Embed Size (px)
Citation preview
bcbswny.com
A division of HealthNow New York Inc., an independent licensee of the BlueCross BlueShield Association. 4382_WNY_02-17
Practice Guidelines for Providers For all Expectant Mothers
Right Start Prenatal Guidelines and Assessment
Approved by Corporate Quality Management Committee on: 10/10/17
Originally approved by Quality Management Committee on: 11/00
Reviewed annually before every January Quality Management Committee meeting (unless otherwise noted)
Revisions: Guideline revisions sent to Quality Management Committee on: 01/11/11, 01/10/12, 01/07/14, 10/05/15, 10/04/16
2
H e l p Yo u r P a t i e n t s G e t T h e M o s t F r o m R i g h t S t a r t
About Right Start• Complete Right Start initial assessment
in the first trimester of pregnancy andfax or mail to program coordinator
• Form must be received before patientreaches 15 weeks gestation for physicianto qualify for $100 reimbursement (highrisk)
For more information or to fax or mailinitial assessment forms, contact the program coordinator at:
Right Start 257 West Genesee Street
P.O. Box 80Buffalo, NY 14202
Phone: 1-716-887-8734 or 1-716-887-79551-800-677-3086 Fax: 1-716-887-7913
For service and reimbursement information contact Provider Service at 1-716-887-6750.
In-Home CareMembers who would benefit from addi-tional educational opportunities can bereferred for in-home care. This individualcounseling is designed to enhance infor-mation and services provided in thephysician’s office.
In-home care is free of charge to pregnant enrolled members and includes:
• Skilled nursing visits by a certifiedmaternal/child care nurse
• One-on-one counseling and meal plan-ning with a registered dietician includ-ing specialty diets and diet-related riskfactors (i.e., obesity, hypertension, ges-tational diabetes, hyperemesis)
• Medical social worker counseling toaddress psychosocial and financialconcerns.
4032 R1 BCBS Right Start Guide_Oct2010 10/15/10 12:10 PM Page 2
3
I n i t i a l V i s i t a n d E d u c a t i o n
Preconception care — includes identifying those condi-
tions that could affect a future pregnancy but may be
avoided by early intervention.
ACOG has grouped the main components of preconcep-
tion care under four categories of intervention.
• Maternal assessment (e.g., family history, behaviors,
obstetrical history, general physical exam, etc.)
• Vaccinations (e.g., Rubella, Varicella and Hepatitis B)
• Screening (e.g., HIV, STD, genetic disorders, etc.)
• Counseling (e.g., folic acid consumption, smoking and
alcohol cessation, weight management, etc.)
When to schedule the initial visit:
Prior to 14th week gestation
• Members must be scheduled for an appointment within
these time frames for 1st, 2nd and 3rd trimesters: Once
enrollee has contact with the provider, initial prenatal
visits: within 3 weeks during first trimester, within
2 weeks during the second trimester, and within 1 week
during the third trimester.
What should be completed at this visit:
0-14 weeks gestation send Prenatal Program initial assess-
ment form to the prenatal coordinator.
Comprehensive health history to include:
• Epilepsy
• Cardiovascular disease
• Hematological disorders
• MHSA (Mental Health & Substance Abuse) history
• Malignancy surgeries/hospitalizations
• Asthma
• UTI/Kidney disease
• Diabetes, other metabolic disorders
• Menstrual history
• Ethnicity, psychosocial, economic history
Family history to include:
• Congenital abnormalities • Cardiovascular diseases
• Genetic abnormalities • Multiple births
– screening for genetic • Malignancy
disorders • Metabolic diseases
Detailed record of current pregnancy
Estimated date of delivery
Nutritional profile — to include folic acid intake
Nutritional screen. Counseling, monitoring and f/u of all
pregnant women at nutritional risk by a nutritionist or
registered dietician.
OB history
• Abnormal pap • Multiple gestations
• Fertility therapy • Number of full term
• Prior amniocentesis pregnancies
• Total number of • Number of spontaneous
pregnancies regardless and induced abortions
of outcome • Dates of previous
• Number of premature pregnancies
deliveries • Birth weight for each delivery
• Number of living children • STD
• Length of each gestation • Previous C/S
• Complication of • Prior LBW (<2,500 gm)
pregnancy, labor or • Toxemia/eclampsia
delivery for each birth • Incompetent cervix
• Route of delivery • Uterine malformation
Physical Exam
• Height • Lungs
• Weight
• BMI• Breast
• Blood pressure
• Abdomen
• HEENT• Extremities
• Lymph nodes
• Heart
• Breast exam
Pelvic Exam
• Cervix/uterus (size and • Adnexa
relation to the pregnancy • Bony pelvis
should be documented - • Rectum
sonogram as per MCO • Vagina
corporate policy) • Vulva
Psychosocial assessment to include: screening for social,
economic, psychosocial and emotional problems including
referrals as appropriate to the needs of the woman and
follow up.
Assessment of the parent’s attitude toward pregnancy
• Support systems available.
• Need for parenting education.
0324 HN Prenatal Guide 01-07 1/22/07 1:28 PM Page 3
• Thyroid
4
I n t e r v a l V i s i t s
When to schedule the interval visits:• Every 4 weeks (0-28 weeks)• Every 2-3 weeks (29-36 weeks)• 1/week > 36 weeks
What should be completed at all interval visits:• Blood pressure• Maternal weight• Urinalysis for sugar and albumin• Gestational age• Fetal heart rate and/or Fundal height• Review and documentation re: identification of
medical, obstetrical, nutritional, psychosocial, genetic and environmental factors
What should also be completed at > 36 weeks visits:• Fetal presentation
Tr e a t m e n t a n d H o m e C a r e O p t i o n s
Home care:• Fetal monitoring/doppler• Movement kick counts• Diabetic management:
- Diet therapy/meal planning with Registered Dietician- Insulin- Blood glucose monitoring- Urine ketone monitoringServices provided by home care for follow up on all ator high risk members in the Prenatal Program.
Skilled nursing referralRegistered dietician referralMedical social workerSmoking cessation counselingBehavioral Health
The Right Start program home care option includesskilled nursing visits by certified maternal/child careRNs, in-home Registered Dietician which includes one-on-one counseling, meal planning for specialty diets anddiet related risk factors, ie: obesity, hypertension, gesta-tional diabetes, hyperemesis. In-home medical socialworker to address psychosocial/financial concerns. All ofthe above services are copay exempt (free of charge to allpregnant members).*
* NYS Maternity Legislation 1/1/97 - early dischargeentitles member to skilled nursing visit in home (within24 hours of discharge, < 48 hours for vaginal deliveryand < 96 hours for c-section). No copay for these visits.
4032 R1 BCBS Right Start Guide_Oct2010 10/15/10 12:10 PM Page 4
Maternal age
Diabetes/GestationalDiabetes
Heart, pulmonary,hepatic, collagen &infectious disease
Hypertension/PIH
Neurologic disorders
Renal disease
Abruptio placenta
History of conizationsof cervix
Pregnancy losses
Placenta previa
Preterm labor (onset of labor > 20 weeks < 37 weeks with contractions and progressive cervical changes)
Previous congenital anomalies
Previous preterm delivery
DES exposure/Teratogens
Depressed social-economic status
Domestic violence
Lead
Medications
Nutritional Status
Smoking
Mental Health
Previous C-Section
Prior LBW (<2500 grams)
Illicit drug use
Nutritional Risk/BME
Patients age > 35 years
Thalassemia (Italian, Greek, Mediterranean or Asian background) MCV < 80
Neural Tube Defect (MeningomyeloceleSpina Bifida orAnencephaly)
Tay-Sachs (e.g. Jewish, Cajun, French Canadian)
Mental Retardation/Autism — if yes, was person tested for Fragile X
Medications (Including, supplements,vitamins, herbs, or OTCdrugs)/ Illicit/RecreationalDrugs/Alcohol since lastmenstrual period
Congenital Heart Defect
Down Syndrome
Sickle Cell Diseaseor Trait (African)
Hemophilia or otherblood disorders
Canavan disease
Cystic Fibrosis
Huntington Chorea
Other inherited genetic orchromosomal disorders
Maternal metabolic disorders (e.g. Insulin-DependentDiabetes, PKU)
Recurrent pregnancyloss, or a stillbirth
Patient or baby’s fatherhad a child with birthdefects not listed above
Muscular Dystrophy
Genetic Screening/Teratology CounselingIncludes patient, baby’s father, or anyone in either family with:
5
Contact Case Manager with Right Start members initialassessment form to enroll in Right Start Case Management.
1-716-887-8734 (phone) 1-716-887-7913 (fax)1-800-677-3086
R i s k F a c t o r s To B e A s s e s s e d
4032 R1 BCBS Right Start Guide_Oct2010 10/15/10 12:10 PM Page 5
6
P r e n a t a l E d u c a t i o n
P r e b o o k i n g / Tr a n s f e r o f I n f o r m a t i o n t o D e l i v e r y S i t e s
• Signs of pregnancy complications
• Toxoplasmosis precautions (cats/raw meat)
• Sexual activity
• Nutrition counseling
• Environmental/work hazards
• Genetic testing
• HIV counseling and education (NYS information line1-800-541-AIDS)
• All patients to be tested for HIV antibodies must be provided with pre-and post-test counseling in compli-ance with New York State HIV Confidentiality Law (Public Health Law Article 27-F). Medical record documentation is required.
• Domestic violence
• VBAC counseling
• Lifestyle modifications:
- Alcohol
- Substance abuse
- Tobacco counseling - refer forsmoking cessation counseling
• Childbirth class (free through our HealthEducation classes)
• Labor signs/preterm labor signs
• Anesthesia plans
• The consequences of ingesting solid food after theonset of labor, given that a general anesthetic could berequired for the delivery
• Maternal postpartum care - including:
- Postpartum contraception
- Sterilization
- Preconception counseling
- The use of folic acid
• Plans for infant feeding
- Breast feeding education
- Available lactation support services
• Newborn screening
- Coordination with neonatal care provider forprovisions of pediatric service
- Choose Pediatrician and/or Family Practice Physician
- Schedule Pediatric Follow up
• A system for sharing medical records with the deliverysite and receiving information from referral sources anddelivery sites.
- Pre-booking women for delivery at 34-36 weeks
gestation for low risk pregnancies.
- Pre-booking women for delivery at 26 weeks
gestation for high risk pregnancies.
4032 R1 BCBS Right Start Guide_Oct2010 10/15/10 12:10 PM Page 6
• Depression
7
L a b o r a t o r y D i a g n o s t i c s
P o s t p a r t u m V i s i t a n d E d u c a t i o n
Initial Labs• Blood type • RPR/VDRL
• D(Rh) type • Urine culture/screen
• Antibody screen • HbsAg
• HCT/HGB • Chlamydia
• Pap test/Cervical Cytology • GC screening
• Rubella/Varicella • HIV counseling/testing
• Vaginal Culture • TSH
Additional Labs (if indicated)
• HgB Electrophoresis • Tay-Sachs
• PPD • Genetic Screening
• Lead Screening
8 - 18 Week Labs (when indicated/elected)
• Ultrasound • Amnio/CVS:
• MSAFP/Multiple Markers, - Karyotype
consent or refusal signed - Amniotic Fluid (AFP)
or documented
24 - 28 Week Labs• HCT/HGB • D(Rh) Antibody screen
• Diabetes screen • D Immune Globulin
• GTT (if screen abnormal) (RhIG) given (28 weeks)(*)
*Administer Rho(D) immune globulin prophylactically by28 weeks if repeat antibody screen indicates unsensitized RH.
32 - 36 Week Labs (when indicated)
• HCT/HGB (recommended) • Chlamydia
• VDRL • Group B Strep• Repeat HIV testing (35-37 weeks) GC
When to schedule the postpartum visit:• 7 - 14 days after cesarean delivery and/or
complicated gestation
• 21 - 56 days for all deliveries
What should be completed at this visit:• Documentation re: delivery outcome and health status
of mother/infant including Medical/psychosocial needswith appropriate referrals if indicated.
• Complete physical exam:
- assessment of the breasts
- blood pressure
- abdomen, external and internal genitalia
- weight
• Laboratory studies - as indicated by the assessment
• Psychosocial: assess for postpartum depression and linkpatient with appropriate services:
• Nutrition/breast feeding counseling
• Family planning:
- sexual activity
- preconception
- contraception
- sterilization counseling
Assess family planning needs and provide adviceand services on referral where indicated
• Tobacco counseling
Source:
ACOG Guidelines for Perinatal Care, Seventh Edition,
2012. New York State Department of Health Standards
Right Start Prenatal Program
4032 R1 BCBS Right Start Guide_Oct2010 10/15/10 12:10 PM Page 7
• Sickle Cell• GTT• TSH• Gonorrhea
8
4382
S m o k i n g C e s s a t i o n
It’s a fact that 21-22%* of low birth weight babies areborn to mothers who smoke.
Identify smokers on the initial assessment form and theywill be referred for smoking cessation counseling.
Implement the 5 A’sPhysicians could improve the 20% low birth weight statistic by implementing the Agency for HealthcareResearch and Quality (AHCPR) tobacco cessation “4 A’s” interventions in their office practice.
AskIdentify and document tobacco use status on all pregnantwomen at every visit.
AdviseDeliver a clear, strong and personalized message to everypregnant tobacco user to quit. Example: “Quitting smok-ing is the best action you can take for your health andyour baby’s health. As your doctor, I strongly encourageyou to quit.”
AssessDetermine client’s willingness to quit.
AssistHelp the pregnant tobacco user with a quit plan and edu-cational materials.
ArrangeRefer the pregnant tobacco user to call 1-716-887-8734 /1-716-887-7955 or 1-800-677-3086 for educational andreferral information.
A Division of HealthNow New York Inc. An Independent Licensee of the BlueCross BlueShield Association.
4032 R1 BCBS Right Start Guide_Oct2010 10/15/10 12:10 PM Page 8
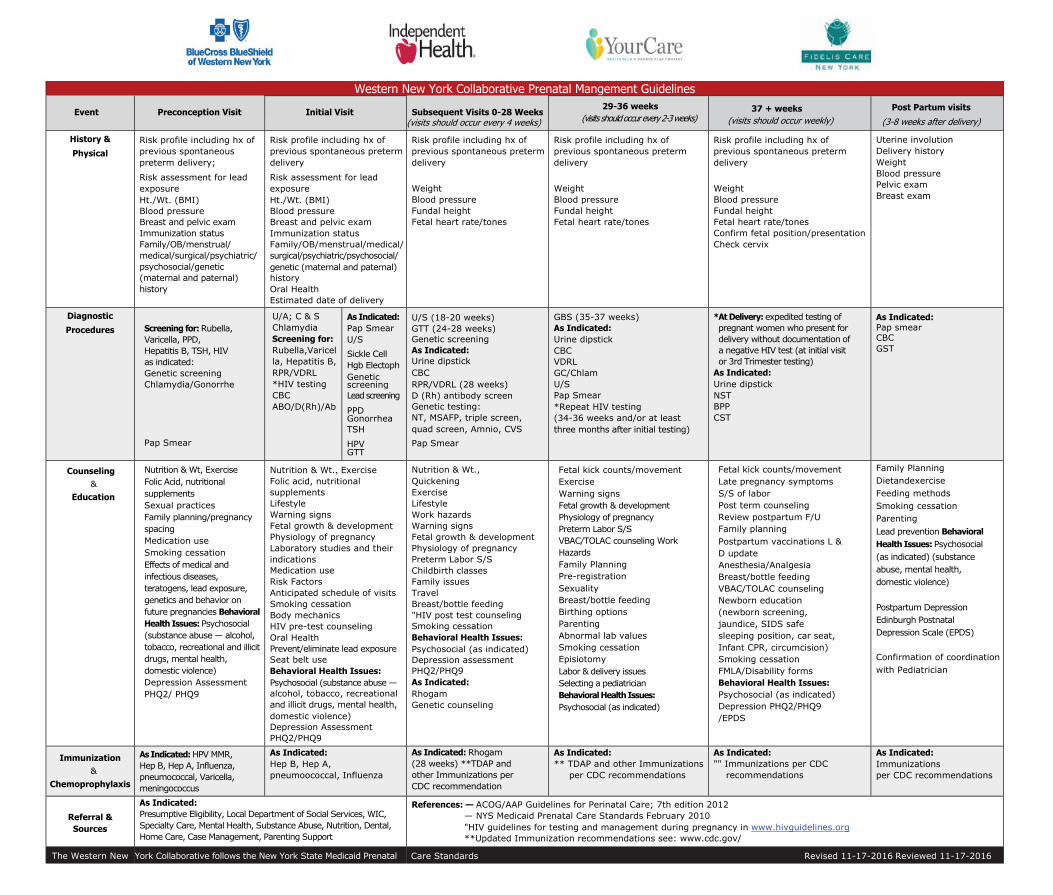
Western New York Collaborative Prenatal Mangement Guidelines
Event Preconception Visit Initial Visit Subsequent Visits 0-28 Weeks(visits should occur every 4 weeks)
29-36 weeks (visits should occur every 2-3 weeks)
37 + weeks (visits should occur weekly)
Post Partum visits
(3-8 weeks after delivery)
History &
Physical Risk profile including hx of previous spontaneous preterm delivery;
Risk assessment for lead exposure Ht./Wt. (BMI) Blood pressure Breast and pelvic exam Immunization status Family/OB/menstrual/ medical/surgical/psychiatric/ psychosocial/genetic (maternal and paternal) history
Risk profile including hx of previous spontaneous preterm delivery
Risk assessment for lead exposure Ht./Wt. (BMI) Blood pressure Breast and pelvic exam Immunization status Family/OB/menstrual/medical/surgical/psychiatric/psychosocial/ genetic (maternal and paternal) history Oral Health Estimated date of delivery
Risk profile including hx of previous spontaneous preterm delivery
Weight Blood pressure Fundal height Fetal heart rate/tones
Risk profile including hx of previous spontaneous preterm delivery
Weight Blood pressure Fundal height Fetal heart rate/tones
Risk profile including hx of previous spontaneous preterm delivery
Weight Blood pressure Fundal height Fetal heart rate/tones Confirm fetal position/presentationCheck cervix
Uterine involution Delivery history Weight Blood pressure Pelvic exam Breast exam
Diagnostic
Procedures Screening for: Rubella, Varicella, PPD, Hepatitis B, TSH, HIV as indicated: Genetic screening Chlamydia/Gonorrhe
Pap Smear
U/A; C & S Chlamydia Screening for: Rubella,Varicel la, Hepatitis B, RPR/VDRL *HIV testingCBC ABO/D(Rh)/Ab
As Indicated: Pap Smear U/S Sickle Cell Hgb Electoph Genetic screening Lead screening
PPD Gonorrhea TSH
HPV GTT
U/S (18-20 weeks) GTT (24-28 weeks) Genetic screening As Indicated: Urine dipstick CBC RPR/VDRL (28 weeks) D (Rh) antibody screen Genetic testing: NT, MSAFP, triple screen, quad screen, Amnio, CVS Pap Smear
GBS (35-37 weeks) As Indicated: Urine dipstick CBC VDRL GC/Chlam U/S Pap Smear *Repeat HIV testing(34-36 weeks and/or at least three months after initial testing)
*At Delivery: expedited testing of pregnant women who present for delivery without documentation of a negative HIV test (at initial visit or 3rd Trimester testing)
As Indicated: Urine dipstick NST BPP CST
As Indicated: Pap smear CBC GST
Counseling &
Education
Nutrition & Wt, Exercise Folic Acid, nutritional supplements Sexual practices Family planning/pregnancy spacing Medication use Smoking cessation Effects of medical and infectious diseases, teratogens, lead exposure, genetics and behavior on future pregnancies Behavioral Health Issues: Psychosocial (substance abuse — alcohol, tobacco, recreational and illicit drugs, mental health, domestic violence) Depression Assessment PHQ2/ PHQ9
Nutrition & Wt., ExerciseFolic acid, nutritional supplements Lifestyle Warning signs Fetal growth & development Physiology of pregnancy Laboratory studies and their indications Medication use Risk Factors Anticipated schedule of visits Smoking cessation Body mechanics HIV pre-test counseling Oral Health Prevent/eliminate lead exposure Seat belt use Behavioral Health Issues: Psychosocial (substance abuse — alcohol, tobacco, recreational and illicit drugs, mental health, domestic violence) Depression Assessment PHQ2/PHQ9
Nutrition & Wt., Quickening Exercise Lifestyle Work hazards Warning signs Fetal growth & development Physiology of pregnancy Preterm Labor S/S Childbirth classes Family issues Travel Breast/bottle feeding "HIV post test counseling Smoking cessation Behavioral Health Issues: Psychosocial (as indicated) Depression assessment PHQ2/PHQ9 As Indicated: Rhogam Genetic counseling
Fetal kick counts/movement Exercise Warning signs Fetal growth & development Physiology of pregnancy Preterm Labor S/S VBAC/TOLAC counseling Work Hazards Family Planning Pre-registration Sexuality Breast/bottle feeding Birthing options Parenting Abnormal lab values Smoking cessation Episiotomy Labor & delivery issues Selecting a pediatrician Behavioral Health Issues: Psychosocial (as indicated)
Fetal kick counts/movement Late pregnancy symptoms S/S of labor Post term counseling Review postpartum F/U Family planning Postpartum vaccinations L & D update Anesthesia/Analgesia Breast/bottle feeding VBAC/TOLAC counseling Newborn education (newborn screening, jaundice, SIDS safe sleeping position, car seat, Infant CPR, circumcision) Smoking cessation FMLA/Disability forms Behavioral Health Issues: Psychosocial (as indicated) Depression PHQ2/PHQ9 /EPDS
Family Planning Dietandexercise Feeding methods Smoking cessation Parenting Lead prevention Behavioral Health Issues: Psychosocial (as indicated) (substance abuse, mental health, domestic violence)
Postpartum Depression Edinburgh Postnatal Depression Scale (EPDS)
Confirmation of coordination with Pediatrician
Immunization &
Chemoprophylaxis
As Indicated: HPV MMR, Hep B, Hep A, Influenza, pneumococcal, Varicella, meningococcus
As Indicated: Hep B, Hep A, pneumoococcal, Influenza
As Indicated: Rhogam (28 weeks) **TDAP and other Immunizations per CDC recommendation
As Indicated: ** TDAP and other Immunizations
per CDC recommendations
As Indicated: "" Immunizations per CDC
recommendations
As Indicated: Immunizations per CDC recommendations
Referral & Sources
As Indicated: Presumptive Eligibility, Local Department of Social Services, WIC, Specialty Care, Mental Health, Substance Abuse, Nutrition, Dental, Home Care, Case Management, Parenting Support
References: — ACOG/AAP Guidelines for Perinatal Care; 7th edition 2012 — NYS Medicaid Prenatal Care Standards February 2010 "HIV guidelines for testing and management during pregnancy in www.hivguidelines.org **Updated Immunization recommendations see: www.cdc.gov/
The Western New York Collaborative follows the New York State Medicaid Prenatal Care Standards Revised 11-17-2016 Reviewed 11-17-2016
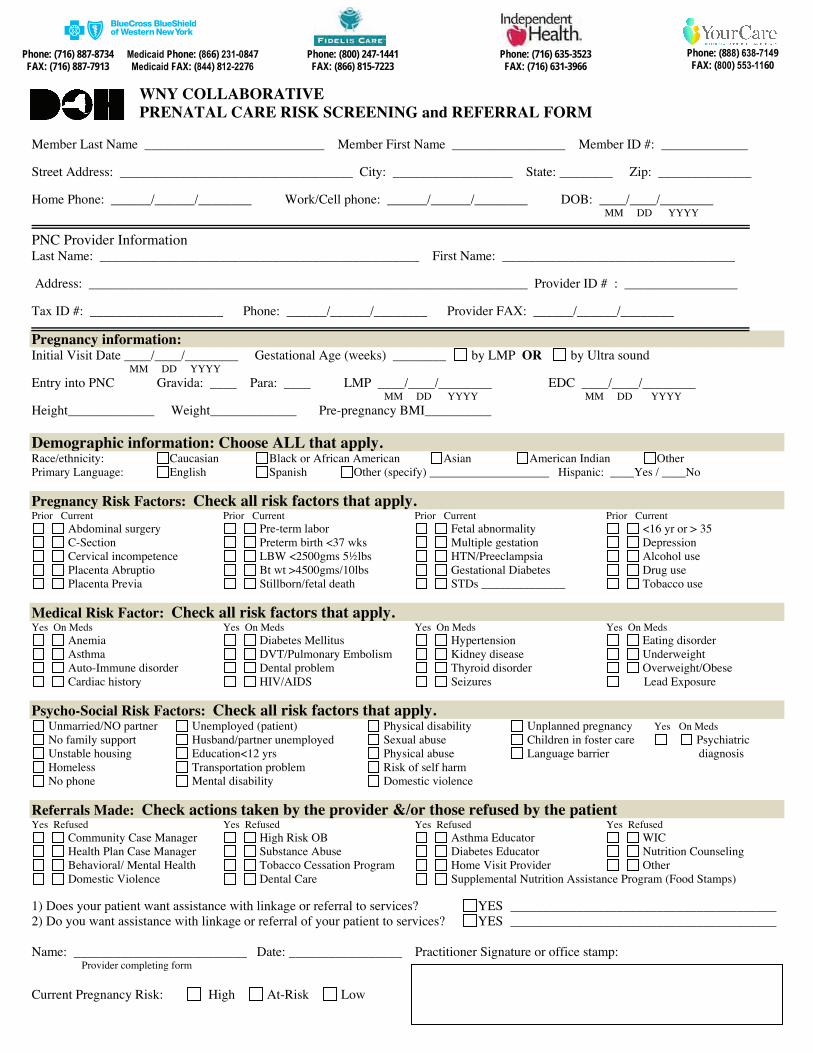
WNY COLLABORATIVE PRENATAL CARE RISK SCREENING and REFERRAL FORM
Member Last Name ___________________________ Member First Name _________________ Member ID #: _____________
Street Address: ___________________________________ City: __________________ State: ________ Zip: ______________
Home Phone: ______/______/________ Work/Cell phone: ______/______/________ DOB: ____/____/________ MM DD YYYY
PNC Provider Information Last Name: ________________________________________________ First Name: ___________________________________
Address: __________________________________________________________________ Provider ID # : _________________
Tax ID #: ____________________ Phone: ______/______/________ Provider FAX: ______/______/________
Pregnancy information:Initial Visit Date ____/____/________ Gestational Age (weeks) ________ by LMP OR by Ultra sound
MM DD YYYYEntry into PNC Gravida: ____ Para: ____ LMP ____/____/________ EDC ____/____/________
MM DD YYYY MM DD YYYY Height_____________ Weight_____________ Pre-pregnancy BMI__________
Demographic information: Choose ALL that apply. Race/ethnicity: Caucasian Black or African American Asian American Indian OtherPrimary Language: English Spanish Other (specify) ____________________ Hispanic: ____Yes / ____No
Pregnancy Risk Factors: Check all risk factors that apply. Prior Current Prior Current Prior Current Prior Current
Abdominal surgery Pre-term labor Fetal abnormality <16 yr or > 35 C-Section Preterm birth <37 wks Multiple gestation Depression Cervical incompetence LBW <2500gms 5½lbs HTN/Preeclampsia Alcohol use Placenta Abruptio Bt wt >4500gms/10lbs Gestational Diabetes Drug use Placenta Previa Stillborn/fetal death STDs ______________ Tobacco use
Medical Risk Factor: Check all risk factors that apply.Yes On Meds Yes On Meds Yes On Meds Yes On Meds
Anemia Diabetes Mellitus Hypertension Eating disorder Asthma DVT/Pulmonary Embolism Kidney disease Underweight Auto-Immune disorder Dental problem Thyroid disorder Overweight/Obese Cardiac history HIV/AIDS Seizures Lead Exposure
Psycho-Social Risk Factors: Check all risk factors that apply. Unmarried/NO partner Unemployed (patient) Physical disability Unplanned pregnancy Yes On Meds No family support Husband/partner unemployed Sexual abuse Children in foster care Psychiatric Unstable housing Education<12 yrs Physical abuse Language barrier diagnosis Homeless Transportation problem Risk of self harm No phone Mental disability Domestic violence
Referrals Made: Check actions taken by the provider &/or those refused by the patient Yes Refused Yes Refused Yes Refused Yes Refused
Community Case Manager High Risk OB Asthma Educator WIC Health Plan Case Manager Substance Abuse Diabetes Educator Nutrition Counseling Behavioral/ Mental Health Tobacco Cessation Program Home Visit Provider Other Domestic Violence Dental Care Supplemental Nutrition Assistance Program (Food Stamps)
1) Does your patient want assistance with linkage or referral to services? YES ________________________________________ 2) Do you want assistance with linkage or referral of your patient to services? YES ________________________________________
Name: __________________________ Date: _________________ Practitioner Signature or office stamp: Provider completing form
Current Pregnancy Risk: High At-Risk Low
Phone: (716) 887-8734 FAX: (716) 887-7913
Phone: (888) 638-7149 FAX: (800) 553-1160
Phone: (716) 635-3523 FAX: (716) 631-3966
Phone: (800) 247-1441 FAX: (866) 815-7223
Medicaid Phone: (866) 231-0847 Medicaid FAX: (844) 812-2276
NEW YORK STATE DEPARTMENT OF HEALTH
BEST PRACTICES FOR BREASTFEEDING
Breastfeeding Promotion Guidelines for Ambulatory Care Settings (Physician Offices, Health Centers,WIC )
1. Visible support for breastfeeding, e.g. culturally appropriate pictures or posters that shows women breastfeeding inpositive and realistic settings.
2. Positive staff attitudes toward breastfeeding at all levels of the organization (from Housekeeping to the MedicalDirector and Chief Executive Officer)
3. Comfortable chairs in waiting room for mothers to sit in while breastfeeding.
4. Private space available for breastfeeding, when desired by mothers.
5. Lactation specialist on staff, preferably IBCLC.
6. Breastfeeding home visit and/or telephone contact with all breastfeeding mothers, provided by staff or peercounselor soon after discharge from hospital.
7. Knowledgeable support for breastfeeding after returning to work.
8. Breastfeeding classes on-site.
9. Appropriate resource materials – pamphlets, books, videos from Best Start, NYSDOH, and other reliable sources.
10. No formula company materials – pamphlets, videos, pens, mugs, other “gifts”.
11. Breastfeeding "warm line” for families to call for advice about breastfeeding.
12. Information provided to mothers about community resources, e.g. peer counselors, sources of pump rentals andother breastfeeding supplies.
13. Breastfeeding assessed at each pediatric and postpartum visit.
14. Medication choices for mother consider her breastfeeding status, e.g. recommend contraceptives other thanestrogen/progestin methods
15. Duration of breastfeeding monitored.
NYSDOH – Updated June 2004
Consent for Release of Information
Patient Name: _________________________ __________________ ____________ Last First Middle Date of Birth: _____________ Managed Care Plan: ______________________________ Enrolled in Medicaid: YES NO County: ____________________________________ CIN #_____________________________ Check all that apply:
I authorize my health care provider, (name of health care provider) to release my confidential information listed on the New York State Prenatal Care Risk Form and any information provided during my evaluation by my health care provider to (name of coordinator) for the purposes of coordination of care, payment of claims for services, quality improvement of services, screening for program eligibility, and care and treatment.
I authorize release of my confidential information listed on the New York State Prenatal Care Risk Form by
(name of coordinator) to any or all of the following providers or organizations that may be providing care or services to me, as applicable: my managed care plan, my health care providers, my county health department, agencies or organizations providing prenatal services or other social or family health services including but not limited to those listed on Attachment A of this consent form.
I understand that my confidential information may include HIV/AIDS, mental health, adult/child abuse or
alcohol/substance abuse information about me. I hereby give my consent to the release of such information to the (name of coordinator) and entities or organizations listed above that will be providing care or services to me. I understand that any disclosure of the records of Federally assisted alcohol or drug abuse treatment programs is bound by
Title 42 of the Code of Federal Regulations. I understand that this consent for release of information is voluntary, and that my health care and the payments for my health care will not be affected if I do not sign this form except in some situations when information is needed for a managed care plan’s eligibility or enrollment determinations relating to me. I understand, with few exceptions, that I may see and copy the information described on this form if I ask for it, and that I may get a copy of this form after I sign it. I understand that the recipient of my confidential information may not be required to comply with the Health Insurance Portability and Accountability Act (HIPAA) and therefore the recipient of my confidential information may re-disclose it. I understand that this consent may be withdrawn by me at any time except to the extent that action has been taken in reliance upon it. I can withdraw my consent by notifying (name of coordinator) in writing at the following address: _____________________________________________________________________________________ If not previously revoked, this consent shall expire one year from its signing. ___________________________________ ___________________________________ Patient’s Signature Date Witness Signature Date __________________________________________ ____________________________________ Print Patient’s Name Signature of Personal Representative of Patient
Phone: 1-716-887-8734 Fax: 1-716-887-7913
Phone: 1-716-635-3523 Fax: 1-716-631-3966
Phone: 1-888-638-7149 Fax: 1-800-553-1160
Home Health Care Referral Dear Provider:
If any high-risk factors are identified on this prenatal member, she is eligible to have prenatal and postpartum Home Health Care visits for education and skilled needs.
Please include this referral form along with the initial referral form Only if referring for homecare services.
Date of Referral:
Patient Name:
Patient ID Number:
Please let us know if you recommend a homecare referral by checking below and faxing to the appropriate managed care organization.
Skilled Nursing
Registered Dietician
Educational Visit
Social Worker
Behavioral Health
Reason:
Physician Signature: Date:
Phone: (800) 247-1441 FAX: (866) 815-7223
Phone: 1-800-247-1441 Fax: 1-800-815-7233





























