Embed Size (px)
Citation preview

MEDICINE
Acute Life-Threatening Complications of Portal Hypertension:a Review of Pathophysiology, Incidence, Management, and Cost
Robert E. Smith1& Alice D. Friedman2
& James A. Murchison1& S. Blake Tanner3 & P. Alexander Smith4
&
Bradley T. Dollar1
Accepted: 28 July 2020# Springer Nature Switzerland AG 2020
AbstractPortal hypertension represents a dysfunctional hemodynamic alteration within the portal venous system, usually due to cirrhosis.These altered hemodynamics play a direct role in the development of acute, life-threatening variceal hemorrhage and mark animportant pathophysiologic step in the development of other sudden and life-threatening complications such as type 1hepatorenal syndrome and spontaneous bacterial peritonitis. Many life-saving interventions in these patients are aimed atreducing portal venous pressure. The contribution of portal hypertension to the development of variceal hemorrhage, type 1hepatorenal syndrome (known also by the name HRS-AKI), and spontaneous bacterial peritonitis in cirrhotic patients isdiscussed. This article reviews the pathophysiology and incidence of life-threatening complications of cirrhotic portal hyperten-sion, with a discussion of management options and treatment costs.
Keywords Portal hypertension . Variceal bleeding . Hepatorenal syndrome . Spontaneous bacterial peritonitis . Hemodynamics .
Cirrhosis
Introduction
Portal hypertension is common, particularly among cirrhoticpatients, and its presentation may be both sudden and fatal. Aclinical understanding of portal hypertension helps physicianstreat and manage these patients, and knowledge of the under-lying diseased hemodynamics enables the development ofnew therapies. The burden of portal hypertension, both eco-nomically and in terms of impact on patient lives and those oftheir families, emphasizes the gravity of portal hypertensivedisease and the urgency to address it.
Cirrhotic Portal Hypertension: Epidemiology andSocioeconomic Factors
Cirrhosis accounts for approximately 90% of portal hyperten-sion cases in the Western world [1, 2]. The estimated preva-lence of cirrhosis in the USA is 0.27% (greater than 600,000)adults, and there is a preponderance of cirrhosis among pa-tients living below the poverty level and those who have notfinished the 12th grade [3]. The annual international death tollfor complications of cirrhosis is estimated at 1 millionpatients.
This article is part of the Topical Collection on Medicine
* Robert E. [email protected]
Alice D. [email protected]
James A. [email protected]
S. Blake [email protected]
P. Alexander [email protected]
Bradley T. [email protected]
1 Department of Radiology, Baylor Scott & White MedicalCenter—Temple, 2401 S. 31st St., Temple, TX 76508, USA
2 Division of Gastroenterology, Austin Diagnostic Clinic, 12221MoPac Expressway North, Austin, TX 78758, USA
3 Department of Nephrology, Baylor Scott & White MedicalCenter—Temple, 2401 S. 31st St., Temple, TX 76508, USA
4 TMC Innovation Institute, Texas Medical Center, 2450 HolcombeBlvd Ste X, Houston, TX 77021, USA
https://doi.org/10.1007/s42399-020-00435-5
/ Published online: 6 August 2020
SN Comprehensive Clinical Medicine (2020) 2:1628–1645

Although alcohol abuse and chronic viral infection havehistorically been the most common causes of cirrhosis, globalrise in obesity has led to the emergence of nonalcoholic fattyliver disease as an important cause not just of cirrhosis but ofportal hypertension as well [4]. The prevalence of portal hy-pertension among obese patients is greater than 25% accord-ing to a study by Mendes et al. Although the authors found alink between degree of nonalcoholic liver fibrosis/cirrhosisand portal hypertension, 12% of patients with indirect signsof portal hypertension had little to no fibrosis on liver biopsy[5]. Alarmingly, the global prevalence of nonalcoholic fattyliver disease is estimated at over 25% [4].
Acute, life-threatening illness directly related to portal hy-pertension among cirrhotic patients is extremely common. Astudy of the United States Healthcare Cost and UtilizationProject Nationwide Emergency Department Sample by Pantet al. looked at the frequency with which these complicationsare encountered in US emergency departments. Of an estimat-ed 131 million emergency visits in 2011, approximately 5.3%,4.4%, and 3.9% were related to variceal bleeding, hepatorenalsyndrome, and spontaneous bacterial peritonitis, respectively.This study also confirmed an inordinate number (31.8%) ofthese patients were in the bottom income quartile, suggestingthat these acute complications disproportionately affect pa-tients of a lower socioeconomic status [6].
Pathophysiology of Portal Hypertension
The portal venous system drains blood from the spleen andgastrointestinal organs into the liver where nutrients andtoxins undergo first-pass metabolism before entering the
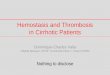
systemic circulation (Fig. 1). Portal hypertension is character-ized by elevated pressures within the portal venous system, apathologic state resulting from a variety of interrelated pro-cesses. The pathophysiology of portal hypertension can bebroadly characterized by two mechanisms: outflow from theportal venous system is obstructed or inflow into the portalvenous system is increased.
Liver cirrhosis, by far the prevailing cause of portal hyper-tension in the Western world, manifests with fibrosis that ob-structs portal venous outflow through the hepatic sinusoids.This and other less common causes of portal hypertension aredepicted in Fig. 1 [1, 7–12]. Increased inflow into the portalvenous system is a distinct pathologic mechanism which oc-curs as a secondary effect in cirrhotic patients with pre-existing portal hypertension. In these patients, altered splanch-nic and systemic arterial tone unfortunately maintains andexacerbates elevated portal venous pressures [13]. Elevatedcirculating blood plasma volume in these patients may alsoplay a role [14].
The altered fluid dynamics in portal hypertension are thedirect cause of clinical syndromes such as portal hypertensivegastropathy and ascites and are a contributing cause to othersincluding cardiomyopathy, hepatopulmonary syndrome, andhepatic encephalopathy [1]. Among the direct manifestationsof portal hypertension, acute variceal bleeding and type 1hepatorenal syndrome are two disease processes which man-ifest acutely and are associated with high short-term mortality.Ascites can complicate acute liver failure, refractory fluid inthe abdomen worsens renal hypoperfusion (hepatorenal syn-drome), and the fluid itself becomes a nidus for infection bytranslocated gut bacteria leading to spontaneous bacterial
Fig. 1 Etiologies of portalhypertension. Cirrhosis is by farthe leading cause of portalhypertension in the Westernworld and results in intrahepaticsinusoidal obstruction (hepaticsinusoid depicted inmagnification). *Schistosomiasisis a major cause of portalhypertension in Africa, parts ofAsia, and the Middle East. A1995 study estimated nearly 200million people were infected bythe Schistosoma parasite, most ofthem on the African continent [7,8]. **Portal vein thrombosis is animportant cause of portalhypertension in the pediatricpopulation but remains rare, withan estimated incidence of 1 permillion [9, 10]
1629SN Compr. Clin. Med. (2020) 2:1628–1645

peritonitis [15]. These infections are a third sudden and deadlyconsequence of portal hypertension [16].
Altered Hemodynamics of PortalHypertension
Portal Hemodynamics: Clinical Measurements
The location of the portal venous system deep within the ab-domen makes direct measurement of portal venous pressureimpractical. A clinical substitute in most patients is the hepaticvenous pressure gradient (HVPG). A hepatic vein is cannu-lated and a free hepatic venous pressure (FHVP) is obtained.The vein is then occluded and a hydrostatic pressure is obtain-ed, termed the wedge hepatic venous pressure (WHVP); thisserves as an estimate of the upstream portal venous pressure.The difference between the WHVP and FHVP is the HVPG.Normal HVPG lies between 1 and 5 mmHg [17]. An elevatedHVPG suggests increased resistance within the liver sinu-soids. In cirrhotic patients, HVPG is predictive of portal ve-nous velocity and flow volumes (although the same may notbe true for other less common causes of portal hypertension)[18–21].
Velocity in the main portal vein can be measured noninva-sively by ultrasound orMRI and is normally 25–40 cm/s, withvelocity < 16 cm/s associated with portal hypertension[22–24]. Unfortunately, there is significant inter- and intra-observer variability in Doppler ultrasound measurement[25–27]. MRI measurements are more consistent but correlatepoorly with Doppler ultrasound [28–30]. As discussed below,there is a downward trend in portal venous velocity and flowvolume as cirrhosis progresses. However, these measurementsare highly variable and values overlap between healthy anddisease states, precluding the use of portal venous velocity andflow volume as a diagnostic tool.
Portal Hemodynamics: Pathologic Changes
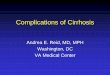
Figure 2 summarizes the primary physiologic causes whichconverge to bring about portal hypertension. The emergenceof variceal hemorrhage, type 1 hepatorenal syndrome, andspontaneous bacterial peritonitis are also included in this chart.
Portal venous flow is dynamic and will differ based uponfasting state, phase of respiration, and whether the patient isupright or supine [31, 32]. While portal venous flows betweenhealthy and early-stage cirrhotic patients may remain similar,portal flow decreases with increasing disease severity [21,33–35]. However, an unpredictable physiologic response toportal hypertension in cirrhotic patients leads to significantvariability in portal venous flow. One factor contributing tothis observation is substantial variation in the location anddevelopment of portosystemic collateral vessels [28, 36].
Flow through the portal vein may become increasingly pulsa-tile, oscillating, or even reversed (hepatofugal) as cirrhosisprogresses. This phenomenon is partly due to increasingintrahepatic resistance to hepatic arterial flow, leading toarterioportal shunting in the hepatic sinusoids and resultingarterial flow through the portal vein in a retrograde fashion.This blood then drains via collateral vessels into the systemiccirculation [22, 37]. Endogenous vasodilators such as nitricoxide are not only released within the splanchnic vasculaturein response to portal hypertension but also have a systemiceffect and can result in systemic hypotension and ahyperdynamic state which may ultimately increase portal ve-nous blood flow, particularly in patients with severe cirrhosis[28, 38]. Ironically, endothelial dysfunction within the hepaticparenchyma leads to impaired local release of vasodilators andincreased intrahepatic vascular tone. This is estimated to ac-count for over 30% of the increased intrahepatic resistanceseen in cirrhotic patients [39, 40].
As resistance increases through the liver, there is a precar-ious balance between forward and reversed flow, with factorssuch as intra-thoracic/intra-abdominal pressures during respi-ration or Valsalva, or splanchnic vasodilation in the postpran-dial state leading to temporary changes in flow direction.Further increases in intrahepatic resistance may result in amore steady-state flow reversal in the main portal vein [41].Oscillating or reversed flow in the portal vein is a findingassociated with increased severity of cirrhosis and is an inde-pendent predictor of poor outcomes [42], but this is a feature,rather than a defining criteria, of disease severity and hasvariable incidence even in patients with mild disease (Child–Pugh class A) [42–44]. The incidence of flow reversal in themain portal vein or its tributaries the splenic vein or superiormesenteric vein has been reported at 2.7% in Child–Pughclass A, 12.5% in class B, and 15% in class C [44]. As withflow volumes, a similar pattern of diminishing flow velocity inthe main portal vein is observed with worsening cirrhosis [21,33–35]. Additionally, a 1996 histologic study of 47 patientsfound a correlation between main portal venous flow velocityand degree of liver fibrosis, but no such correlation was iden-tified between degree of fibrosis and portal venous flow vol-umes [45]. In summary, there is a weak inverse relationshipbetween portal venous flow and severity of liver cirrhosis,with significant variability in each patient’s physiology.
The results of several studies of normal portal flow areincluded below in Table 1. Because the studies by Stankovicand Sugano used small populations which compared healthypatients to cirrhotic patients with early-stage disease, it is dif-ficult to observe the inverse relationship between disease se-verity and portal venous flow [30, 31]. Other studies betterdisplay this relationship (Table 2). In reference to Table 2, theinvestigators describe similar measurement methods forobtaining their measurements, and all patients were keptfasting overnight prior to the exam. Taourel et al. subtracted
1630 SN Compr. Clin. Med. (2020) 2:1628–1645

flow from a patent umbilical vein, if present, which may ac-count for the lower reported flow values particularly in moreadvanced cirrhosis. In addition, Taourel et al. included onlypatients with alcoholic cirrhosis, and a large portion of these
patients (22%) had flow reversal in the main portal vein [21].Indeed, a higher incidence of portal flow reversal has beenreported in cirrhosis secondary to alcohol [48]. Despite slightdifferences in the patient populations chosen for each study
Table 1 Physiologic variability in portal venous flow healthy patients
Investigator Healthy patients Cirrhotic patients(if included)
Modality Population size
Brown et al. [32] 864 ± 188 mL/min N/A Ultrasound 45
Stankovic et al. [30] 640 ± 190 mL/min 790 ± 320 mL/min MRI 40
820 ± 340 mL/min 1020 ± 540 mL/min Ultrasound
Sugano et al. [31] 1300 ± 200 1000 ± 100 MRI 29
Lycklama a Nijeholt et al. [46] 1200 mL/min (960–1600) N/A MRI 8
Yzet et al. [41] 1239 ± 223 mL/min N/A MRI 9
1595 ± 521 mL/min N/A Ultrasound
Fig. 2 Pathophysiology ofcirrhotic portal hypertension andits sudden life-threatening com-plications (variceal hemorrhage,type 1 hepatorenal syndrome, andspontaneous bacterial peritonitis)
1631SN Compr. Clin. Med. (2020) 2:1628–1645

listed in Table 2, such variability in the recorded portal venousflows among the control groups suggests a high degree ofvariability in measurement technique.
Variceal Hemorrhage: a Life-ThreateningComplication of Portal Hypertension
Pathophysiology
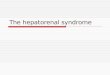
Gastroesophageal varices are the natural sequelae of elevatedportal venous pressures (Fig. 2). As portal venous pressuresrise, collateral blood vessels open to allow blood to bypass theoutflow obstruction and drain directly into the systemic ve-nous circulation. These collateral vessels, either pre-existingor the product of angiogenesis in chronic liver disease [49],have a specific pattern of appearance throughout the abdo-men; however, gastroesophageal collaterals which form inthe esophagus and stomach are clinically significant becausethey have the tendency to grow into dilated varices (venousdrainage of the stomach is illustrated in Fig. 3). According tothe law of Laplace, the surface tension within the vessel wall isdirectly proportional to vessel diameter. The continued dila-tion and wall thinning of gastroesophageal varices is ultimate-ly what leads to variceal rupture and acute hemorrhage [50].Coexistent infection may be the final precipitant of varicealbleeding in many of these patients due to the inflammatoryvasoactive changes and platelet dysfunction which occur sec-ondary to infection [51].
Epidemiology—Incidence and Mortality
Most bleeding in cirrhotic patients originates from esophagealvarices. Only about 10–33% of variceal bleeding arises fromgastric varices, which are associated with higher rates ofrebleeding and increased mortality [52]. While ectopic varicescan occur outside the esophagus and stomach, these are rela-tively rare and only account for 1–5% of variceal bleeds. Themost common locations are the rectum and duodenum. Themanagement of ectopic variceal hemorrhage is lessestablished [53].
Cirrhotic patients are routinely monitored for the presenceof gastroesophageal varices given the high incidence in thispopulation [54]. In cirrhotic patients who do not yet havevarices, the prevalence of esophageal varices increases up to28% by 3 years [55], with up to 44% of patients developingesophageal or gastric varices by 10 years [56]. A 2007 studyreported an overall 52.2% prevalence of varices in cirrhoticpatients undergoing screening endoscopy, which increased toa 71.9% prevalence in a subset of patients with more severe(Child–Pugh class B/C) disease [57]. The lifetime incidenceof variceal bleeding among cirrhotic patients is between 25and 40% [58]. Independent risk factors for predicting variceal Ta
ble2
Portalvenous
flow
incirrhosisas
afunctio
nof
diseaseseverity
(mL/m
in)
Investigator
Health
ycontrols
Child–P
ughclassA
Child–P
ughclassB
Child–P
ughclassC
Notes
Bao
Min-Shi
etal.[33]
1254
±410(20patients)
1358
±384(22patients)
1142
±390(8
patients)
788±234(8
patients)
Excludedpatientson
prophylacticbeta-blockers
Taoureletal.[21]
N/A
685±296(13patients)
177±369(9
patients)
140±472(18patients)
Onlyalcoholic
cirrhosisconsidered.
Perium
bilicalvein
flow
subtracted
Chawlaetal.[35]
835±187(10patients)
737±61
(11patients)
513±92
(13patients)
478±5(13patients)
Scannedduring
expiratio
n
Achim
etal.[47]
1254
±65
(20patients)
1279
±54
(14patients)
1126
±95
(21patients)
857±89
(15patients)
Excludedpatientswith
history
ofbleedor
vasoactiv
edrugs
Haagetal.[23]
810±180(100
patients)
889±414(95patients)
817±465(168
patients)
561±556(112
patients)
Patientsselected
forTIPSafter
varicealbleeding/ascites
Average
flow
volume
930mL/m
in963mL/m
in1071
mL/m
in547mL/m
inHeavily
weightedby
Haagetal.
1632 SN Compr. Clin. Med. (2020) 2:1628–1645

bleeding include the size of the varices and the presence of redwale markings (which are red streaks seen on the varices dur-ing endoscopy) [59].
Although mortality has improved since the 1980s and1990s with the use of primary prophylactic medications, en-doscopic ligation, and the use of antibiotics, the in-hospitalmortality rate associated with variceal hemorrhage remainsaround 15% (versus around 40% in the early 1980s) [60], witha 6-week mortality of 10–20% [61, 62] and an associated 1-year mortality greater than 25% [63]. In patients with severecirrhosis (Child–Pugh class C), in-hospital mortality remainsaround 30% [60]. Thirty-day and 1-year rebleeding rates areas high as 26% and 60%, respect ively [64, 65].Approximately 40% of rebleeding occurs within the first5 days, the time at which rebleeding risk is highest [66, 67].
Due to the prevalence of hepatic cirrhosis and the directcausal relationship between cirrhosis and portal hypertension,comparative data on noncirrhotic portal hypertension and var-iceal hemorrhage is limited. The available studies on patientswith noncirrhotic portal hypertension report a variable inci-dence of hemorrhage, but the overall mortality rate is univer-sally better in these patients. Worse outcomes in cirrhotic pa-tients are likely related to underlying hepatic dysfunction andother comorbidities in the cirrhotic population [68–72].
Management of Variceal Hemorrhage—Diagnosis
Prompt recognition of variceal hemorrhage relies on the iden-tification of hypovolemia in a patient with stigmata of
cirrhosis, including ascites, splenomegaly, jaundice, etc.Evidence of hypovolemia includes resting tachycardia, ortho-static hypotension, or shock. Hematemesis or melena may bepart of the patient history. Esophagogastric varices are con-firmed on endoscopy; these may demonstrate active bleeding/oozing, but an overlying clot or the “white nipple sign”(representing a fibrin plug) are indications of recent bleeding[73, 74].
Management of Variceal Hemorrhage—Prophylaxis
Previous recommendations for prophylaxis in cirrhotic patientswere aimed at preventing the formation of varices (“pre-prima-ry prophylaxis”); however, beta-blockers were shown to be ofno benefit in this regard [75] and current prophylactic measuresaim to reduce the incidence of bleeding in varices that havealready developed. For patients with large varices, advancedcirrhosis, or red wale markings on endoscopy, beta-blockersor endoscopic variceal ligation are indicated to reduce bleedingrisk [76]. Endoscopic variceal ligation requires continued en-doscopic surveillance to identify the formation of new varicesbut is an option for patients who cannot tolerate the systemichemodynamic effect of beta-blockers. Beta-blockers reducecardiac output, which in turn lowers portal venous inflow.Nonspecific beta-blockers, such as carvedilol, also have alphaadrenergic antagonism that constricts the splanchnic vessels(reducing portal venous volumes) and produces vasodilationwithin the hepatic arterial bed (lowering intrahepatic resistance)[76]. Antibiotics are used in the setting of acute variceal
Fig. 3 Venous drainage of thestomach. Varices commonly format the lower esophagus,gastroesophageal junction, oraway from the esophagus alongthe gastric curvatures. GEV(gastroepiploic vein), LGV (leftgastric vein or coronary vein), PV(main portal vein), RGV (rightgastric vein), SGV (short gastricveins), SMV (superior mesentericvein), SV (splenic vein)
1633SN Compr. Clin. Med. (2020) 2:1628–1645

hemorrhage to prevent short-term rebleeding, but antibiotics arenot typically prescribed in the long-term outpatient setting toprevent variceal hemorrhage. However, there is a subset ofpatients with severe cirrhosis and portal hypertension(discussed further with hepatorenal syndrome and spontaneousbacterial peritonitis) for whom long-term outpatient prophylax-is is indicated [77]. For patients with noncirrhotic portal hyper-tension, evidence is scarce and prophylactic recommendationsvary by etiology [78].
Management of Variceal Hemorrhage—AcuteMedical Therapy
During an episode of variceal hemorrhage, acute managementhas these goals: hemostasis, prevention of early rebleedingduring the following 5-day high-risk window, averting/treating complications of variceal hemorrhage, and preservingliver function [79, 80]. Six-week mortality is considered aprimary endpoint [76]. Direct complications of gastrointesti-nal bleeding include shock, encephalopathy, aspiration, andspontaneous bacterial peritonitis [81].
Acute variceal hemorrhage requires ICU level care.Conservative blood transfusion strategies are employed, asmore aggressive volume resuscitation has been associatedwith greater rebleeding and mortality, which may be linkedin part to elevated HVPG following transfusion [82].Antibiotic prophylaxis (commonly fluoroquinolones or ceph-alosporins) for patients admitted with variceal hemorrhage isassociated with decreased all-cause mortality and bacterialinfection in these patients [83]. Other strategies target specificpathophysiologic mechanisms of portal hypertension.Vasoactive drugs such as somatostatin, vasopressin, and theiranalogues (octreotide is most widely used in the USA) aregiven to reduce splanchnic vasodilation (and therefore limitportal venous inflow) [84].
Management of Variceal Hemorrhage—AcuteInterventional Therapy
Interventional therapies are extremely important in the man-agement of variceal bleeding. Endoscopic variceal ligationcan be performed emergently and involves placing rubberbands around dilated varices to prevent or control bleeding.As a temporizing measure in patients whose esophageal var-ices continue to bleed, a tamponade can be achieved endo-scopically with balloons (colloquially referred to asBlakemore tubes) or covered stents [85]. For bleeding gastricvarices, initial endoscopic intervention may involve endo-scopic variceal ligation or direct injection of cyanoacrylateglue into the varix [76], although this second technique isnot widely available in the USA.
During an acute bleed, an HVPG > 20 mmHg is highlypredictive of inability to control bleeding. If HVPG can be
lowered to below 12 mmHg or by > 20% of the patient’sbaseline, the risk of rebleeding drops significantly [86, 87].Additionally, during an acute bleeding episode, a HVPG of >20 mmHg is highly associated with failure to control bleedingand may indicate the need for rescue therapies such astransjugular intrahepatic portosystemic shunt (TIPS),discussed below [86]. HVPG measurement is not always im-mediately available, but in cirrhotic patients, disease severitycorrelates strongly with HVPG, and over 80% of Child–Pughclass C patients have an HVPG of > 20 mmHg [88].
Interventional radiologists are frequently consulted forassistance with emergent variceal bleeding. In the case ofbleeding gastric varices for which endoscopic variceal li-gation and cyanoacrylate injection are unavailable or un-successful, gastric varices may be eradicated by obtainingvascular access into a gastrorenal collateral vessel via theleft renal vein followed by direct occlusion of the venousoutflow of the gastric varices. The name of this proceduredepends on the occlusive material chosen. If an occlusiveballoon is used, the procedure is known as a balloon ret-rograde transvenous obliteration (BRTO). If coils or plugsare employed, the procedure is referred to as a CRTO orPRTO, respectively. This predictably re-routes blood flowinto the portal venous system and may transiently im-prove hepatic blood flow and liver function, but at thecost of increasing portal hypertension and worseningesophageal varices [89].
Another procedure performed emergently by the interven-tional radiologist is the transjugular intrahepatic portosystemicshunt (TIPS), an artificial collateral vessel between a hepaticvein and a branch of the portal vein, which rapidly relievesportal venous pressures. Well-established indications for TIPSinclude prevention of rebleeding in high-risk patients duringinitial presentation for variceal hemorrhage, refractory bleed-ing not amenable to first-line therapies, hepatorenal syndrome,refractory ascites, and other situations on a case-by-case basis(including gastric variceal bleeding not amenable to endo-scopic therapy or BRTO) [76, 90, 91]. Recurrent portal hyper-tension following TIPS is usually due to stent stenosis, throm-bosis, or kinking, though long-term patency rates are as highas 76% at 2 years fol lowing implementat ion ofpolytetrafluoroethylene (PTFE)-covered stents [92, 93].
The HVPG is a useful tool in predicting variceal bleedingand is often obtained during a TIPS procedure. Varices beginto form once the HVPG reaches 10 mmHg, with bleedingoccurring at 12 mmHg. Patients who respond to early man-agement strategies with a reduction in HVPG below12 mmHg or > 20% of their baseline have been shown to beat lower risk of primary bleeding, and a decrease in HVPG by> 20% improves mortality [86, 87, 94].
Surgical portosystemic shunts, largely replaced by theTIPS procedure, are also an emergent or prophylactic optionand may have improved long-term outcomes in those patients
1634 SN Compr. Clin. Med. (2020) 2:1628–1645

with preserved liver function and an otherwise good prognosis[95]. A surgical connection between the left portal vein andsuperior mesenteric vein (a “meso-Rex” shunt) may beemployed to bypass an obstructedmain portal vein and relieveelevated portal pressures, but this is of little clinical utility ifcirrhosis has developed [96].
Though relatively rare, when bleeding occurs from an ec-topic varix (1–5% of bleeds), the general management strate-gy of fluid resuscitation, antibiotic prophylaxis, upper endos-copy, and radiologic intervention is similar but may requireadaptation on a case-by-case basis [53].
Primary therapies for portal hypertension are summarizedin Table 3.
Associated Cost
A 2000 study of acute variceal bleeding among USVA patientsreported an average total cost of greater than $16,000 to treat asingle episode of variceal bleeding [97]. A 2007 report fromFrance documented an average hospital cost of euro 11,000–14,000 (approximately $14,000 to $20,000 in USD in 2007) totreat an episode of variceal bleeding, with costs rising over euro29,000 (approximately $43,000 in USD in 2007) if initial in-terventions were unsuccessful [98]. According to a 2008 study,the average hospital cost of variceal hemorrhage in the USA isover $6600 and skyrockets to over $23,000 if complicationsdevelop (usually rebleeding). The same study reported an av-erage hospital stay of 3.8 days which increased to 15.2 days inthe setting of complications [99].
Hepatorenal Syndrome: a Life-ThreateningComplication of Portal Hypertension
Pathophysiology
Hepatorenal syndrome is defined as reversible diminished re-nal function, usually in the setting of cirrhotic portal hyperten-sion [12]. It may also be observed in the setting of severe liverdysfunction, acute hepatitis [1], hepatic veno-occlusive dis-ease, or Budd–Chiari syndrome [100, 101].
The same vasodilators which engorge the splanchnic vas-culature in the setting of portal hypertension lead to systemichypotension. The effect is multifactorial but involves redistri-bution of the intravascular volume into the engorged splanch-nic vasculature as well as vasodilatory effects on the systemicarterial system [38, 102]. Initially, cardiac output increases tokeep up, but over time cirrhotic cardiomyopathy develops andthere is a diminished capacity for the heart to respond to theincreasing demands placed on it, and cardiac output ultimatelyfalls [102, 103]. Compensatory activation of the renin–angiotensin system occurs and raises blood pressure at the costof diminishing renal perfusion. Diminishing renal perfusionleads to retention of sodium and free water, resulting in anexpanded extracellular fluid volume (Fig. 2). Due to portalhypertension and elevated pressures in the splanchnic capil-laries, this extracellular fluid transudes into the peritoneal cav-ity and accumulates as ascites [104].
Hepatorenal syndrome can be divided into two subtypes.Type 1 is a fulminant form classically characterized by
Table 3 Mechanism of action of portal hypertensive therapies
Therapy Mechanism of action
Nonselective beta-blockers [76] Beta-1 blockade: Reduce cardiac output and portal venous inflow, lowering portal venous pressureBeta-2 blockade: Leads to unopposed alpha adrenergic effect, resulting in splanchnic
vasoconstriction, lowering portal venous pressure*In patients with spontaneous bacterial peritonitis, nonselective beta-blockers can lead to
hemodynamic compromise and increase risk of hepatorenal syndrome
Restrictive blood transfusion Excessive transfusion in the setting of acute variceal bleeding increases HVPG andmay worsen outcomes
Vasoconstrictors Counteracts pathologic splanchnic dilation, lowering portal venous volumes, whileredirecting blood volume back into the systemic circulation. Improves mean arterialpressure and renal perfusion in hepatorenal syndrome
Endoscopic ligation or sclerosant injection Endoscopic therapy may be used prophylactically or in the setting of acute bleeding todirectly occlude varices. There is no effect on portal hypertension, so prophylacticendoscopic therapy requires ongoing surveillance for variceal recurrence
BRTO Direct occlusion of gastric varices. Stops bleeding but worsens portal hypertension
TIPS Artificial portosystemic shunt to rapidly lower portal venous pressures. Hepatic perfusiondecreases which may precipitate worsened liver function and hepatic encephalopathy
Balloon tamponade Direct pressure applied to bleeding esophageal varices. Temporizing measure with riskof aspiration, esophageal rupture
Diuretics Reduce salt and fluid retention, which effectively lowers portal venous pressures and improves ascites*Diuretics can acutely lower circulating arterial volumes and result in low blood pressures
and worsened renal function
1635SN Compr. Clin. Med. (2020) 2:1628–1645

doubling serum creatinine to > 2.5 mg/dL or a 50% reductionin creatinine clearance to below 20 mL/min in under 2 weeks,although newer recommendations published by theInternational Ascites Club and other groups omit these strictcutoffs in favor of a more dynamic evaluation of acute renalfailure [105, 106]. Type 1 hepatorenal syndrome is usuallytriggered by a specific, inciting event including infection,paracentesis, or gastrointestinal bleeding [106] that mightcause a rapid drop in systemic blood pressure. Type 2 is amore chronic decline in renal function without an incitingevent and is associated with the development of chronic asci-tes. As understanding of these entities increases, there havebeen recent recommendations to change the names of type 1and type 2 hepatorenal syndrome toHRS-AKI and HRS-CKDto reflect the acute and chronic nature of these entities, respec-tively. However, for this discussion the familiar terms type 1and type 2 will be employed [105].
Epidemiology—Incidence and Mortality
Prior to the International Ascites Club’s published definitionof type 1 and 2 hepatorenal syndrome in 1996, a study ofcirrhotic patients with chronic ascites reported an incidenceof hepatorenal syndrome of 18% at 1 year and 39% at 5 years[107], with median survival of < 2 weeks. Even after theIAC’s publication of diagnostic criteria, classification remainschallenging, and the exact cause of renal failure in cirrhoticpatients may be multifactorial and not always determined con-fidently [105, 108, 109]. Despite the exact definition, type 1hepatorenal syndrome carries a dismal prognosis.
Among inpatients admitted for infection: In a 2005 study of106 cirrhotic patients who developed sepsis, 27% went on todevelop renal failure. Of those with renal failure, 24% metcriteria for hepatorenal syndrome type 1, all of whom diedwithin 3 months [110]. This study excluded spontaneous bac-terial peritonitis as a cause of sepsis. In a 2006 study whichincluded spontaneous bacterial peritonitis among other causesof infection, of 104 patients with cirrhosis and ascites, 35(33.6%) developed renal failure as a complication of theirinfection, and of that group 15 (42.8%) met the criteria forhepatorenal syndrome type 1, all of whom expired [111].
Among patients admitted for renal failure: A study of 562patients admitted with cirrhosis and renal failure recognizedtype 1 hepatorenal syndrome as the causative factor in 38 ofthose patients (6.7%) [108]. A separate study of 253 patientswith cirrhosis admitted for renal failure attributed the renalfailure to type 1 hepatorenal syndrome type 1 in 30% of thosepatients, with a 3-month survival of 19.7% [109].
In outpatients: In a longitudinal study of 263 patients withcirrhosis and ascites followed for an average of 41 months, 7went on to develop type 1 hepatorenal syndrome, with a meansurvival of 1 week [112]. In patients with compensated cirrho-sis, it is estimated that greater than 50% will have developed
ascites within 10 years [113], placing them at greater risk fordeveloping fulminant renal failure.
Management of Hepatorenal Syndrome Type1—Diagnosis
The identification of type 1 hepatorenal syndrome requires ahigh index of suspicion in patients with stigmata of cirrhosisand evidence of rapidly developing hemodynamic instability.Bounding pulses, decreased mean arterial pressure, and tachy-cardia are example signs of circulatory system compromisewhich occurs in the setting of type 1 hepatorenal syndrome.Acute oliguria is often part of the clinical history. Supportivelaboratory findings include elevated plasma renin, increasedblood urea nitrogen, diminished serum osmolality and elevat-ed urinary osmolality, and electrolyte disturbances [102].
The traditional diagnosis of type 1 hepatorenal syndrome isdefined as a doubling serum creatinine to > 2.5 mg/dL or a50% reduction in creatinine clearance to below 20 mL/min inunder 2 weeks. However, as mentioned previously, the diag-nostic criteria of type 1 hepatorenal syndrome remains in fluxand other causes of acute renal failure should be excluded.Newer criteria published by the IAC attempt to account forconfounding causes of renal failure such as acute kidney in-jury by removing the strict 2.5 mg/dL creatinine cutoff. Inclinical practice, the diagnosis must often be presumed [102,105]. To aid in making an accurate diagnosis of hepatorenalsyndrome, other biomarkers of renal function have been in-vestigated, such as urinary neutrophil gelatinase-associatedlipocalin (NGAL). NGAL is a marker of renal injury in acutetubular necrosis which is not expected to be elevated inhepatorenal syndrome [114]. Cystatin C is an indicator ofglomerular filtration which is less influenced by factors suchas patient age and body mass than serum creatinine. CystatinC has demonstrated prognostic value in predicting the devel-opment of hepatorenal syndrome and 90-day mortality [115].
Management of Hepatorenal Syndrome Type1—Prophylaxis
A prospective study by Fernandez et al. reported that over a12-month period, patients with advanced cirrhosis and asciteswere significantly less likely to develop renal failure orhepatorenal syndrome if they were treated with norfloxacinprophylaxis; the incidence of type 1 hepatorenal syndromespecifically in control versus norfloxacin arms was 27% and17%, respectively [116]. Due to concerns about antimicrobialresistance, antibiotic prophylaxis is typically restricted to pa-tients at especially high risk of spontaneous bacterial peritoni-tis and renal failure. There is strong evidence for long-termantibiotic prophylaxis for patients with low-protein ascites (<1.5 g/dL) who also have laboratory evidence of moderate-severe cirrhosis (Child–Pugh score of at least 9 with serum
1636 SN Compr. Clin. Med. (2020) 2:1628–1645

bilirubin ≥ 3 g/dL) and/or chronic renal disease (serum creat-inine ≥ 1.2 g/dL, blood urea nitrogen ≥ 25 mg/dL, or serumsodium ≤ 130 mEq/L). In the USA where norfloxacin is nolonger available, ciprofloxacin may be substituted [77, 116].Pentoxifylline has been previously suggested as a prophylaxisfor hepatorenal syndrome, but a meta-analysis of the availablestudies determined its effect is inconclusive [117].
Management of Hepatorenal Syndrome Type1—Acute Therapy
Definitive treatment of type 1 hepatorenal syndrome is livertransplant. Type 1 hepatorenal syndrome may resolve in over75% of patients after transplantation, and of this subset there isan excellent 1-year survival of > 95% [118]. In this study,prolonged dialysis prior to transplantation was the only pre-dictor of failure of renal recovery. Unfortunately, transplantsare not always immediately available and certain patients maynot be candidates.
Without transplant, type 1 hepatorenal syndrome carries adismal prognosis. Medical therapy aims to improve renal per-fusion and provide crucial time while the patient awaits trans-plantation [119]. Diuretics should be discontinued [120]. Themainstay of pharmacologic treatment is vasoconstrictor ther-apy, which counteracts splanchnic vasodilation and redistrib-utes blood back into systemic circulation. An analysis of 21clinical studies which investigated several different vasocon-strictors found that these medications increase mean arterialpressure, which is directly associated with improved renalfunction [121].
Outside of the USA, terlipressin, a synthetic vasopressinanalog, is commonly used both to increase splanchnic vaso-constriction as well as raise systemic mean arterial pressure.Terlipressin has been shown to reduce portal venous flowvolumes and HVPG [122]. Vasoconstrictors are combinedwith albumin, a volume expander which improves circulatingsystemic blood volume and improves renal perfusion.Together, vasoconstrictor therapy and albumin improve renalfunction in 40–60% of patients with type 1 hepatorenal syn-drome [123].
Since terlipressin is unavailable in the USA, octreotide(a somatostatin analog) is often substituted as a splanchnicvasoconstrictor, and midodrine is given to increase system-ic blood pressure. This combination of octreotide,midodrine, and albumin has been shown to improve renalfunction and survival in type 1 hepatorenal syndrome[124]. However, there is evidence that terlipressin and al-bumin provide increased survival benefit over octreotide,midodrine, and albumin [125, 126].
Norepinephrine is a vasoconstrictor only available in theICU setting, but several small studies have shown that norepi-nephrine is an equally effective alternative to terlipressin andmay be associated with fewer adverse events. Norepinephrine
may also be more cost-effective [126–129]. One randomizedtrial showed up to a 40% reversal of type 1 hepatorenal syn-drome and no significant difference in mortality at 15 days inboth the terlipressin and norepinephrine treatment arms [128].In this study, only Child–Pugh score was predictive of treat-ment response. Among ICU patients, vasopressin infusion isanother option associated with improved mortality and mayprovide crucial time while the patient awaits transplant avail-ability [130].
Renal replacement therapy (including hemodialysis) isan option when vasoconstrictors are ineffective, but thisis an inadequate long-term solution; one study identifiedan 84% 6-month mortali ty among patients whounderwent renal replacement therapy but were not listedfor liver transplantation [131].
In patients who do not respond to medical therapy,TIPS may be an option to relieve portal hypertensionand redistribute portal venous volume back into the sys-temic circulation. TIPS was shown by Brensing et al. toimprove renal function within 2 weeks and provide a sur-vival benefit when patients are not candidates for livertransplant, although 1-year survival remains low, around20% (of note, this study was performed prior to routineuse of covered TIPS stents, which improves their long-term patency) [132]. However, there are numerous contra-indications to TIPS. Because of the increased portal ve-nous shunting following TIPS, the hepatic artery mustassume a greater role in liver perfusion. If arterial perfu-sion through the hepatic artery is insufficient, liver failurecan precipitate. Increased venous return to the heart mayalso precipitate or exacerbate heart failure. Sepsis, a com-mon precipitant of type 1 hepatorenal syndrome, is anoth-er contraindication to the TIPS procedure [133].
Associated Cost
A 2017 study comparing commercially insured andMedicare patients admitted to the hospital with a diagno-sis of hepatorenal syndrome revealed average 90-daycosts of over $157,000 and $48,000, respectively, withimproved mortality and greater rates of dialysis and liveror kidney transplant among the commercially insured pa-tients. Most of the cost was incurred in the inpatient set-ting. Average hospital stays were 12.3 and 10.8 daysamong commercially insured and Medicare patients re-spectively. The authors estimated a total annual cost of$3.0–3.8 billion annually due to hepatorenal syndrome[134]. This study was limited, however, in that there isno billing distinction between type 1 and type 2hepatorenal syndrome; nevertheless, it is unlikely thatcombining both forms would underestimate the averageeconomic cost of type 1, which is more severe.
1637SN Compr. Clin. Med. (2020) 2:1628–1645

Spontaneous Bacterial Peritonitis:a Life-Threatening Complication of PortalHypertension
Pathophysiology
Portal hypertension is a direct cause of abdominal ascites[135]. Spontaneous bacterial peritonitis (SBP) is an infectionof this ascitic fluid without evidence of an intra-abdominalsource (such as an abscess, bowel perforation, colitis). SBPcarries a high mortality rate and is closely affiliated with cir-rhosis; other causes of portal hypertension and ascites mayresult in SBP, but this is uncommon [136, 137]. Ascitic fluidaccumulates when portal hypertension and the resultingsplanchnic vasodilation and fluid retention discussed previ-ously lead to elevated hydrostatic pressures in the splanchniccapillaries. This results in lymphatic leakage of fluid into theabdomen and overwhelms the lymphatic system’s ability toreturn it to circulation [138].
In SBP, infection occurs via translocation of intestinal bac-teria (most commonly Escherichia coli) across the bowel wall[15, 136]. The bacterium is taken up by mesenteric lymphnodes where it can directly inoculate the ascitic fluid, or itmay instead be taken up by lymphatics and enter the systemiccirculation where it “leaks” through splanchnic capillaries intothe abdomen or colonizes the surface of the liver. Patients withadvanced cirrhosis (and other immunocompromised patients)often have diluted, low levels of antimicrobial complementproteins in their abdominal fluid, crippling the phagocyticresponse to these bacteria [139–141]. In the setting of gastro-intestinal bleeding and hemorrhagic shock, overall infectionrisk further increases due to mucosal disruption and invasivemanipulation [142, 143].
Epidemiology—Incidence and Mortality
A study of ascitic fluid on asymptomatic outpatients revealeda prevalence of subclinical SBP in 3.1% [144]. Among inpa-tients undergoing diagnostic paracentesis, the incidence ofSBP is about 12–25% [145, 146]. Without antibiotic prophy-laxis, recurrence rates are up to 69%within the first 12 months[147]. This decreases to around 28.5% with antibiotic prophy-laxis based on a recent study by Marciano et al. [148].
In-hospital mortality rates for patients admitted with SBPare between 15 and 40% [16, 149]. The most important prog-nostic factor for survival in SBP is the development of renaldysfunction. A systematic review by Tandon et al. reported anin-hospital mortality rate of 11% among patients with SBPand normal renal function; in-hospital mortality in patientswho developed renal dysfunction increased to 67% [150].Delayed diagnostic paracentesis > 12 h after presentation alsoincreases in-hospital mortality [151]. Despite most patientssurviving an episode of SBP, the long-term prognosis remains
grim with a 3-year mortality rate of over 66% based on a largecohort study by Hung et al. [152].
Management of SBP—Diagnosis
SBP has a variable presentation. It may be clinically silent in apatient with cirrhosis and ascites who is admitted for othercauses, or it may manifest as fever, encephalopathy, abdomi-nal tenderness, nausea, or sepsis [153]. A high clinical suspi-cion and early paracentesis are essential for diagnosis; thepatient can be presumed to have SBP with an ascitic PMNcount of ≥ 250/mm3. Timing is crucial. A study by Kim et al.revealed a 2.7-fold increased mortality among patients withSBP whose initial paracentesis was delayed by 12 or morehours [151]. Positive cultures confirm the diagnosis but areoften negative [137]; collection of 10 mL of fluid for culture atthe bedside within standard blood culture bottles increases thesensitivity to 93% [154]. Measuring the serum-ascites albu-min gradient (SAAG) is important as well. A SAAG of >1.1 g/dL is highly correlated with portal hypertension [155];therefore, SBP would be unexpected in the setting of a SAAG< 1.1 g/dL.
The American Association for the Study of Liver Diseases(AASLD) recommends ancillary tests to rule out surgicalcauses of infected abdominal fluid (bowel perforation or ab-scess). Fungal or enterococcal species seen on Gram stain/culture are suspicious for perforation; elevated ascitic protein,elevated lactate dehydrogenase, or diminished glucose alsosupport a diagnosis of perforation [156]. The fluid should betested for carcinoembryonic antigen (CEA) and alkaline phos-phatase as well, as elevation of either of these values is asso-ciated with a 92% sensitivity and 88% specificity of bowelperforation [157]. Computed tomography of the abdomen andpelvis is indicated when there is suspicion for abscess or bow-el perforation or to evaluate for peritoneal metastatic disease[156, 158].
Management of SBP—Prophylaxis
In cirrhotic patients with portal hypertension, general mea-sures to control ascites include alcohol cessation, dietary saltrestriction, and diuretics. Diuretics increase ascitic proteinconcentration, improving the body’s opsonic response totranslocated bacteria. A typical diuretic regimen is combina-tion of daily spironolactone and furosemide [156, 159].Nonsteroidal anti-inflammatory drugs (NSAID’s) may resultin renal failure and fluid retention so should be used cautiously[160]. Patients should also be advised to avoid proton pumpinhibitors due to mixed data about their association with SBP[161, 162].
If medical therapy fails to control ascites, paracentesis maybe performed. This is an extremely safe procedure even incoagulopathic patients which is routinely performed by
1638 SN Compr. Clin. Med. (2020) 2:1628–1645

radiologists using ultrasound guidance [163]. Intravenous al-bumin given after the removal of large volumes of ascitic fluid(> 5 L) may increase intravascular oncotic pressure and pre-vent hypotension or acute renal failure due to plasmareaccumulation within the abdomen following paracentesis[156, 164]. Patients who require frequent, large volumeparacentesis and do not have advanced Child–Pugh C cirrho-sis or hepatic encephalopathy may be candidates for a TIPS,discussed previously with interventional management of var-iceal hemorrhage.
Multiple studies have demonstrated survival benefit andprotection from SBP for cirrhotic patients on prophylacticantibiotics [83]. Daily norfloxacin (currently unavailable inthe USA), ciprofloxacin, and trimethoprim-sulfamethoxazoleare options [165]. However, given the increase in antibioticresistance among infected ascites, prophylactic therapy is nowgenerally reserved for patients deemed at high risk for SBP. Aswith hepatorenal syndrome, evidence supports long-term an-tibiotic prophylaxis in patients with low-protein ascites (<1.5 g/dL) who demonstrate laboratory evidence of moderate-severe cirrhosis (Child–Pugh score of at least 9 with serumbilirubin ≥ 3 g/dL) and/or chronic renal disease (serum creat-inine ≥ 1.2 g/dL, blood urea nitrogen ≥ 25 mg/dL, or serumsodium ≤ 130 mEq/L). Patients who have already survived anepisode of SBP are also at high risk for recurrence and shouldreceive prophylaxis as well [147, 156]. Cirrhotic patients pre-senting with gastrointestinal hemorrhage are another high-riskgroup who should receive a short-term 7-day course of anti-biotics to protect against SBP [166].
Fortunately, although antibiotic resistance is emerging, thesuccess of antibiotic prophylaxis at preventing recurrent SBPmay be unaffected. A recent study by Marciano et al. reporteda 1-year recurrence rate of SBP of 28.5% in patients onnorfloxacin, an incidence similar to initial studies prior toroutine antibiotic prophylaxis [148, 167].
Management of SBP—Acute Therapy
Patients with a provisional diagnosis of SBP based uponparacentesis with PMN count ≥ 250/mm3 are started on em-piric antibiotic therapy, often with a broad-spectrum third-gen-eration cephalosporin such as cefotaxime. However, due toincreasing antibiotic resistance to third-generation cephalo-sporins, particularly among nosocomial infections developing> 48 h after hospital admission, it may be necessary to obtainrepeat cultures or initiate broader coverage and then narrowtreatment once culture results become available [168, 169]. Atypical course of treatment lasts 5 days [170].
Nonselective beta-blockers should be discontinued in pa-tients with SBP. A retrospective study by Mandorfer et al.identified an increased risk of hemodynamic compromiseand hepatorenal syndrome in patients with SBP who wereon nonselective beta-blockers [171].
SBP and other infections are recognized as a direct triggerof type 1 hepatorenal syndrome. There is modest evidence thatalbumin infusions on days 1 and 3 may help prevent the onsetof renal failure in patients with SBP and certain baseline lab-oratory findings (serum creatinine > 1 g/dL, bilirubin > 4 g/dL, blood urea nitrogen > 30) [172, 173].
Associated Cost
Niu et al. recently studied the United States NationwideInpatient Sample between 2006 and 2014 and identified over88,000 cases of spontaneous bacterial peritonitis and an asso-ciated in-hospital mortality rate of 17.6%. In the subgroup ofinpatients who succumbed to SBP, the average hospital costwas higher (over $138,000 versus $78,000 among patientswho survived), and the length of stay was longer (average of11.6 days versus 9.6 days) [16]. A theoretical study performedin 1997 by Inadomi et al. predicted an overall cost savings of$2216 to $9251 per patient per year on antibiotic prophylaxisfor spontaneous bacterial peritonitis [174].
The overall economic burden of ascites, spontaneous bac-terial peritonitis, and other consequences of portal hyperten-sion directly reflect the staggering costs of cirrhosis. The esti-mated direct annual cost of cirrhosis in the USA was $1.4billion in 2013 [175]. This does not include the indirect costsassociated with cirrhosis such as lost work productivity. Anadditional interesting finding is that hospital charges increasedfrom 1993 to 2009 from approximately $20,000 to $47,000despite a decreasing average length of stay (7.3 days in 1993versus 5.3 days in 2009) and a relatively stable incidence ofcomplications related to portal hypertension [175].
Conclusion
Cirrhosis, the most common cause of portal hypertension, ischaracterized by hepatic fibrosis and the obstruction of thehepatic sinusoids, resulting in increased vascular resistancethrough the liver. In combination with retention of fluid bythe kidneys and redistribution of that fluid into the splanchnicvasculature, portal hypertension develops. Portosystemic col-lateral vessels form, dilate, and rupture, resulting in life-threatening variceal hemorrhage. Fluid that is rerouted fromthe systemic vasculature to the splanchnic vasculature no lon-ger perfuses the kidneys, leading to renal dysfunction andfulminant type 1 hepatorenal syndrome. Pressurized fluid inthe splanchnic vasculature leaks into the abdominal cavity asascites, a vulnerable target for infectious spontaneous bacterialperitonitis.
The pathophysiology of cirrhotic portal hypertension iscomplex, and so is its management. Achieving the best possi-ble outcome for a patient requires knowledgeable primary careproviders and gastroenterologists, attentive ICU physicians,
1639SN Compr. Clin. Med. (2020) 2:1628–1645

and subspecialist nephrologists, radiologists, and surgeonswho know how their specialties should intersect in the careof each patient. Awareness of the severity of cirrhotic portalhypertension and clinical signs of impending mortality shouldbe in the minds of all care providers. This enables the coordi-nated team approach which can best manage these precariousclinical situations. Separately (but also importantly), profes-sionals should be aware of the financial impacts of their ac-tions as costs have continued to rise in spite of stable incidenceof portal hypertensive complications. We must be wise stew-ards of limited resources.
In summary, cirrhotic portal hypertension is a prevalent,costly, and life-threatening disease process characterized byaltered hemodynamics. Particularly now, with the global prev-alence of fatty liver disease reaching epidemic proportions,portal hypertension, its management, and its therapeutic short-comings demand increased awareness.
Compliance with Ethical Standards
Conflict of Interest The authors declare that they have no conflict ofinterest.
References
1. Al-Busafi SA, McNabb-Baltar J, Farag A, Hilzenrat N. Clinicalmanifestations of portal hypertension. Int J Hepatol. 2012;2012:203794–10. https://doi.org/10.1155/2012/203794.
2. Garcia-Tsao G. Idiopathic noncirrhotic portal hypertension: whatis it? Clin Liver Dis (Hoboken). 2015;5:120–2. https://doi.org/10.1002/cld.472.
3. Scaglione S, Kliethermes S, Cao G, Shoham D, Durazo R, LukeA, et al. The epidemiology of cirrhosis in the United States: apopulation-based study. J Clin Gastroenterol. 2015;49:690–6.https://doi.org/10.1097/MCG.0000000000000208.
4. Asrani SK, Devarbhavi H, Eaton J, Kamath PS. Burden of liverdiseases in the world. J Hepatol. 2019;70:151–71. https://doi.org/10.1016/j.jhep.2018.09.014.
5. Mendes FD, Suzuki A, Sanderson SO, Lindor KD, Angulo P.Prevalence and indicators of portal hypertension in patients withnonalcoholic fatty liver disease. Clin Gastroenterol Hepatol.2012;10:1028–1033.e2. https://doi.org/10.1016/j.cgh.2012.05.008.
6. Pant C, Olyaee M, Gilroy R, et al. Emergency department visitsrelated to cirrhosis: a retrospective study of the nationwide emer-gency department sample 2006 to 2011. Medicine (Baltimore).2015;94:e308. https://doi.org/10.1097/MD.0000000000000308.
7. Elbaz T, Esmat G. Hepatic and intestinal schistosomiasis: review. JAdv Res. 2013;4:445–52. https://doi.org/10.1016/j.jare.2012.12.001.
8. Chitsulo L, Engels D,Montresor A, Savioli L. The global status ofschistosomiasis and its control. Acta Trop. 2000;77:41–51. https://doi.org/10.1016/s0001-706x(00)00122-4.
9. Sarin SK, Sollano JD, Chawla YK, Amarapurkar D, Hamid S,Hashizume M, et al. Consensus on extra-hepatic portal vein ob-struction. Liver Int. 2006;26:512–9. https://doi.org/10.1111/j.1478-3231.2006.01269.x.
10. Weiss B, Shteyer E, Vivante A, Berkowitz D, Reif S, Weizman Z,et al. Etiology and long-term outcome of extrahepatic portal vein
obstruction in children. World J Gastroenterol. 2010;16:4968–72.https://doi.org/10.3748/wjg.v16.i39.4968.
11. Wani ZA, Bhat RA, Bhadoria AS, Maiwall R. Extrahepatic portalvein obstruction and portal vein thrombosis in special situations:need for a new classification. Saudi J Gastroenterol. 2015;21:129–38. https://doi.org/10.4103/1319-3767.157550.
12. Semela D. Systemic disease associated with noncirrhotic portalhypertension. Clin Liver Dis (Hoboken). 2015;6:103–6. https://doi.org/10.1002/cld.505.
13. Iwakiri Y. Pathophysiology of portal hypertension. Clin Liver Dis(Hoboken). 2014;18:281–91. https://doi.org/10.1016/j.cld.2013.12.001.
14. Bosch J, Pizcueta P, Feu F, Fernández M, García-Pagán JC.Pathophysiology of portal hypertension. Gastroenterol ClinNorth Am. 1992;21:1–14.
15. Pedersen JS, Bendtsen F, Møller S. Management of cirrhotic as-cites. Ther Adv Chronic Dis. 2015;6:124–37. https://doi.org/10.1177/2040622315580069.
16. Niu B, Kim B, Limketkai BN, Sun J, Li Z, Woreta T, et al.Mortality from spontaneous bacterial peritonitis among hospital-ized patients in the USA. Dig Dis Sci. 2018;63:1327–33. https://doi.org/10.1007/s10620-018-4990-y.
17. Kumar A, Sharma P, Sarin SK. Hepatic venous pressure gradientmeasurement: time to learn! Indian J Gastroenterol. 2008;27:74–80.
18. Berzigotti A, Seijo S, Reverter E, Bosch J. Assessing portal hy-pertension in liver diseases. Expert Rev Gastroenterol Hepatol.2013;7:141–55. https://doi.org/10.1586/egh.12.83.
19. Seijo S, Reverter E,Miquel R, Berzigotti A, Abraldes JG, Bosch J,et al. Role of hepatic vein catheterisation and transientelastography in the diagnosis of idiopathic portal hypertension.Dig Liver Dis. 2012;44:855–60. https://doi.org/10.1016/j.dld.2012.05.005.
20. Sarin SK, Sethi KK, Nanda R. Measurement and correlation ofwedged hepatic, intrahepatic, intrasplenic and intravariceal pres-sures in patients with cirrhosis of liver and non-cirrhotic portalfibrosis. Gut. 1987;28:260–6. https://doi.org/10.1136/gut.28.3.260.
21. Taourel P, Blanc P, Dauzat M, Chabre M, Pradel J, Gallix B, et al.Doppler study of mesenteric, hepatic, and portal circulation inalcoholic cirrhosis: relationship between quantitative Dopplermeasurements and the severity of portal hypertension and hepaticfailure. Hepatology. 1998;28:932–6. https://doi.org/10.1002/hep.510280406.
22. Iranpour P, Lall C, Houshyar R, et al. Altered Doppler flow pat-terns in cirrhosis patients: an overview. Ultrasonography. 2016;35:3–12. https://doi.org/10.14366/usg.15020.
23. Haag K, Rössle M, Ochs A, Huber M, Siegerstetter V, OlschewskiM, et al. Correlation of duplex sonography findings and portalpressure in 375 patients with portal hypertension. AJR Am JRoentgenol. 1999;172:631–5. https://doi.org/10.2214/ajr.172.3.10063849.
24. McNaughton DA, Abu-Yousef MM. Doppler US of the livermade simple [published correction appears in Radiographics.2011;31:904]. Radiographics. 2011;31:161–88. https://doi.org/10.1148/rg.311105093.
25. de Vries PJ, van Hattum J, Hoekstra JB, de Hooge P. DuplexDoppler measurements of portal venous flow in normal subjects.Inter- and intra-observer variability. J Hepatol. 1991;13:358–63.https://doi.org/10.1016/0168-8278(91)90081-l.
26. Paulson EK, Kliewer MA, Frederick MG, Keogan MT, DeLongDM, Nelson RC. Doppler USmeasurement of portal venous flow:variability in healthy fasting volunteers. Radiology. 1997;202:721–4. https://doi.org/10.1148/radiology.202.3.9051024.
27. Oppo K, Leen E, AngersonWJ, Cooke TG,McArdle CS. Dopplerperfusion index: an interobserver and intraobserver reproducibility
1640 SN Compr. Clin. Med. (2020) 2:1628–1645

study. Radiology. 1998;208:453–7. https://doi.org/10.1148/radiology.208.2.9680575.
28. Roldán-Alzate A, Frydrychowicz A, Niespodzany E, LandgrafBR, Johnson KM, Wieben O, et al. In vivo validation of 4D flowMRI for assessing the hemodynamics of portal hypertension. JMagn Reson Imaging. 2013;37:1100–8. https://doi.org/10.1002/jmri.23906.
29. Vermeulen MA, Ligthart-Melis GC, Buijsman R, et al. Accurateperioperative flowmeasurement of the portal vein and hepatic andrenal artery: a role for preoperative MRI? Eur J Radiol. 2012;81:2042–8. https://doi.org/10.1016/j.ejrad.2011.06.023.
30. Stankovic Z, Csatari Z, Deibert P, Euringer W, Blanke P, KreiselW, et al. Normal and altered three-dimensional portal venous he-modynamics in patients with liver cirrhosis. Radiology. 2012;262:862–73. https://doi.org/10.1148/radiol.11110127.
31. Sugano S, Yamamoto K, Sasao K, Watanabe M. Portal venousblood flow while breath-holding after inspiration or expirationand during normal respiration in controls and cirrhotics. JGastroenterol. 1999;34:613–8. https://doi.org/10.1007/s005350050381.
32. Brown HS, Halliwell M, Qamar M, Read AE, Evans JM, WellsPN. Measurement of normal portal venous blood flow by Dopplerultrasound. Gut. 1989;30:503–9. https://doi.org/10.1136/gut.30.4.503.
33. Shi BM, Wang XY, Mu QL, Wu TH, Xu J. Value of portal hemo-dynamics and hypersplenism in cirrhosis staging. World JGastroenterol. 2005;11:708–11. https://doi.org/10.3748/wjg.v11.i5.708.
34. Ljubicić N, Duvnjak M, Rotkvić I, Kopjar B. Influence of thedegree of liver failure on portal blood flow in patients with livercirrhosis. Scand J Gastroenterol. 1990;25:395–400. https://doi.org/10.3109/00365529009095505.
35. Chawla Y, Santa N, Dhiman RK, Dilawari JB. Portal hemodynam-ics by duplex Doppler sonography in different grades of cirrhosis.Dig Dis Sci. 1998;43:354–7. https://doi.org/10.1023/a:1018814624307.
36. Philips CA, Arora A, Shetty R, Kasana V. A comprehensive re-view of portosystemic collaterals in cirrhosis: historical aspects,anatomy, and classifications. Int J Hepatol. 2016;6170243:1–15.https://doi.org/10.1155/2016/6170243.
37. Choi BI, Lee KH, Han JK, Lee JM. Hepatic arterioportal shunts:dynamic CT and MR features. Korean J Radiol. 2002;3:1–15.https://doi.org/10.3348/kjr.2002.3.1.1.
38. Hu LS, George J, Wang JH. Current concepts on the role of nitricoxide in portal hypertension. World J Gastroenterol. 2013;19:1707–17. https://doi.org/10.3748/wjg.v19.i11.1707.
39. Iwakiri Y, Groszmann RJ. Vascular endothelial dysfunction incirrhosis. J Hepatol. 2007;46:927–34. https://doi.org/10.1016/j.jhep.2007.02.006.
40. Bosch J, Groszmann RJ, ShahVH. Evolution in the understandingof the pathophysiological basis of portal hypertension: how chang-es in paradigm are leading to successful new treatments. J Hepatol.2015;62(suppl 1):S121–30. https://doi.org/10.1016/j.jhep.2015.01.003.
41. Yzet T, Bouzerar R, Allart JD, Demuynck F, Legallais C, RobertB, et al. Hepatic vascular flow measurements by phase contrastMRI and Doppler echography: a comparative and reproducibilitystudy. J Magn Reson Imaging. 2010;31:579–88. https://doi.org/10.1002/jmri.22079.
42. Kondo T, Maruyama H, Sekimoto T, Shimada T, Takahashi M,Yokosuka O. Reversed portal flow: clinical influence on the long-term outcomes in cirrhosis. World J Gastroenterol. 2015;21:8894–902. https://doi.org/10.3748/wjg.v21.i29.8894.
43. Mittal P, Gupta R, Mittal G, Kalia V. Association between portalvein color Doppler findings and the severity of disease in cirrhotic
patients with portal hypertension. Iran J Radiol. 2011;8:211–7.https://doi.org/10.5812/iranjradiol.4489.
44. Gaiani S, Bolondi L, Li Bassi S, Zironi G, Siringo S, Barbara L.Prevalence of spontaneous hepatofugal portal flow in liver cirrho-sis. Clinical and endoscopic correlation in 228 patients.Gastroenterology. 1991;100:160–7. https://doi.org/10.1016/0016-5085(91)90596-d.
45. Koda M, Murawaki Y, Kawasaki H, Ikawa S. Portal blood veloc-ity and portal blood flow in patients with chronic viral hepatitis:relation to histological liver fibrosis. Hepatogastroenterology.1996;43:199–202.
46. Lycklama à Nijeholt GJ, Burggraaf K, Wasser MN, et al.Variability of splanchnic blood flow measurements using MRvelocity mapping under fasting and post-prandial conditions—comparison with echo-Doppler. J Hepatol. 1997;26:298–304.https://doi.org/10.1016/s0168-8278(97)80045-1.
47. Achim CA, Bordei P, Dumitru E. The role of ultrasonography inthe evaluation of portal hemodynamics in healthy adults and path-ologic conditions. ARS Medica Tomitana. 2016;22:128–34.https://doi.org/10.1515/arsm-2016-0022.
48. Bolognesi M, Verardo A, Di Pascoli M. Peculiar characteristics ofportal-hepatic hemodynamics of alcoholic cirrhosis. World JGastroenterol. 2014;20:8005–10. https://doi.org/10.3748/wjg.v20.i25.8005.
49. Fernandez M, Vizzutti F, Garcia-Pagan JC, Rodes J, Bosch J.Anti-VEGF receptor-2 monoclonal antibody prevents portal-systemic collateral vessel formation in portal hypertensive mice.Gastroenterology. 2004;126:886–94. https://doi.org/10.1053/j.gastro.2003.12.012.
50. Herman J, Baram M. Blood and volume resuscitation for varicealhemorrhage. Ann Am Thorac Soc. 2015;12:1100–2. https://doi.org/10.1513/AnnalsATS.201502-095CC.
51. Goulis J, Patch D, Burroughs AK. Bacterial infection in the path-ogenesis of variceal bleeding. Lancet. 1999;353:139–42. https://doi.org/10.1016/S0140-6736(98)06020-6.
52. Wani ZA, Bhat RA, Bhadoria AS, Maiwall R, Choudhury A.Gastric varices: classification, endoscopic and ultrasonographicmanagement. J Res Med Sci. 2015;20:1200–7. https://doi.org/10.4103/1735-1995.172990.
53. Sarin SK, Kumar CKN. Ectopic varices. Clin Liver Dis(Hoboken). 2012;1:167–72. https://doi.org/10.1002/cld.95.
54. Karatzas A, Konstantakis C, Aggeletopoulou I, KalogeropoulouC, Thomopoulos K, Triantos C. Non-invasive screening foresophageal varices in patients with liver cirrhosis. AnnGastroenterol. 2018;31:305–14. https://doi.org/10.20524/aog.2018.0241.
55. Merli M, Nicolini G, Angeloni S, Rinaldi V, de Santis A, MerkelC, et al. Incidence and natural history of small esophageal varicesin cirrhotic patients. J Hepatol. 2003;38:266–72. https://doi.org/10.1016/s0168-8278(02)00420-8.
56. D’Amico G, Pasta L, Morabito A, et al. Competing risks andprognostic stages of cirrhosis: a 25-year inception cohort studyof 494 patients. Aliment Pharmacol Ther. 2014;39:1180–93.https://doi.org/10.1111/apt.12721.
57. Kovalak M, Lake J, Mattek N, Eisen G, Lieberman D, Zaman A.Endoscopic screening for varices in cirrhotic patients: data from anational endoscopic database. Gastrointest Endosc. 2007;65:82–8.https://doi.org/10.1016/j.gie.2006.08.023.
58. Grace ND. Prevention of initial variceal hemorrhage.Gastroenterol Clin North Am. 1992;21:149–61.
59. North Italian Endoscopic Club for the Study and Treatment ofEsophageal Varices. Prediction of the first variceal hemorrhagein patients with chirrhosis of the liver and esophageal varices. Aprospective multicenter study. N Engl J Med. 1988;319:983–9.https://doi.org/10.1056/NEJM198810133191505.
1641SN Compr. Clin. Med. (2020) 2:1628–1645

60. Carbonell N, Pauwels A, Serfaty L, Fourdan O, Lévy VG, PouponR. Improved survival after variceal bleeding in patients with cir-rhosis over the past two decades. Hepatology. 2004;40:652–9.https://doi.org/10.1002/hep.20339.
61. de Franchis R, Faculty BV. Revising consensus in portal hyper-tension: report of the Baveno V consensus workshop on method-ology of diagnosis and therapy in portal hypertension. J Hepatol.2010;53:762–8. https://doi.org/10.1016/j.jhep.2010.06.004.
62. D’Amico G, De Franchis R, Cooperative Study Group. Upperdigestive bleeding in cirrhosis. Post-therapeutic outcome andprognostic indicators. Hepatology. 2003;38:599–612. https://doi.org/10.1053/jhep.2003.50385.
63. Cho H, Nagata N, Shimbo T, Sakurai T, Sekine K, Okubo H, et al.Recurrence and prognosis of patients emergently hospitalized foracute esophageal variceal bleeding: a long-term cohort study.Hepatol Res. 2016;46:1338–46. https://doi.org/10.1111/hepr.12692.
64. Jairath V, Rehal S, Logan R, Kahan B, Hearnshaw S, Stanworth S,et al. Acute variceal hemorrhage in the United Kingdom: patientcharacteristics, management and outcomes in a nationwide audit.Dig Liver Dis. 2014;46:419–26. https://doi.org/10.1016/j.dld.2013.12.010.
65. Bosch J, García-Pagán JC. Prevention of variceal rebleeding.Lancet. 2003;361:952–4. https://doi.org/10.1016/S0140-6736(03)12778-X.
66. Bambha K, KimWR, Pedersen R, Bida JP, KremersWK, KamathPS. Predictors of early re-bleeding and mortality after acute vari-ceal haemorrhage in patients with cirrhosis. Gut. 2008;57:814–20.https://doi.org/10.1136/gut.2007.137489.
67. Garcia-Tsao G, Sanyal AJ, Grace ND, Carey WD, PracticeGuidelines Committee of American Association for Study ofLiver Diseases; Practice Parameters Committee of AmericanCollege of gastroenterology. Prevention and management of var-ices and variceal hemorrhage in cirrhosis [published correctionappears in Am J Gastroenterol. 2007;102:2868]. Am JGastroenterol. 2007;102:2086–102. https://doi.org/10.1111/j.1572-0241.2007.01481.x.
68. Gioia S, Nardelli S, Pasquale C, Pentassuglio I, Nicoletti V, AprileF, et al. Natural history of patients with non cirrhotic portal hyper-tension: comparisonwith patients with compensated cirrhosis. DigLiver Dis. 2018;50:839–44. https://doi.org/10.1016/j.dld.2018.01.132.
69. Siramolpiwat S, Seijo S,Miquel R, Berzigotti A, Garcia-CriadoA,Darnell A, et al. Idiopathic portal hypertension: natural history andlong-term outcome. Hepatology. 2014;59:2276–85. https://doi.org/10.1002/hep.26904.
70. El Atti EA, Nevens F, Bogaerts K, Verbeke G, Fevery J. Varicealpressure is a strong predictor of variceal haemorrhage in patientswith cirrhosis as well as in patients with non-cirrhotic portal hy-pertension. Gut. 1999;45:618–21. https://doi.org/10.1136/gut.45.4.618.
71. Ferreira CN, Seijo S, Plessier A, et al. Natural history and man-agement of esophagogastric varices in chronic noncirrhotic,nontumoral portal vein thrombosis. Hepatology. 2016;63:1640–50. https://doi.org/10.1002/hep.28466.
72. Mohammed SE, Abdo AE, Mudawi HM. Mortality andrebleeding following variceal haemorrhage in liver cirrhosis andperiportal fibrosis. World J Hepatol. 2016;8:1336–42. https://doi.org/10.4254/wjh.v8.i31.1336.
73. Sarin SK, Kumar A, Angus PW, Asian Pacific Association for theStudy of the Liver (APASL) Working Party on PortalHypertension, et al. Diagnosis and management of acute varicealbleeding: Asian Pacific Association for Study of the Liver recom-mendations. Hepatol Int. 2011;5:607–24. https://doi.org/10.1007/s12072-010-9236-9.
74. Khan NM, Shapiro AB. The white nipple sign: please do notdisturb. Case Rep Gastroenterol. 2011;5:386–90. https://doi.org/10.1159/000330292.
75. Groszmann RJ, Garcia-Tsao G, Bosch J, Portal HypertensionCollaborative Group, et al. Beta-blockers to prevent gastroesoph-ageal varices in patients with cirrhosis. N Engl J Med. 2005;353:2254–61. https://doi.org/10.1056/NEJMoa044456.
76. Garcia-Tsao G, Abraldes JG, Berzigotti A, Bosch J. Portal hyper-tensive bleeding in cirrhosis: risk stratification, diagnosis, andmanagement: 2016 practice guidance by the AmericanAssociation for the Study of Liver Diseases [published correctionappears in Hepatology. 2017;66:304]. Hepatology. 2017;65:310–35. https://doi.org/10.1002/hep.28906.
77. Fernández J, Tandon P, Mensa J, Garcia-Tsao G. Antibiotic pro-phylaxis in cirrhosis: good and bad. Hepatology. 2016;63:2019–31. https://doi.org/10.1002/hep.28330.
78. de Franchis R, Faculty BVI. Expanding consensus in portal hy-pertension: report of the Baveno VI Consensus Workshop: strati-fying risk and individualizing care for portal hypertension. JHepatol. 2015;63:743–52. https://doi.org/10.1016/j.jhep.2015.05.022.
79. Heidemann J, Bartels C, Berssenbrügge C, Schmidt H, Meister T.Hepatorenal syndrome: outcome of response to therapy and pre-dictors of survival. Gastroenterol Res Pract. 2015;2015:457613–8.https://doi.org/10.1155/2015/457613.
80. Kim YD. Management of acute variceal bleeding. Clin Endosc.2014;47:308–14. https://doi.org/10.5946/ce.2014.47.4.308.
81. McKay R, Webster NR. Variceal bleeding. Contin Educ AnaesthCrit Care Pain. 2007;7:191–4. https://doi.org/10.1093/bjaceaccp/mkm038.
82. Villanueva C, Colomo A, Bosch A, Concepción M, Hernandez-Gea V, Aracil C, et al. Transfusion strategies for acute upper gas-trointestinal bleeding [published correction appears in N Engl JMed. 2013;368:2341]. N Engl J Med. 2013;368:11–21. https://doi.org/10.1056/NEJMoa1211801.
83. Chavez-Tapia NC, Barrientos-Gutierrez T, Tellez-Avila F, Soares-Weiser K, Mendez-Sanchez N, Gluud C, et al. Meta-analysis:antibiotic prophylaxis for cirrhotic patients with upper gastrointes-tinal bleeding—an updated Cochrane review. Aliment PharmacolTher. 2011;34:509–18. https://doi.org/10.1111/j.1365-2036.2011.04746.x.
84. Wells M, Chande N, Adams P, Beaton M, Levstik M, Boyce E,et al. Meta-analysis: vasoactive medications for the managementof acute variceal bleeds. Aliment Pharmacol Ther. 2012;35:1267–78. https://doi.org/10.1111/j.1365-2036.2012.05088.x.
85. Escorsell À, Pavel O, Cárdenas A, Morillas R, Llop E, VillanuevaC, et al. Esophageal balloon tamponade versus esophageal stent incontrolling acute refractory variceal bleeding: a multicenter ran-domized, controlled trial. Hepatology. 2016;63:1957–67. https://doi.org/10.1002/hep.28360.
86. Addley J, ThamTC, CashWJ. Use of portal pressure studies in themanagement of variceal haemorrhage. World J GastrointestEndosc. 2012;4:281–9. https://doi.org/10.4253/wjge.v4.i7.281.
87. Villanueva C, Balanzó J. Variceal bleeding: pharmacological treat-ment and prophylactic strategies. Drugs. 2008;68:2303–24.https://doi.org/10.2165/0003495-200868160-00004.
88. Abraldes JG, Villanueva C, Bañares R, Aracil C, Catalina MV,Garci A-Pagán JC, et al. Hepatic venous pressure gradient andprognosis in patients with acute variceal bleeding treated withpharmacologic and endoscopic therapy. J Hepatol. 2008;48:229–36. https://doi.org/10.1016/j.jhep.2007.10.008.
89. Saad WE. Balloon-occluded retrograde transvenous obliterationof gastric varices: concept, basic techniques, and outcomes [com-ment]. Semin Interv Radiol. 2012;29:118–28. https://doi.org/10.1055/s-0032-1312573.
1642 SN Compr. Clin. Med. (2020) 2:1628–1645

90. Win AZ. Image guided portal vein access techniques in TIPScreation and considerations regarding their use. Ann Transl Med.2016;4:226. https://doi.org/10.21037/atm.2016.05.43.
91. Saad WE, Darcy MD. Transjugular intrahepatic portosystemicshunt (TIPS) versus balloon-occluded retrograde transvenousobliteration (BRTO) for the management of gastric varices.Semin Interv Radiol. 2011;28:339–49. https://doi.org/10.1055/s-0031-1284461.
92. Sanyal AJ, Freedman AM, Luketic VA, Purdum PP 3rd, ShiffmanML, DeMeo J, et al. The natural history of portal hypertensionafter transjugular intrahepatic portosystemic shunts.Gastroenterology. 1997;112:889–98. https://doi.org/10.1053/gast.1997.v112.pm9041251.
93. Bureau C,Garcia Pagan JC, Layrargues GP, et al. Patency of stentscovered with polytetrafluoroethylene in patients treated bytransjugular intrahepatic portosystemic shunts: long-term resultsof a randomized multicentre study. Liver Int. 2007;27:742–7.https://doi.org/10.1111/j.1478-3231.2007.01522.x.
94. D’Amico G, Garcia-Pagan JC, Luca A, Bosch J. Hepatic veinpressure gradient reduction and prevention of variceal bleedingin cirrhosis: a systematic review. Gastroenterology. 2006;131:1611–24. https://doi.org/10.1053/j.gastro.2006.09.013.
95. Gur I, Diggs BS, Orloff SL. Surgical portosystemic shunts in theera of TIPS and liver transplantation are still relevant. HPB(Oxford). 2014;16:481–93. https://doi.org/10.1111/hpb.12163.
96. Young V, Rajeswaran S. Management of portal hypertension inthe pediatric population: a primer for the interventional radiologist.Semin Interv Radiol. 2018;35:160–4. https://doi.org/10.1055/s-0038-1660794.
97. Zaman A, Goldberg RJ, Pettit KG, et al. Cost of treating an epi-sode of variceal bleeding in a VA setting. Am J Gastroenterol.2000;95:1323–30. https://doi.org/10.1111/j.1572-0241.2000.02020.x.
98. Thabut D, Hammer M, Cai Y, Carbonell N. Cost of treatment ofoesophageal variceal bleeding in patients with cirrhosis in France:results of a French survey. Eur J Gastroenterol Hepatol. 2007;19:679–86. https://doi.org/10.1097/MEG.0b013e3281bcb784.
99. Viviane A, Barkun AN. Estimates of costs of hospital stay forvariceal and nonvariceal upper gastrointestinal bleeding in theUnited States. Value Health. 2008;11:1–3. https://doi.org/10.1111/j.1524-4733.2007.00208.x.
100. Bayraktar UD, Seren S, Bayraktar Y. Hepatic venous outflowobstruction: three similar syndromes. World J Gastroenterol.2007;13:1912–27. https://doi.org/10.3748/wjg.v13.i13.1912.
101. Humphreys BD, Soiffer RJ, Magee CC. Renal failure associatedwith cancer and its treatment: an update. J Am Soc Nephrol.2005;16:151–61. https://doi.org/10.1681/ASN.2004100843.
102. Low G, Alexander GJ, Lomas DJ. Hepatorenal syndrome:aetiology, diagnosis, and treatment. Gastroenterol Res Pract.2015;2015:207012–1. https://doi.org/10.1155/2015/207012.
103. Zardi EM, Abbate A, Zardi DM, Dobrina A, Margiotta D, vanTassel BW, et al. Cirrhotic cardiomyopathy. J Am Coll Cardiol.2010;56:539–49. https://doi.org/10.1016/j.jacc.2009.12.075.
104. Solà E, Ginès P. Renal and circulatory dysfunction in cirrhosis:current management and future perspectives. J Hepatol. 2010;53:1135–45. https://doi.org/10.1016/j.jhep.2010.08.001.
105. Angeli P, Garcia-Tsao G, Nadim MK, Parikh CR. News in path-ophysiology, definition and classification of hepatorenal syn-drome: a step beyond the International Club of Ascites (ICA)consensus document. J Hepatol. 2019;71(4):811–22. https://doi.org/10.1016/j.jhep.2019.07.002.
106. Wadei HM, Mai ML, Ahsan N, Gonwa TA. Hepatorenal syn-drome: pathophysiology and management. Clin J Am SocNephrol. 2006;1:1066–79. https://doi.org/10.2215/CJN.01340406.
107. Ginès A, Escorsell A, Ginès P, Saló J, Jiménez W, Inglada L, et al.Incidence, predictive factors, and prognosis of the hepatorenalsyndrome in cirrhosis with ascites. Gastroenterology. 1993;105:229–36. https://doi.org/10.1016/0016-5085(93)90031-7.
108. Martín-llahí M, Guevara M, Torre A, et al. Prognostic importanceof the cause of renal failure in patients with cirrhosis.Gastroenterology. 2011;140:488–496.e4. https://doi.org/10.1053/j.gastro.2010.07.043.
109. Salerno F, Cazzaniga M, Merli M, Spinzi G, Saibeni S, Salmi A,et al. Diagnosis, treatment and survival of patients withhepatorenal syndrome: a survey on daily medical practice. JHepatol. 2011;55:1241–8. https://doi.org/10.1016/j.jhep.2011.03.012.
110. Terra C, Guevara M, Torre A, Gilabert R, Fernández J, Martín-Llahí M, et al. Renal failure in patients with cirrhosis and sepsisunrelated to spontaneous bacterial peritonitis: value of MELDscore. Gastroenterology. 2005;129:1944–53. https://doi.org/10.1053/j.gastro.2005.09.024.
111. Fasolato S, Angeli P, Dallagnese L, Maresio G, Zola E, Mazza E,et al. Renal failure and bacterial infections in patients with cirrho-sis: epidemiology and clinical features. Hepatology. 2007;45:223–9. https://doi.org/10.1002/hep.21443.
112. Montoliu S, Ballesté B, Planas R, Álvarez MA, Rivera M, MiquelM, et al. Incidence and prognosis of different types of functionalrenal failure in cirrhotic patients with ascites. Clin GastroenterolHepatol. 2010;8:616–22, e80. https://doi.org/10.1016/j.cgh.2010.03.029.
113. Ginés P, Quintero E, Arroyo V, Terés J, Bruguera M, Rimola A,et al. Compensated cirrhosis: natural history and prognostic fac-tors. Hepatology. 1987;7:122–8. https://doi.org/10.1002/hep.1840070124.
114. Fagundes C, Pépin MN, Guevara M, Barreto R, Casals G, Solà E,et al. Urinary neutrophil gelatinase-associated lipocalin as bio-marker in the differential diagnosis of impairment of kidney func-tion in cirrhosis. J Hepatol. 2012;57:267–73. https://doi.org/10.1016/j.jhep.2012.03.015.
115. Markwardt D, Holdt L, Steib C, Benesic A, Bendtsen F, BernardiM, et al. Plasma cystatin C is a predictor of renal dysfunction,acute-on-chronic liver failure, and mortality in patients with acute-ly decompensated liver cirrhosis. Hepatology. 2017;66:1232–41.https://doi.org/10.1002/hep.29290.
116. Fernández J, Navasa M, Planas R, Montoliu S, Monfort D,Soriano G, et al. Primary prophylaxis of spontaneous bacterialperitonitis delays hepatorenal syndrome and improves survivalin cirrhosis. Gastroenterology. 2007;133:818–24. https://doi.org/10.1053/j.gastro.2007.06.065.
117. Whitfield K, Rambaldi A, Wetterslev J, Gluud C. Pentoxifyllinefor alcoholic hepatitis. Cochrane Database Syst Rev. 2009;2009:CD007339. https://doi.org/10.1002/14651858.CD007339.pub2.
118. Wong F, Leung W, Al Beshir M, Marquez M, Renner EL.Outcomes of patient with cirrhosis and hepatorenal syndrome type1 treated with liver transplantation. Liver Transpl. 2015;21:300–7.https://doi.org/10.1002/lt.24049.
119. Modi RM, Patel N, Metwally SN, Mumtaz K. Outcomes of livertransplantation in patients with hepatorenal syndrome. World JHepatol. 2016;8:999–1011. https://doi.org/10.4254/wjh.v8.i24.999.
120. Dundar HZ, Yılmazlar T. Management of hepatorenal syndrome.World J Nephrol. 2015;4:277–86. https://doi.org/10.5527/wjn.v4.i2.277.
121. Velez JC, Nietert PJ. Therapeutic response to vasoconstrictors inhepatorenal syndrome parallels increase in mean arterial pressure:a pooled analysis of clinical trials. Am J Kidney Dis. 2011;58:928–38. https://doi.org/10.1053/j.ajkd.2011.07.017.
122. Narahara Y, Kanazawa H, Taki Y, Kimura Y, Atsukawa M,Katakura T, et al. Effects of terlipressin on systemic, hepatic and
1643SN Compr. Clin. Med. (2020) 2:1628–1645

renal hemodynamics in patients with cirrhosis. J GastroenterolHepatol. 2009;24:1791–7. https://doi.org/10.1111/j.1440-1746.2009.05873.x.
123. Arroyo V, Fernández J. Management of hepatorenal syndrome inpatients with cirrhosis. Nat Rev Nephrol. 2011;7:517–26. https://doi.org/10.1038/nrneph.2011.96.
124. Skagen C, Einstein M, LuceyMR, Said A. Combination treatmentwith octreotide, midodrine, and albumin improves survival in pa-tients with type 1 and type 2 hepatorenal syndrome. J ClinGastroenterol. 2009;43:680–5. https://doi.org/10.1097/MCG.0b013e318188947c.
125. Cavallin M, Kamath PS, Merli M, Fasolato S, Toniutto P, SalernoF, et al. Terlipressin plus albumin versus midodrine and octreotideplus albumin in the treatment of hepatorenal syndrome: a random-ized trial. Hepatology. 2015;62:567–74. https://doi.org/10.1002/hep.27709.
126. Rajekar H, Chawla Y. Terlipressin in hepatorenal syndrome: evi-dence for present indications. J Gastroenterol Hepatol.2011;26(suppl 1):109–14. https://doi.org/10.1111/j.1440-1746.2010.06583.x.
127. Gupta K, Rani P, Rohatgi A, Verma M, Handa S, Dalal K, et al.Noradrenaline for reverting hepatorenal syndrome: a prospective,observational, single-center study. Clin Exp Gastroenterol.2018;11:317–24. https://doi.org/10.2147/CEG.S153858.
128. Singh V, Ghosh S, Singh B, Kumar P, Sharma N, Bhalla A, et al.Noradrenaline vs. terlipressin in the treatment of hepatorenal syn-drome: a randomized study. J Hepatol. 2012;56:1293–8. https://doi.org/10.1016/j.jhep.2012.01.012.
129. Nassar Junior AP, Farias AQ, D’ Albuquerque LA, Carrilho FJ,Malbouisson LM. Terlipressin versus norepinephrine in the treat-ment of hepatorenal syndrome: a systematic review and meta-analysis. PLoS One. 2014;9:e107466. https://doi.org/10.1371/journal.pone.0107466.
130. Kiser TH, Fish DN, Obritsch MD, Jung R, MacLaren R, ParikhCR. Vasopressin, not octreotide, may be beneficial in the treatmentof hepatorenal syndrome: a retrospective study. Nephrol DialTransplant. 2005;20:1813–20. https://doi.org/10.1093/ndt/gfh930.
131. Allegretti AS, Parada XV, Eneanya ND, Gilligan H, Xu D, ZhaoS, et al. Prognosis of patients with cirrhosis and AKI who initiateRRT. Clin J Am Soc Nephrol. 2018;13:16–25. https://doi.org/10.2215/CJN.03610417.
132. Brensing KA, Textor J, Perz J, Schiedermaier P, Raab P, Strunk H,et al. Long term outcome after transjugular intrahepaticportosystemic stent-shunt in non-transplant cirrhotics withhepatorenal syndrome: a phase II study. Gut. 2000;47:288–95.https://doi.org/10.1136/gut.47.2.288.
133. Copelan A, Kapoor B, Sands M. Transjugular intrahepaticportosystemic shunt: indications, contraindications, and patientwork-up. Semin Interv Radiol. 2014;31:235–42. https://doi.org/10.1055/s-0034-1382790.
134. Rice JB, White AG, Galebach P, Korenblat KM, Wagh A,Lovelace B, et al. The burden of hepatorenal syndrome amongcommercially insured and Medicare patients in the United States.Curr Med Res Opin. 2017;33:1473–80. https://doi.org/10.1080/03007995.2017.1331211.
135. Ripoll C, Groszmann R, Garcia-Tsao G, Grace N, Burroughs A,Planas R, et al. Hepatic venous pressure gradient predicts clinicaldecompensation in patients with compensated cirrhosis.Gastroenterology. 2007;133:481–8. https://doi.org/10.1053/j.gastro.2007.05.024.
136. Zacharia GS, Rangan K, Kandiyil S, Thomas V. Spontaneousbacterial peritonitis in extrahepatic portal venous obstruction.Ann Gastroenterol. 2013;26:363–4.
137. Dever JB, Sheikh MY. Review article: spontaneous bacterial peri-tonitis—bacteriology, diagnosis, treatment, risk factors and
prevention. Aliment Pharmacol Ther. 2015;41:1116–31. https://doi.org/10.1111/apt.13172.
138. Arroyo V. Pathophysiology, diagnosis and treatment of ascites incirrhosis. Ann Hepatol. 2002;1:72–9. https://doi.org/10.1016/S1665-2681(19)32178-7.
139. Runyon BA, Morrissey RL, Hoefs JC, Wyle FA. Opsonic activityof human ascitic fluid: a potentially important protective mecha-nism against spontaneous bacterial peritonitis. Hepatology.1985;5:634–7. https://doi.org/10.1002/hep.1840050419.
140. Sheer TA, Runyon BA. Spontaneous bacterial peritonitis. Dig Dis.2005;23:39–46. https://doi.org/10.1159/000084724.
141. Runyon BA. Low-protein-concentration ascitic fluid isp red i sposed to spon taneous bac te r i a l pe r i ton i t i s .Gastroenterology. 1986;91:1343–6. https://doi.org/10.1016/0016-5085(86)90185-x.
142. Hou MC, Lin HC, Liu TT, Kuo BIT, Lee FY, Chang FY, et al.Antibiotic prophylaxis after endoscopic therapy preventsrebleeding in acute variceal hemorrhage: a randomized trial.Hepatology. 2004;39:746–53. https://doi.org/10.1002/hep.20126.
143. Deitch EA,Morrison J, Berg R, Specian RD. Effect of hemorrhag-ic shock on bacterial translocation, intestinal morphology, andintestinal permeability in conventional and antibiotic-decontaminated rats. Crit Care Med. 1990;18:529–36. https://doi.org/10.1097/00003246-199005000-00014.
144. Cadranel JF, Nousbaum JB, Bessaguet C, Nahon P, Nguyen-KhacE, Moreau R, et al. Low incidence of spontaneous bacterial peri-tonitis in asymptomatic cirrhotic outpatients. World J Hepatol.2013;5:104–8. https://doi.org/10.4254/wjh.v5.i3.104.
145. Pinzello G, Simonetti RG, Craxì A, Di Piazza S, Spanò C,Pagliaro L. Spontaneous bacterial peritonitis: a prospective inves-tigation in predominantly nonalcoholic cirrhotic patients.Hepatology. 1983;3:545–9. https://doi.org/10.1002/hep.1840030411.
146. Oey RC, de Man RA, Erler NS, Verbon A, van Buuren HR.Microbiology and antibiotic susceptibility patterns in spontaneousbacterial peritonitis: a study of two Dutch cohorts at a 10-yearinterval. United European Gastroenterol J. 2018;6:614–21.https://doi.org/10.1177/2050640617744456.
147. Titó L, Rimola A, Ginès P, Llach J, ArroyoV, Rodés J. Recurrenceof spontaneous bacterial peritonitis in cirrhosis: frequency andpredictive factors. Hepatology. 1988;8:27–31. https://doi.org/10.1002/hep.1840080107.
148. Marciano S, Dirchwolf M, Diaz JM, Bermudez C, Gutierrez-Acevedo MN, Barcán LA, et al. Spontaneous bacterial peritonitisrecurrence in patients with cirrhosis receiving secondary prophy-laxis with norfloxacin. Eur J Gastroenterol Hepatol. 2019;31:540–6. https://doi.org/10.1097/MEG.0000000000001331.
149. Nobre SR, Cabral JE, Gomes JJ, Leitão MC. In-hospital mortalityin spontaneous bacterial peritonitis: a new predictive model. Eur JGastroenterol Hepatol. 2008;20:1176–81. https://doi.org/10.1097/MEG.0b013e32830607a2.
150. Tandon P, Garcia-Tsao G. Renal dysfunction is the most importantindependent predictor of mortality in cirrhotic patients with spon-taneous bacterial peritonitis. Clin Gastroenterol Hepatol. 2011;9:260–5. https://doi.org/10.1016/j.cgh.2010.11.038.
151. Kim JJ, Tsukamoto MM, Mathur AK, Ghomri YM, Hou LA,Sheibani S, et al. Delayed paracentesis is associated with increasedin-hospital mortality in patients with spontaneous bacterial perito-nitis. Am J Gastroenterol. 2014;109:1436–42. https://doi.org/10.1038/ajg.2014.212.
152. Hung TH, Tsai CC, Hsieh YH, Tsai CC. The long-term mortalityof spontaneous bacterial peritonitis in cirrhotic patients: a 3-yearnationwide cohort study. Turk J Gastroenterol. 2015;26:159–62.https://doi.org/10.5152/tjg.2015.4829.
153. Alaniz C, Regal RE. Spontaneous bacterial peritonitis: a review oftreatment options. P T. 2009;34:204–10.
1644 SN Compr. Clin. Med. (2020) 2:1628–1645

154. Runyon BA, Canawati HN, Akriviadis EA. Optimization tech-nique of ascitic fluid culture. Gastroenterology. 1988;95:1351–5.https://doi.org/10.1016/0016-5085(88)90372-1.
155. Runyon BA, Montano AA, Akriviadis EA, Antillon MR, IrvingMA, McHutchison JG. The serum-ascites albumin gradient is su-perior to the exudate-transudate concept in the differential diagno-sis of ascites. Ann Intern Med. 1992;117:215–20. https://doi.org/10.7326/0003-4819-117-3-215.
156. Runyon BA, AASLD. Introduction to the revised AmericanAssociation for the Study of Liver Diseases Practice Guidelinemanagement of adult patients with ascites due to cirrhosis 2012.Hepatology. 2013;57:1651–3. https://doi.org/10.1002/hep.26359.
157. Wu SS, Lin OS, Chen YY, Hwang KL, Soon MS, Keeffe EB.Ascitic fluid carcinoembryonic antigen and alkaline phosphataselevels for the differentiation of primary from secondary bacterialperitonitis with intestinal perforation. J Hepatol. 2001;34:215–21.https://doi.org/10.1016/s0168-8278(00)00039-8.
158. Filippone A, Cianci R, Delli Pizzi A, et al. CT findings in acuteperitonitis: a pattern-based approach. Diagn Interv Radiol.2015;21:435–40. https://doi.org/10.5152/dir.2015.15066.
159. Runyon BA, AntillonMR, Montano AA. Effect of diuresis versustherapeutic paracentesis on ascitic fluid opsonic activity and serumcomplement. Gastroenterology. 1989;97:158–62. https://doi.org/10.1016/0016-5085(89)91430-3.
160. Arroyo V, Ginés P, Rimola A, Gaya J. Renal function abnormal-ities, prostaglandins, and effects of nonsteroidal anti-inflammatorydrugs in cirrhosis with ascites. An overview with emphasis onpathogenesis. Am J Med. 1986;81:104–22. https://doi.org/10.1016/0002-9343(86)90912-5.
161. Deshpande A, Pasupuleti V, Thota P, Pant C, Mapara S, Hassan S,et al. Acid-suppressive therapy is associated with spontaneousbacterial peritonitis in cirrhotic patients: a meta-analysis. JGastroenterol Hepatol. 2013;28:235–42. https://doi.org/10.1111/jgh.12065.
162. Terg R, Casciato P, Garbe C, Cartier M, Stieben T, Mendizabal M,et al. Proton pump inhibitor therapy does not increase the inci-dence of spontaneous bacterial peritonitis in cirrhosis: a multicen-ter prospective study. J Hepatol. 2015;62:1056–60. https://doi.org/10.1016/j.jhep.2014.11.036.
163. Rowley MW, Agarwal S, Seetharam AB, Hirsch KS. Real-timeultrasound-guided paracentesis by radiologists: near zero risk ofhemorrhage without correction of coagulopathy. J Vasc IntervRadiol. 2019;30:259–64. https://doi.org/10.1016/j.jvir.2018.11.001.
164. Ginès P, Titó L, Arroyo V, Planas R, Panés J, Viver J, et al.Randomized comparative study of therapeutic paracentesis withand without intravenous albumin in cirrhosis. Gastroenterology.1988;94:1493–502. https://doi.org/10.1016/0016-5085(88)90691-9.
165. Generali JA, Cada DJ. Ciprofloxacin: spontaneous bacterial peri-tonitis (prevention). Hosp Pharm. 2015;50:678–80. https://doi.org/10.1310/hpj5008-678.
166. Fernández J, Ruiz del Arbol L, Gómez C, et al. Norfloxacin vsceftriaxone in the prophylaxis of infections in patients with ad-vanced cirrhosis and hemorrhage. Gastroenterology. 2006;131:1049–56, quiz 1285. https://doi.org/10.1053/j.gastro.2006.07.010.
167. Ginés P, Rimola A, Planas R, et al. Norfloxacin prevents sponta-neous bacterial peritonitis recurrence in cirrhosis: results of a dou-ble-blind, placebo-controlled trial. Hepatology. 1990;12(4, pt 1):716–24. https://doi.org/10.1002/hep.1840120416.
168. Fernandez J, Acevedo J, Castro M, et al. Prevalence and riskfactors of infections by multiresistant bacteria in cirrhosis: a pro-spective study. Hepatology. 2012;55:1551–61. https://doi.org/10.1002/hep.25532.
169. Sheikhbahaei S, Abdollahi A, Hafezi-Nejad N, Zare E. Patterns ofantimicrobial resistance in the causative organisms of spontaneousbacterial peritonitis: a single centre, six-year experience of 1981samples. Int J Hepatol. 2014;2014:917856. https://doi.org/10.1155/2014/917856.
170. Runyon BA, McHutchison JG, Antillon MR, Akriviadis EA,Montano AA. Short-course versus long-course antibiotic treat-ment of spontaneous bacterial peritonitis. A randomized con-trolled study of 100 patients. Gastroenterology. 1991;100:1737–42. https://doi.org/10.1016/0016-5085(91)90677-d.
171. Mandorfer M, Bota S, Schwabl P, et al. Nonselective β blockersincrease risk for hepatorenal syndrome and death in patients withcirrhosis and spontaneous bacterial peritonitis. Gastroenterology.2014;146:1680–1690.e1. https://doi.org/10.1053/j.gastro.2014.03.005.
172. Sort P, Navasa M, Arroyo V, Aldeguer X, Planas R, Ruiz-del-Arbol L, et al. Effect of intravenous albumin on renal impairmentand mortality in patients with cirrhosis and spontaneous bacterialperitonitis. N Engl J Med. 1999;341:403–9. https://doi.org/10.1056/NEJM199908053410603.
173. Sigal SH, Stanca CM, Fernandez J, Arroyo V, Navasa M.Restricted use of albumin for spontaneous bacterial peritonitis.Gut. 2007;56:597–9. https://doi.org/10.1136/gut.2006.113050.
174. Inadomi J, Sonnenberg A. Cost-analysis of prophylactic antibi-otics in spontaneous bacterial peritonitis. Gastroenterology.1997;113:1289–94. https://doi.org/10.1053/gast.1997.v113.pm9322524.
175. Neff J, Kemmer N, Duncan C, Alsina A. Update on the manage-ment of cirrhosis—focus on cost-effective preventative strategies.Clinicoecon Outcomes Res. 2013;5:143–52. https://doi.org/10.2147/CEOR.S30675.
Publisher’s Note Springer Nature remains neutral with regard to jurisdic-tional claims in published maps and institutional affiliations.
1645SN Compr. Clin. Med. (2020) 2:1628–1645