Embed Size (px)
Citation preview

Practical TB Infection Controlfor
Community-based TB Programs
Kevin Fennelly, MD, MPH
Center for Emerging & Re-emerging PathogensInterim Director
Division of Pulmonary & Critical Care MedicineUMDNJ-New Jersey Medical School
[email protected] June 2008

Objectives• To help identify situations in which there is
an increased risk of TB transmission– people (patients) and places (settings)
• To recommend practical solutions – for programs to help protect staff
• principles and provisions
– for staff • knowledge is power … and prevention !!

Areas I will NOT cover
• Abundant evidence that HCWs are at increased risk for occupational TB infection (and disease)– HCW= anyone exposed to patients
• Risk assessment– Would consider most environments in TB-
endemic countries at high risk

Riley experimental TB ward
from Sol Permutt, 2004

TB is transmitted by aerosols (NOT sputum)

*NOT organism size
Particle size* & suspension in air
• Particle size & deposition site– 100 – 20 – 10 – upper airway– 1 - 5 – alveolar
deposition
• Time to fall the height of a room– 10 sec– 4 min– 17 min– Suspended indefinitely
by room air currents
from Sol Permutt, 2004

Estimates of Mtb Aerosol Production (quanta per hour)
TB ward: pt on Rx
Cavitary TB: no Rx
Laryngeal TB
Bronchoscopy/ETT
Autopsy
1.25
13
60
250
1000
- Fennelly KP. Int J Tuberc Lung Dis 1998; 2: S103

Who is Infectious?
• Sputum smear + > smear –– AFB 3-4+ > AFB 1-2+
• Cavitary > non-cavitary• Close > casual contact• Prolonged > brief contact• Men > women• Young > old
• Borgdorff MW et al. Am J Epidemiol 2001; 154:934
• HIV+ = HIV – • Cruciani M et al. Clin Infect Dis 2001; 33:1922
• MDR vs. DS: ?

Where are Patients Most Infectious?
• Congregate settings– Hospitals– Correctional facilities– Bars– Choirs– Airplanes, ships
• Indoors >> outdoors– Increased with crowding & proximity– But no data on UV-A or UV-B effects

When are Patients Most Infectious?
• Coughing > Singing > Talking• Loudon RG et al. Am Rev Respir Dis 1969;100:165
• Aerosol producing procedures: intubation, bronchoscopy, sputum induction
• Sepkowitz KA. Clin Infect Dis 1996;23:954
• Not on treatment– Unrecognized/undiagnosed– Drug-resistant on standard therapy

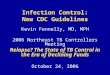
H ouseho ld Mem bers w ith P ositive TS Ts by C ough Frequency
0
10
20
30
40
50
Few Moderate Frequent
O v e rnight C ough Fre que ncy
Per
cen
t H
HC
s w
ith
TS
T+
Loudon RG Am Rev Respir Dis 1969, 99: 109.
Cough Frequency & Infectiousness

What is Infectious?
• Dogma: 1-5 micron infectious droplet nuclei (Wells, 1955)– Risk associated with prolonged exposures
• Reality: Wells estimated particle size distribution based on experimental nebulization of bacillary suspensions in lab
– No data from patient-generated aerosols
– Wells calculated droplets less than 25 microns dessicated to size of infectious droplet nuclei in less than one second

Cough Aerosol Sampling System
- Fennelly KP et al. Am J Resp Crit Care Med 2004; 169; 604-9

Six-stage Andersen cascade impactor
Andersen AA. J Bacteriol 1958;76:471.

Cough-generated aerosols of M.tb National Jewish Medical & Research Center
- Fennelly KP et al. Am J Resp Crit Care Med 2004; 169; 604-9


Cough Aerosol Sampling System

Frequency Distribution of Cough-generated Aerosols of M. tuberculosis and
Relation to Sputum Smear Status
0
0.5
1
1.5
2
2.5
3
3.5
1 7 13 19 25 31 37 43 49 55 61 67 73 79 85 91 97 103 109
Subjects Sorted by Aerosol CFU then by Sputum AFB
Aer
oso
l Lo
g C
FU
0
1
2
3
4
5
Sp
utu
m A
FB
Aerosol Log 10 CFU Sputum AFB

1 2 3 4 5 60
10
20
30
40
50
Stage of Andersen Cascade Impactor
Pe
r C
en
t C
FU
Cough-generated Aerosols of M. tuberculosis:
Normalized Particle Sizes
Lower limit of size range(µ) 7.0 4.7 3.3 2.1 1.1 0.65
Deposition Upper airway - bronchi -- alveoli
Abstract, ATS International Conference, 2004.

Cough Aerosol Production:Multivariate Analysis
• Best model in logistic regression– Bacillary concentration: BACTEC™ < 4 days to positive
(OR=11.35, p=0.02) and – strong cough (OR=5.41, p=0.04)
• Cough strength is associated with performance score (physical health) (Chi-square, p=0.004).
– Cough strength tends to be associated with CD4 counts (less advanced HIV infection) (Chi-square, p=0.07).
– CD4 counts and performance scores drop out of multivariate models probably due to correlation with cough strength.
• These data suggest that healthier patients are more likely to be infectious than very ill patients.

0.75 1.00 1.25 1.50 1.75 2.00 2.250
1
2r = 0.77(p<0.001)
Log Aerosol Mtb CFU by Andersen
Lo
g L
un
g C
FU
Da
y 0
Aerosol CFUs Predict Infectivity in Mice
Abstract, Keystone Symposium on Tuberculosis, 2005.

Probability of MTB Infection: Isolation Room with 6 ACH:
Infectiousness and Duration of Exposure
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0.1 1 10 100 1000
Duration of Exposure (hours)
Ris
k o
f M
TB
In
fecti
on
1
10
100
1000

Assumptions: Homogenous distribution of infectious aerosol over 10 hours; uniform susceptibility.
- Fennelly KP & Nardell EA. Infect Control Hosp Epidemiol 1998; 19;754
Wells-Riley Mathematical Model of Airborne Infection

Summary: PrinciplesTB-IC for Community Programs
• The most infectious TB patients are those who are not on appropriate therapy– Undiagnosed, i.e., unrecognized– Drug resistant
• TB is transmitted by aerosols– Coughing and bacillary load important– Healthier patients may be more infectious
• Poorly ventilated indoor environments the highest risk

Summary: PracticesTB-IC for Community Programs
• Best administrative control: – Suspect and separate until diagnosed– Surveillance of HCWs with TST (and/or IGRAs) and rapid
treatment of LTBI if conversions occur
• Best environmental control: Ventilation– Do as much as possible outdoors– Use directional airflow when possible
• Natural breeze or fans: HCW ‘upwind’; patient ‘downwind’
• Personal respiratory protection– N95 respirators when indoors or very close (procedures)– Surgical masks on patients to control source