Embed Size (px)
Citation preview

Leveraging Advanced Practice Providers to mitigate
physician burnout: Opening multi-specialty surgical
practice in medically underserved area.
Business Plan Submission
Marcus Bobbitt, PhDc, MiM, FACMPE, FMC
March 25th, 2021
This paper is being submitted in partial fulfillment of the requirements of Fellowship in
the American College of Medical Practice Executives.

1
Contents
Project Summary ........................................................................................................................ 3
Executive Summary .................................................................................................................... 3
Mission Statement ................................................................................................................... 4
Vision ..................................................................................................................................... 4
Market Opportunity................................................................................................................. 4
Management & Key Personnel ................................................................................................ 6
Business Competitive Advantages ........................................................................................... 7
Financial Analysis ................................................................................................................... 9
Pro forma Income Statement breakdown ............................................................................. 9
Organizational Plan ................................................................................................................... 11
Summary of Business ............................................................................................................ 11
Short term goals ................................................................................................................ 11
Long-term goals ................................................................................................................ 12
Business Model ..................................................................................................................... 12
SWOT Analysis .................................................................................................................... 14
Strategy & Relationships ....................................................................................................... 15
Key Stakeholders .................................................................................................................. 15
Services Provided.................................................................................................................. 16
Administrative Plan............................................................................................................... 16
Three Year Operational Plan ................................................................................................. 17
Year 1 – 2021 .................................................................................................................... 18
Year 2 – 2022 .................................................................................................................... 19
Year 3 – 2023 .................................................................................................................... 19
Regulatory & Accreditations ................................................................................................. 20
The Marketing plan ................................................................................................................... 20
Overall Marketing Strategy ................................................................................................... 21
People: .............................................................................................................................. 21
Product/ Services: ............................................................................................................. 22
Radiology ......................................................................................................................... 23
Podiatry: ........................................................................................................................... 23
Nephrology ....................................................................................................................... 24
Market Analysis – Market Research & Data .......................................................................... 24
Competitors Analysis ............................................................................................................ 25
Financial Documentation .......................................................................................................... 26

2
Summary of Financial needs: ................................................................................................ 26
Income Statement .............................................................................................................. 26
Capital Infusion ................................................................................................................. 27
Balance Sheet .................................................................................................................... 27
Cash Flow Statement ......................................................................................................... 27
APP Interactive Return on Investment Dashboard.............................................................. 28
Pro Forma Income Statement............................................................................................. 29
Cash Flow Statement............................................................................................................. 31
APP Interactive ROI Dashboard ............................................................................................ 32
Innovative Elements & Operational Outcomes .......................................................................... 32
Positive Impact ..................................................................................................................... 32
Challenges ............................................................................................................................ 32
Next Steps............................................................................................................................. 33
Appendixes & Illustrations: ....................................................................................................... 34
Medical Underserved Areas & Populations – Appendix A ..................................................... 34
Health Professional Shortage Area (HPSA) – Appendix B ..................................................... 35
Market Space – Practice Location – Appendix C ................................................................... 35
Administrative Plan: Workflow – Appendix D ...................................................................... 36
Strategic Roadmap Milestone – Three-year Strategic Plan ..................................................... 37
CLIVIA Organizational Chart ............................................................................................... 38
APP ROI Dashboard – Appendix X....................................................................................... 39

3
Project Summary
Physician burnout has been discussed for decades yet continues to rise year over year. Recent studies suggest that physician burnout has surpassed crisis proportions and reflects a continual
increase in the frequency of emotional fatigue, depersonalization, and or mental and exhaustion.
One study conducted by AMA suggests that more than half (56%) of physicians experience burnout syndrome, which negatively impacts patient relationships, patient records, and physician self-
worth, ultimately resulting in physician derailment, absenteeism, or severe cases, suicidal thoughts
or actions. Medscape physician burnout and depressions survey identified the top ten contributors
to burnout, most of which surround administrative tasks, which in their view, absorb valuable time,
which is better spent with patients.
Over 55% of the population experiencing physician burnout contribute 'patient charting' and EMR
use the top cause the burnout syndrome. More sharply, a recent study published by The New York Times suggests that physicians spent an average of 54% of their time charting notes on patients
seen. The analysis concludes that charting per patient takes longer than the clinical visit itself.
Diving deeper, the Medscape National Physician Burnout & Suicide Report of 2020 states of the millennial generate, generation X, and boomer generation, over a third of each generation would,
on average, forego between ten thousand and twenty thousand in compensation dollars in exchange
for 20% fewer work hours. Of the generation X category, they are willing to forego between a
staggering twenty and fifty thousand in compensation in exchange for fewer work hours.
Nonetheless, the following proposes the creation of a new business with an operational structure
that leverages an Advanced Practice Provider (APP) such as a physician assistant or nurse
practitioner. More sharply, the business plan structures the APP to suppress and mitigate physician burnout while building a multi-discipline practice. Although the critical components of opening a
practice are also demonstrated through the business plan, the approach intertwines advanced
practice providers in a clinical setting. In theory, it provides the physician more time with patients and less time charting within an EHR during the visit. Moreover, the top three causes of burnout
are EHR, charting, and long hours. The following proposal outlines a model where the APP role is
structured to perform the majority of the clinical visit notes, consult notes, discharges, medical
management, and conducting the clinic. All of the previously mentioned tasks will conceivably save the physician time, provide autonomy to the APP, and in theory, mitigate top contributors of
physician burnout. This approach serves as an organizational-level strategy to address the growing
health crisis from a human resources perspective.
The model also proposes a financial structure where the APP can help compensate for their
associated labor / overhead costs by incident-to billing and surgical assist fees. Furthermore, in
theory, when the APP is incentivized both monetarily and psychologically, the APP is provided
structured autonomy and increased compensation as the physician hedges top causes of physician
burnout.
Executive Summary
CLIVIA, Critical Limb Ischemia & Vascular Institute of Alaska, is a healthcare delivery system specializing in nephrology, podiatry, radiology, and vascular surgery. This healthcare organization
is geared toward treating Critical Limb Ischemia (CLI). CLI is a severe obstruction of arteries that
serves as roadblocks within the vascular system; such roadblocks reduce flow to the stated
extremities to the point of acute life-debilitating pain, ulcers, or sores requiring intervention. Untreated CLI increases morbidity such as severe infections, risk of limb loss, homeostatic

4
imbalances, or worse, loss of life. CLI and Peripheral Artery Disease (PAD) are among the world's lists of healthcare pandemics of growing proportions. On a global scale, such disease burdens
exceed over 200 million adults who suffer from one or both mentioned conditions.
CLI represents a higher prevalence than Heart Disease, which reported at 154 million patients. Heart Failure reported 64 million, Alzheimer/Dementia 44 million, Cancer 43 million, HIV/AIDS
36 million, or Opioid addiction 27 million. Thus said, CLIVIA's patient population encompasses a
vast array of individuals from diabetics, end-stage renal, and cerebrovascular complications to moderate to severe peripheral artery disease and advanced imaging diagnostics all over Alaska.
The organization is structured mechanistically, thus compartmentalized within six sections:
Nephrology, Nursing, Radiology, Podiatry, Vascular Surgery, and Administration. Of each department, except administration, a physician/provider director is specializing in that field. The
organization leverages horizontal and vertical integration benefits, allowing each department to be
considered a cost center responsible for generating revenue and managing its administratively
approved budget.
The directors' span of control commensurate with the physicians' scope of practice and supports
CLIVIA's strategic plan. This structure espouses a 'one health stop' approach that allows for the continuity of care and market share dominance. To anticipate the immense patient demand, the
organization will combat a growing concern with physician burnout syndrome by leveraging
advanced practice practitioners (APPs) such as Physician Assistants and Nurse Practitioners. The APPs will take on many of the physician's clinical administration items, allowing them to establish
and espouse CLIVIA's patient-centric culture.
This clinical structure derives from numerous clinical studies centered around physician burnout calling out the number one reason for such syndrome are bureaucratic processes and electronic
health record charting. On average, organizations that experience physician turnover spends one to
one and half times the physicians' salary in talent acquisition and training costs. Hedging such a
burnout environment will attract superior talent while ensuring a long-term employment outcome.
The advanced practice providers are also empowered as they will generate bonus incentivized
revenue. This structure subsumes overhead and allows labor efforts to contribute positively to
organizationally supported physician burnout avoidance techniques and strategies.
Mission Statement
To provide excellent patient-centered healthcare while mitigating amputations and inspiring hope
to foster improved life expectancy.
Vision
To prolong the life of humanity
Market Opportunity
CLIVIA, located within the healthcare epicenter of Alaska's acute and preventative market,
Anchorage. The population within this market is shy of eight hundred thousand total, with over
50% of the people residing in Anchorage municipality, with an average age around the mid-

5
thirties. Yet, over 33% of the population is age 60 or older, which would be CLIVIA's targeted
patient population.
According to the U.S. Health Resources & Service Administration, Alaska has deemed an MUA
state, which stands for Medically Underserved Area, depicted in appendix A. Also, Alaska has
considered a Health Professional Shortage Area (HPSA) according to appendix B. Alaska
currently does not have any vertical or horizontally integrated practices housing the six specialties
under one umbrella. The demand for health services within Alaska is highly disproportionate,
which places additional stress, pressure, and time on the physicians. According to Medscape
National physician burnout report, the 'number of hours worked' contributes a great deal to
physician burnout; when working a standard 41-50 hours per week, the physician is 40% more
likely to experience emotional exhaustion. It is not uncommon for a physician to work 51-60
hours per week, which deduces a 48% likelihood of contributing to physician burnout. When
assessing physicians' national population, general surgeons are more likely to work longer hours
by 77%.
As a human capital market opportunity, over 48% of physicians experiencing physician burnout
cope with such syndrome by exercising and spend time with friends and family. CLIVIA will
provide free wellness fringe benefits to all employees i.e. gym membership of their choice. Also,
each employee is awarded a minimum of three weeks or 120 hours of leave starting in order to
promote work-life balance.
On a national scale, only 23-28% of the office-based multi-specialty provide workplace programs
to reduce stress or burnout, CLIVIA will incorporate strategies and programs pursuant the short-
term and long-term goals listed below.

6
CLIVIA will also apply and secure a Federally Qualified Health Center (FQHC) certification to
gain access to grant funding (approximately $1.2-$2.7M) geared toward medically underserved
areas/facilities to support the above fringe benefits and operational costs.
Management & Key Personnel
Within CLIVIA, there is seven key management personnel that spearhead the essential
departmentalized functions within the organization.
1. President – This position would be held by an individual with a Medical degree and
serve as a practicing physician in one of CLIVIA's specialties with a vascular surgery
preference. The incumbent must be fellowship-trained with ten years of experience
within their specialty and an additional five years of organizational leadership. This
position will oversee the vision and direction of the medical division of the organization.
2. Chief Executive Officer – The individual will hold a minimum of a master's in business
administration; however, a Doctorate in Health Administration is ideal with ten years of
organization executive-level leadership, operations, finance, and banking. This role will
be responsible for the administrative and operational oversight of the organization.
President
Director of Nephrology
Director of Clinical Operations
Director of Radiology
Director of PodiatryDirector of Vascular
Surgery
Chief Executive Officer

7
3. Director of Nephrology – This individual must hold an M.D. practicing as a
Nephrologist for a minimum of 5 years. They will manage and lead the Nephrology
department, which includes other nephrologists and dialysis operations.
4. Director of Clinical Operations – This position will filled by an Advanced Nurse
Practitioner experienced with clinical operations of 5 years. This position will manage
and lead registered nurses, co-lead OIS labs, medical assistants, and all essential
personnel to support clinical visitations and Advance Practice Provider functionality.
5. Director of Radiology – This individual would specialize in radiology and be considered
an interventionalist, specifically in endovascular surgery. The ideal candidate would be
equipped with a wide range of experience to include ten years of practicing within
interventional radiology and five years of experience in departmental leadership. The
incumbent would manage and lead Ultrasonography operations and personnel, Positron
Emission Tomography / Computed Tomography (PET/CT) imagery to include
technologist and Medical Director of the Outpatient Interventional Suite (OIS) and
essential personnel.
6. Director of Podiatric Services – Incumbent would possess a Doctor of Podiatric
Medicine degree DPM and five years of podiatry practicing to include surgical
experience within the podiatry scope of practice. This individual would be responsible for
leading Podiatric services and associated personnel.
7. Director of Vascular Surgery – The incumbent would possess a Medical degree and
have completed a vascular surgery residency program to include five private practice
leadership years. The ideal candidate would have experience within an OIS setting of
medicine and hold a Registry of Physician in Vascular Interpretation (RPVI) certification
allowing vascular studies to read/managed.
Business Competitive Advantages
CLIVIA's predominant business advantages are the horizontal and vertical integrated
organizational model it offers its patients while placing mitigation burnout strategies at the forefront
of operations. As shown below, Anchorage serves as the epicenter of acute care, which requires patients to travel to Anchorage to receive care. The Alaska market requires immense care
coordination, travel arrangement, and synchronization between several practices, often leading to
multiple trips, subsequently increasing associated healthcare costs. For example, patients within this population struggle to travel from facility to facility, requiring facilities to work together to
share clinical information. At CLIVIA, patients can: schedule a visit with their Nephrologist, visit
the access center for dialysis, fistula revisions, see our radiology for imaging studies, among many other convenient options. Overall, this vertical and horizontal structure allows for complete
treatment under one healthcare organization.
The above-referenced competitive advantages aren't possible without fully engaged physicians; CLIVIA's burnout mitigation strategies provide attractive frameworks to foster this. More sharply,
APP's are assigned to each physician to address the following:
• All APP's are to conduct a weekly clinic for the physician to include all incident-to clinical services
• All surgical CPT codes have been identified on the APP Interactive Dashboard appendix
X

8
o The Administration department will conduct reimbursement analysis by way of appendix X on all scheduled surgeries to determine if:
o If the surgery has an assist fee, APPs will assist
o If surgery is not assistive, APPs will conduct additional clinics or be assigned an
OIS day to perform vein treatments
• For physician clinics, APPs will serve as a clinical scribe for the physician and leverage incident-to billing when appropriate; the physician must sign off on all final notes.
o APPs must perform "preclinical rounds" to preview all charts before the clinic
• APPs must round on all inpatients daily and report findings and status to the physician
• All APPs are issued a paging device. All hospital and staff paging requests are directed to
the assigned APPs except physician-to-physician pages or pages from the Emergency Department for EMTALA.
Yet perhaps the critical advantages of CLIVIA are that we recognize that physician burnout is an occupational hazard that needs a systematic approach to ensure the organization doesn't fall victim
to such. Research suggests that when organizations leverage engaging physicians within the system
and enterprise change management, it can vastly improve professional fulfillment and reduce
burnout while contributing positively to organizational performance, inpatient experience,
healthcare quality, and associated costs.
This is accomplished by building off a framework inspired by Stanford University designed to incorporate strategic interventions to improve physician well-being in three segments, culture of
self-efficacy, workplace efficiency, and personal resilience.
▪ Culture: Promoting a unison mission where physicians are involved and feel valued,
collegiality, and community which prompts a sense of belonging to a cause meaningful
and much larger than themselves.
▪ Workplace efficiency: All resources within the organization are strategically designed to promote efficiencies from clinical to admin to maintain quality, espouse high productivity,
and, most importantly, work-life balance.
▪ Personal Resilience: CLIVIA highly promotes work-life integration allowing the physicians to indulge in self-care, which allows for high performance, personal time, and
high elasticity of bouncing back from high-performance / mentally rigorous periods.
Shown below are the strategies utilized to ensure high performance, attracting top-level physicians
while mitigating physician burnout:
Segment Competitive Strategy Justification
Culture Appreciation Behavior within the
organization
Equity, diversity and inclusion
Control & Autonomy
Workplace Efficiency Efficiency of Practice Sufficient Workflows
Personal Resilience Supporting Work-life balance Organizational strategy –
perseverance
9
Financial Analysis
The following will depict CLIVIA's financial structure; as a new organization, essential assets,
personnel, and facility will be procured.
Pro forma Income Statement breakdown
• Revenue – According to the Pro-forma below, the income consists of patient fees,
including payments for insurance payers and self-pay patients. Entering the market
o Year one patient fees projected to be a mere $425K per month or $5.1M; this
would include all services rendered (all departmental services).
o Year two revenue projected to increase 35% assuming milestone objectives
addressed below are achieved, summing $573K or $6.88M
o Year three revenue is expected to increase an additional 20% assuming the
objectives below are met, summing $688K or $8.2M. Year three would be
considered our breakeven year allowing cash flow statements to depict positive
cash, allowing debt allocation execution.
• Expenses – For simplicity, the proforma income statement demonstrates significant
expense categories. CLIVIA will anticipate and budget a consequential accounting loss in
years one and two deducing just north of $-3.2M with breakeven in year three of an
estimated EBITA of $90.5K. Capital expense drill-down analysis:
o Administration & General – Overall office supplies, legal fees & professional
fees
▪ Year One - Averaging $15K per month or $180K with a 5% progression
each year
o Wages & Salaries – Accounting for the practices largest expensive, labor
associated dollars and benefits
▪ $466K per month or $5.6M progressing 5% each year
o APP Dashboard – According to appendix X, each APP has an overhead
interactive dashboard of which will track return on investment:
o Orange Table: Budgetary items such as salary, employer-associated
taxes, health insurance etc., are listed within the example demonstrating
the total cost associated with the APP. These costs are then summed and
sliced into year, quarterly, monthly, and percentages.
▪ In the example of appendix X, APP has a year cost of
$137,487.00 or a quarterly cost of $34,346.75.
o Blue Table: Quarterly revenue averages are calculated and compared
to the stated APP costs, should the revenue exceed the associated
quarterly costs, a profit is deduced; in this example the APP is
entitled to a 30% incentive.
▪ Quarterly average revenue is $44,000.00 – average quarterly
costs of $34,346.75 sum a gross profit of $9,365.25,
therefore the APP is awarded $2,895.98 in that quarter.
o Green Table: Revenue per quarter is tracked here along with total of
encounters, most used CPT codes and total return for said CPT code.

10
o Rent – CLIVIA will secure a leased facility space in the University-Medical (U-
Med) district of Anchorage. The square footage would be 10,500 sqft. Typical
buildout within Alaska's medical construction is $125 per square; CLIVIA will
negotiate a triple net 10-year lease agreement in exchange for a tenant
improvement allowance of $125 or $1.3M ($125sqft * 10,500sqft) maximum for
the space buildout with an annual increase of 3%.
▪ The current market space targeted shown in appendix C, the current
market rate is around the area is $2-2.5 per sqft, with the proposed T.I.'s
amortized over the length of the lease; this would add approximately
$1.04 per sqft. The pro forma assumes a maximum of $3.15 per sqft, thus
roughly $33K per month or $396.9K for year one, following 3%
escalators.
o Supplies – Each department specific to their specialty:
▪ Surgical supplies – Encompasses materials, devices pertaining to the OIS
budgeted for $10K per month or $120K annually, with an annual
increase of 5% each year.
▪ Imaging Supplies – Encompasses materials doses and lubricates within
imaging budgeted at $15K per month or $180K annually with a 5%
increase per year.
▪ Clinical supplies – Encompasses, medical materials such as disposals,
sharps, etc., budgeted for $5k or $60K per year with a 5% increase
annually.
o Misc. Other - .05% of monthly projected revenue will be budgeted as a
miscellaneous expense of $25.5K year one, $34.4k year two, and $41.3K year
three.
Capital Expenditure Plan
Equipment Lease - CLIVIA will invest in medical equipment to deliver quality healthcare; this
can be placed within five distinct cost centers summing approximately $2.5M. CLIVIA will lease
all medical equipment with the option to purchase the equipment at the end of the lease. The lease
option allows CLIVIA to hedge maintenance costs. The $2.5M equipment leases will be
amortized over 60 months, summing an approximate payment of $41K per month or just south of
½ a million per year.
• Clinical and administration operations will need approximately $300K (Furniture, chairs,
scales, I.T., exam room tables, EMR, etc.)
• Vascular Surgery department would be allocated the associated cost of outfitting the OIS
intraoperatively; this would include mobile C-arm, Mobile display head units, Exam
table, Pyxis for medical management, all items essential for the execution of
endovascular procedures, estimated costs - $900K
o All supplies and disposal procedural devices will be consigned to mitigate
overhead expenses until year four of solvency.
• Radiology department would be allocated costs associated with outfitting
Ultrasonography which would include Ultrasound sound machines, Ankle Brachial Index
(ABI) machines, PET/CT machine, and Picture archiving and communication system
(PACS), summing $1.2M

11
• Podiatry & Nephrology department will procure instrumentation, wound care equipment,
and autoclave, summing to $90K.
Funding Sources
According to the below proforma, a forecasted $3.2M will be lost within the first 24 months.
CLIVIA will secure a drawn-down line of credit of $4M, backed by an ISDA (International
Swaps & Derivatives Association) master agreement amortized over 25 years yet renewable
every ten years (10 X 25). The ISDA swap will allow CLIVIA to hedge floating interest rates
allowing costs to be consistent. This draw-down loan will only be utilized to cover losses for the
first 24 months.
As stated above, all medical equipment and physical assets would be secured by way of a lease or
consignment to minimize initial outlay and hedge maintenance costs, yet with the option to
purchase.
Organizational Plan
Summary of Business
CLIVIA, an Alaska-based healthcare organization, has a mission to provide excellent patient-
centered healthcare while mitigating amputations and inspiring hope to foster improved life
expectancy. This is accomplished by leveraging key specialties centered around the disease and
providing easy access to the patient population while leveraging our APP's to suppress physician burnout. The vision is to prolong the life of humanity. Outside of the strategic initiatives, CLIVIA
promotes workplace efficiency from clinical to administration to ensure proper work-life balance,
which mitigates providers' emotional exhaustive state. There are many short and long-term goals that must be achieved to achieve and sustain solvency with a core point of organizational support
for work-life integration and resilience of rejuvenation and self-care.
Short term goals
There are four primary goals/objectives of CLIVIA within the first six months to one year of
operations. The referral process & design, and creation are imperative to structure a sustainable
revenue cycle flow process. CLIVIA's culture is critical from patient-centric to our reputation;
CLIVIA must understand patient needs and perform more efficiently while providing better
quality healthcare than the market. Lastly, the ability to be deemed a federally qualified health
center is critical to gain access to federal grants:

12
Long-term goals Widening the lens to long-term goals, CLIVIA will achieve a 15% profitability margin / EBITDA
within 48 months of doors open. To attest to the high quality, we will advocate, having several
accreditations adds to the prestigious reputation and culture in development; this includes
Intersocietal Healthcare Accreditation for vascular testing and Joint Commission.
Business Model
The business model of CLIVIA is considered a blended organizational model from
mechanistic as well as organic. More specifically, CLIVIA does have individual departments
allowing specialists to be grouped accordingly. Yet, the span of control and decision-making
abilities are not centralized, which will enable departments to make snap decisions that aid in more efficient patient care. The organization is patient-centered; all work processes and flows are built
with the patient's experience at the forefront.
Furthermore, CLIVIA takes on the entire healthcare management of the patient and places it under
one umbrella allowing CLIVIA to be a one-stop healthcare delivery solution for the patient
Effi
cien
cy o
f P
ract
ice
Develop referral relationships –establish referral pipeline of 45% of market within 6 months prior to doors open and 6 month after ( 1 year)
Cu
ltu
re o
f W
elln
ess
Building an organizational culture that supports physician well-being by factoring the intrinsic drivers of the physician -Collect & reflect on said drivers to establish work-life balance, incorporating protected time slots during work day
Per
son
al R
esili
ence
Pursuant to SWOT analysis and market research, perform 20% more efficient in patient services than industry / market standard bench market within 1 year
Fed
eral
Ce
rtif
icat
ion
CLIVIA must become a Federal qualified health center which allows access to federal grants assocated with Medically underserved areas / populations within 12 months of operations. In addition to securing a Certificate of Need (CON)
Achieve 15% profitability within 48 months from doors open
Profitability
Secure Intersocietal Healthcare accreditation for Vascular Testing, MRI and Carotid Stenting within 36 months from doors open
Vascular Accreditation
Achieve Joint Commission accreditation within 24 months from doors open
Quality Care
Secure over 80% of the CLI/ Vascular / Radiology/ Podiatry market within 48 months
Control Market

13
population accepting all payers and uninsured patients. This absorbs both the vertical and horizontal components/steps of the patient's healthcare and integrates seamlessly within one electronic
medical record and company.
At the core of the organization, physician burnout mitigation strategies are around all processes allowing the physician to focus on the patient and will enable the support staff to absorb the
administration aspect. This approach espouses a high degree of continuity within the patient's care.
Additionally, this approach allows the physician to focus on the patient's healthcare plan compliance. This model is unique. This specialty of care is generally episodic; a patient normally
sees a podiatrist for a non-healing wound, which then needs to be referred over to a vascular
surgeon. The vascular surgeon then needs to assist the vasculature, which then needs an ultrasound or C.T., which requires a Radiologist referral; once images are returned and read, the vascular
surgeon may determine an intervention is necessary then requires a referral to a cardiologist for
clearance.
If the patient has kidney complications, which is generally the case, a nephrologist must be
consulted, requiring a referral. Once this is complete, the surgeon's practice must identify surgical
block time within a healthcare facility to perform the intervention.
CLIVIA brings all the required specialties within one company as well as establishes independence
from hospital organizations allowing the specialties to have their own procedural / surgery facility. Additionally, due to the increased continuity and lower overhead compared to a hospital, the
healthcare savings are passed on to the patients. This then saves healthcare payers resulting in a
high yield with respect to fee for value i.e., increased access to healthcare, convenience / safe and
significantly less costs. The values received are both tangible and intangible.
Our advanced practice providers (APP) are trained rigorously to medically and clinical manage
patients, allowing our physicians to focus on treatment. In exchange, the advance practice provides a higher yield pertaining to their associated cost as they perform billable services such as clinic
visits and consults; such autonomy empowers the employee. CLIVIA's APP's perform over 80%
of clinical duties from clinic visits, consults, follow-ups, and postops allowing the physician to
focus on operations.
CLIVIA has developed a series of physician burnout alert systems and mitigation strategies. Firstly,
all physicians are assigned an APP that will be clinically and surgically trained. The APP can assist in all clinics and surgeries set to the physician, yet it is at the physician's discretion. This process
allows the physician to remain in complete control of their work and schedule. The CLIVIA model
groups non-surgical assist procedures such as Cath lab or surgical operations that are deemed "non-
payable with an assist".
When the APP is not needed, they are to conduct clinical visits, which generates revenue and
mitigates the physician's seemly burden tasks (See appendix X for APP dashboard analysis). All assist-able surgeries are also grouped, allowing the APP to scrub in and assist the physician for
more efficiency while also generating revenue. When grouping surgeries, a Current Procedure
Terminology (CPT) analysis is performed to determine the level of return of the assist fee (see Appendix X); if the APP will generate more revenue in the clinic than assist in surgery, the
physician is notified. This includes financial analysis and clinical/patient level of impact analysis
(see appendix X).

14
The APP is provided a range of percentage of return from 5-30%; they are incentivized based on
productivity. The formula: if the APP generates $50,000 per quarter, and their overhead costs
$30,000 within that quarter, this deduces a $20,000 gross profit. If their percentage were 30%, they
would be entitled to a $6,000 bonus ((Revenue – Overhead) * Incentive Percentage) (See appendix
X).
Each quarter, all physicians are required to participate in a physician satisfaction survey; their participation automatically enters them into a random drawing of a vacation to a destination of their
choice under specific budgetary restrictions. The survey is driven by Maslach Burnout Inventory
(MBI), an assessment that measures the physician's burnout. Should levels indicate signs of burnout, the physicians' workload is paired down to a manageable scale. Should the physician
continue to show increased burnout levels, the administration department will intervene and
develop a structure that will advocate a corrective path.
SWOT Analysis The following is a CLIVIA SWOT:
Strengths
1. APP's are leveraged to keep the physicians focus on surgery, thus potentially decreasing the likelihood of physician burnout by 55% (Medscape)
2. All specialties under one organization provide increased market power, a convenience that
places increased barriers to entry 3. Physicians perspectives are factored in order to garner appreciation and respect, which
decreases contribution to physician burnout by 32% (Medscape)
4. Healthcare independence – complete control of patient's experience, products, healthcare standards
5. Longitudinal healthcare services allowing relationships to be built for longevity
6. Employee/physician burnout strategies infused within the culture.
7. Patients are seen frequently and consistently due to leveraging APP's versus waiting on
physicians' availability.
Weaknesses
1. Patients spend more time/relationship building with the APP compared to the surgeon
2. Physician could become overreliance and dependent on APP for notes and clinical visit
assistance 3. Initial years, practice will carry increased liabilities increasing financial risks
4. Increased Risk profile when clinical visits are heavily reliant on APP's medical decision /
judgment.
5. APP's autonomy could encroach and encourage complete medical independence increasing associated medical decision-making risks.
6. Limited OR surgeries compared to endovascular procedures, thus relying on hospitals for
open surgeries
7. Limited isotopes access due to initial low volumes of CT/CTA's
Opportunities

15
1. Potential to capitalize on APP perform minor procedures within the OIS 2. Impact the community by providing physician burnout mitigation strategies to positively
impact the physician shortage in Alaska.
3. Current market competitors are experiencing decreased volumes due to increasing
physicians entering the market. Merger/acquisition of practices could raise barriers to entry 4. Only 1 PET/CT serving the entire state, purchasing an additional PET/CT will capture
market share
5. No current Endovascular OIS exist within Alaska, Alaska regulations are silent on
Endovascular Cath labs
Threats
1. Consistent management of APP workload compared to physicians could shift burnout syndrome from physician to APP.
2. Regulations within the Alaska market seek to alter the role of an APP and scope of practice
– thus can be driven positively or negatively.
3. Alaska is a Certificate of Need (CON) state, which requires diligence to secure; inability to secure such will increase reliance on hospitals. It also limits referrals for outpatient-
based imaging. Should CLIVIA want to leverage outpatient-based imaging, it must be
deemed an imaging center that requires a CON. 4. Without accreditation, certain services will be disallowed for purchase
5. COVID-19 pandemic has rendered all patients required testing prior to surgery for the next
12-18 months. Current testing delays are 4-8 days, must procure COVID-19 equipment however priority is given to high volume facilities i.e. Hospitals. Failure to secure testing
will delay care.
Strategy & Relationships
Overall, the strategy is to absorb all vertical and horizontal services pertaining to patient care and integrate such within one umbrella of care to leverage the convenience and safe harbors of STARK
violations driven by APP utilization. Developing strong referral relationships prior to opening and
the continuation of such will aid tremendously in generating revenue. Starting the certificate of
need process before construction will be essential in order to navigate and plan for any design
requirements.
Establishing on-call partnerships with Providence Medical Hospital, Alaska Regional Hospital, Matsu Regional Medical Center and Alaska Native Medical Center allowing the practice to garner
consults and have a rather large footprint in the community. All on-call / paging activity will be
directed to the APP except physician-to-physician calls. This strategy shields the physician from
daily/nightly non-physician calls to avoid exhaustion. Additional partnerships would include the University of Alaska Anchorage and community colleges, allowing students to extern within the
company for the experience.
We are partnering with the University of Washington and MedEx for residency rotations, medical
students, or Physician Assistants during their training. During the APP rotation, we will heavily
emphasize the need and intent to become a critical component in mitigating physician burnout;
thus, becoming clinically and surgically equipped intelligentially is the central goal.
Key Stakeholders Within CLIVIA there are three specific levels of authority, the Board of Directors,
Administration and Operations, all of which have key personnel, as shown below.

16
Services Provided
In the effort to treat CLI, CLIVIA has a genetic makeup of four specific services:
Vascular surgery is defined as a specialty that treats the diseases found within the vascular system
by way of medical therapies, minimally or invasive surgeries to revascularize / reestablish flow.
Radiology – a branch of medicine that leverages imaging technology to discover, understand and
treat diseases. CLIVIA offers both diagnostic radiology and interventional radiology.
Nephrology – Medicine focus on the kidney functionality with the goal of sustaining and
preservation of kidney health ranging from diet management approaches, medication and rental
replacement.
Podiatry – Podiatric medicine in which focuses on the treatment of foot, ankle injuries by way of
surgical intervention.
Administrative Plan
According to appendix D an enterprised resource plan and administrative workflow cycle is
displayed.
Due to CLIVIA's complex nature, the healthcare delivery system is triggered by a referral being
received, typically by way of fax, EMR notification, or internal communication (physican to
staff). At a high level, the illustration below depicts the overall operational cycle:
OperationsAdministrationBoard of Directors
President CEO
Physicians
Providers
Managers
CLIVIA Services
Podiatry & Nephrology
Radiology
Vascular Surgery

17
Predominately, as CLIVIA treats complicated diseases, a referral is required/preferred. Rather, it
is from a primary care provider, other specialists, or the Emergency Department (E.D.) who may
have identified a need for one of our services provided. This step one, the referral is sent to our
facility/physician, this is the triggering event a patient may need care. The referral is then sent to
clinical operations, specifically the nursing team to review the referral to assess if the scope of
care fits within CLIVIA's scope of healthcare delivery. Once this is complete, the nursing team
will build the patients electronic medical record allowing all clinical information to be gathered.
The patient must be assigned to one of the following departments, Nephrology, Radiology,
Podiatry or Vascular Surgery, the referral will be interpreted and assigned accordingly, along
with an action to review and perform a needs analysis. The department that reviews the referral
must assess and review the patients and then determine "next steps" rather than an ultrasound
order, CTA, follow-up, etc. Once this assessment is selected, the department must document such
within the EMR then send scheduling instructions to the scheduling team. The scheduling team
are then to contact the patient and schedule their visit pursuant to the next availability of the
physician or APP.
Once the visit is scheduled, it is then sent to the clinical team in order to pre-chart in preparation
of the upcoming encounter with an APP. Once the patient's charts are prepped and reviewed by
an APP, the patient's chart is then sent to our billing and coding team to ensure all prior
authorizations are secured and insurance/means of paying for the services are verified and
confirmed.
Upon arrival, the patient provides a digitized check-in method to verify all their personal
information/demographics, the visit transpires, and or a surgery/study/procedure is scheduled and
performed.
Three Year Operational Plan
CLIVIA's three year operational plan is categorized within four main categories as shown below.
Milestones of which are imperative achievements, Administrative which are Human Resource
Incoming Referral
Clinical Operations
Departmental Assignment
Clinical Prep/scheduling/billing
Clinical visit & or Surgery

18
and Strategy, Services which are geared toward healthcare delivery and lastly Growth which
addresses CLIVIA's expansion initiatives.
Year 1 – 2021
CLIVIA is set for doors open within 2021:
• Milestones
o Securing funding specific to operating capital must be finalized by the end of
quarter 2 of 2021
o Design clinical appointment visits structure to be APP driven by Q1
o Accreditation of CLIVIA's services is paramount in order to support other
strategic goals such as growth and market share, by the end or quarter 4 of 2021,
CLIVIA most hold accreditation of the Joint Commission and Intersocietal
Accreditation Commission pertaining to Vascular Testing, Carotid Stenting and
Veins.
o By quarter 4, revenue should indicate a trajectory or a 25% growth rate from
doors open
• Administration
o Hiring & training critical staff personnel by quarter one of 2021 must be
completed
o Design and implement MBI physician feedback survey by Q1.
o Develop H.R. manual which strong engages physicians and surgical team teams
exhaust PTO – completed before doors open.
o Establishing and executing the workflow process outlined in the administrative
plan (appendix D) by the end of quarter 4 of 2021
o The Medicare Access CHIP Reauthorization Act (MACRA) measures must be
identified and structured within CLIVIA's EMR for mandatory reporting
requirements by the end of quarter 4 of 2021.
• Services
o Establishing a referral network by leveraging APP's is vital for the survival of
CLIVIA, identifying all primary care providers, hospitals and Ambulatory
Surgery Centers to establish easy access structure by quarter three.
o The organization will launch various initial assessments taking in perspectives of
internal and external agents (employees and patients) by the end of quarter 4;
scores pertaining to skills attainment and mental engagement/exhaustion should
indicate improvement.
o By quarter three of 2021, all surgical instrumentation is purchased and allocated.
o Identification and contract implementation of product/device consignment
agreements by the end of quarter 3.
• Growth
o Establishing partnerships with neighboring clinics & hospitals fostered by APP's
o By Quarter one of 2021, CLIVIA must have hired and onboarded all key
personnel and essential personnel for operations

19
Year 2 – 2022
CLIVIA is set for doors open within 2021:
• Milestones
o Upon doors opening, the Ambulatory Surgery Center will operate under the
Alaska exemption and or the safe harbor laws of 'extension of physician practice'
until the establishment and successful securement of a Certificate of Need by the
end of quarter four of 2022.
o In order to leverage the $1.2-$2.7M federal grant funds of a rural operation
within a medically under severed area, this will be secured before the end of
quarter three of 2021
o Financials should reflect a 25% growth over previous year by the end of quarter 4
of 2021.
o Ensuring all APP's are operating within the black financially (generating their
overhead on a breakeven basis by year end 2022
• Administration
o Pursuant to the internal surveys of performance, an element of measure will be
operational strategy, by the end of 2021, survey results should reflect
improvement over prior year.
o Before analysis to ensure APP & Physician's have maximized PTO to hedge
physician burnout
• Services
o Following there results of the external survey, the performance safety rating
should deduce an excellent rate by the end of 2022.
o CLIVIA will procure a Pyxis medicine station for med dispensing with the ability
to stock all schedule 2-5 medications.
• Growth
o Driven by the patient population demands of services, CLIVIA will perform
research and develop additional services pursuant to a needs analysis by the end
of quarter 4 of 2022.
o Upon completion of becoming federally certified, CLIVIA will submit and
obtain preliminary approval on a rural grant administrated by the Health
Resources & Services Administration.
o CLIVIA cash flow should show improved cash positioning by 10%.
Year 3 – 2023
CLIVIA is set for doors open within 2021:
• Milestones
o Upon doors opening, the Imaging Center will operate under the Alaska
exemption and or the safe harbor laws of 'extension of physician practice' not to
exceed 40% imaging studies outside of the physicians specialty, until the
establishment and successful securement of a Certificate of Need by the end of
quarter four of 2023.
o By the end of quarter fourth of 2023, CLIVIA key performance indicators should
indicate 25% growth.

20
o Physician burnout survey results reviewed and implementation of strategies by
Mid year
• Administration
o CLIVIA will not deviate from financial budgetary plan, by the end of quarter
three of 2022 financial statements should reflect on target, otherwise budgetary
cuts will be implemented.
o Prep and implement physician burnout mitigation survey for 2023 by end of Q4
2023.
• Services
o Internal and external survey should reflected increased service quality by the end
of quarter three of 2022
• Growth
o Internal survey should reflect vivid organizational citizenship behavior deducing
excellent job satisfaction score from employees by the end of quarter three of
2022
▪ Similarly, by the end of quarter, three financial measures should reflect
improved cost competitiveness.
Regulatory & Accreditations
• Certificate of Need (CON)
o In order for an Ambulatory Surgery Center or Imaging Center to operate in full
capacity, a CON must be secured by the state of Alaska. The CON
process/program consist of presenting the state of Alaska legitimate rationale of
why CLIVIA services are necessary and provide lack of services within the area.
• Federally Qualified Health Center (FQHC)
o Securing a FQHC certification provides access to funds from the Human
Resource & Services Administration, in order to achieve this is geared toward
community-based facilities.
• Intersocietal Accreditation Commission (IAC)
o The achievement of an IAC provides improved healthcare measures pertaining to
diagnostic imaging and vascular studies.
• The Joint Commission
o The Joint Commission is not only a gold standard of accreditation of healthcare
service, but it is also the only accreditation agency the state of Alaska recognizes.
• Department of Health & Human Services
o HHS within Alaska has discussed changes in expanding the scope and changing
the collaboration agreement requirements for APP's. These changes have yet to
be released yet could impact our utilization of the resources.
The Marketing plan
The following will outline the overall Marketing plan from entry of the market and addressing the
5P's of marketing: Product, Price, Promotion, Place and People.
21
Overall Marketing Strategy
The overall goal and strategy are twofold: 1) The marketing strategy's external goals are to educate patients that there is a private practice that is 100% vertically and horizontally integrated, allowing
key specialties to be under one roof, adding to convenience and continuity of care. 2) to attract
superior talent, marketing the organizational strategies that CLIVIA leverages in order to combat physician burnout and vivid organization citizenship behavior will be the approach i.e. APP model
addressed above.
People:
When patients identify the CLIVIA care leaf as shown above, the brand will signify vascular & imaging prestige care, a patient-centered offering a complete line of service sought to end
amputation and bellicosely treat acute peripheral vascular disease. Combating physician burnout is
the epicenter of how we distinguish ourselves from the competitors, we've incorporated burnout
mitigation strategies in which 5P sector:
CLIVIA provides a host of health services as discussed and executed within the Outpatient
Endovascular Interventional Suite, Ambulatory Surgery Center and Imaging Center. Each visit
type, as well as procedure/surgery, is scheduled for an adequate amount of time to ensure
1) The patient feels that's enough time was allotted for questions and
2) The surgery has enough time to provide the procedure with room for complications and delays
thus mitigation additional stress and pressure.
Strategic gaps are embedded in the surgeon's and APP's schedule referred to as "rejuvenation
time," allowing time for the provider to either catch-up, take a breather, or time to partake in any
destressing/recreational activities of their choosing. Physicians are involved during the design and
evaluation of the allowed times and averages to ensure buy-in and efficiency. During patient check-in and physician interviewing, these key benefits are communicated to demonstrate our focus
further.
Embedded into our talent acquisition practices, all employment recruitment initiatives for physicians are acutely informed of the APP leveraging in order to mitigate physician burnout. More
specifically, during all pre-interviews, physicians must participate in a physician burnout

22
assessment to understand their current burnout condition and garner feedback on their awareness of physician burnout. The approach is also masked by asking the physician their preferred activities
during their recreational time such as traveling, sports etc in order to build this into the
"rejuvenation time" discussed previously.
All physician recruitment ads will incorporate the above-referenced burnout statistics within the ad to justify why CLIVIA leverages APP's rotation to mitigate such burnout syndrome. The APP
employment ad will be driven to harness more surgical and clinical autonomy with lucrative
incentive potential.
Product/ Services:
Specific Services:
Vascular Surgery
Conditions treated:
Aortic aneurysm
Aortic dissection
Aortic ulcers
Aortic valve disease Arteriosclerosis / atherosclerosis
Arteriovenous fistula
Arteriovenous malformation Blood clots
Carotid artery disease
Chylothorax Chylous complications
Chylous effusions
Critical limb ischemia
Deep vein occlusions
Deep vein thrombosis
Ehlers-Danlos syndrome
Fibromuscular dysplasia
Intestinal ischemia Klippel-Trenaunay syndrome
Lymphedema
Marfan syndrome Median arcuate ligament
syndrome
Nutcracker syndrome Pelvic congestion syndrome
Peripheral artery disease (PAD)
Popliteal artery aneurysm
Renal aneurysms
Renal artery stenosis
Takayasu's arteritis
Thoracic outlet syndrome
Thrombophlebitis Varicocele
Varicose veins
Vascular infections and complications
Vascular malformations
Venous diseases Venous leg swelling
Venous tumors
Venous ulcers
Vertebral artery disease
Procedures / Surgeries:
Aortic aneurysm repair Aortocaval fistula repair
Aortoenteric fistula repair
Arteriovenous fistula surgery Arteriovenous malformation
surgery
Bypass surgery
Carotid angioplasty and stenting Carotid artery stenting
Carotid endarterectomy
Celiac artery bypass
Coronary angioplasty and stents Endovascular reconstruction
Endovenous laser therapy
Ex vivo renal artery reconstructions
Inferior vena cava (IVC) filter
retrieval
Inferior vena cava (IVC) placement
Laser ablation
Mesenteric artery bypass
Open vascular reconstruction Radiofrequency ablation
Renal artery angioplasty
Renal artery bypass Renal artery endarterectomy
Stenting to repair aneurysms
Subfascial endoscopic perforator
surgery Thoracic duct embolization
Thoracic outlet decompression
Thrombectomy

23
Vascular stenting Vein removal
Vena cava reconstructions Vertebral artery reconstructions
Radiology
Diagnostic Radiology Procedures:
Abdominal
Breast imaging
Mammography
Magnetic resonance
imaging (MRI)
Ultrasound Diagnostic
Neuroradiology and
Neurointervention MRI radiology
Musculoskeletal imaging
Nuclear medicine
Pediatric radiology
Thoracic radiology
division
Vascular and
interventional radiology Angiography
Embolization (cancer
care) Computed tomography
(C.T.) scan
Dual energy X-ray absorptiometry (DEXA)
scan
Fluoroscopy
Magnetic resonance
imaging (MRI)
Mammography
Endovenouslaser ablation (minimally invasive
varicose vein treatment)
Nuclear medicine Positron emission
tomography (PET) scan
Ultrasound Uterine fibroid therapy
Vertebroplasty
X-Rays
Podiatry:
Debridement of ulcer
Digital exostectomy
Digital fusions Digital tendon transfers,
lengthening, repair
Digital/ray amputation
Excision of accessory ossicles, midfoot and rearfoot
Excision of benign bone cysts
and bone tumors, forefoot Excision of sesamoids
Excision of skin lesion of
foot and ankle Excision of soft tissue mass
(neuroma, ganglion, fibroma)
Hallux valgus repair with or
without metatarsal osteotomy (including first metatarsal
cuneiform joint)
Incision of abscess Incision of onychia
Open/closed reduction,
metatarsal fractures
Order and interpret diagnostic tests related to
podiatric patients, apply or
prescribe foot appliances,
orthotics, shoe modifications,
and special footwear
Osteotomies of midfoot Perform history and physical
exam
Plantar fasciotomy with or
without excision of calc spur Removal of foreign body
Soft-tissue surgery involving
a nail or plantar wart excision, avulsion of toenail,
excision or destruction of nail
matrix, removal of superficial foreign body and treatment of
corns and calluses
Syndactylism revision
Syndactylization of digits Tenotomy/capsulotomy, digit
Tenotomy/capsulotomy,
metatarsal, phalangeal joint Treatment of deep wound
infections, osteomyelitis

24
Nephrology
Dialysis
Hemodialysis
Peritoneal dialysis
Kidney Biopsy
Kidney Transplant
Market Analysis – Market Research & Data
The targeted market is contingent on the division within CLIVIA. Generally speaking, patients of geriatric
age who have failed to adopt a healthy lifestyle find themselves experiencing multi-system failaures. These
failures can include kidney failure, deep vein thrombosis, diabetes, and high cholesterol, leading to various vascular arterial blockages within their vascular system requiring intervention. Thus, the patient
demographics will range vastly on ethnicity yet will generally range age-wise from 50-95 years old of both
genders.
Although this is mainly for the vascular division. In addition, vascular response to acute injuries such as
shootings, stabbings and accidents in which cause a laceration which would cause the vascular surgeon to
have to control bleeding and or reestablish proper flow/revascularization.
Podiatry has a wide range of patients. The focus is a lower extremity scope, which could include poor flow
to the foot or ankle, leg structural damages, tissue / muscle complications, toe nail or phalanx phalanges injuries or fungus. Yet the specific targeted market will be males and females over 50 years of age residing
in Alaska.
Of the specialties, there are two radiologist practices, one vascular practice, three podiatry practices and
three nephrology clinics serving the entire state. According to Alaska's Department of Health & Human
Services as to patient health stats of the market, approximately 88% of Anchorage has health coverage, of
which over 40% of the health plans are employer-driven.
Over 17% of the population is on Medicaid, which reimburses higher than Medicare, which deduced a
rate of 6% of the population, 14% on individual plans, and 6.5% is military or V.A. plans. Physicians see
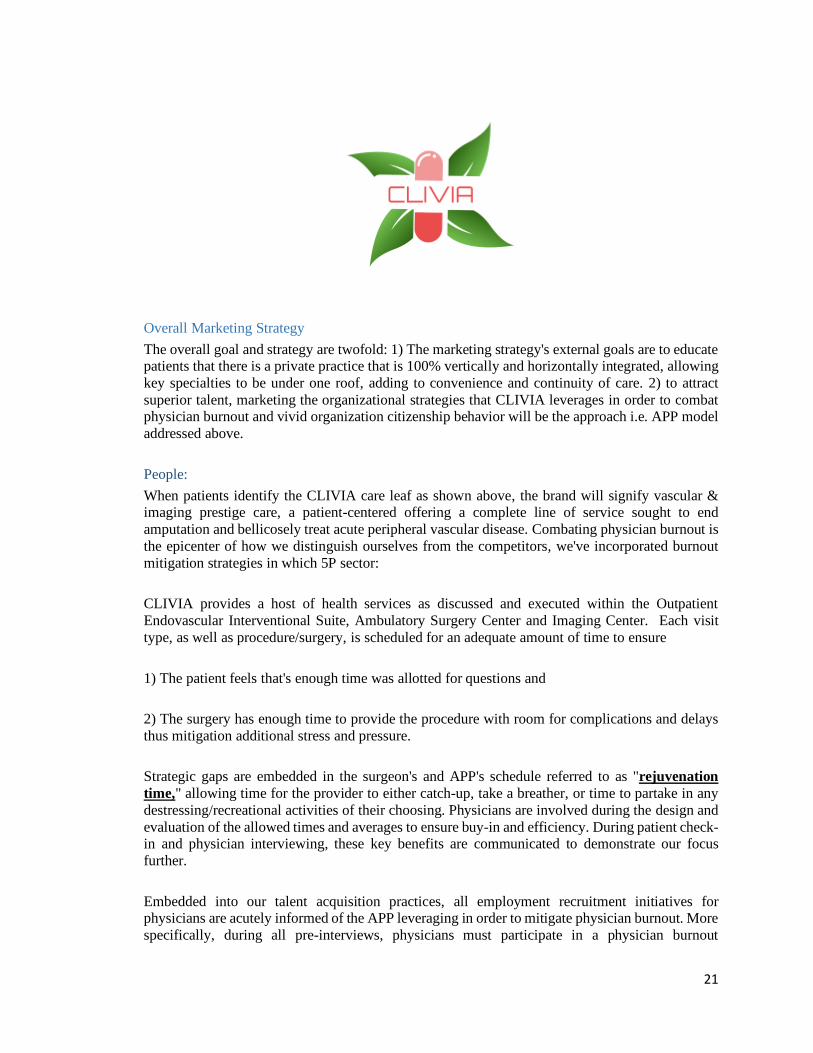
an average of 1130 patients per year yet appear to be on a downward trajectory of 2% from previous years
as shown below. As to the market's overall health, several counties of Alaska show relatively high audit
obesity and diabetes exceeding 40%.
Overall, with the prevailing healthcare facility and healthcare provider shortages spamming the state,
nearly 90% healthcare coverage and highly elevated adult obesity, CLIVIA would be positioned with
competitive advantages.
25
From a market research perspective, recent surveys state physicians work long hours which vastly
contributes to physician burnout. Both the APP and the physician are limited in the amount of hours and
bound to templates in which limits the amount of patients and surgeries can be booked. Should the
physician seek to add additional workload, they are subsequently required to reduce their workload
Competitors Analysis
Within the state of Alaska three distinct competitors in which has strong market share within the six
specialties. The following competitor listed focus predominately within the Anchorage market yet has a
patient population scope that encompasses all of Alaska. Three distinct strengths and weaknesses are
demonstrated below :

26
Financial Documentation
Summary of Financial needs:
As discussed within the financial analysis, securing 1.5 times the projected loss of $3.4
million secured by an ISDA agreement to hedge interest rates pursuant to the Pro forma below will be the
financial strategy.
Income Statement
CLIVIA is projected to produce $5.1 million in year one or $425K per month on average with a projected
monthly carrying cost of $623K or $7.47M, thus a monthly loss of approximately -$200k per year or -
$2.4M in year one. Year two is expected to generate 35% more revenue over year one summing $573k
monthly or nearly $7.0M. Projected overhead per month increases to $650k with a total yearly
expenditure of $7.8M, thus an expected loss of nearly one million. This is largely due to the full scope of
imaging services coming online in year two. Finally, in year three, a projected increase of 20% of revenue
over year two summed nearly $700K per month in revenue, with an annual revenue projection just north
of $8.2M netting a positive $60k year-end. The income statement does not reflect grant funding.
CLIVIA has placed capital expenditure/liquidity structure thresholds. More elaboratively, minimum cash
on hand should not fall below $250K years one and two; all capital infusion requirements from owners
are capped at 25% of the required outlay/revenue shortage. All dividends disbursement will be suspended
Alyeska Vascular Surgery
•Strengths
• Competitor has over 90% of vascular / acute care marketshare
•Competitor has an Outpatient Interventional Suite (OIS)
•Strateghic strategic alliance / partnership with nephrologist / podiatry
•Weaknesses
•Practice is not equipped with the radiology speciality
•Practice is not a Imaging center or in possession of a Certificate of Need (CON)
•Limited Number of providers to serve the population demand - mismatch of labor supply for care demand
Alaska Heart & Vascular Insistute
• Strengths
• Competitor has over 90% of cardiology market-share
• Competitor has over 30 cardiologist and interventionalist
• Financial backing / contractual partnership with large hosptials
•Weaknesses
• Practice is not staffed with vascular surgeons
• Limited experience and exposure to Crtical Limb Ischemia
• Cardiology focus only
Imaging Associates
• Strengths
• Competior has over 90% of outpatient imaging due to joint venture with large hospital
• Competitor has over 15 Radiologist of which several are inventionalist
•Has several location with CT, has the only PET/CT in market, demand to influence cyclotron radiation dose for market
•Weaknesses
• Practice is not satffed with vascular surgeons
• Predominate focus on outpatient imaging
• Episodic Care model - limited long-term patient relatioship (interventional)

27
until year three. In year three, the minimum cash on hand threshold increases to $500K, capital infusion
percentage remains at 25%; dividend disbursement are then declared quarterly at 10% of net earnings.
Capital Infusion
According to the below income statement proforma, a forecasted $3.2M will be lost within the first 24
months. CLIVIA will secure a drawn-down line of credit of $4M (10 X 25) backed by an ISDA
(International Swaps & Derivatives Association) master agreement amortized over 25 years yet renewable
every ten years. The ISDA swap will allow CLIVIA to hedge floating interest rates allowing costs to be
consistent. This draw-down loan will only be utilized to cover losses for the first 24 months.
Balance Sheet
CLIVIA will initially operate on the capital infusion funds explained above once funds are secured. In
summary, in year one, we will procure medical equipment (fixed assets) in the amount of $2.4M (includes
I.T.), $99K in office furniture, deducing $2.5 in total assets. As stated above, all medical equipment will
be leased, which reflects in the long-term note of the liabilities, ending with the long-term liabilities
capital infusion of CLIVIA's draw-down line of credit of $2.3M. Cash on hand threshold expected to be a
minimum of $200K, primarily due to drawn down overage, CLIVIA will secure at least $800K in federal
grant funds as explained above, showing current assets of $1.05M.
An additional capital improvement outlay of $500K will be invested to assist in the opening of the
imaging center, increasing assets to $4.1M. As payments are made, our long-term note on medical
equipment will decrease; accordingly, long-term liabilities will increase the exact amount of the projected
loss of approximately $888K as expressed in the income statement. Lastly year three, CLIVIA will secure
a $1.5M, which substantially increases current assets; all other liabilities are projected to decrease
accordingly, resulting in positive retained earnings in year three.
Cash Flow Statement
As discussed within the income statement, 2021 has a revenue projection of $5.1M from revenue
operations yet will have $6.5M in operating expenses; cash flow stemming from operations activity is
projected to net a $1.4M loss. As to investing activities, the payments remitted toward the medical lease
purchase will be captured in addition to furniture assets which will sum an outlay of approximately -
$600k total (rounded).
Regarding financial activities, CLIVIA will draw-down on its line of credit, therefore monies borrowed of
approximately $2.5M in anticipation to offset the projected loss of year one, netting a positive cash
position of $430K.
Year two revenue is projected at $6.8M coupled with a federal grant of $850K netting cash flow from
operations to be $844K. As to investment activities, the standard yearly outlay for medical equipment
liability with an additional $500k investment toward imaging center activities summing nearly $1M
(rounded) in investing activities for 2022.
As to financial activities, an additional $888K will be drawn-down from the line of credit in anticipation
of the projected loss accounting for positive cash. However, the drawn-down line of credit repayment
period starts 2022, resulting in total yearly expense payments of $419K. This deduces a net of $468.8K in
financing activities, thus a year-end projection of $315.5K in net cash flow.
Year three reflects a revenue projection of $8.2M coupled with a federal loan of approximately $1.5M,
summing a net positive cash position of operations of $2.5M. Investment activities remain stable with

28
standard payments to medical equipment of $498K and financial activities only reflecting repayment
outlays of $419k, netting a year-end cash position of $1.5M.
APP Interactive Return on Investment Dashboard
The APP interactive dashboard tracks all CPT code claim activity and funds received per provider; the
revenue generated quarterly / yearly is then compared to the employees' overall expense, thus treating
each APP as a micro cost center. As stated above, when a surgery assist fee can be generated, the APP is
scheduled with the physician accordingly, which directly impacts these figures.
The orange table serves as the cost allocation category for the employees' overall associated expenses
such as salary, employer taxes, health insurance premiums paid by the employer, etc. For example, the
APP analysis shown in appendix X denotes an employee with a salary of $110k per year, with a
summation of $137.4K per year or $34.3k per quarter with all associated costs. This dashboard has built-
in formulas allowing items such as salary to be adjusted, and all other associated costs will adjust
accordingly. Also shown is a pie chart that factors all related costs in a percentage depiction; in the
sample, it is easy to denote salary accounts for the majority (80%) of the overall APP's costs.
The blue table calculates the quarterly revenue averages of the APP, then compares said average to the
fixed quarterly costs of the APP, and deduces a profit or loss. In this example, the APP generates $44K in
revenue per quarter, with an overhead of $34.3K, therefore, yielding $9.6k in profit. As stated above, each
APP is entitled to a percentage of their profit. The gray table depicts the percentage of profits the APP is
entitled to and the minimum payout threshold that must be achieved.
The green table sums each quarterly revenue, determines the number of encounters / assigned surgeries,
most used CPT code, and overall return of investment of the APP.
The yellow table is referred to as a "what if scenario employee revenue analysis" which allows the
administrator to plug in a CPT scenario to determine which capacity the APP will yield most from a
financial perspective. For example, the current figures propose a scenario where the APP is currently
scheduled for a clinical day, which is projected to produce $3,750.00. The tool reviews the visit type in
comparison with the insurance payer and quantifies an estimated claim reimbursement. More specifically,
concerning the clinic, estimated E&M codes according to visit types are evaluated and calculated. It then
provides the average clinic claim reimbursement of the APP in question, which in this situation is
$3,000.00. This is then compared to a scenario where the physician has added several surgeries and is
requesting an APP to assist them with said surgeries. The administrator can enter said CPT codes, and the
algorithm would calculate an estimated claim reimbursement, which in this scenario is $4,800.00
compared to their average of $3,600.00. Should the decision be purely based on financial return, the what-
if scenario analysis depicts the APP will yield more in a surgical assist capacity over the clinic.
Overall, each APP can mitigate physician burnout by keeping the physician's focus on surgery and
building and sustaining micro-cost centers that are proven to be beneficial financially to both the APP and
the practice.
Shown below are the three Pro Forma Financial Statements forecasting 36 months of activity and the APP
Interactive Return on Investment Dashboard:

29
Pro Forma Income Statement

30
Pro-Forma Balance Sheet CLIVIA For 2021 to 2023
(all numbers in $000) Pro Forma Balance Sheet
ASSETS 2021 2022 2023
Current Assets
Cash $200,000 $200,000
Net accounts receivable
Federal Grant Funds $850,000 $1,500,000
Surgical Inventory
Temporary investment
Prepaid expenses
Total Current Assets $1,050,000 $1,700,000
Fixed Assets
Long-term investments
Land
Tenant/Cap Improvements $500,000
Buildings (net of depreciation)
Medical equipment (net) $2,490,000 $2,490,000 $2,490,000
Furniture & fixtures (net) $99,600 $99,600 $99,600
Total Net Fixed Assets $2,589,600 $3,089,600 $2,589,600
TOTAL ASSETS $2,589,600 $4,139,600 $4,289,600
LIABILITIES Current Liabilities
Accounts payable $0 $0 $0
Short-term notes $0 $0 $0
Current portion of long-term notes $2,490,000 $1,992,000 $ 1,523,880.00
Accruals & other payables
Total Current Liabilities $2,490,000 $1,992,000 $1,523,880
Long-term Liabilities
Mortgage
Operating Capital Infusion $ 2,354,108.00 $ 2,958,807.00 $ 2,539,599.00
Total Long-term Liabilities $2,354,108 $2,958,807 $2,539,599
SHAREHOLDERS' EQUITY
Capital stock
Retained earnings ($2,254,508) ($811,207) $226,121
Total Shareholders' Equity ($2,254,508) ($811,207) $226,121
TOTAL LIABILITIES & EQUITY
$2,589,600 $4,139,600 $4,289,600

31
CLIVIA 3-Year Cash Flow Statement
Cash Flow Statement
For the Year Ending 12/31/2021 12/31/2022 12/31/2023 Cash at Beginning of Year 15,700 445,700 761,275 Cash at End of Year 445,700 761,275 2,351,781
Operations 2021 2022 2023 Cash receipts from
Patient Fees 5,100,000 6,885,000 8,262,000 Federal Funds 850,000 1,500,000
Cash paid for
Administration & General (180,000) (189,000) (208,373) Wages & Salaries (5,600,000) (5,880,000) (6,174,000) Rent (396,900) (408,807) (433,703) Surgical Supplies (120,000) (126,000) (132,300) Imaging Supplies (180,000) (189,000) (198,450) Clinical Supplies (60,000) (63,000) (66,150) Misc. Other (25,500) (34,425) (41,310)
Net Cash Flow from Operations (1,462,400) 844,768 2,507,714
Investing Activities Cash receipts from
Sale of property and equipment Collection of principal on loans Sale of investment securities
Cash paid for
Purchase of property and Medical equipment (597,600) (498,000) (498,000) Tenant / Cap Improvements (500,000) Making loans to other entities Purchase of investment securities
Net Cash Flow from Investing Activities (597,600) (998,000) (498,000)
Financing Activities Cash receipts from
Issuance of stock Borrowing (Capital infusion) 2,490,000 888,015
Cash paid for
Repurchase of stock (treasury stock) Repayment of loans (419,208) (419,208) Dividends
Net Cash Flow from Financing Activities 2,490,000 468,807 (419,208)
Net Cash Flow 430,000 315,575 1,590,506

32
APP Interactive ROI Dashboard
Innovative Elements & Operational Outcomes
Positive Impact As stated above, the state of Alaska, according to HSRA, is deemed a medically underserved area to
include being in a state of a professional medical shortage. This results in patients unable to receive the
treatment within the community in which they reside, thus resulting in innate delays of care, limited
options, increased amputations that negatively impact the patient population's morbidity, or transferring
the patient out of state for further treatment. CLIVIA becomes the solution to mitigate and or eliminate
the above by providing a one-stop solution with its multi-specialty approach to treatment and limb
salvage. With this solution it allows Alaskans to be treated in the community in which they reside.
From a physician burnout mitigation perspective, over 58% of physicians who experience burnout state
the number one cause of the syndrome is due to too many bureaucratic tasks; CLIVIA's model ensures the
APP absorbs this to ensure this number one cause isn't a factor. Secondly, CLIVIA has organizational
structures to identify if the physician has worked over the allowed threshold in order to ensure the number
two cause of physician burnout is also mitigated. More sharply, the number two cause for physician
burnout is "spending too many hours at work." Lastly, the third leading cause is the lack of respect from
administration; as stated above, physicians are leveraged heavily with respect to physician feedback
through surveys, strategic meetings, and complete control of the diversity of cases/ schedules/resources.
Without a firm such as CLIVIA, the current state statistics will continue to rise. One of Alaska's
healthcare facilities stated a minimum of one patient is transferred out of state for further treatment due to
Alaska's inability to treat adequately. The vertical and horizontal approach coupled with medical
technology allows critical limb ischemia to be treated effectively while protecting CLIVIA's physicians
from burnout symptoms.
Challenges
The challenges encountered during this journey were essentially how to develop a sustainable practice
while incorporating an organizational strategy that mitigated a grown crisis i.e. physician burnout. On the
surface level developing a medical practice is relatively simple, yet if the medical demand for the services
in question are not sustainable, insolvency of said practice is imminent.

33
Contrarily, if the demand curve for medical services is such that the physician is overly exhausted and
compounded with the health professional shortage, healthcare quality is negatively affected. It was critical
to ensuring that the model shifted key physician burnout contributors from physicians to avoid negative
impact. More sharply, even when identifying a need for healthcare services, many regulatory tape
presents itself, making it increasingly difficult to execute from Certificate of Need requirement, referral
restrictions due to stark provisions.
The financial component is rather complex as new practices seek to secure funds for operations. Much
was learned regarding the certificate of need requirements and various grant funding offered to medically
underserved facilities.
Outside of the regulatory and financial aspects of opening the practice, physician burnout continues to be
a concern, burnout by work setting according to Medscape research of 2021; Healthcare organizations are
47% likely to experience burnout while outpatient clinics are 46% and office-based multi-specialty is
44%. It was/is imperative CLIVIA continues to adopt and implement organizational strategies to mitigate
this syndrome. The challenge will be to ensure CLIVIA's organization strategies are geared toward
supporting top-reducing burnout relievers to ensure compensation is competitive and appropriate to avoid
financial stress.
In addition, to ensure the physicians' work and schedule are manageable while the culture supports and
encourages mutual respect and appreciation. Furthermore, this model's framework has a calculated risk;
due to leveraging APP's more within clinic, the patient builds a strong relationship with the APP
compared to the surgeon. This could increase the overall risk profile of the surgeon if an adverse outcome
were to surface.
Next Steps
To initiate the above project, first steps would be to secure a state of Alaska business license, devise an
operation agreement, develop articles of incorporation, select a few members for the Board of Directors,
and secure operational funds.
Yet perhaps the fundamental elements are to identify like-minded physicians and administrators who
believe and can support CLIVIA's mission. The physician burnout strategies are vital within the
organization's foundation of operations to attract superior talent and sustain high engagement and
employee satisfaction. The key will be to identify the right individuals and ensure they are in the right
seat within the organization to achieve the mission to provide excellent patient-centered healthcare while
mitigating amputations and inspiring hope to foster improved life experience.
Conclusively, the culture must unequivocally advocate actions that seek to materialize the vision to
prolong humanity's life while leveraging resources to mitigate physician burnout.

34
Appendixes & Illustrations:
Medical Underserved Areas & Populations – Appendix A

35
Health Professional Shortage Area (HPSA) – Appendix B
Market Space – Practice Location – Appendix C

36
Administrative Plan: Workflow – Appendix D

37
Strategic Roadmap Milestone – Three-year Strategic Plan

38
CLIVIA Organizational Chart
Physician CEO
Dir. Clinical Operations
Nursing Manager
Registered Nurses
Medical Assistants
Patient Care Techs
Billing & Coding Manager
Medical Coders
Medical Billers
Outpatient Interventional Suite Mgr.
Registered Cardiovascular
Interventional specialists
Scrub Techs
Dir. of Vascular Surgery
Vascular Surgeons
Advance Practice Providers (PA's & NP)
Dir. of Podiatry
Podiatrists
Advance Practice Providers (PA's & NP's)
Dir. of Radiology
Radiologists
Technical Dir of Imaging
Radiology Technicians
Technical Director of Ultrasound
Sonographers
Advance Practice Providers (PA's & NP's)
Dir. of Nephology
Nephologists
Advance Practice Providers (PA's & NP's)
Chief Executive Officer
Med Staff Dir. of Administration
Human Resources Accounting

39
APP ROI Dashboard – Appendix X