Embed Size (px)
Citation preview
Pre-Cancerous Skin Lesions
& Skin Cancer
Ian D.R. Landells, MD, FRCPCClinical Associate Professor
Memorial University of NewfoundlandMedical Director Dermatology
Nexus Clinical ResearchSt. John’s, NL
Canada
Copyright © 2017 by Sea Courses Inc.
All rights reserved. No part of this document may be
reproduced, copied, stored, or transmitted in any form or
by any means – graphic, electronic, or mechanical,
including photocopying, recording, or information storage
and retrieval systems without prior written permission of
Sea Courses Inc. except where permitted by law.
Sea Courses is not responsible for any speaker or
participant’s statements, materials, acts or omissions.
Learning Objectives
• After attending this session, participants will be
able to:
– Explain the link between actinic keratoses (AKs) and
non-melanoma skin cancers (NMSCs)
– Describe current treatment options for Aks,
– Discuss the features of squamous cell carcinoma
– Discuss the features of basal cell carcinoma
– Discuss the features of dysplastic nevi and melanoma
Actinic Keratoses and NMSC
• AK is a pre-cancerous skin lesion1,2
• AKs may progress to squamous cell carcinoma
(SCC),
a type of NMSC3-5
– SCC can be in situ (Bowen’s disease) or invasive
– NMSC is the most common type of cancer6
• The other type of NMSC is basal cell carcinoma
(BCC)
1. Criscione VD, et al. Cancer. 2009;115(11):2523-30. 2. Lober BA, et al. South Med J. 2000;93:650-5.
3. Marks R, et al. Lancet. 1988;1:795-7. 4. Mittelbronn MA, et al. Int J Dermatol. 1998;37:677-81.
5. Dinehart SM, et al. Cancer. 1997;79:920-3. 6. Rogers HW, et al. Arch Dermatol. 2010;146(3):283-7.
Actinic Keratoses and NMSC
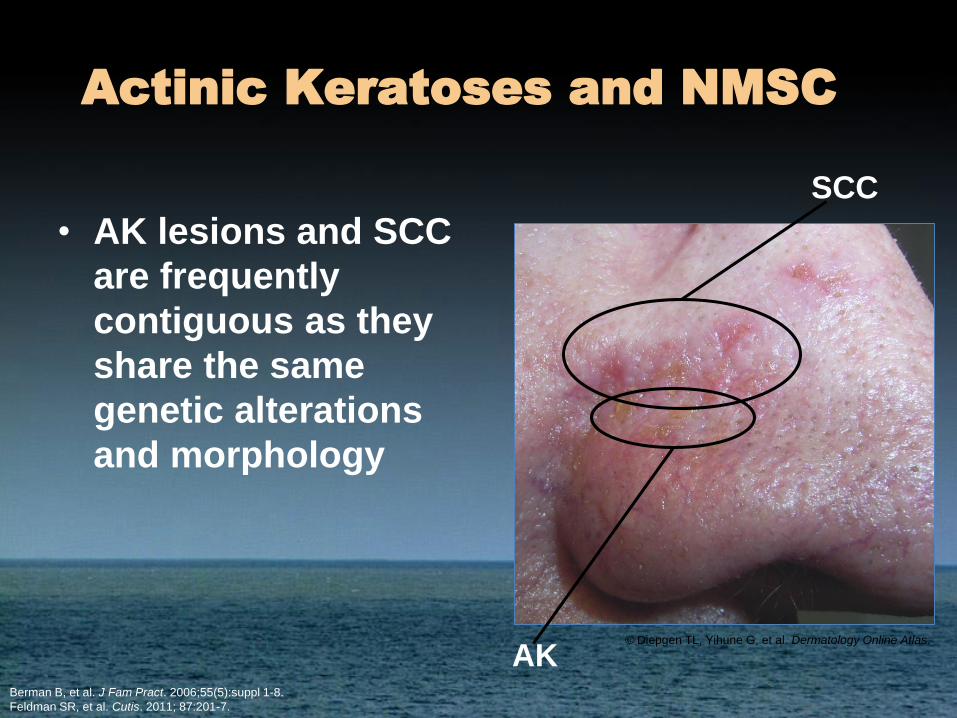
• AK lesions and SCC
are frequently
contiguous as they
share the same
genetic alterations
and morphology
Berman B, et al. J Fam Pract. 2006;55(5):suppl 1-8.
Feldman SR, et al. Cutis. 2011; 87:201-7.
SCC
AK© Diepgen TL, Yihune G, et al. Dermatology Online Atlas.
Natural History of AKs
• Natural course of AKs is unpredictable1-5
– Estimates of 40% to 80% of cutaneous SCCs
arise from, or near, AKs2-5
• AKs may persist, regress, or progress1,3
– Some lesions that regress will recur, from 32%
within
1 year to 92% within 5 years
– Progression identified as hypertrophic AK, SCC in
situ (Bowen’s disease), and/or invasive SCC
1. Criscione VD, et al. Cancer. 2009;115(11):2523-30.
2. Feldman SR, et al. Cutis. 2011;87(4):201-7.
3. Marks R, et al. Lancet. 1988;1(8589):795-7.
4. Mittelbronn MA, et al. Int J Dermatol. 1998;37:677-81.
5. Dinehart SM, et al. Cancer. 1997;79:920-3.
What factors put patients at risk of AKs?
• What questions should you ask patients to determine AK risk
factors?
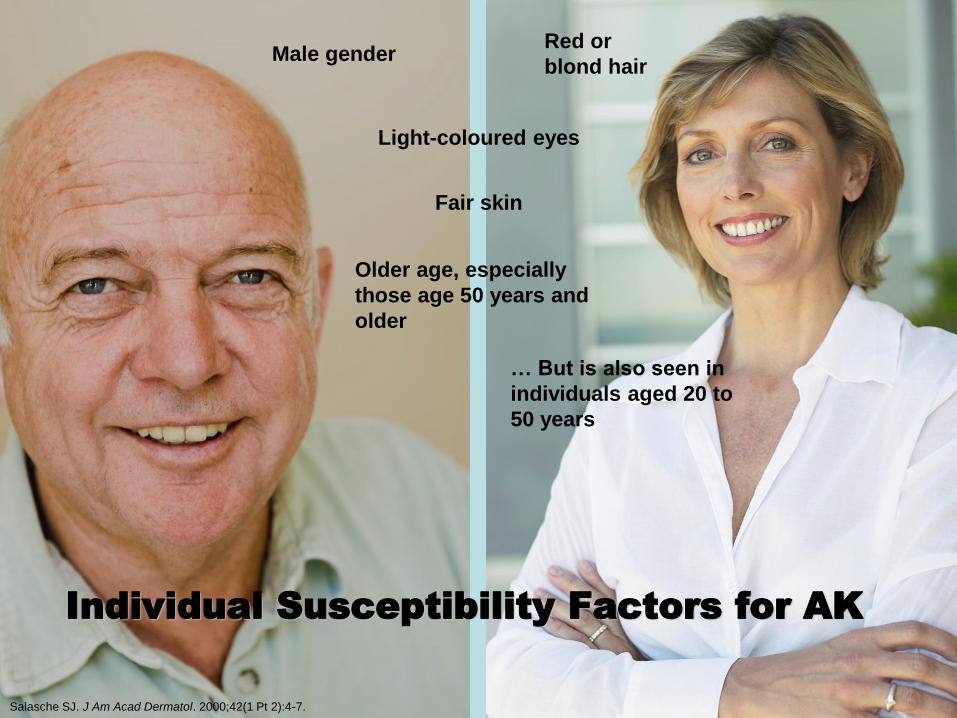
Male gender
… But is also seen in
individuals aged 20 to
50 years
Older age, especially
those age 50 years and
older
Fair skin
Red or
blond hair
Light-coloured eyes
Individual Susceptibility Factors for AK
Salasche SJ. J Am Acad Dermatol. 2000;42(1 Pt 2):4-7.
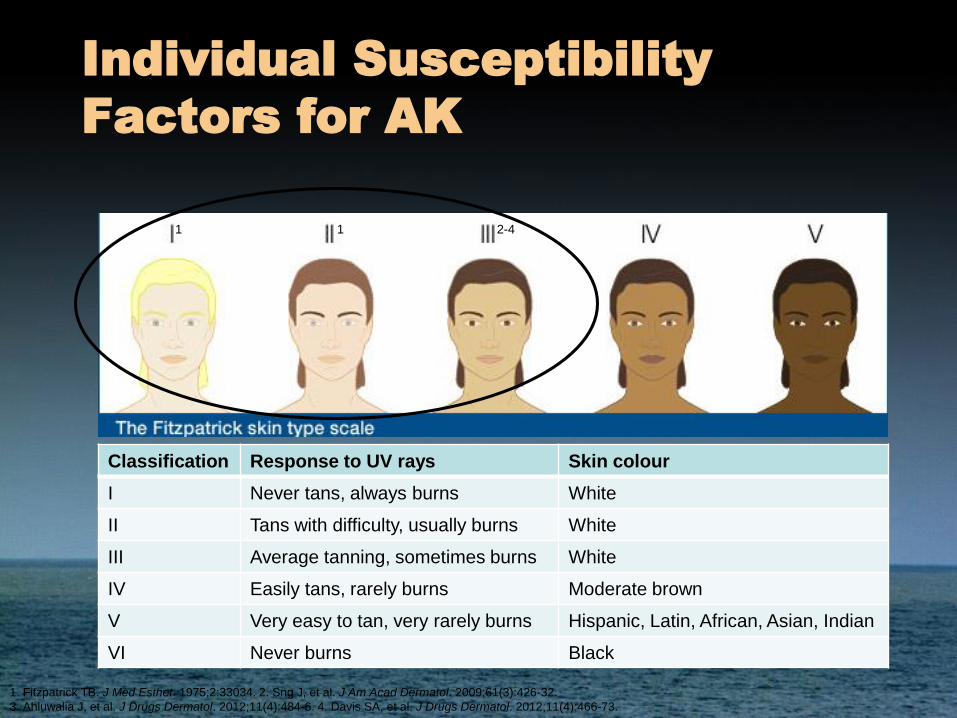
Individual Susceptibility
Factors for AK
Classification Response to UV rays Skin colour
I Never tans, always burns White
II Tans with difficulty, usually burns White
III Average tanning, sometimes burns White
IV Easily tans, rarely burns Moderate brown
V Very easy to tan, very rarely burns Hispanic, Latin, African, Asian, Indian
VI Never burns Black
1. Fitzpatrick TB. J Med Esthet. 1975;2:33034. 2. Sng J, et al. J Am Acad Dermatol. 2009;61(3):426-32.
3. Ahluwalia J, et al. J Drugs Dermatol. 2012;11(4):484-6. 4. Davis SA, et al. J Drugs Dermatol. 2012;11(4):466-73.
1 1 2-4
General Risk Factors for AKs
• High intensity or cumulative exposure to UV
radiation1-3
– Sunburns easily, history of severe or blistering sunburn
– Use of tanning beds or sunlamps
– Sun vacations, lived in sunny location, “snowbirds”
– Outdoor occupation
– Outdoor hobbies, e.g., golf, skiing, sailing
– Light therapy or phototherapy for treatment of skin
conditions, e.g., psoriasis
• Prior history of AKs or other skin cancer4
1. Diepgen TL, et al. Br J Dermatol.2002;146(suppl 61):1-6.
2. Berman B, et al. J Fam Pract. 2006;55(5):suppl 1-8.
3. Hemminki K, et al. Arch Dermatol. 2003;139:885-9.
4. Feldman SR, et al. Cutis. 2011;87(4):201-7.
General Risk Factors for AKs
(cont’d)
• Clinical signs of photodamage, such as solar/senile
lentigines, facial telangiectasia, and solar elastosis of the
neck1
• Immunosuppression2
– Organ transplantation
– Immunosuppressive drugs, e.g., abatacept, azathioprine,
basiliximab, ciclosporin, glucocorticoids, infliximab, mycophenolate
mofetil, tacrolimus
– HIV
• Human papillomaviruses may play a role in the etiology
of AKs2
– Strongest association in immunosuppressed patients, particularly
organ transplant recipients
1. Feldman SR, et al. Cutis. 2011;87(4):201-7.
2. Goldberg LH, et al. J Drugs Dermatol. 2010;9(9):1125-32.

Clinical Signs of Photodamage
Facial telangiectasia
Solar elastosis of the neck Solar/senile lentigines©
Die
pg
en
TL
, Y
ihu
ne
G,
et
al.
Derm
ato
log
y O
nlin
e A
tla
s.
© D
an
de
rm
© D
an
de
rm
Clinical Signs
of Actinic Keratoses
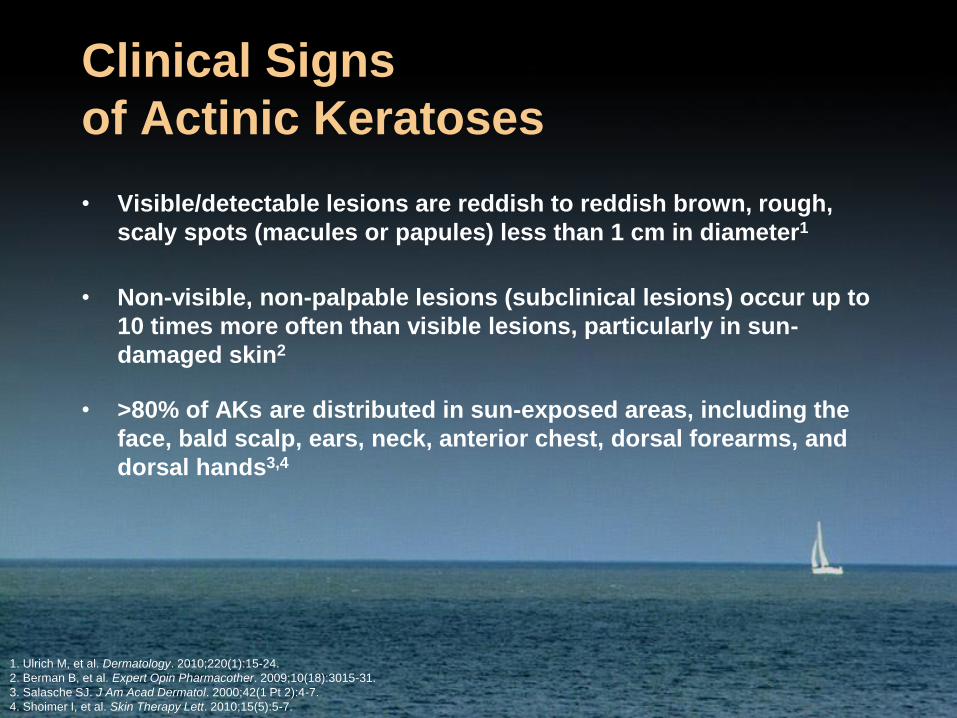
• Visible/detectable lesions are reddish to reddish brown, rough,
scaly spots (macules or papules) less than 1 cm in diameter1
• Non-visible, non-palpable lesions (subclinical lesions) occur up to
10 times more often than visible lesions, particularly in sun-
damaged skin2
• >80% of AKs are distributed in sun-exposed areas, including the
face, bald scalp, ears, neck, anterior chest, dorsal forearms, and
dorsal hands3,4
1. Ulrich M, et al. Dermatology. 2010;220(1):15-24.
2. Berman B, et al. Expert Opin Pharmacother. 2009;10(18):3015-31.
3. Salasche SJ. J Am Acad Dermatol. 2000;42(1 Pt 2):4-7.
4. Shoimer I, et al. Skin Therapy Lett. 2010;15(5):5-7.
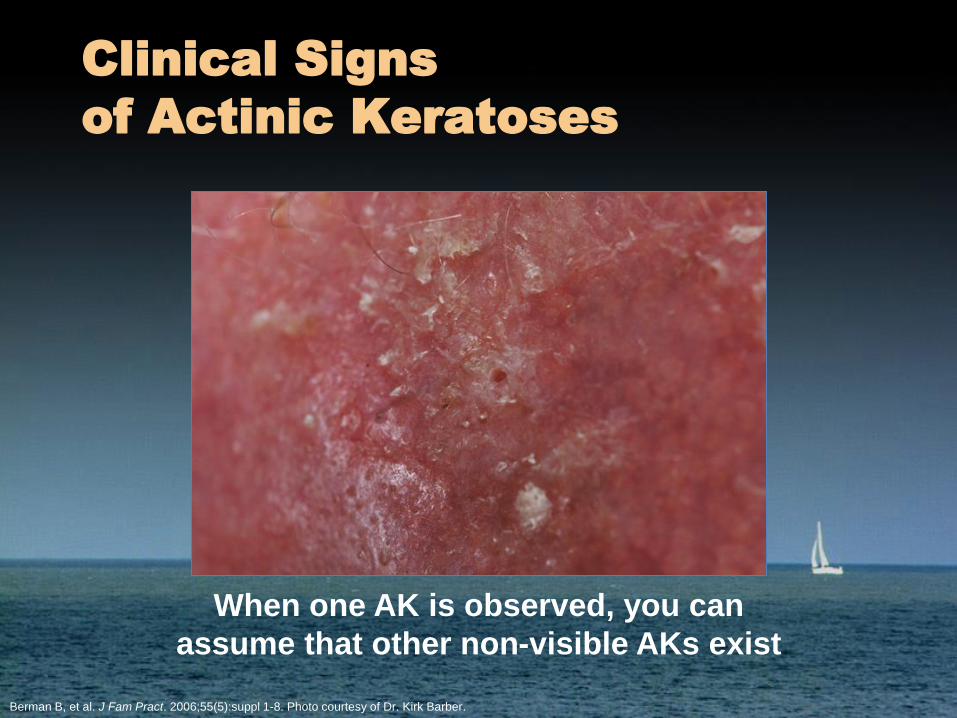
Clinical Signs
of Actinic Keratoses
When one AK is observed, you can
assume that other non-visible AKs exist
Berman B, et al. J Fam Pract. 2006;55(5):suppl 1-8. Photo courtesy of Dr. Kirk Barber.
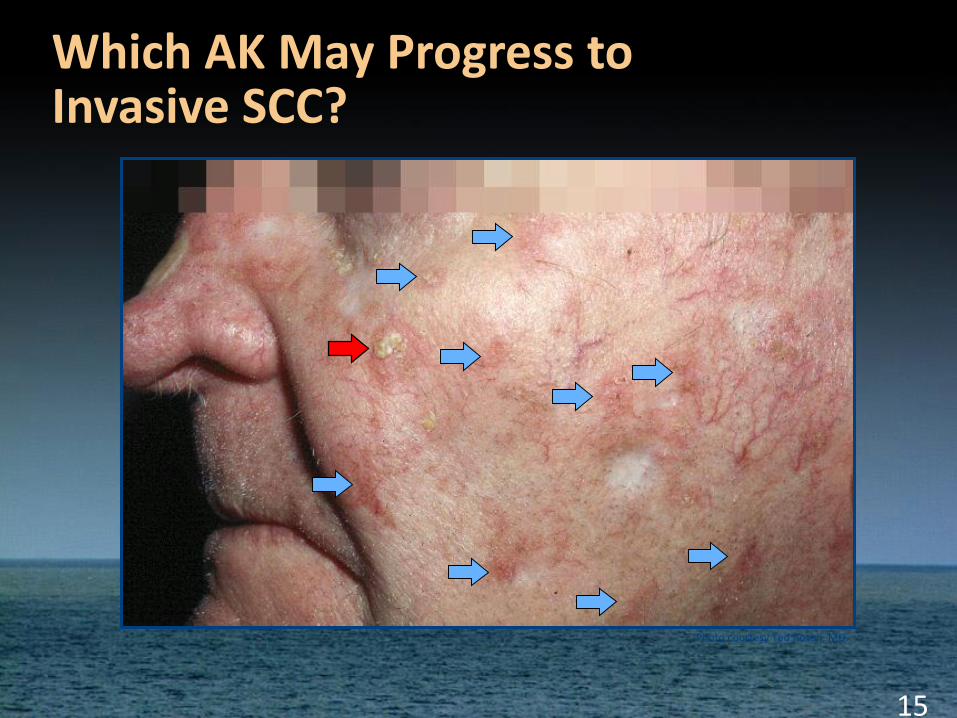
15
Photo courtesy Ted Rosen, MD.
Which AK May Progress to Invasive SCC?
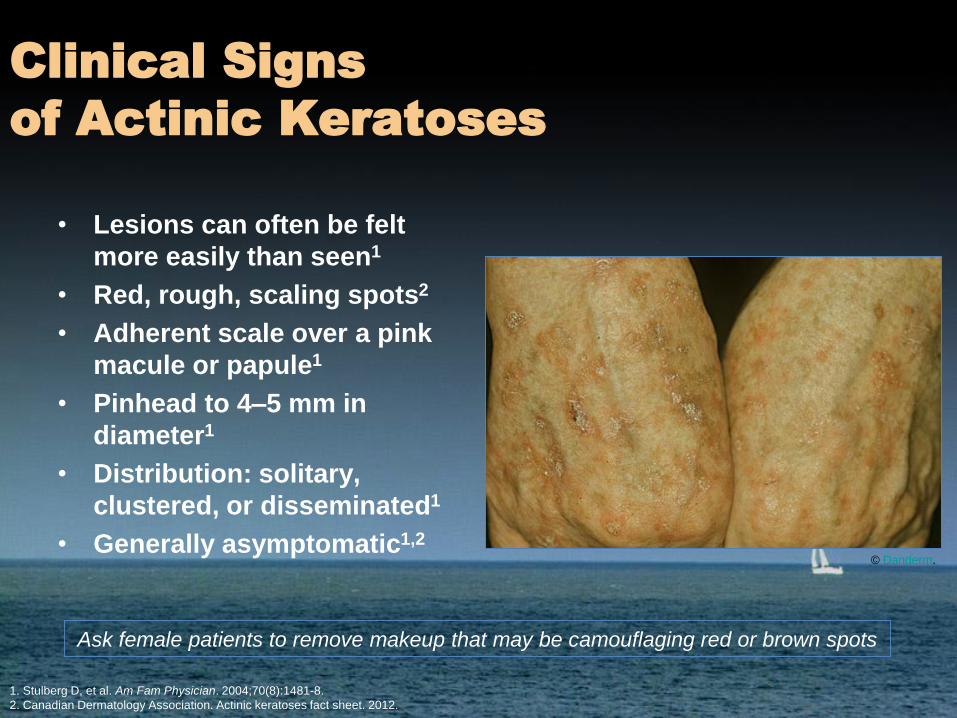
• Lesions can often be felt
more easily than seen1
• Red, rough, scaling spots2
• Adherent scale over a pink
macule or papule1
• Pinhead to 4–5 mm in
diameter1
• Distribution: solitary,
clustered, or disseminated1
• Generally asymptomatic1,2
1. Stulberg D, et al. Am Fam Physician. 2004;70(8):1481-8.
2. Canadian Dermatology Association. Actinic keratoses fact sheet. 2012.
© Danderm.
Clinical Signs
of Actinic Keratoses
Ask female patients to remove makeup that may be camouflaging red or brown spots
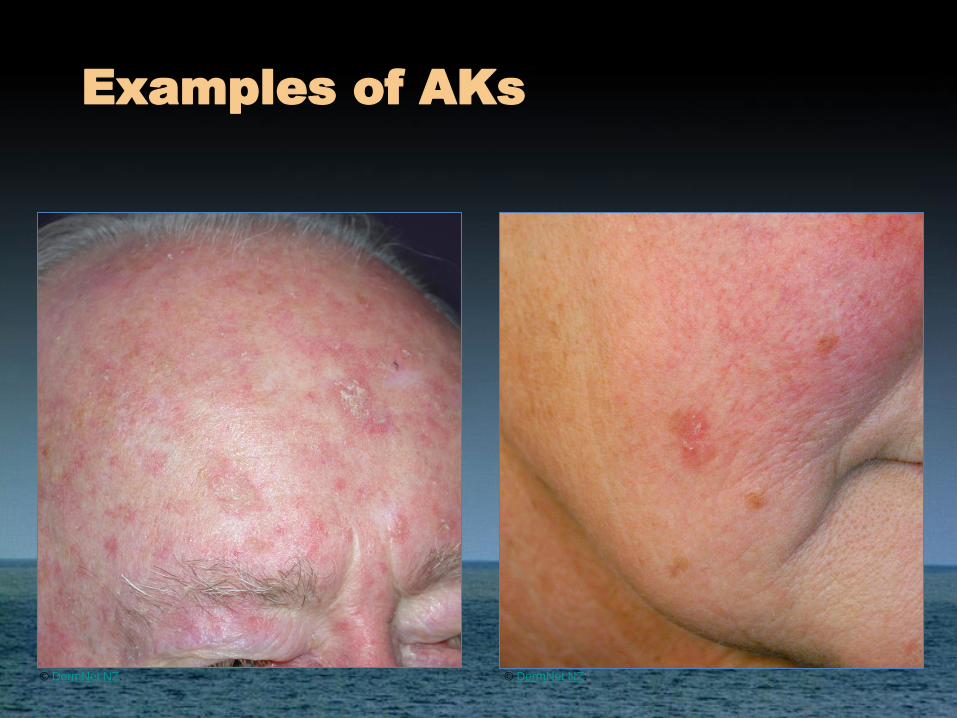
Examples of AKs
© DermNet NZ. © DermNet NZ.

Examples of AKs
© DermNet NZ.
© DermNet NZ.
© DermNet NZ.
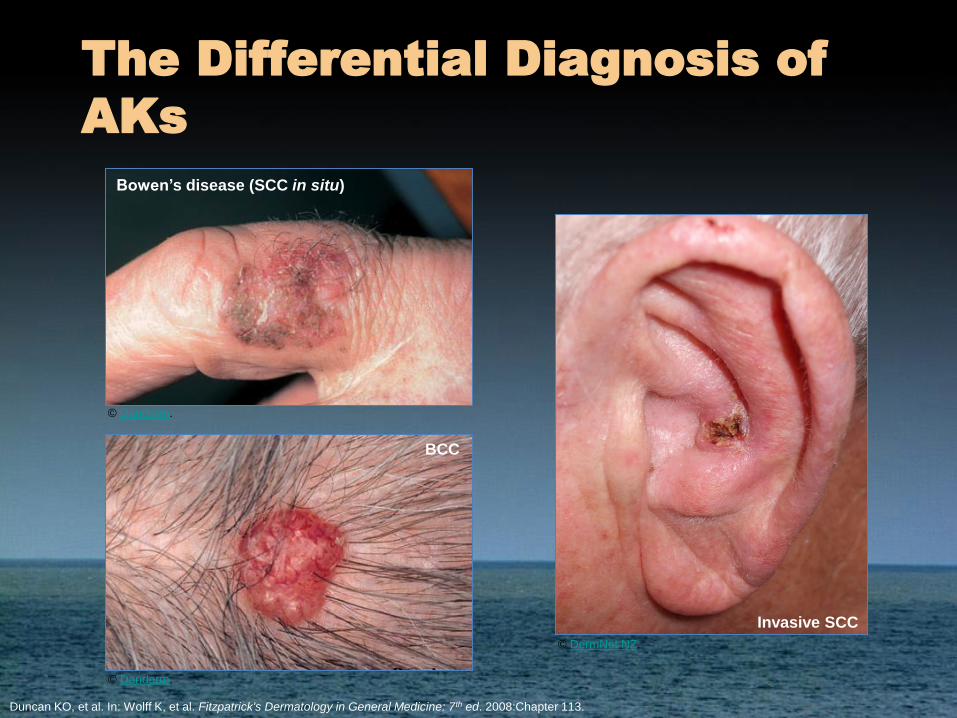
The Differential Diagnosis of
AKs
BCC
Bowen’s disease (SCC in situ)
Invasive SCC
Duncan KO, et al. In: Wolff K, et al. Fitzpatrick's Dermatology in General Medicine: 7th ed. 2008:Chapter 113.
© Danderm.
© DermNet NZ.
© Danderm.
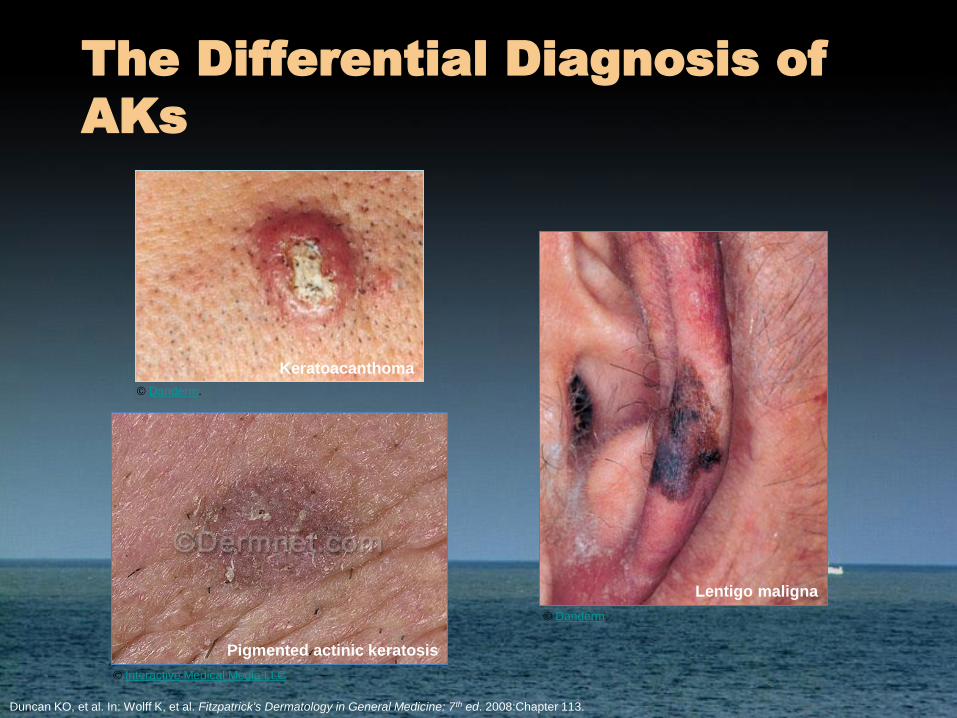
The Differential Diagnosis of
AKs
Keratoacanthoma
Lentigo maligna
Duncan KO, et al. In: Wolff K, et al. Fitzpatrick's Dermatology in General Medicine: 7th ed. 2008:Chapter 113.
Pigmented actinic keratosis
© Danderm.
© Interactive Medical Media LLC.
© Danderm.
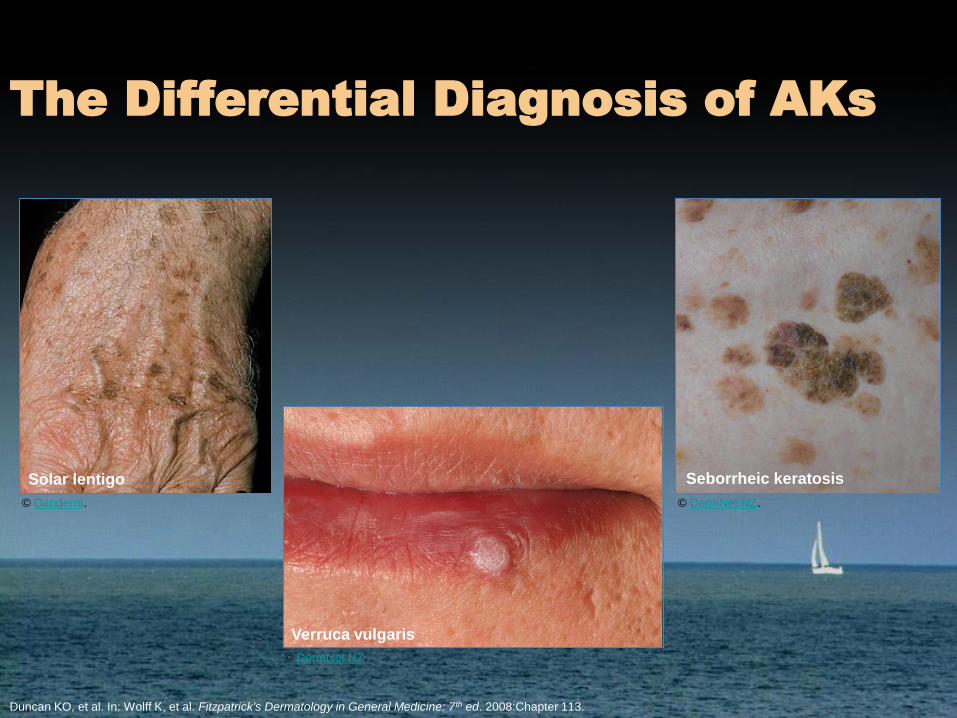
The Differential Diagnosis of AKs
Solar lentigo
Verruca vulgaris
Seborrheic keratosis
Duncan KO, et al. In: Wolff K, et al. Fitzpatrick's Dermatology in General Medicine: 7th ed. 2008:Chapter 113.
© Danderm.
© DermNet NZ.
© DermNet NZ.
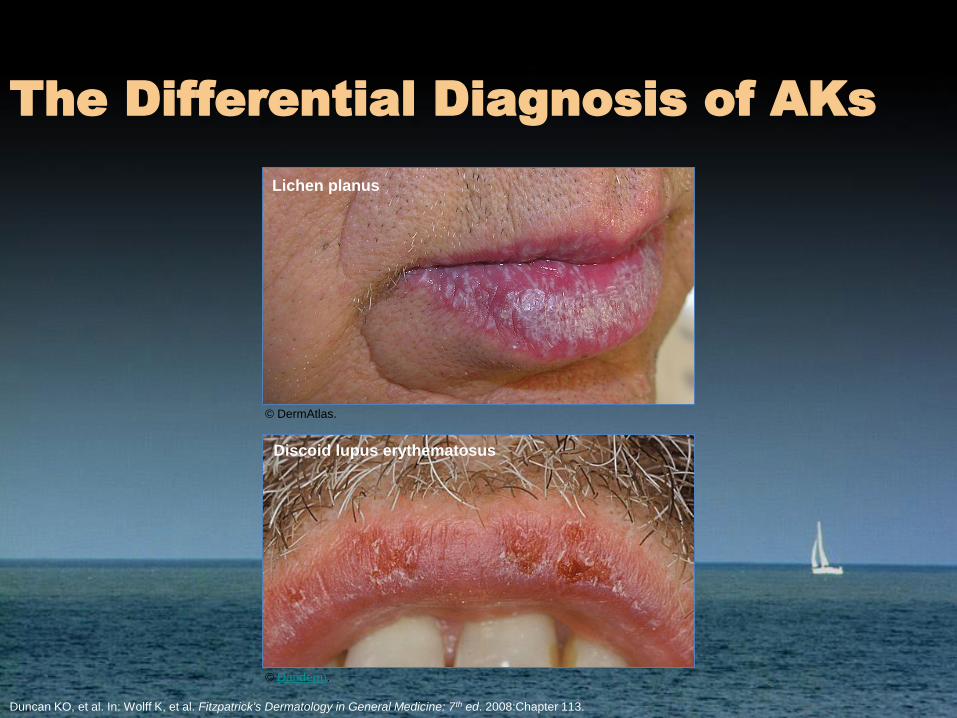
The Differential Diagnosis of AKs
Lichen planus
Discoid lupus erythematosus
Duncan KO, et al. In: Wolff K, et al. Fitzpatrick's Dermatology in General Medicine: 7th ed. 2008:Chapter 113.
© Danderm.
© DermAtlas.
What is the rationale for prompt
treatment of AKs?
Actinic Keratosis is a
Field Disease
• Field of cancerisation surrounds clinical AKs and
can be clinically invisible with multifocal,
paraneoplastic, subclinical changes1
• Histopathology of AK is found in surrounding
skin2
• Subclinical (non-palpable, non-visible) AK lesions
occur ~10 times more often than clinical AK
lesions in sun-damaged skin3
1. Vatve M, et al. Br J Dermatol. 2007;157(Suppl 2):21-4.
2. Berman B, et al. Exp Opin Pharmacother. 2009;10(18):3015-31.
3. Braakhuis BJM, et al. Cancer Res. 2003;63(8):1727-30.
25
Field Cancerization: A Key Concept Driving Treatment Choices for AK1,2
• In addition to visible AKs, the surrounding area (“field”) of sun-damaged skin may contain subclinical AKs• This results from UV-induced
damage over an extended area, termed “field cancerization”
• Therefore, an AK lesion is the “tip of the iceberg”
1. Slaughter DP, et al. Cancer. 1953;6:963-968; 2. Quatresooz P, et al. Eur J Dermatol. 2008;18:6-10.
© iStockphoto.com/Alexander Soloviev
26
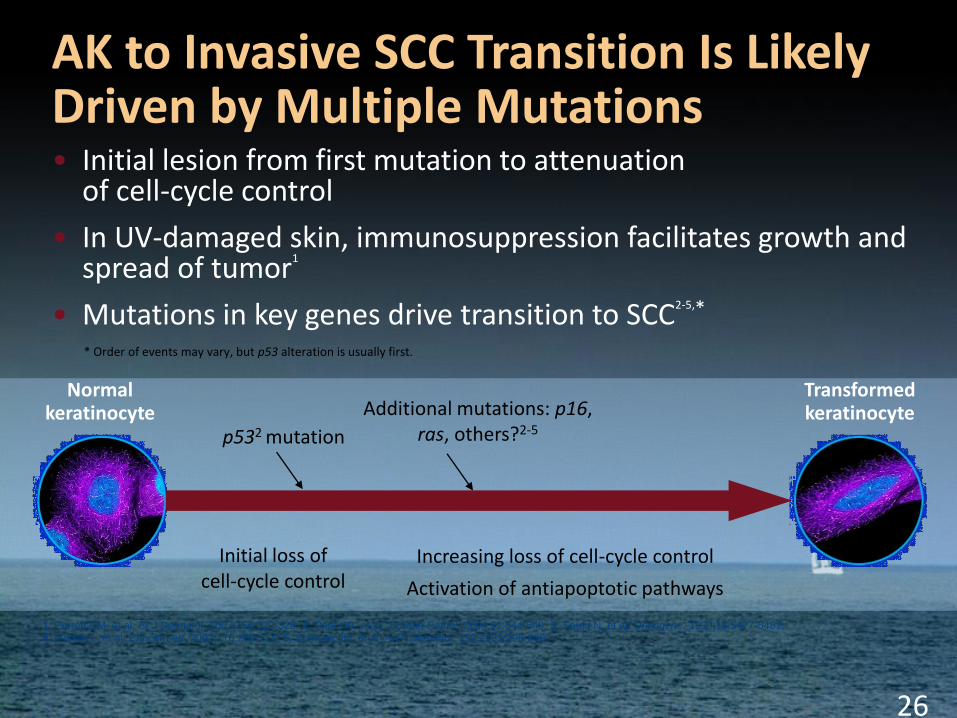
AK to Invasive SCC Transition Is Likely Driven by Multiple Mutations• Initial lesion from first mutation to attenuation
of cell-cycle control
• In UV-damaged skin, immunosuppression facilitates growth and spread of tumor1
• Mutations in key genes drive transition to SCC2-5,*
1. Perrett CM, et al. Br J Dermatol. 2007;156:320-328; 2. Park HR, et al. J Cutan Pathol. 2004;31:544-549; 3. Soufir N, et al. Oncogene. 1999;18:5477-5481;
4. Mortier L, et al. Cancer Lett. 2002;176:205-214; 5. Spencer JM, et al. Arch Dermatol. 1995;131:796-800.
p532 mutation
Initial loss of cell-cycle control
Additional mutations: p16, ras, others?2-5
Increasing loss of cell-cycle control
Activation of antiapoptotic pathways
Normal keratinocyte
Transformed keratinocyte
* Order of events may vary, but p53 alteration is usually first.
27
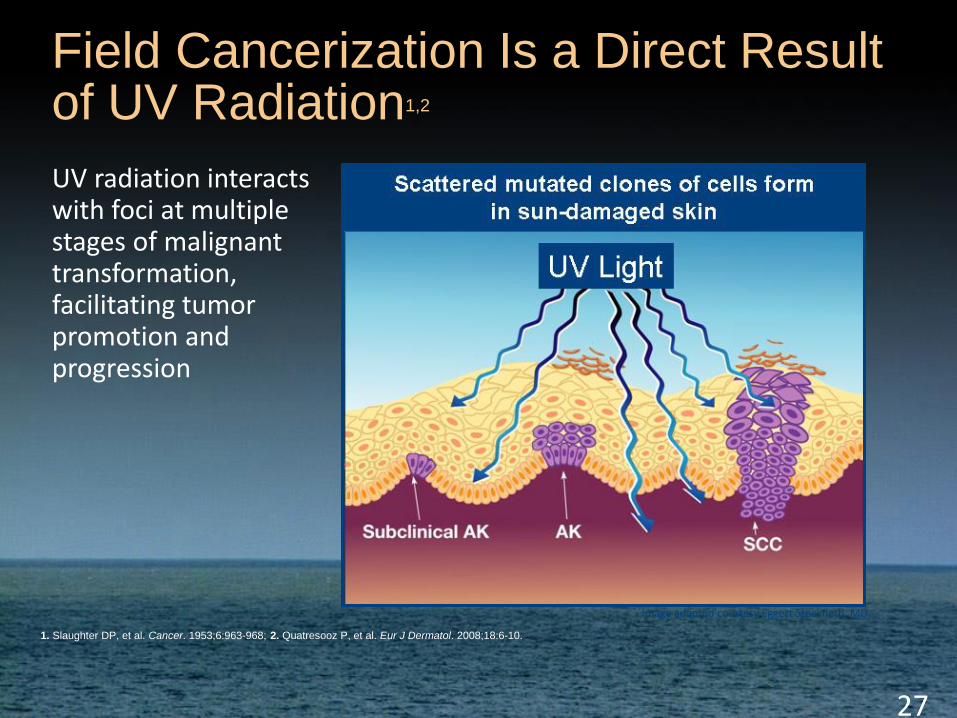
Field Cancerization Is a Direct Result of UV Radiation1,2
UV radiation interacts with foci at multiple stages of malignant transformation, facilitating tumor promotion and progression
1. Slaughter DP, et al. Cancer. 1953;6:963-968; 2. Quatresooz P, et al. Eur J Dermatol. 2008;18:6-10.
Image adapted courtesy Eggert Stockfleth, MD.
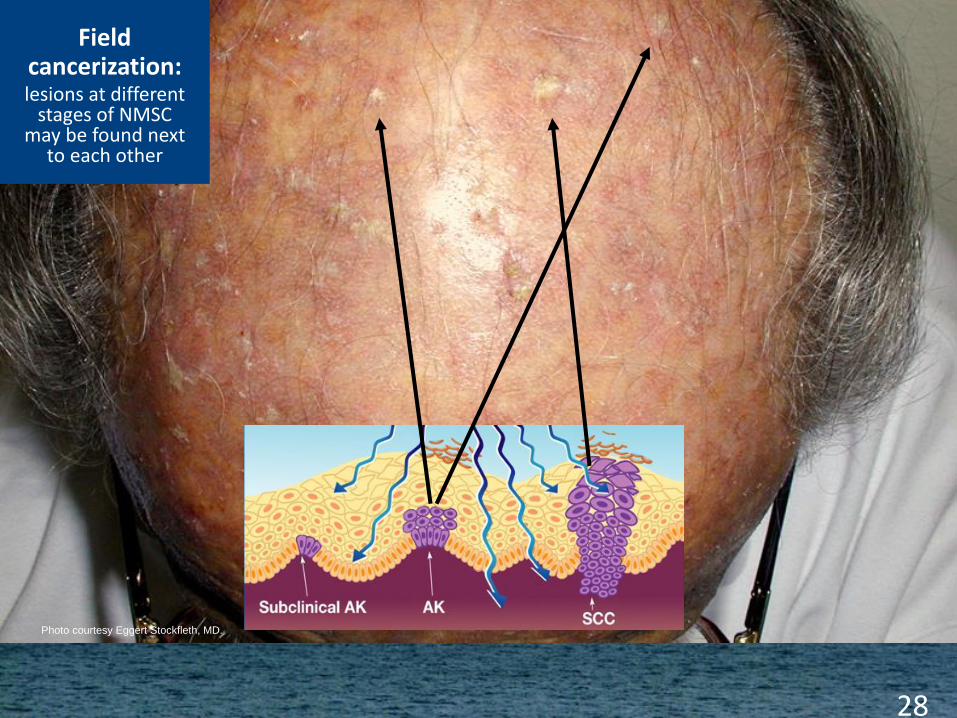
Photo courtesy Eggert Stockfleth, MD.
Field cancerization:lesions at different
stages of NMSC may be found next
to each other
28
Lesion-directed Treatments:
Physically Destructive Methods
• Place in therapy: scattered AKs, AKs limited in number, thick,
hyperkeratotic AKs, patients non-adherent to topical regimens1,2
• Cryotherapy with liquid nitrogen is most common method1,2
– Standard treatment for isolated AK lesions, especially small lesions
with well demarcated borders3
– Thin lesions may respond better than thick lesions3
– Freeze times determine response: 39% for <5 seconds, 83% for
>20 seconds at 3-month follow-up2,3
• Electrodesiccation
– Best applied to well demarcated, non-invasive tumours2
1. Shoimer I, et al. Skin Therapy Lett. 2010;15(5):5-7.
2. Han A, et al. J Drugs Dermatol. 2010;9(7):864-9.
3. Berman B, et al. J Fam Pract. 2006;55(5):suppl 1-8.
Lesion-directed Treatments:
Surgical Removal
• Shave excision or curettage ± electrodesiccation1-3
• Place in therapy: individual AKs, well demarcated,
non-invasive tumours; biopsy required to rule out
frank carcinoma; hypertrophic AKs refractory to other
treatments1,3
• May be followed by electrocautery to destroy
additional atypical cell layers and provide
hemostasis2
• No documented cure rates with these treatments2
1. Shoimer I, et al. Skin Therapy Lett. 2010;15(5):5-7.
2. de Berker D, et al. Br J Dermatol. 2007;156:222-30.
3. Berman B, et al. J Fam Pract. 2006;55(5):suppl 1-8.
Is Field Therapy the
Necessary Approach?
• It is impossible to know which AKs will progress to
invasive SCC, so it is recommended that all AKs be
treated1
• The ultimate goal of treatment is to clear the entire
actinically damaged field2
– Addressing both clinical and non-visible lesions may
significantly reduce recurrence rates of AKs2
• Early diagnosis and treatment of the field of actinic
damage decreases overall disease burden and helps
to prevent development of invasive SCC1,2
1. Martin G. J Clin Aesthet Dermatol. 2010;3(11):20-5.
2. Ulrich M, et al. Exp Opin Emerg Drugs. 2010;15(4):545-55.
Field-directed Topical
Therapy Options
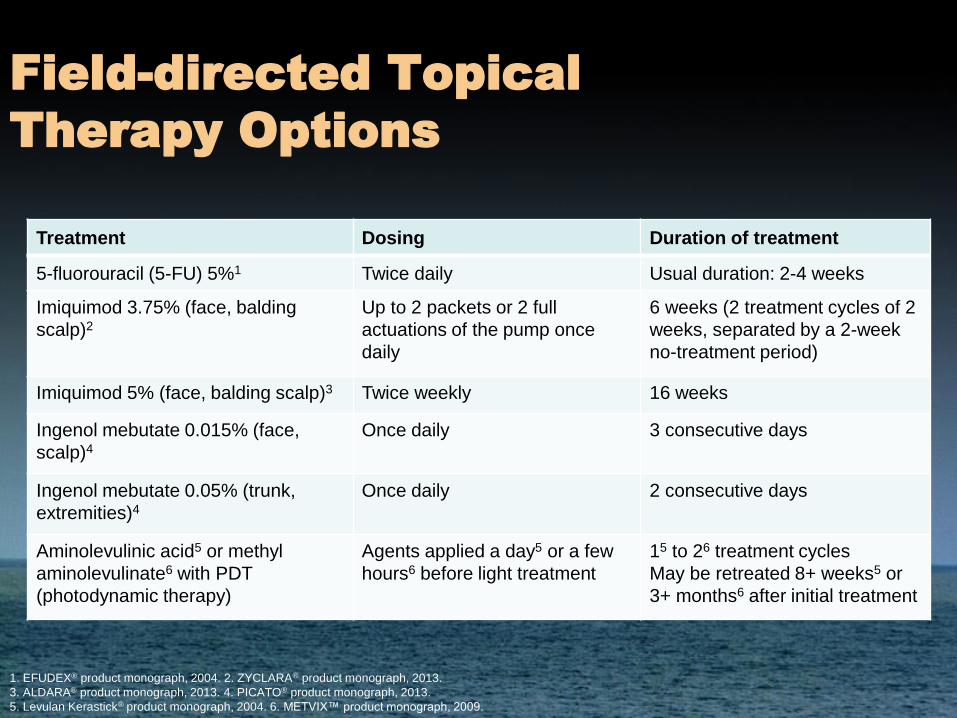
Treatment Dosing Duration of treatment
5-fluorouracil (5-FU) 5%1 Twice daily Usual duration: 2-4 weeks
Imiquimod 3.75% (face, balding
scalp)2
Up to 2 packets or 2 full
actuations of the pump once
daily
6 weeks (2 treatment cycles of 2
weeks, separated by a 2-week
no-treatment period)
Imiquimod 5% (face, balding scalp)3 Twice weekly 16 weeks
Ingenol mebutate 0.015% (face,
scalp)4
Once daily 3 consecutive days
Ingenol mebutate 0.05% (trunk,
extremities)4
Once daily 2 consecutive days
Aminolevulinic acid5 or methyl
aminolevulinate6 with PDT
(photodynamic therapy)
Agents applied a day5 or a few
hours6 before light treatment
15 to 26 treatment cycles
May be retreated 8+ weeks5 or
3+ months6 after initial treatment
1. EFUDEX® product monograph, 2004. 2. ZYCLARA® product monograph, 2013.
3. ALDARA® product monograph, 2013. 4. PICATO® product monograph, 2013.
5. Levulan Kerastick® product monograph, 2004. 6. METVIX™ product monograph, 2009.
Combination/Sequential
Therapy
• Cryotherapy or curettage to treat visible AKs +
topical treatment to treat underlying field
cancerisation:
– 5-fluorouracil (5-FU) 5% followed by cryotherapy1
– Cryotherapy followed by imiquimod 3.75%2
– Cryotherapy followed by ingenol mebutate 0.015% on face
or scalp3
1. Jorizzo J, et al. Arch Dermatol. 2004;140:813-6.
2. Jorizzo J, et al. J Drugs Dermatol. 2010;9:1101-8.
3. Swanson N, et al. 22nd EADV Congress. Abstract P532; IST13-1514.
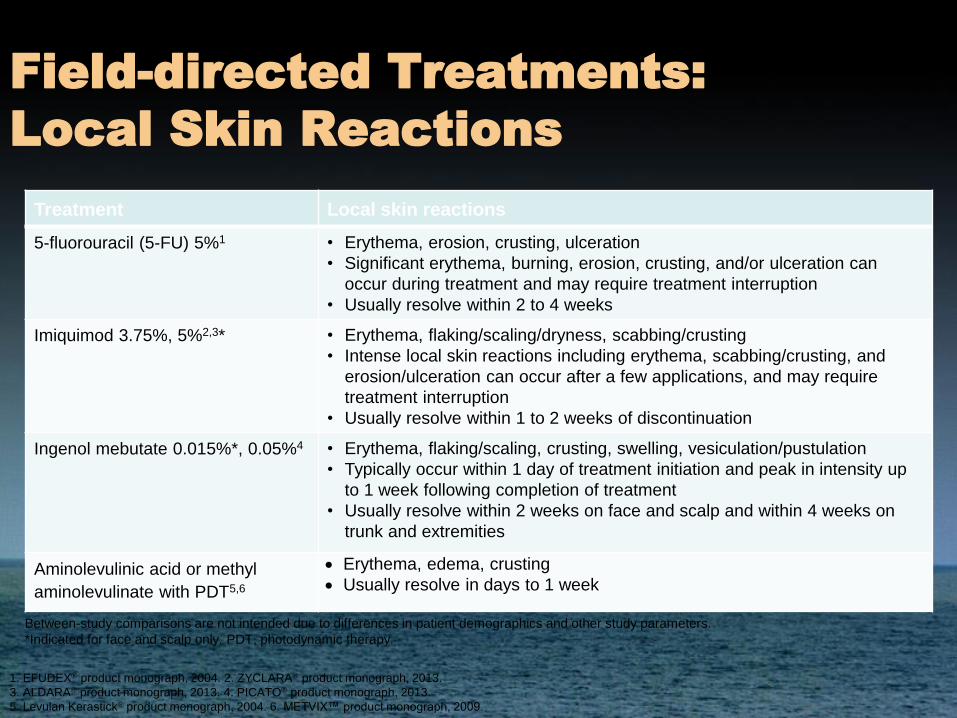
Field-directed Treatments:
Local Skin Reactions
Treatment Local skin reactions
5-fluorouracil (5-FU) 5%1 • Erythema, erosion, crusting, ulceration
• Significant erythema, burning, erosion, crusting, and/or ulceration can
occur during treatment and may require treatment interruption
• Usually resolve within 2 to 4 weeks
Imiquimod 3.75%, 5%2,3* • Erythema, flaking/scaling/dryness, scabbing/crusting
• Intense local skin reactions including erythema, scabbing/crusting, and
erosion/ulceration can occur after a few applications, and may require
treatment interruption
• Usually resolve within 1 to 2 weeks of discontinuation
Ingenol mebutate 0.015%*, 0.05%4 • Erythema, flaking/scaling, crusting, swelling, vesiculation/pustulation
• Typically occur within 1 day of treatment initiation and peak in intensity up
to 1 week following completion of treatment
• Usually resolve within 2 weeks on face and scalp and within 4 weeks on
trunk and extremities
Aminolevulinic acid or methyl
aminolevulinate with PDT5,6
• Erythema, edema, crusting
• Usually resolve in days to 1 week
1. EFUDEX® product monograph, 2004. 2. ZYCLARA® product monograph, 2013.
3. ALDARA® product monograph, 2013. 4. PICATO® product monograph, 2013.
5. Levulan Kerastick® product monograph, 2004. 6. METVIX™ product monograph, 2009.
Between-study comparisons are not intended due to differences in patient demographics and other study parameters.
*Indicated for face and scalp only. PDT, photodynamic therapy.

Examples of Local Skin
Reactions
This LSR comprises erythema,
vesiculation, and mild swelling.
This LSR comprises more pronounced
swelling and erythema.
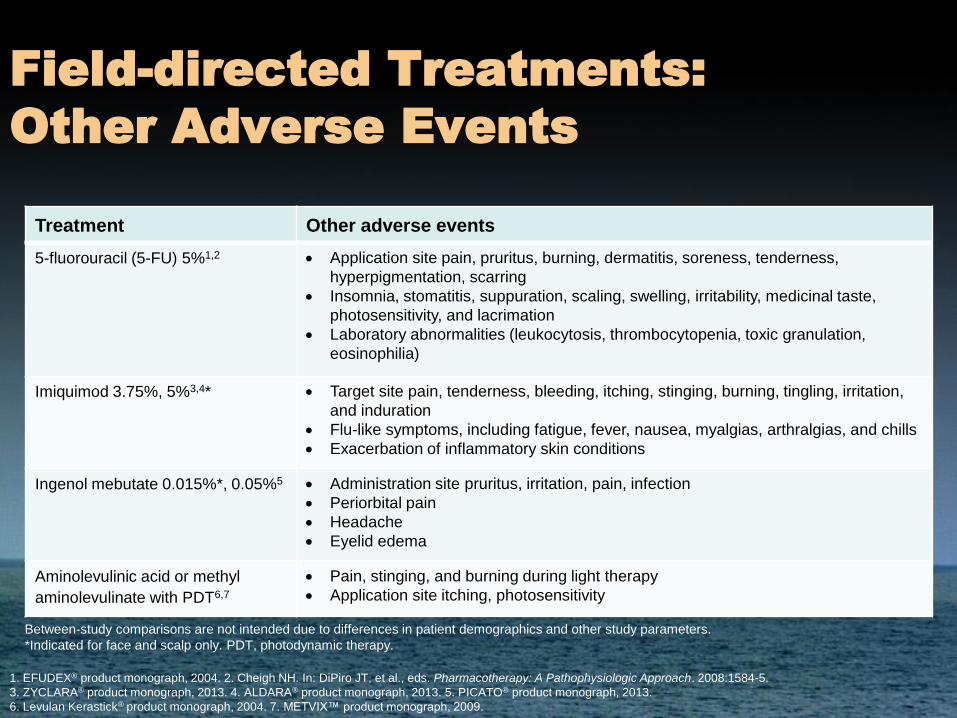
Field-directed Treatments:
Other Adverse Events
Treatment Other adverse events
5-fluorouracil (5-FU) 5%1,2 • Application site pain, pruritus, burning, dermatitis, soreness, tenderness,
hyperpigmentation, scarring
• Insomnia, stomatitis, suppuration, scaling, swelling, irritability, medicinal taste,
photosensitivity, and lacrimation
• Laboratory abnormalities (leukocytosis, thrombocytopenia, toxic granulation,
eosinophilia)
Imiquimod 3.75%, 5%3,4* • Target site pain, tenderness, bleeding, itching, stinging, burning, tingling, irritation,
and induration
• Flu-like symptoms, including fatigue, fever, nausea, myalgias, arthralgias, and chills
• Exacerbation of inflammatory skin conditions
Ingenol mebutate 0.015%*, 0.05%5 • Administration site pruritus, irritation, pain, infection
• Periorbital pain
• Headache
• Eyelid edema
Aminolevulinic acid or methyl
aminolevulinate with PDT6,7
• Pain, stinging, and burning during light therapy
• Application site itching, photosensitivity
Between-study comparisons are not intended due to differences in patient demographics and other study parameters.
*Indicated for face and scalp only. PDT, photodynamic therapy.
1. EFUDEX® product monograph, 2004. 2. Cheigh NH. In: DiPiro JT, et al., eds. Pharmacotherapy: A Pathophysiologic Approach. 2008:1584-5.
3. ZYCLARA® product monograph, 2013. 4. ALDARA® product monograph, 2013. 5. PICATO® product monograph, 2013.
6. Levulan Kerastick® product monograph, 2004. 7. METVIX™ product monograph, 2009.
Summary
• AKs are pre-cancerous skin lesions that may
progress to SCC; progression is unpredictable
• Risk factors for development of AKs include:
– Amount of cumulative/prolonged exposure to UV
– Fair skin
– Light-coloured hair/eyes
– Older age
– Immunosuppression
• AKs may be visible or non-visible/non-palpable
• Effective treatment of AKs may help to prevent
recurrence and/or progression to SCC
40
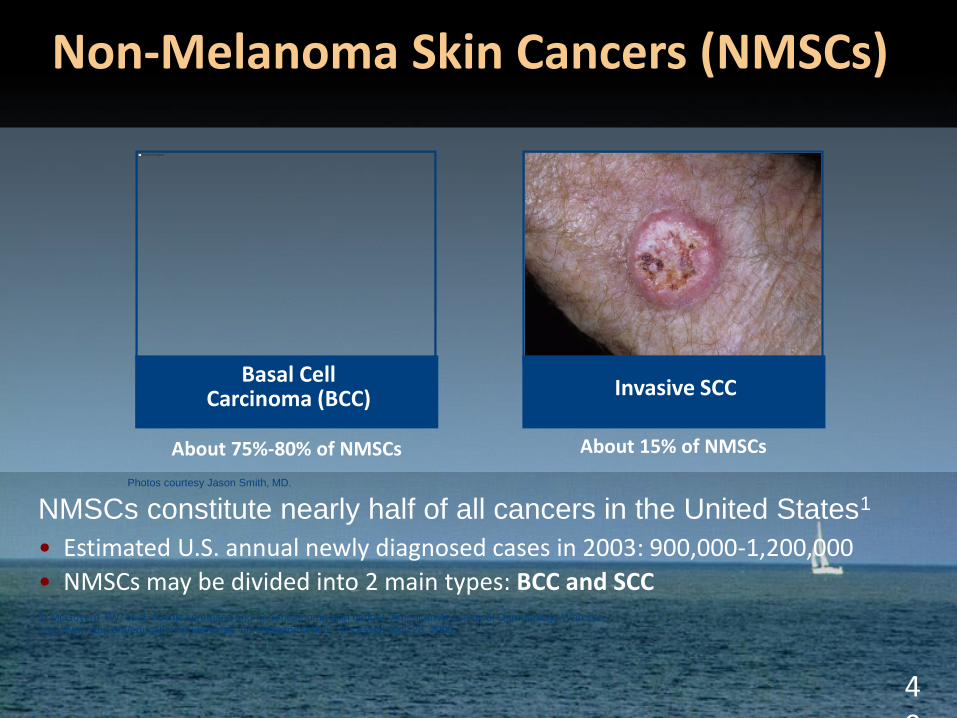
Non-Melanoma Skin Cancers (NMSCs)
NMSCs constitute nearly half of all cancers in the United States1
• Estimated U.S. annual newly diagnosed cases in 2003: 900,000-1,200,000
• NMSCs may be divided into 2 main types: BCC and SCC1. McGovern TW, et al. Actinic keratoses and non-melanoma skin cancer. American Academy of Dermatology Web site.
http://www.aad.org/education/students/ak_nonmelanoma.htm. Accessed April 28, 2009.
About 75%-80% of NMSCs About 15% of NMSCs
Basal Cell Carcinoma (BCC) Invasive SCC
Photos courtesy Jason Smith, MD.
Non- Melanoma Skin Cancer
– Basal Cell Carcinoma (BCC)
– Bowen’s Disease (SCC in situ)
– Squamous Cell Carcinoma (SCC)
Skin Cancers
Basal Cell Ca
Most common
cancer in humans
80% of skin ca
Tumour of Basal
cells
Nodular, ulcerating,
pigmented,
sclerosing and
superficial types
Locally
invasive/slow
growing
Squamous Cell Ca
Malignant
15 % of skin ca
Tumour of
keratinocytes
Arises from
epidermis
Low rate of distant
metastases
Nodes
Malignant Melanoma
Tumour of
melanocytes
5% of skin ca
Commonly back
and legs
A,B,C,D,E’s
Assoc dysplastic
nevus
MIS (melanoma in
situ)
Metastasize
Skin, nodes, liver,
lungs, brain
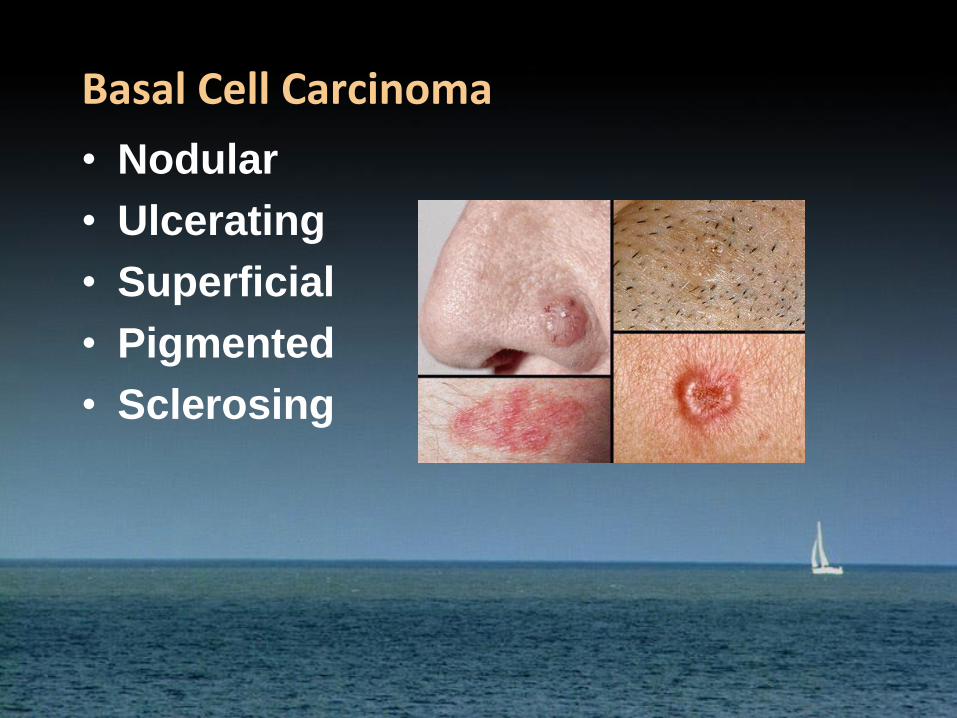
Basal Cell Carcinoma
• Nodular
• Ulcerating
• Superficial
• Pigmented
• Sclerosing

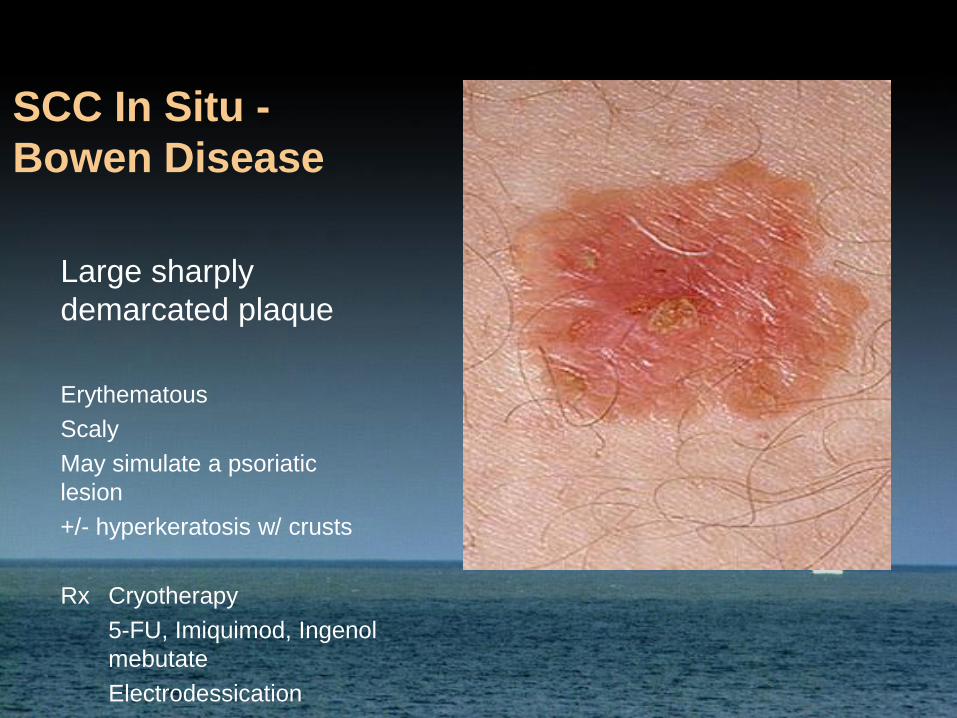
SCC In Situ -
Bowen Disease
Large sharply
demarcated plaque
Erythematous
Scaly
May simulate a psoriatic
lesion
+/- hyperkeratosis w/ crusts
Rx Cryotherapy
5-FU, Imiquimod, Ingenol
mebutate
Electrodessication
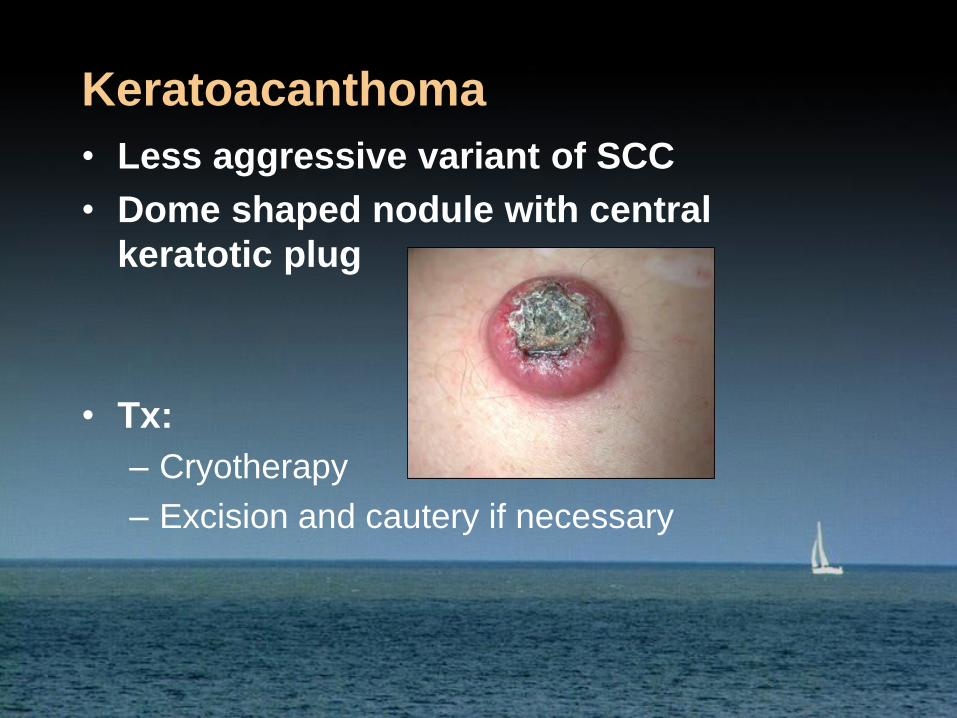
Keratoacanthoma
• Less aggressive variant of SCC
• Dome shaped nodule with central
keratotic plug
• Tx:
– Cryotherapy
– Excision and cautery if necessary
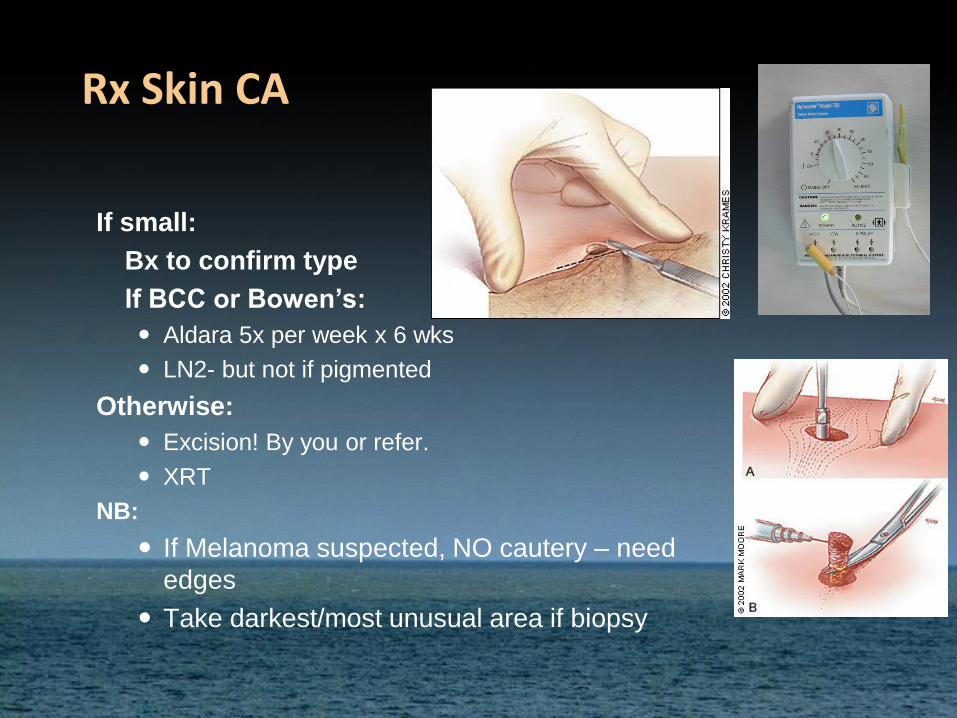
Rx Skin CA
If small:
Bx to confirm type
If BCC or Bowen’s:
Aldara 5x per week x 6 wks
LN2- but not if pigmented
Otherwise:
Excision! By you or refer.
XRT
NB:
If Melanoma suspected, NO cautery – need
edges
Take darkest/most unusual area if biopsy
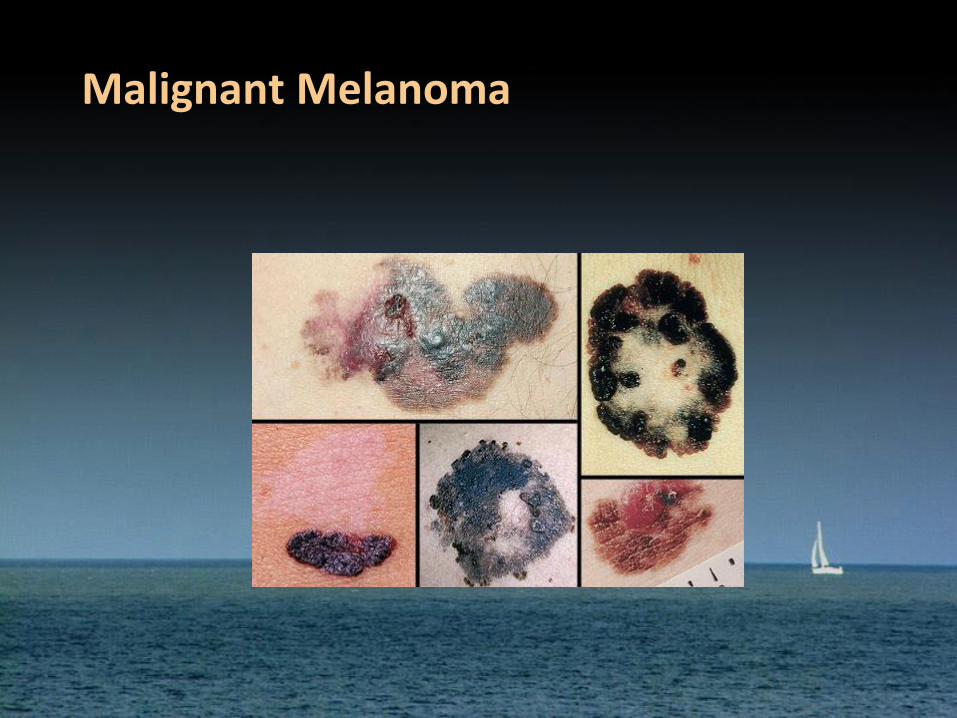
Malignant Melanoma
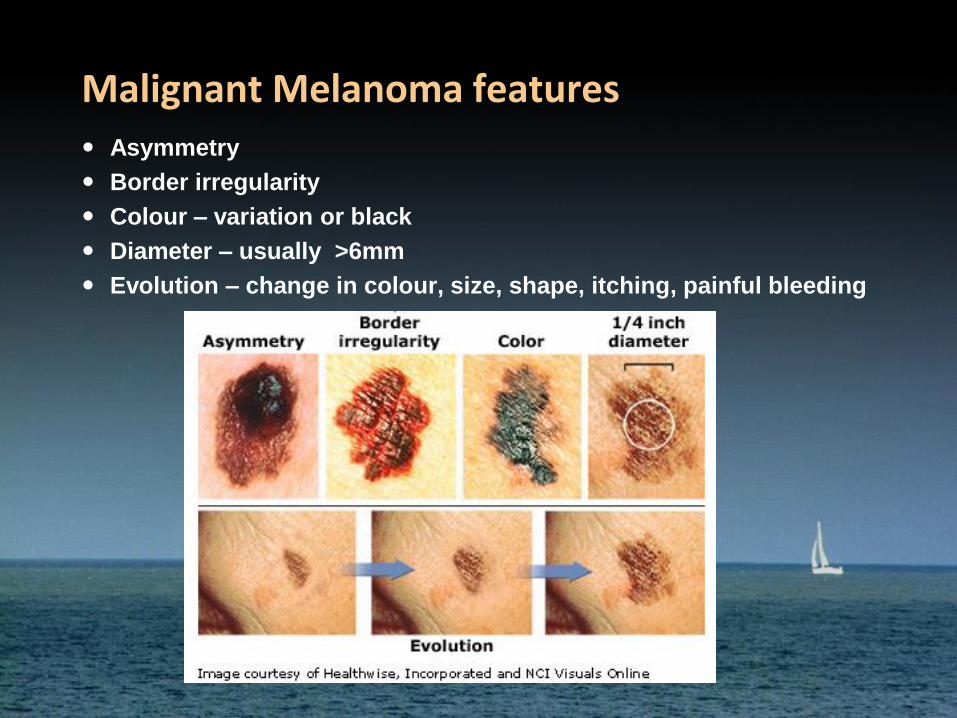
Malignant Melanoma features
Asymmetry
Border irregularity
Colour – variation or black
Diameter – usually >6mm
Evolution – change in colour, size, shape, itching, painful bleeding
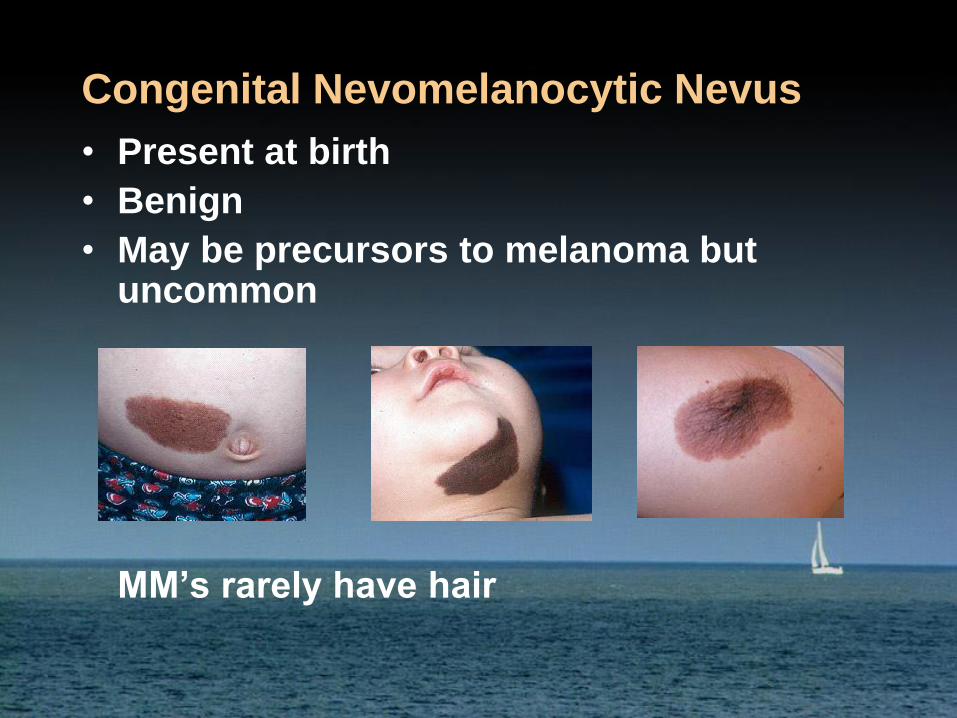
Congenital Nevomelanocytic Nevus
• Present at birth
• Benign
• May be precursors to melanoma but uncommon
MM’s rarely have hair
If not sure…
• Punch BIOPSY!
– DONT use forceps!!!!
• Can crush specimen
• Pathology may come back inconclusive
For Excision of any papule or superficial nevus

Equipment• 30 gauge needle with local
• 15 blade
• Drysol solution
• Cotton tipped applicator
• Band-aid
– DONT use forceps!!!!
• Can crush specimen
• Pathology may come back inconclusive

For Excision of any papule or superficial nevus

Intradermal Local
Bend 30 g needle 45 degrees
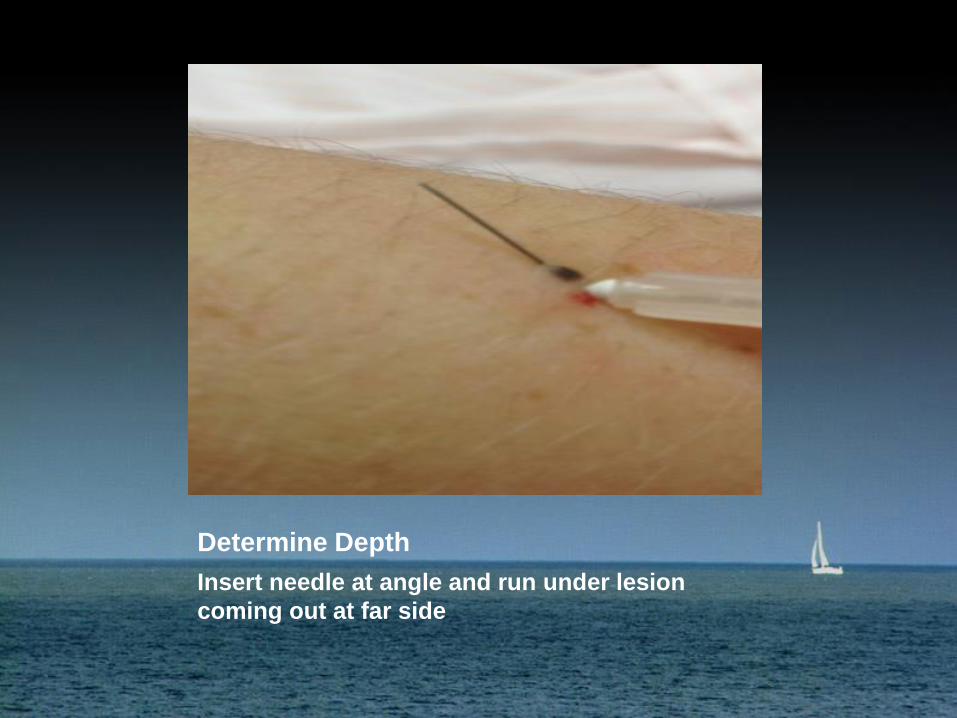
Determine Depth
Insert needle at angle and run under lesion
coming out at far side
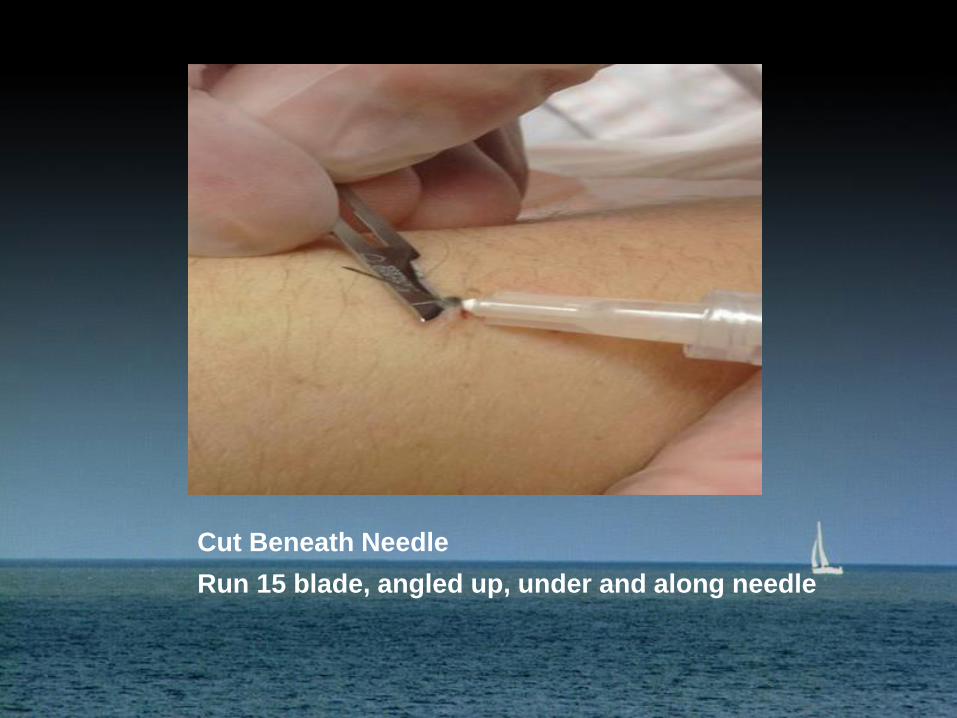
Cut Beneath Needle
Run 15 blade, angled up, under and along needle


Specimen
Remains on needle for easy transfer to formalin
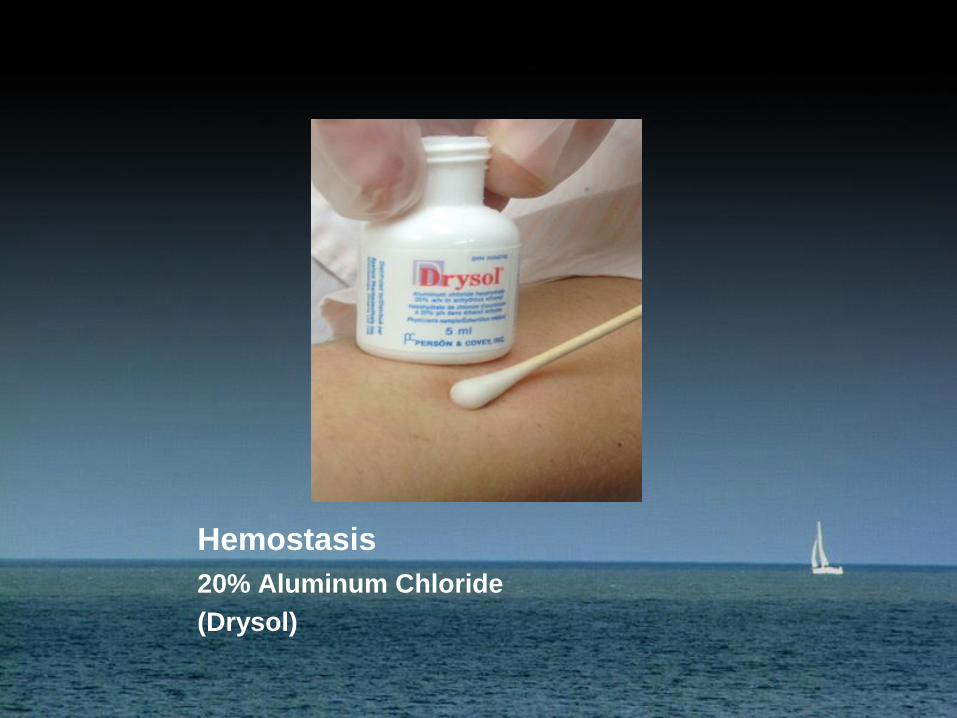
Hemostasis
20% Aluminum Chloride
(Drysol)

Minimal Scar
Superficial wound heals with minimum scarring

Always Send Specimen
Use Separate containers for each specimen
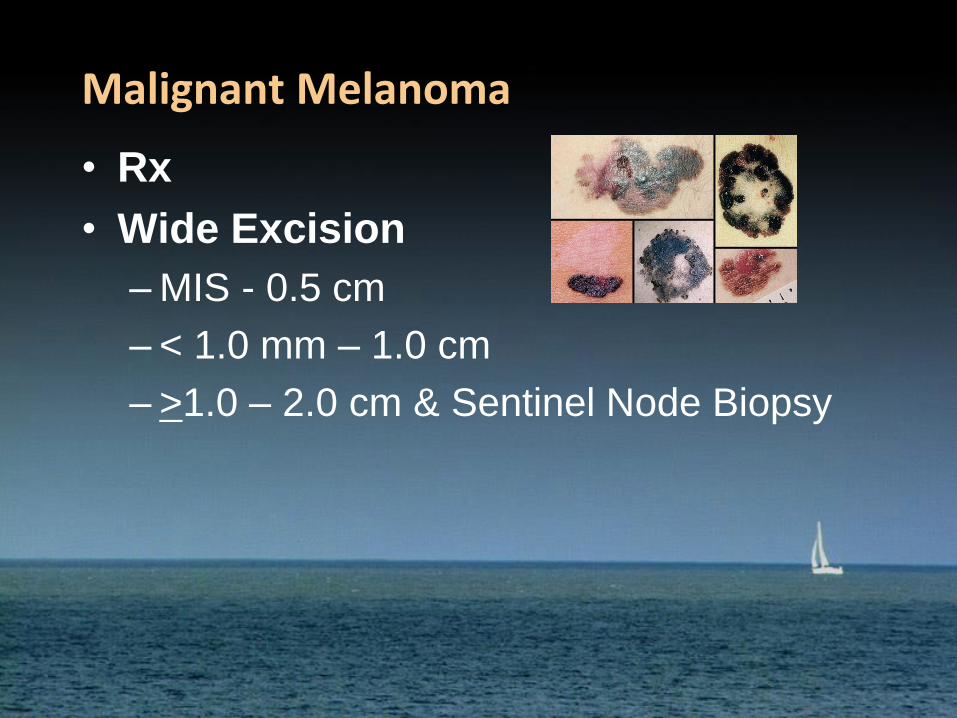
Malignant Melanoma
• Rx
• Wide Excision
– MIS - 0.5 cm
– < 1.0 mm – 1.0 cm
– >1.0 – 2.0 cm & Sentinel Node Biopsy
Stage III Melanoma That Cannot Be
Removed By Surgery, Stage IV
Melanoma, and Recurrent Melanoma
• Immunotherapy
– Ipilimumab, pembrozilumab, nivolumab, IL-2
• Targeted Therapy
– Vemurafenib, debrafenib, trametinib, cobimetinib
• Injections into tumor
– Oncolytic virus therapy
• Chemotherapy
• Palliative surgery or radiation
And Now for Something
Completely Different
A few skin lesions often mistaken for
skin cancer
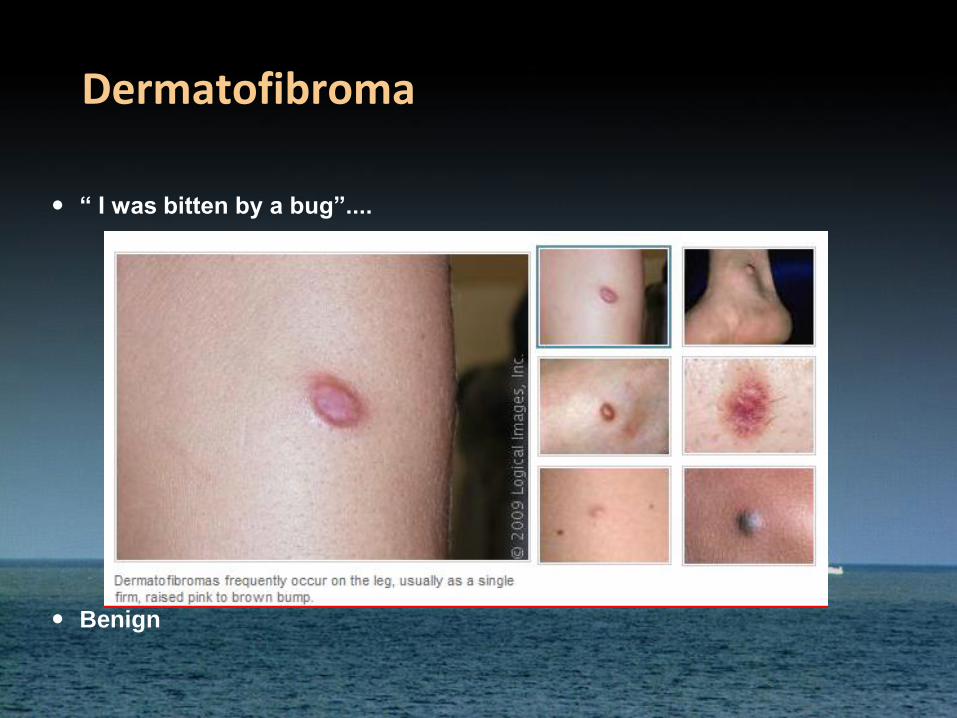
Dermatofibroma
“ I was bitten by a bug”....
Benign
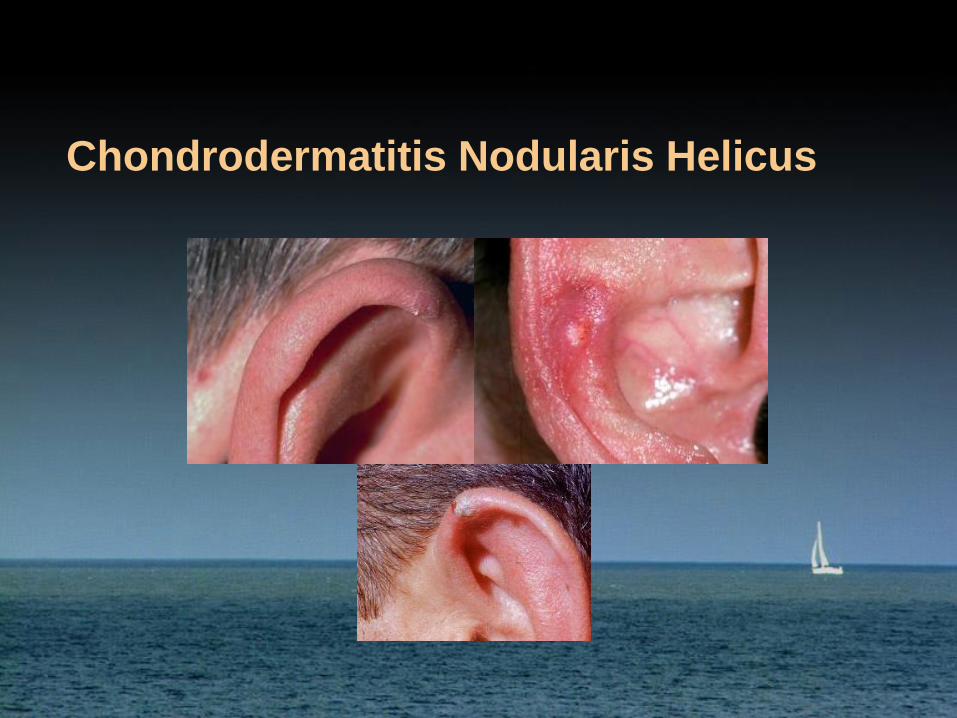
Chondrodermatitis Nodularis Helicus
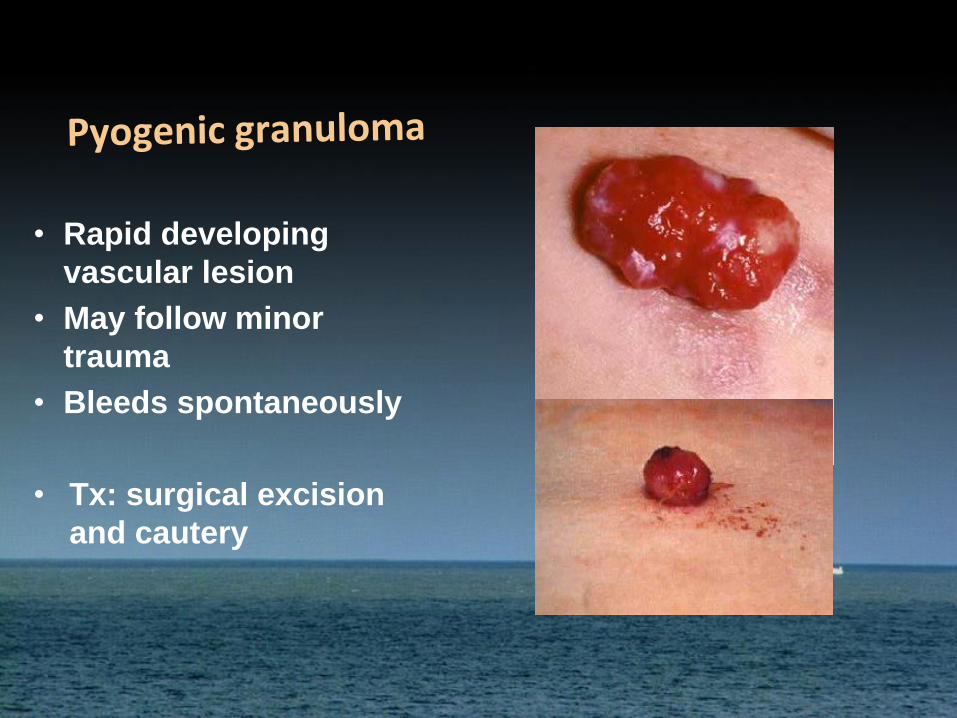
• Rapid developing
vascular lesion
• May follow minor
trauma
• Bleeds spontaneously
• Tx: surgical excision
and cautery
Summary
• BCC 80%
– Almost never spread
• SCC 15%
– May metastasize to nodes
• Melanoma 5%
– Potentially lethal
– Early detection critical
• A B C D E
• All related to UV radiation exposure
• Please protect yourself!!
– Sunscreen, Hat, Shirt, Shade, Sunglasses