Embed Size (px)
Citation preview

Practical Considerations in Managing Hepatorenal Syndrome
Juan Carlos Q. Velez, MDAssociate Professor of Medicine, Ochsner Clinical School / The University of Queensland
Chair, Department of Nephrology, Ochsner Clinic Foundation
2019 Crescent City GI, Endoscopy and Liver Disease Update
New Orleans, LA, September, 2019
@VelezNephHepato

Disclosure of Conflict of Interest
• I have served in an Advisory Board for Mallinckrodt Pharmaceuticals, maker of terlipressin
• I am a member of the Speaker Bureau for Mallinckrodt Pharmaceuticals (corticotropin gel) and for Otsuka Pharmaceuticals (tolvaptan)

Hepatorenal physiology/syndrome (HRS-1)✓ Splanchnic vasodilation, nitric oxide, decrease in SVR
✓ Renal vasoconstriction
✓ Activation of sympathetic nervous and renin-
angiotensin systems
✓ Hepatorenal reflex
✓ Increased sensitivity to vasoconstriction (endotoxin,
endothelin-1, ROS)
✓ Reduction in cortical renal blood flow
✓ Derangement in renal autoregulatory curve
ACS
Cholemic
nephropathy✓ Toxic and pro-
inflammatory tubular
injury from bile
salts, endotoxin,
intraluminal casts
(total bilirubin ~ > 20
mg/dL)
Ischemic ATN✓ Prolonged
prerenal azotemia
✓ Progression from
unresolved HRS-1
Inflammatory
ATI ✓ Endotoxin, toll
receptor
stimulation
PRA
ATI / ATN
Prerenal azotemia (PRA)✓ Decreased effective arterial blood volume
✓ GI losses: lactulose use, GI bleeding, LVP
✓ Renal losses: diuretic use
✓ Other: infections, poor po intake
✓ Cardiorenal: PoPH, high output HF,
cirrhotic cardiomyopathy
HRS-1
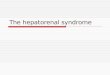
Control kidney cortex
Cirrhotic kidney cortex
A
B
Abdominal
compartment
syndrome (ACS)✓ Tense ascites,
intraabdominal
hypertension (bladder
pressure ~ > 20
mmHg)
AGN
AIN
Acute glomerulonephritis
(AGN)✓ HCV-MPGN, IgAN
Acute interstitial
nephritis (AIN)✓ Antibiotics for SBP
(e.g., quinolones)
AKICKD
✓ IgAN, GS
✓ HCV-MPGN
✓ Prior AKIs
Practical Consideration # 1: Differential diagnosis of AKI in cirrhosis is broad

Spontaneous Bacterial
Peritonitis (SBP)
%
25
50
13/27
(48%)
7/27
(27%)
9/27
(33%)
%
25
50HRS-1
83/252
(33%)
Follo A et al(Hepatology 1994)
Hampel H et alAm J Gastro 2001)
Watt K et al(Am J Gastro 2002)
%
25
50 10/23
(43%)
4/23
(17%)
252 SBPs
n = 197
Fernandez J et al(Gastroenterology 2007)
n = 68 n = 23 n = 27
SBP prophylaxis prevents HRS
Practical Consideration # 2
HRS-1 should be suspected in the context of the
presence of a precipitating factor

2015 ICA
HRS-1 Criteria
Angeli P et al(Gut 2015)
Wong F & Angeli P(J Hepatology 2016)
CVP ≥ 8 mmHg?
IVC diameter?
Practical Consideration # 3
First step should involve
determining if the patient may
respond to intravenous volume
expansion

Velez et al, Am J Nephrol 2019

• Sarcopenia
• High bilirubin interference with Cr
colorimetric assay – artifact
• Daily change in serum Cr is still
useful and valid Control
Cirrhosis
Ebadi M et al(J Gastroenterol 2019)
Practical Consideration # 4:
Absolute serum creatinine (Cr) values
could be misleadingly lower than expected
by degree of AKI

Practical Consideration # 5:
FENa < 1% to diagnose HRSFENa according to
biopsy-proven diagnosis
Alsaad & Wadei et al(World J Hepatol 2016)
n = 88
FENa < 1% and/or Urine Na < 20 mEq/L
is always present but not diagnostic

antibiotics?
10-50 RBCs/hpf?
Foley?
chronic IgA GN?
pyuria?
Angeli P et al(Gut 2015)
Wong F & Angeli P(J Hepatology 2016)
Granular casts, RTECs, WBCs?
UNa < 20 mEq/L ?
IAP < 25 mmHg ?
Low BP “normal” for cirrhotics? What if MAP 90?
Practical Consideration # 6
Some essential aspects of the HRS-1
phenotype are not included in the
ICA criteria
Hyponatremia? Oliguria?
2015 ICA
HRS-1 Criteria

For liver transplant ineligible patients, why should we treat HRS-1?
Boyer T et al. Terlipressin Study Group
(Liver Transplantation 2011)
3-month transplant-free survival
Responders
41% (7/17)
Non-responders
4% (2/47)
Transplanted: 97% (34/35)n = 99
Practical Consideration # 7
Even if a patient is not eligible
for liver transplantation, there
is potential benefit in treating
HRS-1

Velez JC & Nietert PJ(Am K Kidney Dis 2011)
Vasoconstrictor Therapy in HRS-1:Raising the Mean Arterial Pressure (MAP)
The main goal of treatment of
HRS-1 with vasoconstrictor
therapy is to raise the MAP
by 15 mmHg or to a target
MAP ~ 85 – 90 mmHg
Practical Consideration # 8

Vasoconstrictor Therapy in HRS-1
Norepinephrine vs. Terlipressin
% H
RS
Revers
al
43 % 39 %
25
50
75
100
40
50
60
70
80
90
100
0 d15
Mean ∆ MAP(mmHg)
Singh et al.(J Hepatol 2012)
n = 46
% H
RS
Revers
al
50 % 50 %
25
50
75
100
Sharma et al.(Am J Gastroenterol 2008)
n = 40
40
50
60
70
80
90
100
0 4d 8d
Mean ∆ MAP(mmHg)

Vasoconstrictor Therapy in HRS-1:Terlipressin (CONFIRM Trial)
https://clinicaltrials.gov/ct2/show/NCT02770716?term=CONFIRM&cond=Hepatorenal+Syndrome&rank=1
https://www.biospace.com/article/releases/mallinckrodt-announces-positive-top-line-results-from-its-pivotal-phase-3-confirm-trial-of-terlipressin-in-patients-with-hepatorenal-syndrome-type-1-hrs-1-/

40
50
60
70
80
90
100
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37m
mH
g
Baseline MAP at the time of HRS diagnosis
37 cohorts
Mean: 74.6 mmHg
Median: 76 mmHg
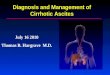
Vasoconstrictor Therapy in HRS-1:Meta-Analysis of 21 Clinical Studies
The MAP at baseline in HRS-1
isn’t necessarily very low,
certainly not less than 65
mmHg. Some patients may
have a MAP up to 80 mmHg
and still benefit from further
rise in MAP
Practical Consideration # 9
Velez JC & Nietert PJ(Am K Kidney Dis 2011)

Vasoconstrictor Therapy in HRS-1: Raising the MAP
Stadlbauer V et al(Gastroenterology 1999)
Persson P et al(Am J Physiol 1999)
Kelleher S et al(Am J Physiol 1984)

Midodrine / Octreotide is
largely ineffective raising MAP
and revering AKI in HRS-1
Practical Consideration # 10
Velez JC et al(Nephron 2015)

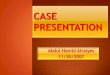
Acute Kidney Injury during Acute Liver Failure due to Acetaminophen Toxicity is NOT a form of HRS-1
Toxic Acute Tubular Injury
Cultured Proximal Tubular Epithelial Cells: Pyknotic Nuclei
Lorz C et al(JASN 2004)
BONUS: Practical Consideration # 11

4.4 4.1 4.3
1 2 3day
sCr
(mg/dL)3.8
4
4.2 3.93.6
3.12.6
2.4
5 6 7 8 9 10
Biliary tube exchange / IVF (NS)
80MAP
(mmHg)
45 39 36T Bili
(mg/dL)
OLT
1.8
4.2
20
❖ Primary Sclerosing
Cholangitis - ESLD
❖ Baseline sCr 1.1
RFA: worsening jaundice
✓ BP 121/66 mmHg
✓ sNa 138; uNa 22
Case Example 01
70 yo man

4.95.9
7.0
1 2 3day
sCr
(mg/dL)
6.7
4
6.8 – 7.2
5.6
5 6 7 8 9 10
MAP
(mmHg)
3.5
T Bili
(mg/dL)27
❖ Alcoholic, Fatty - ESLD
❖ Baseline sCr 1.0
RFA: ACLF, ETOH intoxication
✓ BP 135/64 mmHg, MAP 88
✓ sNa 132; uNa < 20
Case Example 02
27 yo man
87
LVEF 35%
Leukocytosis37

3.3
4.15.0
1 2 3day
sCr
(mg/dL)
4.5
4
4.8 4.4 3.93.5
3.22.9
5 6 7 8 9 10
IV norepinephrine
7368
8488 8687 88
70
87MAP
(mmHg)
RHC: PAP 55 PCWP 21
IV furosemide
UOP
1 L/d
❖ HCV - ESLD
❖ Baseline sCr 1.3
❖ Pulmonary HTN
RFA: worsening ascites,
evaluation for HCC
✓ BP 92/53 mmHg, MAP 63
✓ sNa 134; uNa < 20
Case Example 03
IV albumin
Midodrine / Octreotide
61 yo man
T Bili
(mg/dL)3.8

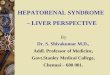
❖ ETOH - ESLD
❖ Baseline sCr 1.0
❖ Recently hospitalized
with “sepsis, abdominal
pain, transaminitis”
RFA: elevated serum Cr
✓ BP 92/51 mmHg
✓ sNa 129; uNa 39
✓ Urine leukocytes
Case Example 04
59 yo woman
1.0
4.0
1 2 3day
sCr
(mg/dL)
4
4.3 4.7 4.63.8
2.0
2.9
5 6 7 8 9 10
Clinic lab check,
admitted
Started midodrine +
octreotide
7570
8480
868783
72
85MAP
(mmHg)
T Bili
(mg/dL)1.0
Discharged
from Hosp.
Kidney biopsy: AIN (exposed to Cipro!)
4.3
1.3
Steroids began

AKI stage 1
Initiate Vasoconstrictor Therapy + IV Albumin
Midodrine PO / Octreotide SQ
Not HRS-1 (ATN, AIN, AGN, OU)
Target MAP rise 15 mmHg
or MAP 85 mmHg
Possible HRS-1
AKI stage ≥ 2
Approach to Management of Hepatorenal AKI
>50 RBCs, dysm RBC
>10 WBCs
Cell casts, MBGCs
UPCR >>1.0
UNa > 30
Shock, ↓↓BP, hydronephros
DO NOT Initiate
Vasoconstrictor Therapy for HRS-1
Treat 3-7 days, switch/continue
Midodrine PO / Octreotide SQ
History, physical, IVCd: volume expansion 0 - 3 days: IV albumin
(-) RBCs
(-) WBCs
(-) Prot
UNa < 10
Definite HRS-1
No ResponseNorepinephrine IV or Terlipressin IV
sCr stable or
Volume-unresponsive Hepatorenal AKI
sCr
Target MAP rise 15 mmHg
Repeat if
Recurrence
Response
No Response in 2-3 days
STOP
↑↓ sCr course
urine findings +/-
drug confounders
Abnl RUS or ECHOC
Improbable HRS-1 Probable HRS-1
MAP<80, sNa<135,
oliguria
SpectrumMAP<80, sNa<135, oliguria

Summary
1. Differential diagnosis of AKI in cirrhosis is broad, do not rush to label it HRS
2. If SBP is present, suspicion for HRS increases
3. If history & physical supports it, volume expansion with IV albumin is OK, but watch for volume overload
4. Serum Cr underestimates degree of AKI in cirrhosis, but ∆daily still valid
5. If FENa >1% and/or UNa > 20 mEq/L, think not HRS
6. The ICA HRS criteria are far from perfect, attention to detail is needed
7. In the absence of OLT, successful HRS reversal may improve survival
8. The cornerstone of HRS treatment is pursuance of a rise in MAP by ~15 mmHg or to a goal ≥ 85 mmHg
9. Baseline MAP in HRS could be “normal” (e.g., ~ 70 - 75 mmHg)
10. Midodrine / octreotide is largely ineffective in HRS-1
@VelezNephHepato