Embed Size (px)
DESCRIPTION
end
Citation preview

Journal of Geriatric Cardiology December 2007 Vol 4 No 4 225
Clinical Research
Prediction of acute stroke progression by the NationalInstitutes of Health Stroke Scale
Vinh Phuong, Tran Van Huy
Department of Geriatric Cardiology, Khanh Hoa Hospital,Vietnam
Objective To determine the occurrence of neurological changes during the first 48 hours after acute stroke as it relates to the initialstroke severity assessment. Methods The assessment with the National Institutes of Health Stroke Scale (NIHSS) was performedserially for the first 48 hours on 68 consecutive ischemic stroke patients admitted to the Department of Geriatric Cardiology at theKhanh Hoa Hospital, Nha Trang, Vietnam. Incidence of stroke progression (a¡Ý3-point increase on the NIHSS) was recorded andanalysis performed to determine its association with initial stroke severity and other demographic and physiological variables. Deficitresolution by 48 hours, defined as an NIHSS score of 0 or 1, measured the frequency of functional recovery predicted by the initial deficit.Results Overall progression was noted in 28% of events (19/68). Applying Bayes’ solution to the observed frequency of worsening, thegreatest likelihood of predicting future patient progression occurred with NIHSS score of =7 and >7. Patients with an initial NIHSS scoreof =7 experienced a 13% (6/47) worsening rate versus those of an initial score of >7 with a 62% (13/21) worsening rate (P<0.01). 42.5%(20/47) of those with an initial score of =7 were functionally normal at 48 hours, whereas only 4.7% (1/21) of those with scores of >7returned to a normal examination within this period (χ2, P<0.05). Conclusions This study suggests that the early clinical course ofneurological deficit after acute stroke be dependent on the initial stroke severity and that a dichotomy in early outcome exist surroundingan initial NIHSS score of 7. These findings may have significant implications for the design and patient stratification in treatmentprotocols with respect to primary clinical outcome.(J Geriatr Cardiol 2007;4:225-228.)
Key Word stroke; prediction
Corresponding author: Dr. Vinh Phuong. Department of GeriatricCardiology, Khanh Hoa Hospital. 19 Yersin Nha Trang, Vietnam.Tel: 8458-812344. E-mail: [email protected]
Introduction
Clinical observations suggest that the first 48 hoursafter an ischemic stroke be associated with potential insta-bility and secondary worsening.1-3 Recent researches havedemonstrated that much of the cell death from stroke resultsfrom a complex series of biochemical events (often termedthe “ischemic cascade”) that occur over a period of hours oreven days after the initial stroke.4- 6 In addition, compo-nents of the inflammatory pathways, which are consideredto be the hallmarks of reperfusion injury, can result in sec-ondary tissue injury and further vascular compromise.7-9
The National Institutes of Health Stroke Scale (NIHSS)of the USA is widely used in the assessment of initial andfinal neurological deficits in all acute stroke studies.10 It wasone of multiple variables analyzed for its capacity to predictprogression and improvement of the patient suffering fromstroke.10
The objective of this study was to determine the char-acteristics of patients likely to show neurological changesduring the first 48 hours after the onset of acute cerebralischemia by NIHSS in the setting of a stroke- patient-admit-
ting department.
Subjects & methodsSubjects
The study include all patients > 18 years admitted tothe Department of Geriartic Cardiology at Khanh HoaHospital, Nha Trang, Vietnam from June 2005 to September2006 with the diagnosis of acute ischemic stroke. The NIHSSwas performed at presentation and every 8 hours for 48hours on all patients.
Inclusion criteria: 1) Ischemic stroke onset within 24hours of enrollment, 2) identifiable time of onset, 3) stabledeficit lasting longer than 1 hour without rapid improvement.
Exclusion criteria: 1) Hemorrhagic stroke, 2) prior neu-rological deficit that obscured the ability to follow the neu-rological examination from the most recent infarct, 3) Coma.
NIHSS scoringNIHSS is short for National Institutes of Health Stroke
Scale. It was a commonly used yardstick for measuring theoutcome of neurological deficits in stroke patients. Ratersare well trained and given detailed instructions from theNIH Stroke Scale Training Digital Video Disk provided bythe National Institute of Neurological Disorders and Stroke.10
The scale consists of 11 items, and each item includes a

Journal of Geriatric Cardiology December 2007 Vol 4 No 4226
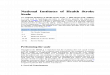
0%0%
10%
43%
83%
60%
50%
13%
0102030405060708090
1 - 7 8 - 14 15 - 21 > 21
Improved Worsened
scale of several scores, with a total score of 42 .10
Imaging classificationComputer tomography (CT) scan was performed on
all patients to confirm the location and size of the infarct.Imaging classifications of the strokes were divided into thefollowing 5 categories: 1) lacunar infarcts (subcortical le-sions =1 cm), 2) small to moderate cortical or subcorticalinfarcts [>1cm and <1/3 of the mid-cerebral artery (MCA)distribution], 3) moderate to large cortical or subcorticalinfarcts (>1/3 MCA distribution), 4) brain stem, and 5) normal.
Monitoring: Patients were monitored carefully for clini-cal changes: 1) neurological worsening was defined as a 3-point or greater increase on the NIHSS during the first 48hours. 2) patients were classified as having “improved” ifthey had a normal examination at the end of 48 hours (NIHSSscore of 0 or 1).
Statistical analysis: Bayes’ solution rule16 was ap-plied to identify a threshold initial NIHSS score. The prob-ability is that a patient with a score below the threshold whois predicted to improve in 48 hours and the probability thata patient with a score above the threshold who is predictedto worsen in 48 hours. A χ2 test was performed to determinewhether the rates of worsening and improvement were dif-ferent between the groups of patients above and below theinitial stroke scale threshold. A stepwise logistic regressionanalysis was performed to assess which variables were as-sociated with stroke progression. The demographic data,baseline characteristics, and risk factors for stroke werecompared between those who showed progression andthose who did not by the Student’st test and Mann-Whitneyrank sum as appropriate.
Results
From June 2004 to September 2005, sixty eight patientswere admitted, and among those, forty four (65%) were menand twenty four (35%) were women. The average patientage was 66.2 years. The average time from onset of strokesymptoms to enrollment into the study was 15 hours, andthe average initial NIHSS score was 6.5. Overall, progres-sion of neurological deficits occurred in 19 of the 68 events(28%)(Table 1).
Patients with an NIHSS of score>7 worsened in 13 of21 cases (62%) compared with those with an initial score of
Table 1 Demographic data & baseline characteristics ofpatients
Characteristics Frequency %
Sex Male(n) 44 65 Female(n) 24 35No. of patients worsened(n) 19 28No. of pts without progression(n) 49 72Average age(yr) 66.2Average time from onset to admission (hr) 15Average progression time (hr) 34.9±13.2Average initial NIHSS score 6.5
Figure 1 Neurological progression related to the NIHSS score
7, who worsened in only 6 of 47 cases (13%) (χ2 = 8,790, P<0.01). In addition, 20 of 47 patients (42.5%) with an initialNIHSS score 7 were normal (NIHSS score of 0 or 1) at 48hours, whereas only 1 of 21 (4,7%) of those with scores >7were normal at the same time point (χ2 = 5.883, P<0.05) (Figure1 Table 2).
Stepwise logistic regression of the factors tested forassociation with stroke progression [demographic data: age,sex, baseline characteristics: completed blood count (CBC),atrial fibrillation, initial NIHSS score, mean arterial pressure(MAP), and risk factors for stroke: hypertenion (HTN),smoking, hypercholesterolemia, diabetes] revealed that onlythe initial neurological score, MAP and atrial fibrillation wereuseful in predicting which patients would worsen (Table 3).
Atrial fibrillation and mean arterial blood pressure
Table 2 Neurological worsening or return to normal related to the NIHSS score
Neurological changes Score:1-7 Score:8-14 Score:15-21 Score:>21 TotalImprovement 20 (43%) 1 (10%) 0 (0%) 0 (%) 21 (31%)Without progression 21 (45%) 4 (40%) 2 (40%) 1 (17%) 28 (41%)Worsening 6 (13%) 5 (50%) 3 (60%) 5 (83%) 19 (28%)Total 47 10 5 6 68 (100%)

Journal of Geriatric Cardiology December 2007 Vol 4 No 4 227
(MAP) in the first 48 hours were significant factors associ-ated with patients who worsened (P=0.014 & P=0.012).Especially, the initial neurological score strongly tendedtoward association with worsening neurological progres-sion (P<0.001). There was no significant association withother factors such as age, sex, CBC on admission, as well asHTN, smoking, diabetes, and high LDL-cholesterol.
Analysis of stroke subtypes by CT demonstrated asignificantly greater likelihood of progression in patientswith large to moderate cortical and subcortical infarcts,whereas patients with lacunar and small subcortical infarctsor normal scans had significantly fewer episodes of neuro-logical deterioration (Table 4).
Discussion
Our study demonstrates the potential value of the ini-tial NIHSS score in identifying those patients who are likelyto progress as well as those likely to improve over the first48 hours. A sharp demarcation in the occurrence of improve-ment was also seen at a threshold of 7. The observed fre-quency of clinical worsening sharply increased above aninitial NIHSS score of 7, with the probability of worseningbeing 5 times greater with a score of >7 (62%) than with a
score of =7 (13%). With a score of =7 on admission, a pa-tient was 9 times more likely to be normal in 48 hours thanthose presenting with higher scores.
Other recent prospective studies of progression inacute stroke have highlighted the high frequency of changein the neurological examination that can occur in the firstseveral hours to days after ischemic injury, and that de-layed edema may play a role in symptom progression. 3, 13-17
Early deterioration has been noted in as many as 22-40% ofpatients in the first 48 hours, 3 and “major neurological im-provement” has been reported in 22-28% of acute strokevictims during the same time frame. 14,16 This may allow thera-pies targeting the ischemic penumbra to be instituted dur-ing the phase of lesion extension in these patient subgroupswith greater chances of stroke progression.
The importance of understanding the frequency ofalterations in the clinical condition after acute stroke is il-lustrated by the data that show the predictive value of earlychanges on long-term outcome. Toni, et al 3,15 reveals thatpatients with early deterioration have an increased mortal-ity of 35% to 50%. Conversely, patients with early improve-ment have been reported to have a high frequency of goodoutcome (79%) at 30 days.3 In addition, it has been shownthat the clinical course of recovery stabilizes beyond day 4,
Table 4. Stroke progression related to stroke subtype by CT
Stroke subtype Progression (n=19) Nonprogression (n=49) p value
(¢ñ) Lacunar/small subcortical infarction 1 (5.3%) 21(42.9%) <0.05(¢ò) Moderate to large cortical /subcortical infarcts(>1/3 MCA) 12 (63.2%) 7(14.3%) <0.01(¢ó) Small cortical / subcortical infarcts(<1/3 MCA) 2 (10.5%) 5(10.2%) 0.61(¢ô) Brain stem 1 (5.3%) 5(10.2%) 0.32(¢õ) Normal 3 (15.8%) 11(22.4%) 0.30
Table 3. The factors tested for associations with stroke progression
No Factors Progression (n=19) Nonprogression (n=49) p
1 Age 1 2 67.6 66.0 0.2372 Sex, M/F 13/6 31/18 0.6903 Hypertension 16(84.2%) 31(63.2%) 0.0934 Smoking 11(57.9%) 18(36.7%) 0.1135 Hypercholesterolemia 9 (47.3%) 12 (24.5%) 0.0676 Diabetes 3 (15.8%) 9 (18.4%) 0.8027 Atrial fibrillation 1 6(31.5%) 4 (8.2%) 0.0148 Initial NIHSS score 1 2 8.95 5.57 <0.0019 White blood cell1 2 9.105 9.285 0.72410 Platelet 1 2 198.9 207.3 0.30311 MAP1 114.2 108.2 0.012
Note:1 Stepwise logistic regression analysis2 Mann-Whitney rank-sum test.

Journal of Geriatric Cardiology December 2007 Vol 4 No 4228
with improvement becoming more linear from that time on. 3
We found that infarct size was closely associated withneurological changes, as previously noted by someinvestigators.15 Patients with lacunar infarcts were 10 timesmore likely to remain stable or improve than to experienceneurological deterioration. Conversely, patients with mod-erate to large cortical and subcortical infarcts (>1/3 of theMCA territory) were significantly more likely to progressthan any other imaging-defined subgroup.
In addition, our study demonstrated that strokes oc-curring in patients with atrial fibrillation are more likely toprogress. Whether this is due to larger strokes (more com-monly seen with cardioembolic ischemic events) or re-em-bolization is unknown. Of those with atrial fibrillation whoprogressed, 5 of 6 had moderate to large cortical or subcor-tical infarcts. Of those who did not progress, 50% had smallcortical or subcortical infarcts.
Conclusion
This study strongly suggests that the course of neu-rological deficit following acute stroke is dependent on theinitial stroke severity and that a dichotomy in early outcomeexists with respect to the initial NIHSS scores when pa-tients are stratified to =7 and >7.
Additionally, MAP and atrial fibrillation were foundto be useful in predicting neurological worsening.
These findings may have significant implications forthe design and patient stratification in treatment protocolswith respect to primary clinical outcome.
References
1. Johnston KC, Li JY, Lyden PD, et al. Medical and neurologicalcomplications of ischemic stroke: experience from theRANTTAS trial. Stroke 1998;29:447–53.
2. Davalos A, Cendra E, Teruel J, et al. Deteriorating ischemicstroke: risk factors and prognosis. Neurology 1990; 40:1865-9.
3. Toni D, Fiorelli M, Bastianello S, et al. Acute ischemic strokesimproving during the first 48 hours of onset: predictability,outcome, and possible mechanisms. Stroke 1997;22:10-14.
4. Choi D. Cerebral hypoxia: some new approaches and unan-swered questions. J Neurosci 1990;10:2493-501.
5. Kuroda S, Siesju BK. Reperfusion damage following focalischemia: pathophysiology and therapeutic windows. ClinNeurosci 1997;4:199-212.
6. Chalmers-Redman RME, Fraser AD, Ju WYH, et al. Mecha-nisms of nerve cell death: apoptosis or necrosis after cerebralischemia. Int Rev Neurobiol 1997;40:1-25.
7. Hallenbeck JM. Inflammatory reactions at the blood-endot-helial interface in acute stroke. Adv Neurol 1996;71:281-300.
8. DeGraba TJ. The role of inflammation following acute stroke:utility of pursuing anti-adhesion molecule therapy. Neurol-ogy 1998;51(Suppl 3):S62-8.
9. Bjork J, Hedqvist P, Arfors KE. Increase in vascular perme-ability induced by leukotriene B4 and the role of polymor-phonuclear leukocytes. Inflammation 1982;6:189-200.
10. Lyden P, Raman R, Liu L, et al. NIHSS training and certifica-tion using a new digital video disk is reliable. Stroke 2005; 36:2446-9.
11. Goldstein LB, Bertels C, PA-C, Davis JN. Interrelatel reliabil-ity of the NIH Stroke Scale. Arch Neurol 1989;46:660-2.
12. Rao CR. Linear Statistical Inference and Its Applications.New York, NY: John Wiley & Sons; 1965: 413-9, 487-93.
13. Biller J, Love BB, Marsh EE, et al. Spontaneous improve-ment after acute ischemic stroke. Stroke 1990; 21:1008-12.
14. Toni D, Fiorelli M, Zanette EM, et al. Early spontaneousimprovement and deterioration of ischemic stroke patients.Stroke 1998; 29:1144-48.
15. Toni D, Fiorelli M, Gentile M, et al. Progressing neurologicaldeficit secondary to acute ischemic stroke. Arch Neurol 1995;52:670-5.
16. Wityk RJ, Pessin MS, Kaplan RF, et al. Serial assessment ofacute stroke using the NIH Stroke Scale. Stroke 1994; 25:362-5.
17. Fiorelli M, Alperovitch A, Argentino C, et al. Prediction oflong-term outcome in the early hours following acute ischemicstroke. Arch Neurol 1995;52:250-5.

















![Progressing haemorrhagic stroke: categories, causes ... · to the initial haemorrhagic stroke progression [46, 113, 182]. Inflammation Sun et al. [155] reported that a white blood](https://img.pdfslide.us/doc/110x75/5ca04eb688c993c5178cebec/progressing-haemorrhagic-stroke-categories-causes-to-the-initial-haemorrhagic.jpg)