Embed Size (px)
Citation preview

631
respectively, and therefore enabled us to reliably detect thesesubunits even in the presence of a 100-1000-fold excess of
holo-hCG, as is often seen in choriocarcinoma (unpublishedresults). With these assay systems, we determined the physiologicalrange of hCG and its free subunits in the sera of 15 healthy malesubjects: 240 pg/ml for holo-hCG, 190 pg/ml for hCGfx, and 48pg/ml for hCG&bgr; (mean serum concentrations plus 3 SD, 99-7%confidence interval).Serum concentrations of holo-hCG, hCG&bgr;, and hCGa of 13
patients with confirmed testicular tumours were analysed in
retrospective long-term follow-up studies ranging between 6months and 1 year. The concentrations of all three analytes werestrikingly raised before chemotherapy was initiated. In agreementwith in vitro observations on two choriocarcinoma cell lines (BeWo,JAR) holo-hCG had the highest concentration, followed by hCG &bgr;and gCGot. The patients’ serum ratio of hCG(hCG&bgr;/hCG&agr; wasabout 100 to 1000/1/0.5, and remained approximately constant in allpatients, irrespective of whether the disease was in remission or not.The diagnostic value of the free subunits of hCG in comparison
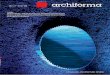
with the holo-hormone was further examined in 109 patients withhistologically, irnmunhistologically, and serologically confirmedtesticular cancer (33 seminomatous, 76 non-seminomatous).’ 43(57%) of non-seminomatous patients were holo-hCG-positive, 24(32%) were hCG(x-positive and 30 (40%) were hCG&bgr;-positive; weobserved a selective rise in the free ot-suburiit in 9 (12%) of patients,whereas only 1 patient presented with an augmentation of the free&bgr;-subunit alone. The percentage of marker-positive sera was raisedfrom 57% (holo-hCG measurement alone) to 70% by the additionof measurement of the free hCG-subunits (figure).
In seminomatous patients all three molecules were almost equallypotent markers: 5 (15%) patients showed positivity for holo-hCG, 7(21 %) for hCG 0, and 6 ( 18 %) for hCGot; in 19 (58%) of patients allthree markers remained within the physiological range. A rise in theserum concentration of one tumour marker alone was seen in 2 (6%)for holo-hCG, in 4 (12%) for hCG&bgr;, and in 5 (15%) for hCGot. Asin non-seminomatous patients, the additional analysis of free hCG&bgr;and free hCGa increased the proportion of tumour-marker-positivepatients from 15% (holo-hCG alone) to 42% (figure). Thediagnostic potency of the three markers in these two patient-groupsdiffered: holo-hCG was by far the most important marker innon-seminomatous patients, whereas all three markers were almostequally potent in patients with seminomatous tumours. Theproportion of tumour-marker-positive sera could be raised
substantially in both groups by the analysis of the free fx-subunit incombination with holo-hCG, compared with the singlemeasurement of holo-hCG or holo-hCG plus hCG&bgr;, as is usual inroutine tumour diagnosis.
Diagnostic sensitivities of hCG, free hCGct, and free hCG&bgr; asserumtumour markers in 33 patientswithseminomatous()and 76 with non-seminomatous ([]) testicular cancer.
None= negative for hCG, free hCGx, and free hCGp B
Our data clearly indicate the diagnostic usefulness of the serumanalysis of the free hCG-subunits in non-seminomatous and
especially in seminomatous patients, who generally lack othertumour markers such as alphafetoprotein.
Immunoendocrinology Research Unit,Austrian Academy of Sciences,Innsbruck, Austria
S. MADERSBACHERP. BERGER
Department of Internal Medicine II,Klinikum Grosshadern,University of Munich, West Germany K. MANN
Department of Internal Medicine,University of Vienna, Austria R. KUZMISTS
Institute for Generaland Experimental Pathology,
University of Innsbruck G. WICK
1. Hussa RO. Human chorionic gonadotropin, a clinical marker: review of its
biosynthesis. Ligand Rev 1981; 3 (suppl 2): 1-49.2. Cole LA, Hartle RJ, Lafferla JJ, Ruddon RW. Detection of the free &bgr;-subunit of
human chorionic gonadotropin in cultures of normal and malignant trophoblastcells, pregnancy sera, and sera of patients with chonocarcinoma. Endocrinology1983, 113: 1176-78.
3 Ozturk M, Bellet D, Manil L, Hennen G, Frydman R, Wands J. Physiological studiesof human chorionic gonadotropin, &agr;hCG, and &bgr;hCG as measured by specific monoclonal immunoradiometric assays. Endocrinology 1987; 120: 549-58
4. Saller B, Clara R, Spottl G, Siddle K, Mann K. Testicular cancer secretes intacthuman chorio gonadotropin (hCG) and its free &bgr;-subunit: evidence that hCG(+hCG&bgr;) assays are the most reliable m diagnosis and follow-up. Clin Chem 1989;35: 1-7.
5 Berger P, Klieber R, Panmoung W, Madersbacher S, Wolf H, Wick G. Monoclonalantibodies against free hCG subunits. J Endocrinol 1990; 125: 301-09.
Precautions with oral live typhoid (Ty 21a)vaccine
SIR,-The oral live typhoid vaccine Ty 21a (’Vivotef Berna’) hasrecently been licensed in the United States. It is given in the form ofone enteric-coated gelatin capsule containing attenuated Salmonellatyphi Ty 21a every other day for four doses. An identical vaccinemarketed abroad is given in a three-dose course. The protectionafforded by four doses of the vaccine is equal to that conferred by thehighly reactogenic heat/phenol-inactivated parenteral vaccine, theonly other widely available effective typhoid vaccine. The
parenteral vaccine requires two doses 4 weeks apart, with a boosterevery 3 years while exposure risk persists. Ty 2 la a vaccine has shownno discernible adverse reactions compared with the frequentadverse reactions experienced with the phenol-inactivated vaccine.1Ty 21a vaccine is the vaccine of choice for travellers to areas withincreased risk of typhoid fever.
Contraindications and warnings given in the package insert statethat the vaccine is not to be taken during an acute febrile illness or anacute gastrointestinal illness; and should not be given to individualson sulphonamides and antibiotics, or to those with a congenitalor acquired immunodeficiency, including patients on
immunosuppressive or antimitotic drugs. The insert also notes thatthe safety and efficacy of the vaccine has not been established inchildren under 6 years of age, and is not recommended for childrenof this age; that pregnant women should receive the vaccine only if itis clearly needed for protection; that all four doses must be taken inthe prescribed alternate-day scheme; and that the vaccine should bestored under refrigeration at all times.
In personal discussions, the manufacturer has made otherstatements not in the current package insert, which is beingreviewed by the US Food and Drug Administration (FDA).However, a revised package insert may not be ready for somemonths. Physicians prescribing Ty 21a vaccine for travellers maylike to have my personal recommendations, based on answers toquestions posed to the manufacturer (but not sanctioned by theFDA).
In an unpublished study from Austria, there seemed to be nosignificant difference in immune response between recipients of liveTy 21a vaccine and vaccine with standard amounts of chloroquineplus pyrimethamine/sulfadoxine. However, other unpublished datahave shown that antimalarials at high concentration can inhibitgrowth of Ty 21 a in vitro. The manufacturer recommends that 7

632
days should elapse between vaccination and initiation ofantimalarial prophylaxis; however, if combined use of these
products is initiated inadvertently, there may be no harm. Inpackage inserts abroad antimalarials are contraindicated withantibiotics and sulphonamides. When malaria prophylaxis isindicated and there is a time constraint with oral Ty 2 la vaccine use,priority must go to the use of antimalarial drugs. Although it isdesirable, and usually recommended, that malaria prophylaxis bestarted 1-2 weeks before arrival in a malarious area, this is notessential and drugs can be started on arrival. This may allow use ofTy 21a vaccine for travellers requiring antimalarials who can onlycomplete the vaccine series 7 days before arrival in a malarious area.
Another unpublished study from Austria showed thatadministration of Ty 21 a vaccine engenders a strong local interferonresponse in the gastrointestinal tract which may interfere with thetake of oral poliovaccine. The investigators recommend a 2-weekinterval after the final dose of Ty 21a vaccine before oral
poliovaccine is given. Should this interval not be available for thosewho need both vaccines, enhanced potency inactivated polio-vaccine can be used with no interference.
Simultaneous administration of yellowfever 17D vaccine with Ty21a vaccine did not diminish the antibody response to the
yellowfever vaccine. Antibody responses to Ty 21a vaccine in thissituation have not been determined.The manufacturer states that immune globulin would not be
expected to interfere with development of antibodies to Ty 21avaccine, although they have not given data directly applicable to thispoint. Immune globulin can be administered simultaneously withlive poliovaccine and yellowfever vaccine, but not with live measles,mumps, rubella vaccine.2
Traveler’s Medical Service,Suite 408, 2141 K Street NW,Washington, DC 20037, USA MARTIN S. WOLFE
1. Levine MM, Ferreccio C, Black RE, et al. Progress in vaccines against typhoid fever.Rev Infect Dis 1989; 11 (suppl 3): S552-567.
2. Centers for Disease Control. Health information for international travel, 1989. (DHSSPubl CDC 89-8280). Atlanta, CDC 1989, 71.
Does caffeine contribute to postoperativemorbidity?
SIR,-Chance remarks by patients made us, like Galletley andcolleagues,l consider that caffeine withdrawal might be relevant inpostoperative headache. 409 randomly selected day-case patientswho had minor procedures under local (LA) or general (GA)anaesthesia completed a questionnaire at time of discharge.Questions were asked about preoperative and postoperativeheadaches and their severity, proneness to headaches and migraine,regular caffeine intake, and the amount of caffeine which had beenomitted that day. Patients were starved from midnight and theprocedures took place the following morning. Headaches weregraded as mild if no analgesia was requested, or moderate/severe ifan analgesic was required. Headache proneness was recorded asnegative for less than 1 headache per month, or positive if morefrequent. Migraine was recorded if characteristic symptomsoccurred. Any combination with migraine was possible. Caffeineintake was calculated on the basis of the following assumptions (mgper cup): weak tea, 50; medium tea, 65; strong tea, 80; instant coffee,90; filtered coffee, 120; decaffeinated coffee, 3.2 Anaesthetic andpostoperative analgesic drugs were recorded but no attempt wasmade to control these. Data on caffeine intake were normalised bysquare root transformation. Data were analysed by chi-square andthe t test. Logistic progression was used to study simultaneously theeffect of predictors on occurrence of postoperative headache.Significance was taken as p < 0.005.Data were collected from 334 GA patients and 75 who had LA.
Mean (SD) age was 39 (16-3), and there was no significant agedifference between the LA and GA groups. There were 156 male
patients (381%), with significantly more men in the LA group(53-3%) and significantly less in the GA group (347%). Caffeineintake ranged from 0 to 3340 mg per day (median 490 mg). Caffeinemissed because of preoperative and postoperative fasting ranged
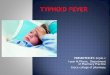
POSTOPERATIVE HEADACHE AND CAFFEINE INTAKE
from 0 to 1180 mg (median 220 mg). There was no significantdifference in caffeine intake between the LA and GA groups.Overall incidence of postoperative headache was 17-4%: 17 6% inthe LA group and 17-3% in the GA group. No significantcorrelation was found between postoperative headache and age,caffeine intake (table), caffeine missed, sex, postoperative use ofanalgesics, or any of the anaesthetic drugs (mainly propofol andalfentanil or fentanyl). A history of migraine was not significant.The only factor significantly associated with severity of headachewas sex, with women having more moderate/severe headaches(p < 005). For all patients the best predictor of postoperativeheadache was preoperative headache (p < 0,00 1), closely followedby proneness to headache (p<0’001): 43% of patients with
preoperative headache and 33 % of those who were headache pronecomplained of postoperative headache. The GA group had the sameresults, while in the LA group a history of migraine was the secondbest predictor (p<0’01). No other significant predictors of
postoperative headache were found. Specifically no correlation withcaffeine intake or omission could be shown.Headache is one of the most common complaints following
day-case surgery3 but its cause remains obscure. Previous studieshave related it to female sex,3.4 age,5 dehydration lack of sedativepremedication,7 volatile anaesthetic agents,8 and caffeine intake.None of these factors has been confirmed. Bell et al9 found thatbreakfast helped while preoperative intravenous dextrose did not.The only factor which is reliably related to postoperative headacheis proneness to headaches.5,7,9,10 Our finding that headache with LAwas similar to that with GA would appear to exonerate generalanaesthesia as a factor. We have not found the relation betweencaffeine and postoperative headache described by Galletley et al.1The only firm conclusion that can be drawn is that if you are proneto headaches or have a preoperative headache you will be prone topostoperative headache.
We are grateful to Dr E. A. van der Velde, Rijksuniveriteit, Leiden,Netherlands, for statistical analyses.
Leiden University,Netherlands FRANCINE H. VERHOEFF
Radcliffe Infirmary,Oxford OX2 6HE, UK JEAN M. MILLAR
1. Galletley DC, Fennelly M, Whitwan JG. Does caffeine withdrawal contribute topostanaesthetic morbidity? Lancet 1989; i: 1335.
2 Greden JF. Anxiety or caffeinism. a diagnostic dilemma. Am J Psychiatry 1974; 131:1089-92.
3. Fahy A, Marshall M. Postanaesthetic morbidity in outpatients. Br J Anaesthesiol 1969;41: 433-38.
4. Ogg TW. An assessment of postoperative outpatient cases. Br Med J 1972; iv: 573-765. Faithfull NS Factors affecting headache following anaesthesia for urological daycase
surgery. Br J Anaesthesiol 1989; 63: 220-21P.6. Keane P, Murray P. Intravenous fluids in minor surgery: their effect on recovery from
anaesthesia. Anaesthesia 1986; 41: 635-37.7 Hannington-Kiff JG. Headache before and after operation in gynaecological patients
Br J Anaesthesiol 1969; 41: 401-05.8 Jones DF. Recovery from day case anaesthesia, companson of a further four
techniques including use of the new induction agent diprivan Br J Ananthesiol1982, 54: 629-32.
9. Bell PF, Hawthorne P, Lavery GG, et al. Influence of fasting on postoperativeheadache in day-stay patients. Br J Anaesthesiol 1987; 59: 934P
10. McDowall SA, Dundee JW, Pandit SK. Para-anaesthetic headache in female patientsAnaesthesia 1970; 25: 334-40.