (septal longitudinal deformation in green and anterolateral wall deformation in
red) showing: 1) early shortening of at least 1 basal/midventricular segment of the septal wall; 2) early septal peak shortening (within the first
70% of the ejection phase); and 3) delayed lateral peak shortening occurring after aortic valve closure (AVC). (C) Pulsed-wave Doppler in the
apical 4-chamber view showing abnormal mitral inflow with A and E waves fusion and critical shortening of the left ventricular filling time.
Online Video 1.
J A C C V O L . 7 2 , N O . 2 4 , 2 0 1 8 Auffret et al.D E C E M B E R 1 8 , 2 0 1 8 : 3 1 7 7 – 8 8 LBBB-Induced Left Ventricular Dysfunction
3181
systolic circumferential shortening. After 8 weeks ofBVP, LV end-diastolic volume returned to pre-LBBBvalues, and hypertrophy regressed in the lateactivated LV lateral wall. These observations arecompatible with reverse remodeling by BVP.
In summary, in this model of normal canine heart,LBBB per se is responsible for progressive LV struc-tural remodeling. The particularity of this model isthe speed at which the phenomenon develops.This could be due to the much larger extent ofLBBB-related electrical asynchrony in dogs(doubling of QRS duration) compared with otherspecies (26).
HUMAN MODELS OF LBBB-INDUCED
CARDIOMYOPATHY: CLINICAL IMPACT
IDIOPATHIC ISOLATED LBBB. The prevalence ofLBBB is <1% in the general population but increases
with age, up to 5% at 80 years (1,30). Most patientswith LBBB have evidence of SHD: in particular, CADor cardiomyopathy. The prevalence of LBBB withoutapparent or suspected heart disease appears low,approximately 0.1% (31). Idiopathic isolated LBBB istherefore a rare diagnosis that can be ascertained onlyafter an extensive etiological assessment. In theabsence of consensus guidelines on how to evaluatethese patients, a noninvasive assessment for SHD(echocardiography and/or CMR to identify subtlemyocardial abnormalities) and ischemia is reason-able, especially in patients with known cardiovascu-lar risk factors (32).
In the absence of patient cohort followed pro-spectively over a very long time, the natural historyand the prognostic impact of idiopathic isolated LBBBremain largely unknown. Data from already old seriessuggested that patients with apparently isolatedLBBB were not at increased risk of all-cause mortality
CENTRAL ILLUSTRATION Left Bundle Branch Block–Induced Ventricular Remodeling in Animal and Human Models
A
B
120
110
100
90
802BL 4 6 8
LV wall mass
Septal-to-Lateral wall mass ratio
10 12 14
* * * *
* * *
†
†
16
130
†140
120
100
802BL 4 6 8
LV end-diastolic volume
10 12 14 16
** *
**
160
* * ** * *
* *
†
100
80
60
402BL 4 6 8
Time (Weeks)
LVEF
10 12 14 16
120
LVEF
, %
Before CRT 12 Months
p = 0.027LVEF (%)
60
50
40
30
20
10
0
70
LVED
D, m
m
Before CRT 12 Months
p = 0.027LVEDD (mm)
70
60
50
40
80
QRS
Dur
atio
n, m
s
Before CRT 12 Months
p = 0.027QRS Duration (ms)
180Intrinsic QRS
158±9 ms
160
140
120
100
200Paced QRS123±9 ms
Patient 1 Patient 2 Patient 3 Patient 4 Patient 5 Patient 6
Auffret, V. et al. J Am Coll Cardiol. 2018;72(24):3177–88.
Reverse ventricular remodeling after cardiac resynchronization therapy (CRT) in animal and human cases of left bundle branch block (LBBB)–induced cardiomyopathy.
(A) Dog model of isolated LBBB induced by radiofrequency catheter ablation. Changes in left ventricular (LV) wall mass, left ventricular ejection fraction (LVEF),
and LV end-diastolic volume during 16 weeks of LBBB. Adapted with permission from Vernooy et al. (2). (B) Human model of LBBB-induced cardiomyopathy;
6-month effects of CRT on QRS duration, LVEF, and LV end-diastolic diameter (LVEDD). Adapted with permission from Vaillant et al. (5).
Auffret et al. J A C C V O L . 7 2 , N O . 2 4 , 2 0 1 8
LBBB-Induced Left Ventricular Dysfunction D E C E M B E R 1 8 , 2 0 1 8 : 3 1 7 7 – 8 8
3182
but may have an increased risk of cardiac death and ofdeveloping overt cardiovascular disease (31), whichhas never been confirmed.
More data are available in patients with LBBB andmildly to moderately reduced LVEF (36% to 50%).Using a hospital database, Witt et al. (33) comparedthe long-term outcomes of 1,436 LBBB patients withmean baseline LVEF 44 � 4% and 1,436 matchedcontrols without intraventricular conduction abnor-malities. After 5 years of follow-up, a higher mortalityrate (hazard ratio [HR]: 1.17; 95% confidence interval[CI]: 1.00 to 1.36), and a higher rate of LVEF decrease(37% vs. 30%) were observed in the LBBB group (33).A similar analysis would be welcome in patients withLBBB and preserved LVEF.
Data regarding the risk of developing LV dysfunc-tion in patients with probable isolated LBBB wererecently reported, but the results are inconclusiveowing to methodological issues. From a hospitaldatabase of 77,944 subjects with ECG testing, Leeet al. identified a small subset of 51 patients with wideQRS (>120 ms), no evidence of SHD, and serial echo-cardiographies during 4-year follow-up (34). Theaverage change in LVEF was significantly greater(–7.3 � 12%) in patients with LBBB compared withRBBB (–1.9 þ 4%) or intraventricular conductiondefect (–1.1 � 1%). At the end of follow-up, a decreasein LVEF >5% or >10% was documented in 80%and 30% of patients with LBBB, respectively. Anearly similar approach was used by Sze et al. (35) in a

FIGURE 4 Incidence of New-Onset Left Bundle Branch Block After Transcatheter Aortic Valve Replacement
%
50
Both Valves Edwards SAPIEN/SAPIEN XT Medtronic CoreValve
30
40
20
10
0
Aktu
g et
al 2
012
(n =
139)
Kats
anos
et a
l 201
4 (n
= 9
4)Ak
tug
et a
l 201
2 (n
= 7
2)
Aktu
g et
al 2
012
(n =
67)
Calv
i et a
l 201
2 (n
= 16
2)
Uren
a et
al 2
014
(n =
858
)
Uren
a et
al 2
014
(n =
668
)
Uren
a et
al 2
012
(n =
202
)
Web
er e
t al 2
015
(n =
212
)Te
sta
et a
l 201
3 (n
= 8
18)
Uren
a et
al 2
014
(n =
698
)
Nazif
et a
l 201
4 (n
= 11
51)
Uren
a et
al 2
015
(n =
353
9)Re
geer
et a
l 201
7 (n
= 10
9)Fr
anzo
ni e
t al 2
013
(n =
238
)
Schy
mik
et a
l 201
5 (n
= 6
34)
Hout
huize
n et
al 2
012
(n =
679
)
Hout
huize
n et
al 2
014
(n =
476
)
Hout
huize
n et
al 2
012
(n =
292
)
Hout
huize
n et
al 2
012
(n =
387
)Ho
uthu
izen
et a
l 201
4 (n
= 2
23)
Khaw
aja
et a
l 201
1 (n
= 18
5)
Hout
huize
n et
al 2
014
(n =
253
)He
in-R
othw
eile
r et a
l 201
7 (n
= 2
25)
Schy
mik
et a
l 201
5 (n
= 5
12)
Schy
mik
et a
l 201
5 (n
= 12
2)
Nish
iyam
a et
al 2
017
(n =
90)
Joch
heim
et a
l 201
5 (n
= 3
54)
Fran
zoni
et a
l 201
3 (n
= 15
1)
Fran
zoni
et a
l 201
3 (n
= 8
7)
Bern
ardi
et a
l 201
6 (n
= 18
4)
Bern
ardi
et a
l 201
6 (n
= 5
77)
Sinn
ing
et a
l 201
7 (n
= 19
4)
Van
der B
oon
et a
l 201
5 (n
= 2
72)
Van
der B
oon
et a
l 201
5 (n
= 2
77)
Layn
ez e
t al 2
012
(n =
125)
Mun
oz-G
arcia
et a
l 201
3 (n
= 12
20)
Lope
z-Ag
uile
ra e
t al 2
016
(n =
153)
Lope
z-Ag
uile
ra e
t al 2
016
(n =
137)
Carr
abba
et a
l 201
5 (n
= 9
2)Le
nder
s et a
l 201
4 (n
= 2
32)
De T
orre
s-Al
ba e
t al 2
016
(n =
287
)
Bern
ardi
et a
l 201
6 (n
= 7
61)
Rates of new-onset left bundle branch block associated with the use of first-generation transcatheter valves. Adapted with permission from
Auffret et al. (38).
J A C C V O L . 7 2 , N O . 2 4 , 2 0 1 8 Auffret et al.D E C E M B E R 1 8 , 2 0 1 8 : 3 1 7 7 – 8 8 LBBB-Induced Left Ventricular Dysfunction
3183
case-control study comparing 2 groups of matchedpatients with baseline LVEF >50%, a group withLBBB, and a control group with normal QRS duration.After 3.8 years of follow-up, progression to LVdysfunction, defined as LVEF <45%, was observedin 36% of patients with LBBB compared with 10%controls. However, the median percent change inLVEF was relatively modest (from 55% to 50%) in theLBBB group.
Finally, some privileged clinical observationsreinforce the hypothesis of LBBB-CM, potentiallyreversible by CRT. Vaillant et al. (5) reported a seriesof patients (mean age 50 years) with a long history ofLBBB (>5 years). At the time of LBBB diagnosis, LVEFwas >50%, and no SHD was detected. All patientsdeveloped progressive LV dysfunction (LVEF <40%)and HF (New York Heart Association [NYHA] func-tional class II to IV). Major mechanical dyssynchronywas documented by cardiac imaging. All patientswere hyper-responders to CRT with complete
resolution of symptoms (NYHA functional class I),correction of mechanical dyssynchrony, and regres-sion of LV dysfunction (LVEF: 56 � 8%) (5) (CentralIllustration). Interestingly, the delay from LBBBdiagnosis to overt HF and to CRT implantation wasvery long: on average, 12 years (range 5 to 21 years)and 14 years (range 5 to 22 years) (5). These datasuggest that LBBB-CM is a slow and potentiallyreversible process.Pract i ca l impl ica t ions : p lace for prevent iveresynchron izat ion therapy . There are experi-mental and clinical arguments supporting theconcept of LBBB-CM. However, its actual incidence,evolution over time, and predisposing factors remainpoorly understood. The current priority is to reinforcethe clinical evidence. Ideally, a large cohort studywith prospective follow-up would be required. How-ever, its feasibility remains uncertain, given therelative rarity of isolated LBBB and the probable needfor very long-term follow-up.

TABLE 1 Mid-Term Evolution of Measures of Left Ventricular Function Following Transcatheter Aortic Valve Replacement According to the Occurrence of
Periprocedural New-Onset Left Bundle Branch Block
First Author,Year, Ref #
LBBBPatients, n (%)
ValveType (%)
LastEchocardiographic
Follow-Up
Pre-TAVR vs. Post-TAVRMean Left Ventricular Ejection
Fraction (%)
Other FindingsLBBB Patients No LBBB Patients
Urena et al., 2012 (54) 38 (19.0) ESV (100.0) 6–12 months 57 vs. 52*† 56 vs. 60*† LBBB was independently associated withdecreased LVEF at follow-up
Testa et al., 2013 (46) 224 (27.4) MCV (100.0) 1 yr 51 vs. 55 51 vs. 54 No significant difference in LV volumes over timewithin or among groups
Nazif et al., 2014 (50) 121 (10.5) ESV (100.0) 6–12 months 54.4 vs. 53.4*† 55.4 vs. 57.4*† The difference in LVEF recovery was the greatestamong patients with LVEF <35% at baseline.
Urena et al., 2014 (48) 79 (11.8) ESV (100.0) 6–12 months 56 vs. 56† 56 vs. 59*† LBBB was independently associated with the lackof LVEF improvement over time
Carrabba et al., 2015 (55) 34 (37.0) MCV (100.0) 1 yr 49.0 vs. 50.2 49.4 vs. 53.5* Significantly lower reduction in LV volumes in theLBBB group
Lopez-Aguilera et al., 2016 (56) 80 (42.0) MCV (100.0) NA NA NA Nonsignificant LVEF improvement among patientswithout LBBB vs. stable LVEF in LBBB patients
Dobson et al., 2017 (57) 24 (50.0) MCV (71.0)ESV (29.0)
6 months‡ 57 vs. 54 54 vs. 59* Significant reduction in LV volumes andimprovement in GLS among patients withoutLBBB vs. no significant changes in LBBBpatients
Values are n (%) unless otherwise indicated. *Significant difference between baseline and the last echocardiographic follow-up. †Significant difference between LBBB and non-LBBB patients at follow-up.‡Patients were evaluated by cardiac magnetic resonance at baseline and 6 months post-TAVR.
ESV ¼ Edwards Sapien Valve; MCV ¼ Medtronic CoreValve; GLS ¼ global longitudinal strain; LBBB ¼ left bundle branch block; LV ¼ left ventricle; LVEF ¼ left ventricular ejection fraction; NA ¼ notavailable.
Auffret et al. J A C C V O L . 7 2 , N O . 2 4 , 2 0 1 8
LBBB-Induced Left Ventricular Dysfunction D E C E M B E R 1 8 , 2 0 1 8 : 3 1 7 7 – 8 8
3184
In the current state of knowledge, early indicationsof CRT cannot be recommended in these patients, butas they are at risk of developing progressive LVdysfunction, it seems reasonable to recommendcloser monitoring with annual echocardiography.Follow-up could be strengthened if symptoms appearbut also if QRS widening or clear mechanicaldyssynchrony occur. Current evidence suggests thatthe process is largely reversible by CRT, even at anadvanced stage of LV dysfunction (5).
NEW-ONSET IATROGENIC LBBB AFTER AORTIC
VALVE OR SEPTAL INTERVENTIONS. Except thecases of new LBBB following septal myectomy fortreating hypertrophic obstructive cardiomyopathy(36,37), most iatrogenic LBBBs are related to aorticvalve interventions, which will therefore be the focusof this section.Mechan isms . Conduction disturbances followingtranscatheter aortic valve replacement (TAVR) orsurgical aortic valve replacement (SAVR) arise from adirect mechanical insult to the conduction systemdue to the close proximity between the aortic valve,and the His bundle, particularly its left branch (38).Various degrees of edema, hematoma, and ischemiamay associate with this mechanical interaction andpromote the occurrence of new-onset conductiondisturbances (39). Finally, aortic stenosis per se,through extending calcifications or granuloma,frequently associates with conduction disturbances.Among 435 candidates for TAVR, a 3.5% rate of
advanced atrioventricular block or LBBB was docu-mented by 24-h ECG monitoring immediately beforethe procedure (40).
Electr i ca l and mechan ica l dyssynchrony . Giventhe mechanical interaction usually involved, almostall patients exhibiting new-onset LBBB have “strict”LBBB (41), according to the ECG criteria recentlyproposed by Strauss (7). This observation may be ofimportance considering that patients with “strict”LBBB might have more pronounced LV dyssynchronycompared with their “nonstrict” LBBB counterpartsand could potentially derive greater benefit fromCRT. However, ventricles submitted to a chronicpressure overload, such as in patients with aorticstenosis, being severely remodeled, may not havenecessarily the same mechanical behavior as dilatedor normal hearts.Inc idence . A recent review reported that new LBBBcomplicated approximately 25% (range: 4% to 65%) ofTAVR procedures with first-generation devices, butthe incidence decreased to 12% to 22% with the latest-generation balloon-expandable valves (38). Of note,LBBB was more frequent following the implantationof the self-expandable CoreValve prosthesis (Cor-eValveSystem, Medtronic, Minneapolis, Minnesota)(range: 18% to 65%) or the mechanically expandedBoston Scientific Lotus valve (Boston Scientific,Marlborough, Massachusetts) (rates: 55% and 77%)compared with the rates observed with balloon-expandable valves (38). Figure 4 summarizes the
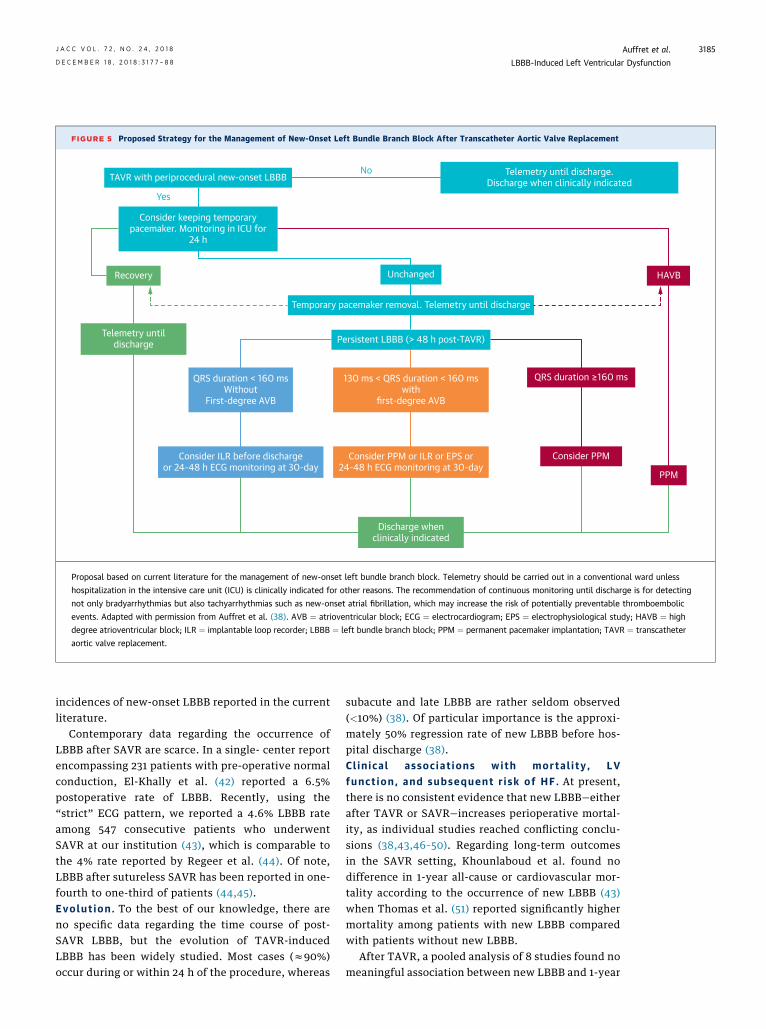
FIGURE 5 Proposed Strategy for the Management of New-Onset Left Bundle Branch Block After Transcatheter Aortic Valve Replacement
Discharge whenclinically indicated
Consider PPM or ILR or EPS or24-48 h ECG monitoring at 30-day
Consider PPM
QRS duration ≥160 ms
PPM
HAVB
Consider ILR before dischargeor 24-48 h ECG monitoring at 30-day
Telemetry untildischarge
Recovery
Persistent LBBB (> 48 h post-TAVR)
Temporary pacemaker removal. Telemetry until discharge
Telemetry until discharge.Discharge when clinically indicated
Unchanged
No
Yes
130 ms < QRS duration < 160 mswith
first-degree AVB
QRS duration < 160 msWithout
First-degree AVB
Consider keeping temporarypacemaker. Monitoring in ICU for
24 h
TAVR with periprocedural new-onset LBBB
Proposal based on current literature for the management of new-onset left bundle branch block. Telemetry should be carried out in a conventional ward unless
hospitalization in the intensive care unit (ICU) is clinically indicated for other reasons. The recommendation of continuous monitoring until discharge is for detecting
not only bradyarrhythmias but also tachyarrhythmias such as new-onset atrial fibrillation, which may increase the risk of potentially preventable thromboembolic
events. Adapted with permission from Auffret et al. (38). AVB ¼ atrioventricular block; ECG ¼ electrocardiogram; EPS ¼ electrophysiological study; HAVB ¼ high
degree atrioventricular block; ILR ¼ implantable loop recorder; LBBB ¼ left bundle branch block; PPM ¼ permanent pacemaker implantation; TAVR ¼ transcatheter
aortic valve replacement.
J A C C V O L . 7 2 , N O . 2 4 , 2 0 1 8 Auffret et al.D E C E M B E R 1 8 , 2 0 1 8 : 3 1 7 7 – 8 8 LBBB-Induced Left Ventricular Dysfunction
3185
incidences of new-onset LBBB reported in the currentliterature.
Contemporary data regarding the occurrence ofLBBB after SAVR are scarce. In a single- center reportencompassing 231 patients with pre-operative normalconduction, El-Khally et al. (42) reported a 6.5%postoperative rate of LBBB. Recently, using the“strict” ECG pattern, we reported a 4.6% LBBB rateamong 547 consecutive patients who underwentSAVR at our institution (43), which is comparable tothe 4% rate reported by Regeer et al. (44). Of note,LBBB after sutureless SAVR has been reported in one-fourth to one-third of patients (44,45).Evolut ion . To the best of our knowledge, there areno specific data regarding the time course of post-SAVR LBBB, but the evolution of TAVR-inducedLBBB has been widely studied. Most cases (z90%)occur during or within 24 h of the procedure, whereas
subacute and late LBBB are rather seldom observed(<10%) (38). Of particular importance is the approxi-mately 50% regression rate of new LBBB before hos-pital discharge (38).Cl in ica l assoc iat ions with morta l i ty , LVfunct ion , and subsequent r i sk of HF . At present,there is no consistent evidence that new LBBB—eitherafter TAVR or SAVR—increases perioperative mortal-ity, as individual studies reached conflicting conclu-sions (38,43,46–50). Regarding long-term outcomesin the SAVR setting, Khounlaboud et al. found nodifference in 1-year all-cause or cardiovascular mor-tality according to the occurrence of new LBBB (43)when Thomas et al. (51) reported significantly highermortality among patients with new LBBB comparedwith patients without new LBBB.
After TAVR, a pooled analysis of 8 studies found nomeaningful association between new LBBB and 1-year

Auffret et al. J A C C V O L . 7 2 , N O . 2 4 , 2 0 1 8
LBBB-Induced Left Ventricular Dysfunction D E C E M B E R 1 8 , 2 0 1 8 : 3 1 7 7 – 8 8
3186
all-cause mortality (risk ratio [RR]: 1.21; 95% CI: 0.98to 1.50) but found an increased risk of 1-year cardio-vascular mortality (RR: 1.39; 95% CI: 1.04 to 1.8) (52).These data may suggest a specific relationship thatmight be driven by an increased risk of sudden car-diac death, especially in patients with the widest QRScomplexes (>160 ms) (53) reproducing previousfindings in the setting of SAVR (42,51).
Numerous studies reported a deleterious effect ofnew-LBBB on LV function after TAVR (46,48,54–57)(Table 1), this effect being increasingly pronouncedwith decreasing baseline LVEF (48). This effect mayresult in a less favorable functional evolution afterthe procedure as well as a higher incidence of HFevents, including hospitalizations, among new LBBBpatients. However, in that regard, studies have so farbeen inconsistent (43,46,48,50), but the limitedfollow-up (#1 year) may have hampered the demon-stration of a difference in HF events in some studies.Cl in i ca l assoc iat ion with the need forpermanent pacemaker implantat ion . In recentguidelines on cardiac pacing and CRT, the onlyrecommendations for permanent pacemaker implan-tation (PPI) after SAVR or TAVR concern high-degreeAV block (HAVB) (58). At present, there is no recom-mendation for new-onset LBBB. Delayed HAVBbefore hospital discharge has been reported in up to13% of TAVR recipients with new LBBB (38). PPI ratesof 5% to 14% have been found at follow-up (38).Although individual studies were retrospective withdifferent thresholds prompting PPI among patientswith new LBBB, new LBBB was shown to be associ-ated with an approximately 2-fold higher risk of PPI(38,52). In accordance with guidelines, HAVB was theleading indication for PPI in new LBBB patients inmost studies.Management of pat ients with new-LBBB:potent ia l ro le of CRT. The clinical evidence onhow to manage patients with new LBBB after TAVR/SAVR remains scarce. Therefore, any recommenda-tion should only be regarded as proposals drawn fromobservational data. In that way, Auffret et al. recentlyproposed a management strategy to identify patientsat high risk of delayed HAVB or sudden cardiac death
during the early post-procedural period (Figure 5)(38).
This discussion does not take into account thelong-term hemodynamic risk of persistent LBBB andthe potential role of CRT, the clinical experience ofwhich remains limited to a few case reports (59,60).Data presented here suggest that CRT could bereasonable in patients with preexisting LV dysfunc-tion (LVEF <50%) and new LBBB persisting at 30 daysafter TAVR, which might put these patients at highermortality and morbidity risk (38).
Similarly, it is known that distal His bundle pacingcan normalize QRS duration and correct the bundlebranch block pattern in selected patients with pre-existing LBBB (61). It has recently shown promisingoutcomes regarding the occurrence of HF hospitali-zation and a trend toward reduced mortalitycompared with RV pacing and could therefore repre-sent a valuable alternative to CRT in these patientswith persisting LBBB after TAVR and pre-existing LVdysfunction (62,63).
Nonetheless, these hypotheses deserve to beproperly evaluated in an adequately designed ran-domized controlled trial.
CONCLUSIONS
As in animal models, isolated LBBB, whetheridiopathic or iatrogenic, may induce ventricularstructural remodeling and lead to LV systolicdysfunction. CRT could reverse this process andprevent progression to overt HF. However, currentepidemiological and clinical data are not strongenough to recommend its use as a preventive mea-sure. Large-scale prospective registries in LBBBpopulations and randomized CRT or His bundlepacing trials in selected at-risk populations areneeded.
ADDRESS FOR CORRESPONDENCE: Dr. VincentAuffret, Cardiology and Vascular Diseases Depart-ment, Pontchaillou University Hospital, 2 rue HenriLe Guilloux, 35033 Rennes, France. E-mail: [email protected]. Twitter: @CHURennes.
RE F E RENCE S
1. Francia P, Balla C, Paneni F, Volpe M. Leftbundle-branch block: pathophysiology, prognosis,and clinical management. Clin Cardiol 2007;30:110–5.
2. Vernooy K, Verbeek XA, Peschar M, et al. Leftbundle branch block induces ventricular remodel-ling and functional septal hypoperfusion. EurHeart J 2005;26:91–8.
3. Vernooy K, Cornelussen RN, Verbeek XA,et al. Cardiac resynchronization therapy curesdyssynchronopathy in canine left bundle-branch block hearts. Eur Heart J 2007;28:2148–55.
4. Blanc JJ, Fatemi M, Bertault V, Baraket F,Etienne Y. Evaluation of left bundle branchblock as a reversible cause of non-ischaemic
dilated cardiomyopathy with severe heart fail-ure: a new concept of left ventriculardyssynchrony-induced cardiomyopathy. Euro-pace 2005;7:604–10.
5. Vaillant C, Martins RP, Donal E, et al. Resolutionof left bundle branch block-induced cardiomyop-athy by cardiac resynchronization therapy. J AmColl Cardiol 2013;61:1089–95.

J A C C V O L . 7 2 , N O . 2 4 , 2 0 1 8 Auffret et al.D E C E M B E R 1 8 , 2 0 1 8 : 3 1 7 7 – 8 8 LBBB-Induced Left Ventricular Dysfunction
3187
6. Surawicz B, Childers R, Deal BJ, et al. AHA/ACCF/HRS recommendations for the standardiza-tion and interpretation of the electrocardiogram.Part III: Intraventricular conduction disturbances. JAm Coll Cardiol 2009;53:976–81.
7. Strauss DG, Selvester RH, Wagner GS. Definingleft bundle branch block in the era of cardiacresynchronization therapy. Am J Cardiol 2011;107:927–34.
8. Vassallo JA, Cassidy DM, Marchlinski FE, et al.Endocardial activation of left bundle branch block.Circulation 1984;69:914–23.
9. Auricchio A, Fantoni C, Regoli F, et al. Charac-terization of left ventricular activation in patientswith heart failure and left bundle-branch block.Circulation 2004;109:1133–9.
10. Derval N, Duchateau J, Mahida S, et al.Distinctive left ventricular activations associatedwith ECG pattern in heart failure patients. CircArrhythm Electrophysiol 2017;10:e005073.
11. Ploux S, Lumens J, Whinnett Z, et al. Nonin-vasive electrocardiographic mapping to improvepatient selection for cardiac resynchronizationtherapy: beyond QRS duration and left bundlebranch block morphology. J Am Coll Cardiol 2013;61:2435–43.
12. Dillon JC, Chang S, Feigenbaum H. Echocar-diographic manifestations of left bundle branchblock. Circulation 1974;49:876–80.
13. Gjesdal O, Remme EW, Opdahl A, et al.Mechanisms of abnormal systolic motion of theinterventricular septum during left bundle branchblock. Circ Cardiovasc Imaging 2011;4:264–73.
14. Bramlet DA, Morris KG, Coleman RE, Albert D,Cobb FR. Effect of rate-dependent left bundlebranch block on global and regional left ventric-ular function. Circulation 1983;67:1059–65.
15. Parsai C, Bijnens B, Sutherland GR, et al. To-ward understanding response to cardiac resynch-ronization therapy: left ventricular dyssynchronyis only one of multiple mechanisms. Eur Heart J2009;30:940–9.
16. Voigt JU, Schneider TM, Korder S, et al. Apicaltransverse motion as surrogate parameter todetermine regional left ventricular function in-homogeneities: a new, integrative approach to leftventricular asynchrony assessment. Eur Heart J2009;30:959–68.
17. Risum N, Strauss D, Sogaard P, et al. Leftbundle branch block: the relationship betweenelectrical activation and echocardiography me-chanical contraction. Am Heart J 2013;166:340–8.
18. Russell K, Eriksen M, Aaberge L, et al. A novelclinical method for quantification of regional leftventricular pressure–strain loop area: a non-invasive index of myocardial work. Eur Heart J2012;33:724–33.
19. Galli E, Leclercq C, Fournet M, et al. Value ofmyocardial work estimation in the prediction ofresponse to cardiac resynchronization therapy.J Am Soc Echocardiography 2017;31:220–30.
20. Risum N, Tayal B, Hansen TF, et al. Identifi-cation of typical left bundle branch blockcontraction by strain echocardiography is additiveto electrocardiography in prediction of long-term
outcome after cardiac resynchronization therapy.J Am Coll Cardiol 2015;66:631–41.
21. Grines CL, Bashore TM, Boudoulas H, Olson S,Shafer P, Wooley CF. Functional abnormalities inisolated left bundle branch block: the effect ofinterventricular asynchrony. Circulation 1989;79:845–53.
22. Cvijic M, Duchenne J, Unlu S, et al. Timing ofmyocardial shortening determines left ventricularregional myocardial work and regional remodel-ling in hearts with conduction delays. Eur Heart JCardiovasc Imaging 2018;19:941–9.
23. Hirzel HO, Senn M, Nuesch K, et al. Thallium-201 scintigraphy in complete left bundle branchblock. Am J Cardiol 1984;53:764–9.
24. Skalidis EI, Kochiadakis GE, Koukouraki SI,et al. Phasic coronary flow pattern and flowreserve in patients with left bundle branch blockand normal coronary arteries. J Am Coll Cardiol1999;33:1338–46.
25. Zanco P, Desideri A, Mobilia G, et al. Effects ofleft bundle branch block on myocardial FDG PET inpatients without significant coronary artery ste-noses. J Nucl Med 2000;41:973–7.
26. Strik M, van Middendor LB, Vernooy K. Animalmodels of dyssynchrony. J Cardiovasc Trans Res2012;5:135–45.
27. Liu L, Tockman B, Girouard S, et al. Left ven-tricular resynchronization therapy in a caninemodel of left bundle branch block. Am J PhysiolHeart Circ 2002;282:H2238–44.
28. Verbeek XA, Vernooy K, Peschar M, Van DerNagel T, Van Hunnik, Prinzen FW. Quantification ofinterventricular asynchrony during LBBB andventricular pacing. Am J Physiol Heart Circ 2002;283:H1370–8.
29. Leclercq C, Faris O, Tunin R, et al. Systolicimprovement and mechanical resynchronizationdoes not require electrical synchrony in the dilatedfailing heart with left bundle-branch block. Cir-culation 2002;106:1760–3.
30. Schneider JF, Thomas HE Jr., Kreger BE,McNamara PM, Kannel WB. Newly acquired leftbundle-branch block: the Framingham Study. AnnIntern Med 1979;90:303–10.
31. Fahy GJ, Pinski SL, Miller DP, et al. Naturalhistory of isolated bundle branch block. Am JCardiol 1996;77:1185–90.
32. Kumar V, Venkataraman R, Aljaroudi W, et al.Implications of left bundle branch block in patienttreatment. Am J Cardiol 2013;111:291–300.
33. Witt CM, Wu G, Yang D, Hodge DO, Roger VL,Cha YM. Outcomes with left bundle branch blockand mildly to moderately reduced left ventricularfunction. JACC Heart Fail 2016;4:897–903.
34. Lee SJ, McCulloch C, Mangat I, Foster E, DeMarco T, Saxon L. Isolated bundle branch blockand left ventricular dysfunction. J Card Fail 2003;9:87–92.
35. Sze E, Dunning A, Loring Z, et al. Comparisonof incidence of left ventricular systolic dysfunctionamong patients with left bundle branch blockversus those with normal QRS duration. Am JCardiol 2017;120:1990–7.
36. Qin JX, Shiota T, Lever HM, et al. Conductionsystem abnormalities in patients with obstructivehypertrophic cardiomyopathy following septalreduction interventions. Am J Cardiol 2004;93:171–5.
37. Daubert C, Gadler F, Mabo P, Linde C. Pacingfor hypertrophic obstructive cardiomyopathy: anupdate and future directions. Europace 2018;20:908–20.
38. Auffret V, Puri R, Urena M, et al. Conductiondisturbances after transcatheter aortic valvereplacement: current status and future perspec-tives. Circulation 2017;136:1049–69.
39. Moreno R, Dobarro D, López De Sá E, et al.Cause of complete atrioventricular block afterpercutaneous aortic valve implantation: insightsfrom a necropsy study. Circulation 2009;120:e29–30.
40. Urena M, Hayek S, Cheema AN, et al.Arrhythmia burden in elderly patients with severeaortic stenosis as determined by continuous elec-trocardiographic recording: toward a better un-derstanding of arrhythmic events aftertranscatheter aortic valve replacement. Circulation2015;131:469–77.
41. Sundh F, Simlund J, Harrison JK, et al. Inci-dence of strict versus non-strict left bundle branchblock after transcatheter aortic valve replacement.Am Heart J 2015;169:438–44.
42. El-Khally Z, Thibault B, Staniloae C, et al.Prognostic significance of newly acquired bundlebranch block after aortic valve replacement. Am JCardiol 2004;94:1008–11.
43. Khounlaboud M, Flecher E, Fournet M, et al.Predictors and prognostic impact of new leftbundle branch block after surgical aortic valvereplacement. Arch Cardiovasc Dis 2017;110:667–75.
44. Regeer MV, Merkestein LR, de Weger A, et al.Left bundle branch block after sutureless, trans-catheter, and stented biological aortic valvereplacement for aortic stenosis. EuroIntervention2017;12:1660–6.
45. Bouhout I, Mazine A, Rivard L, et al. Conduc-tion disorders after sutureless aortic valvereplacement. Ann Thorac Surg 2017;103:1254–60.
46. Testa L, Latib A, De Marco F, et al. Clinicalimpact of persistent left bundle-branch block aftertranscatheter aortic valve implantation with Cor-eValve Revalving System. Circulation 2013;127:1300–7.
47. Houthuizen P, Van Garsse LA, Poels TT, et al.Left bundle-branch block induced by trans-catheter aortic valve implantation increases risk ofdeath. Circulation 2012;126:720–8.
48. Urena M, Webb JG, Cheema A, et al. Impact ofnew-onset persistent left bundle branch block onlate clinical outcomes in patients undergoingtranscatheter aortic valve implantation with aballoon-expandable valve. J Am Coll Cardiol Intv2014;7:128–36.
49. Schymik G, Tzamalis P, Bramlage P, et al.Clinical impact of a new left bundle branch blockfollowing TAVI implantation: 1-year results of theTAVIK cohort. Clin Res Cardiol 2015;104:351–62.

Auffret et al. J A C C V O L . 7 2 , N O . 2 4 , 2 0 1 8
LBBB-Induced Left Ventricular Dysfunction D E C E M B E R 1 8 , 2 0 1 8 : 3 1 7 7 – 8 8
3188
50. Nazif TM, Williams MR, Hahn RT, et al. Clinicalimplications of new-onset left bundle branchblock after transcatheter aortic valve replacement:analysis of the PARTNER experience. Eur Heart J2014;35:1599–607.
51. Thomas JL, Dickstein RA, Parker FB, et al. Prog-nostic significance of the development of left bundleconduction defects following aortic valve replace-ment. J Thorac Cardiovasc Surg 1982;84:382–6.
52. Regueiro A, Abdul-Jawad Altisent O, DelTrigo M, et al. Impact of new-onset left bundlebranch block and periprocedural permanentpacemaker implantation on clinical outcomes inpatients undergoing transcatheter aortic valvereplacement: a systematic review and meta-analysis. Circ Cardiovasc Interv 2016;9:e003635.
53. Urena M, Webb JG, Eltchaninoff H, et al. Latecardiac death in patients undergoing transcatheteraortic valve replacement: incidence and predictorsof advanced heart failure and sudden cardiacdeath. J Am Coll Cardiol 2015;65:437–48.
54. Urena M, Mok M, Serra V, et al. Predictivefactors and long-term clinical consequences ofpersistent left bundle branch block followingtranscatheter aortic valve implantation with aballoon-expandable valve. J Am Coll Cardiol 2012;60:1743–52.
55. Carrabba N, Valenti R, Migliorini A, et al.Impact on left ventricular function and remodelingand on 1-year outcome in patients with left bundlebranch block after transcatheter aortic valve im-plantation. Am J Cardiol 2015;116:125–31.
56. Lopez-Aguilera J, Segura Saint-Gerons JM,et al. Effect of new-onset left bundle branch blockafter transcatheter aortic valve implantation(CoreValve) on mortality, frequency of re-hospitalization, and need for pacemaker. Am JCardiol 2016;118:1380–5.
57. Dobson LE, Musa TA, Uddin A, et al. The impactof trans-catheter aortic valve replacement inducedleft-bundle branch block on cardiac reverseremodeling. J Cardiovasc Magn Reson 2017;19:22.
58. Brignole M, Auricchio A, Baron-Esquivias G,et al. 2013 ESC Guidelines on cardiac pacing andcardiac resynchronization therapy. Eur Heart J2013;34:2281–329.
59. Meguro K, Lellouche N, Teiger E. Cardiacresynchronization therapy improved heart failureafter left bundle branch block during trans-catheter aortic valve implantation. J InvasiveCardiol 2012;24:132–3.
60. Osmancik P, Stros P, Herman D, et al. Cardiacresynchronization therapy implantation following
transcatheter aortic valve implantation. Europace2011;13:290–1.
61. Sharma PS, Ellison K, Patel HN, Trohman RG.Overcoming left bundle branch block by perma-nent His bundle pacing: evidence of longitudinaldissociation in the His via recordings from a per-manent pacing lead. Heart Rhythm Case Rep 2017;3:499–502.
62. Abdelrahman M, Subzposh FA, Beer D, et al.Clinical outcomes of His bundle pacing comparedto right ventricular pacing. J Am Coll Cardiol 2018;71:2319–30.
63. Vijayaraman P, Chung MK, Dandamudi G, et al.His bundle pacing. J Am Coll Cardiol 2018;72:927–47.
KEY WORDS cardiac resynchronizationtherapy, LBBB-induced cardiomyopathy, leftbundle branch block, left ventriculardysfunction, mechanical dyssynchrony,transcatheter aortic valve replacement
APPENDIX For a supplemental video,please see the online version of this paper.




























