Embed Size (px)
Citation preview

practice changing practice
16 Nursing Times 2 February 2010 Vol 106 No 4 www.nursingtimes.net
Keywords dyiNg | PalliaTiVe care | criTical care
While policy has been a driver for this project, on its own it is not enough to ensure success. The following are vital: a clear purpose and objective; preparation and planning before implementation; and reflection and revision.
Projects like this enable those involved to gain enormous satisfaction, which regenerates clinical practice and creates expert practitioners.
Practice POiNtS
Implementing a pathway for end of life care can aid decision making and clarify treatment plans and goals for critically ill patients. A trust explains how
How to improve services for dying patients in critical care: adapting protocols
AUTHOR Jane Morgan, BSc, RN, is staff nurse, critical care, Colchester Hospital University Foundation Trust.ABSTRACT Morgan J (2010) How to improve services for dying patients in critical care: adapting protocols. Nursing Times; 106: 4, 16-18.This article outlines a project to improve end of life care for those who are critically ill, by adapting and implementing a national protocol specially developed for the intensive care unit. The rollout of the pathway is discussed along with an audit which found the trajectory towards death following withdrawal of treatment can be swift. The extent of documentation is, therefore, an important consideration to ensure nurses can balance patients’ needs with those of grieving relatives while ensuring bereavement care is accurately documented.
INTROdUCTIONWe identified a need to improve care of dying patients in critical care (see Background box).
We decided that following the Liverpool Care Pathway (LCP) for the dying patient would be beneficial. Already familiar with Integrated Care Pathways (ICP), the LCP was the obvious vehicle for change.
We decided to adapt the generic LCP to suit our purpose and patient group: those who are critically ill. This coincided with work by John Ellershaw and the Liverpool Hospital palliative care team who were about to publish the LCP for the intensive care unit. As a result, we adopted this national pathway for ICU with minor amendments, while keeping the original format.
THe pROCeSSWe set up a focus group to ensure we worked with clinicians during the project’s design and implementation. The group comprised 10 nurses of different grades and its aim was to maximise dissemination of the LCP across the unit.
We registered with the Marie Curie Palliative Care Institute ICU Action Research Project, which provided support, a template for the LCP in ICU and use of the LCP 10 steps continuous quality improvement programme (Marie Curie Palliative Care Institute Liverpool, 2009; 2007). This programme brought with it resources and reliability beyond the scope of a small trust project, making implementation cost effective in terms of time, expertise and people.
The transferability of the quality improvement programme to the critical care unit needed sensible application, as the resources trusts can offer dying patients varies according to organisation and staff. It is important to be realistic about what can and cannot be changed. Our palliative care service is fairly minimal; extra work would be burdensome. A solution was to create links with the local hospice, which could also prove to be useful when rapid discharge from ICU becomes part of end of life care.
pRepARINg FOR CHANgeBeing responsible for planning and implementing change in practice/behaviour involves bringing about a cultural shift. As end of life care in critical care is possibly more varied and complex than other areas of the hospital, this will take time, from both a personal and professional perspective.
It is imperative to have a thorough
understanding of the legal and ethical issues involved. In the UK, the legal practice of withholding and withdrawing treatment is determined by doctors, although usually carried out after a consensual decision making process involving other professionals and family members. Moreover, we live and work in a multicultural and ethnically diverse society, which requires greater understanding and sensitivity.
It was therefore necessary to conduct a literature review to understand end of life care in critical care. This review reinforced the notion that deep seated beliefs affect care of dying people (Morgan, 2008).
To raise awareness and promote the project, regular meetings gave healthcare professionals the opportunity to: l Meet the end of life care coordinator for the PCT; l Learn how to complete the LCP; l Understand variations in care; l Reflect on care of dying people.
This process empowered clinicians and enabled them to disseminate knowledge to other staff. Subsequent education and support was delegated to key members of staff.
The focus group was keen to offer bereavement care and felt the synergy between the LCP and a bereavement service for ICU was inescapable. This provided the opportunity to capitalise on earlier work, which had identified the need for ICU bereavement care. As two different strands of care were being implemented at the same time, we planned a staggered rollout.
A range of major government initiatives have highlighted the need to improve the care of dying patients, including the DH’s (2008) end of life care strategy and report on this (DH, 2009).
We used the Marie Curie Palliative Care Institute Liverpool’s (2007) Liverpool Care Pathway for the dying patient within the intensive care unit version 11 in drawing up our care pathway.
BackgrOuNd

17Nursing Times 2 February 2010 Vol 106 No 4 www.nursingtimes.net
This arTicle has beeN double-bliNd Peer-reViewed
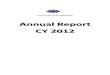
Goal 13 – GP practice contacted regarding patient’s death date
Goal 14 – Procedure for laying out discussed Goal 15 – Procedure following death
discussed or carried out Goal 16 – Family/other given information on
procedures Goal 17 – Hospital policy followed for patients’
valuables and property Goal 18 – Documentation and advice is given
to the appropriate person Goal 19 – Bereavement leaflet given
graPh key: care after death
Al Grant weds 27th
Al Grant weds 27th
13 14 15 16Goals
17 18 19
100 100 35 70 15 95 60
65
305
85
40
0
10
203040
6050
7080
10090
%
Yes No
fig 1. Pre-imPlemeNtatiON Pathway feedBack – care after death
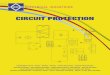
13 14 15 16Goals
17 18 19
65 60
5
50 50 55 50 45
50 50 5045
55
0
10
203040
6050
7080
10090
%
MissingAchieved Variance
3530
5
fig 2. POSt-imPlemeNtatiON Pathway feedBack – care after death
al g
rant
LAUNCHINg THe CARe pATHwAyDocumentation for the LCP ICU was approved and the launch date was set for early autumn in 2007. This allowed enough time to gather data for a base review. It was important to examine practice before implementation to measure change after the launch. Data was collected on 20 level 3 patients (those requiring advanced respiratory support, as defined by the Intensive Care Society, 2002), following withdrawal of treatment in critical care.
As the trust had already signed up to the national end of life care programme (see www.endoflifecare.nhs.uk), gaining permission for the audit was a formality.
data collectionComputerised analysis and feedback was provided by the Marie Curie Palliative Care Institute Liverpool and contributed to their national research project.
Initial observations reinforced the need to adhere to legal and professional requirements, as some documentation was missing (Figs 1 and 2). In addition, GPs are rarely made aware of patients who are dying, but routinely notified after death (goal 13).
Under these circumstances the pathway for ICU acts as a prompt. A cultural shift in end of life care is evident when ICU doctors involve GPs in the decision making before withholding or withdrawing treatment.
Aspects of care thought to be embedded in practice, such as providing explanations and advice booklets after death for relatives were, according to the documentation, carried out in part.
When documentation is poor it is difficult to ascertain if, or how, the needs of dying people and their families have been met.
Completing documentation was a main teaching point in the education programme.
The base review also produced some incidental findings. For example, compared with Wunsch et al (2005), who found the median time to death after withdrawal of treatment was 2.4 hours, our time was longer. This was surprising, but may not be a reliable representation of events due to the snapshot sample and variation in participants. Also, it was apparent that decision making often occurred between 10.30am and noon, with death following some 45 minutes to six hours later. This reinforces the idea bedside nurses have absolute responsibility for the LCP ICU during their shift, as 12 hour shifts mean they are likely to see the care episode through from decision making to withdrawal of treatment to death. This was another point to consider during the education programme.
IMpLeMeNTATIONThe pathway’s rollout was gradual and based on an average of two deaths a week,
remembering that not all deaths in critical care follow withdrawal of treatment.
After training, there was a “hands on” phase where key nurses were the first to use or support staff using the pathway. This was because findings from the base review supported a step by step programme. However, compliance increased as nurses appreciated the authority to stop inappropriate treatments, which reflected findings by Lhussier et al (2007). Also, once the decision had been made to withdraw treatment, the pathway enabled a course of actions, which would have otherwise been ambiguous and subject to variation. Furthermore, as Lhussier et al (2007) said, the end of life ICP used by
trusts in the north of England promoted an enhanced openness between families and healthcare professionals.
Continued education ensures staff understand the documentation and also wider issues such as communication, symptom relief and spiritual and cultural awareness. As part of the educational

practice changing practice
18 Nursing Times 2 February 2010 Vol 106 No 4 www.nursingtimes.net
programme, feedback was considered essential. Many methods were chosen, including: one to one, group and critical care meetings; the intranet; publications; and an inter-hospital multidisciplinary team study day.
A more formal means of reflection involved a post-pathway analysis: 20 pathways were audited and submitted to the LCP Central Team UK for computer analysis and feedback. Improvements were expected and some were found, but these were not the issue. Strangely, bereavement
care that was accurately documented pre-implementation was comprehensively absent after it. This was attributed to the size of the document versus the speed of death, as the trajectory towards death following withdrawal of treatment can be swift and extremely demanding for nurses, who must balance patients’ needs with those of grieving relatives and extensive documentation. Slower and “traditional” palliative care deaths afford more time for patients, relatives and documentation.
The response to this audit finding was to
renew the educational input, reduce the number of pages and make the documentation more concise. These changes were appreciated and await audit before any further modification.
CONCLUSIONThe LCP for ICU has facilitated quality care during the final hours of life. Furthermore, the pathway is acknowledged during decision making, which helps to clarify treatment plans and goals for critically ill patients. l
Telling talesVisit nursingtimes.net the UK’s Nº1 nursing website for essential informationFront-line nurses, clinical specialists and national opinion leaders tell it like it is - Nursing Time’s blogging team has something for everyone. nursingtimes.net/blogs
nursingtimes.net the UK’s Nº1 nursing website
newlook
Nursing Times Learning is a new way for you to update your knowledge and skills. Our online learning units are written by experts using case scenarios.
For an online learning unit on Nausea in Oncology and Palliative Care go to:
nursingtimes.net/learning-nausea
Department of Health (2009) End of Life Care Strategy: First Annual Report. london: dh. tinyurl.com/end-of- life-stratDepartment of Health (2008) End of Life Care Strategy. Promoting High Quality Care for All Adults at the End of Life. london: dh. tinyurl.com/eolc-stratIntensive Care Society (2002) Levels of Critical Care for Adult Patients: Standards and Guidelines. london: intensive care society. tinyurl.com/
crit-care-standLhussier M et al (2007) The evaluation of an end of life integrated care pathway. International Journal of Palliative Nursing; 13: 2, 75-81.Marie Curie Palliative Care Institute Liverpool (2009) 10 Step Continuous Quality Improvement Programme for Care of the Dying Using the LCP. liverpool: McPcil. tinyurl.com/lcP-in-icuMarie Curie Palliative Care Institute Liverpool (2007) Care of the Dying
Pathway (LCP) Hospital Intensive Care Unit – ICU. liverpool: McPcil. tinyurl.com/lcP-in-icu Morgan J (2008) end of life care in uK critical care units – a literature review. Nursing in Critical Care; 13: 3, 152-161.Wunsch H et al (2005) end of life decisions: a cohort study of the withdrawal of all active treatment in intensive care units in the united Kingdom. Intensive Care Medicine; 31: 6, 823-831.
ReFeRenCeS