Embed Size (px)
Citation preview

LIVERAssoc. prof. Edyta Mądry MD PhD
Poznań University of Medical SciencesDepartment of Physiology

Function of the LIVER
Liver Physiology, Larry
Frolich, Yavapai College,
March 10, 2006
Liver Brainstorm
• Perhaps least
understood, both
popularly and
scientifically?
• Brainstorm: 30 seconds
and three adjectives or
phrases
30 seconds to write
what comes out…top of
your head
Adjective/phrase 1:…….
Adjective/phrase 2:…..
Adjective/phrase 3:…..

Some answers: Liver
• the largest solid organ inside the body.
• in an adult it can weigh up to 1.4 kgs.
• It is located behind the ribs in the upper right-hand portion of the abdomen

Some answers: Liver function
• Metabolic
• Storage
• Excretory/Secretory – bile excretion
• Protective
• Circulatory – large blood storage organ
• Coagulation – production of clotting factors

Some answers: Liver
• Both a metabolic and excretory organ
• Has “double” blood supply:
hepatic artery – oxygenated blood portal vein – nutrient rich blood

Liver Physiology, Larry
Frolich, Yavapai College,
March 10, 2006
Locate your liver
• Upper right quadrant deep to inferior ribs
• Left/right lobes
• Gall bladder- thin muscular sac on inferior surface where bile collects
1. ANATOMY

In in-situ photograph of
the chest and abdominal
contents. Liver is the
largest parenchymal
organ, lying just below
the diaphragm.
The right lobe (at the left
in the photograph) is
larger than the left lobe..
1. ANATOMY

Dual blood supply to liver:
1. Hepatic portal system
• Nutrient-rich,
oxigen-poor
from gut
Liver Physiology, Larry
Fro1. ANATOMYlich, Yavapai College, March

Liver Physiology, Larry
Frolich, Yavapai College,
March 10, 2006
• Brings oxygen-rich blood
• Within liver lobules, blood mixes:– Nutrient-rich, toxin-laden,
oxygen-poor blood from
gut via- hepatic portal vein
– Oxygen-rich blood from-
hepatic artery
Dual blood supply to liver
2. Hepatic artery

Liver Physiology, Larry
Frolich, Yavapai College,
March 10, 2006
What is the TRIAD?
Triads: Branches of three vessels:
• hepatic portal vein,
• hepatic artery,
• bile drainage ductile
all run together to infiltrate all parts of liver.
3. HISTOLOGY
Liver Physiology, Larry
Frolich, Yavapai College,
March 10, 2006
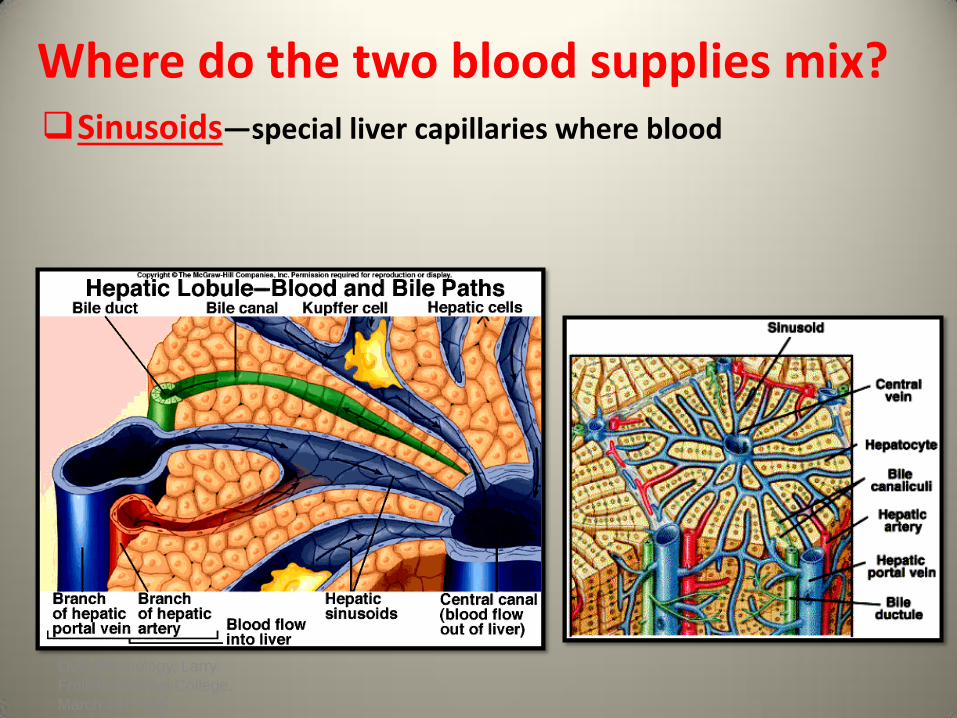
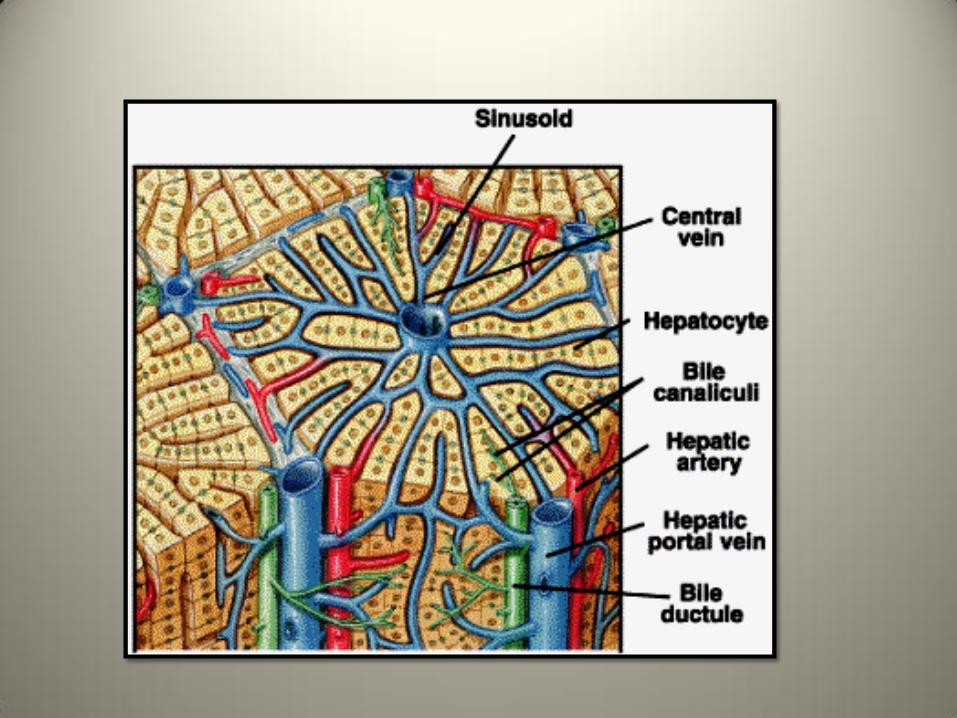
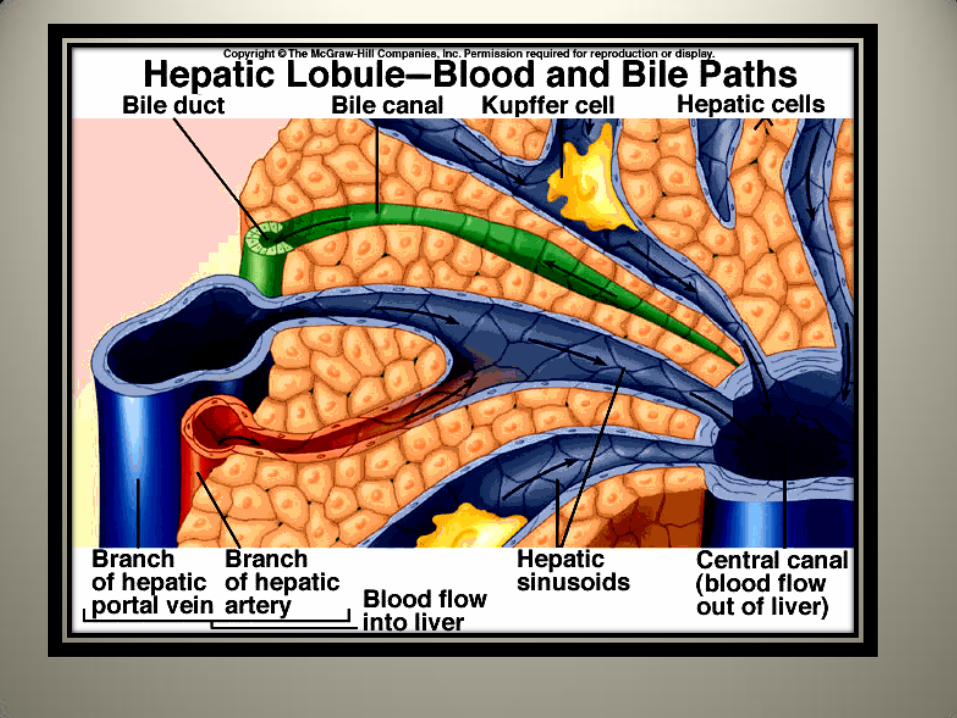
Where do the two blood supplies mix?Sinusoids—special liver capillaries where blood



Liver-Manufacturing Functions
• Protein- for the bloodstream (albumin)
• Glycogen- storage form of glucose for energy
• Bile- to help digest fats that are needed for cell structure and energy)
• Cholesterol – and special proteins to carry fat through the blood

Liver-Storage Facility
• Glycogen - released when our bodies need energy
• Iron - most is stored in the liver

Liver-Waste Disposal
• Ammonia - from the breakdown of dietary
protein and muscle tissue
• Bilirubin - from the breakdown of red blood cells
• Bacteria – removed from the bloodstream
• Drugs and Alcohol - are metabolized in the liver
Functions of the Liver: Kupffer "Cleaning System"
• The Kupffer (macrophage) cells that line the sinusoids phagocytose and digest bacteria .
• Only 1% of the bacteria entering the portal blood from the intestines will pass through the liver in viable form to enter the systemic circulation.
Metabolic Functions of the Liver
• Carbohydrate metabolism
• Gluconeogenesis
• Glycogenolysis and glycogenesis
• Hormone metabolism
• Lipid Metabolism
• Synthesis of fatty acids, cholesterol, lipoproteins
• Ketogenesis
• Drug Metabolism
• Protein Metabolism
• Synthesis of plasma proteins
• Urea synthesis

Liver Physiology, Larry
Frolich, Yavapai College,
March 10, 2006
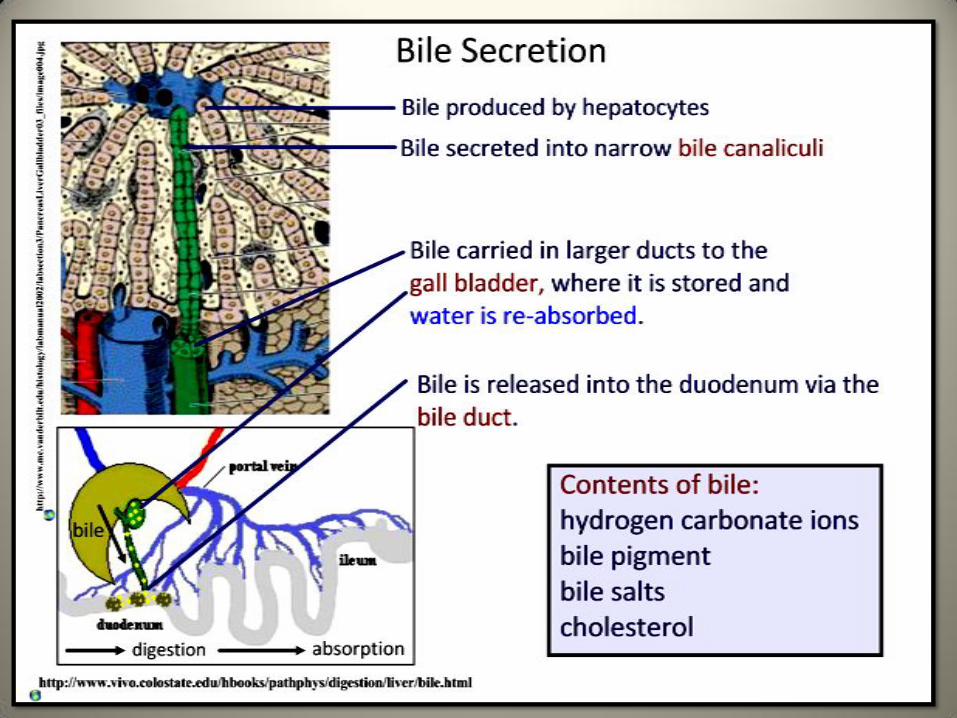
What is bile?• Bile composed of water, ions, bile acids,
organic molecules (including cholesterol, phospholipids, bilirubin)
• Gallstones are mostly cholesterol
• Acids and salts emulsify fats for absorption across wall of small intestines into lacteal lymph capillaries (review)
• Contains waste products from RBC breakdown and other metabolic processing (color of feces from bilirubin in bile)
• Ions buffer chyme from stomach

Storage and Secretion of Bile into the Intestine
• During the ingestion of a meal, vagalparasympathetic dischargesstimulate gallbladder contractions.
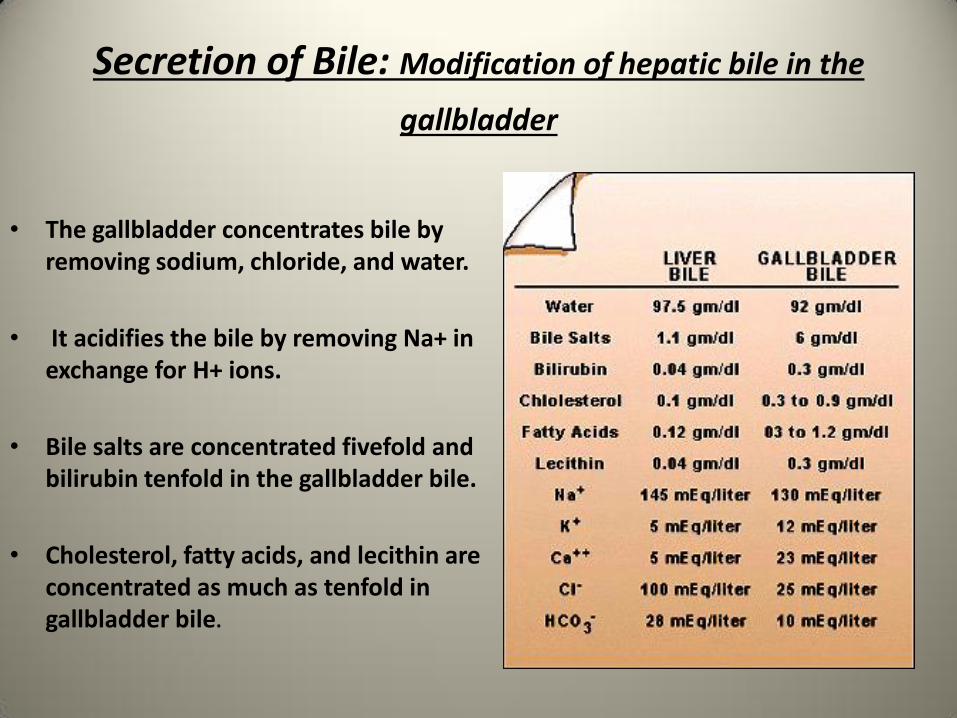
Secretion of Bile: Modification of hepatic bile in the
gallbladder
• The gallbladder concentrates bile by removing sodium, chloride, and water.
• It acidifies the bile by removing Na+ in exchange for H+ ions.
• Bile salts are concentrated fivefold and bilirubin tenfold in the gallbladder bile.
• Cholesterol, fatty acids, and lecithin are concentrated as much as tenfold in gallbladder bile.

Primary/Secondary Bile Acids
•
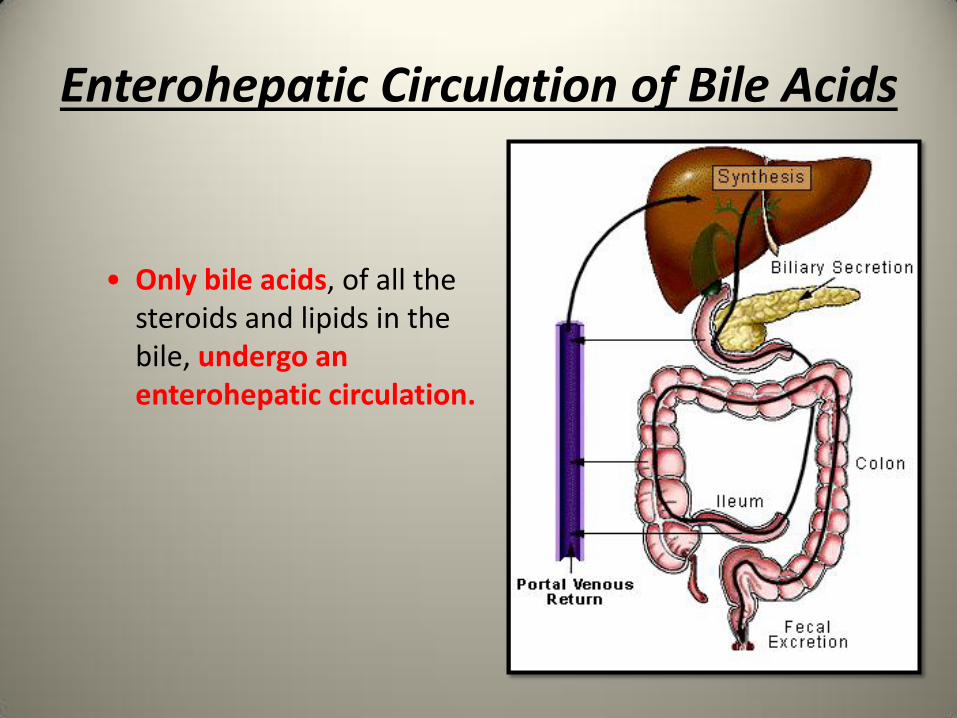
Enterohepatic Circulation of Bile Acids
• Only bile acids, of all thesteroids and lipids in thebile, undergo an enterohepatic circulation.
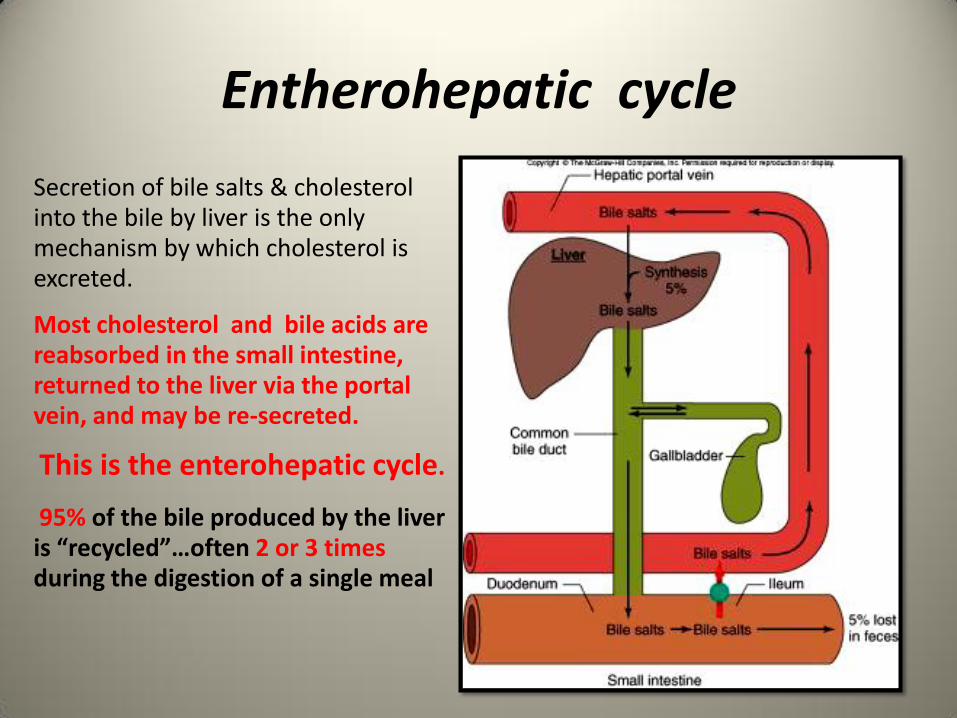
Entherohepatic cycle
Secretion of bile salts & cholesterol into the bile by liver is the only mechanism by which cholesterol is excreted.
Most cholesterol and bile acids are reabsorbed in the small intestine, returned to the liver via the portal vein, and may be re-secreted.
This is the enterohepatic cycle.
95% of the bile produced by the liver is “recycled”…often 2 or 3 times during the digestion of a single meal
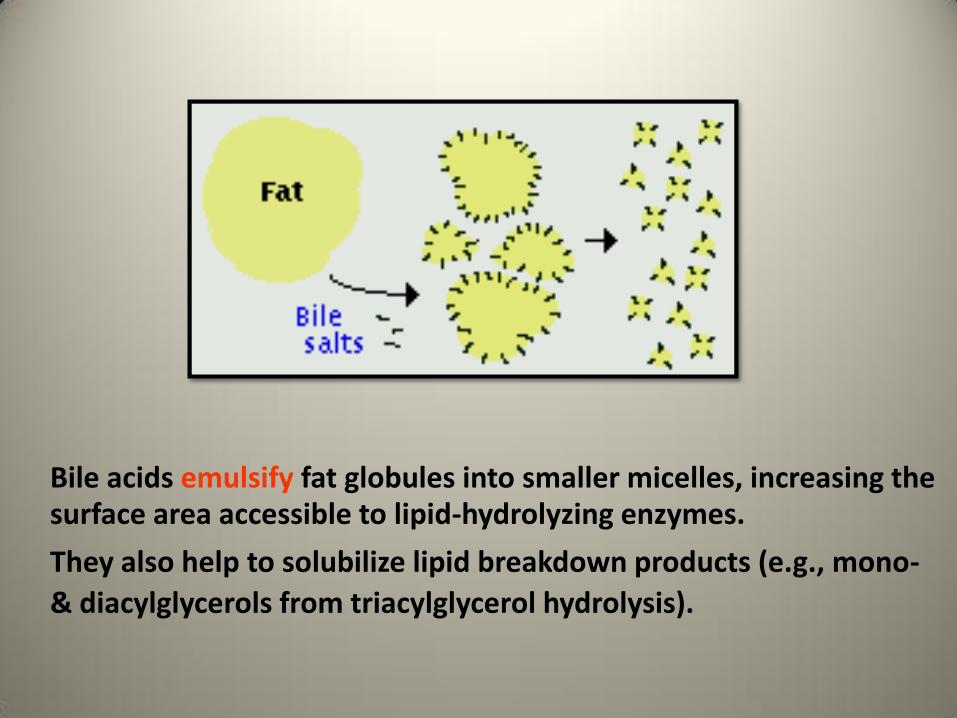
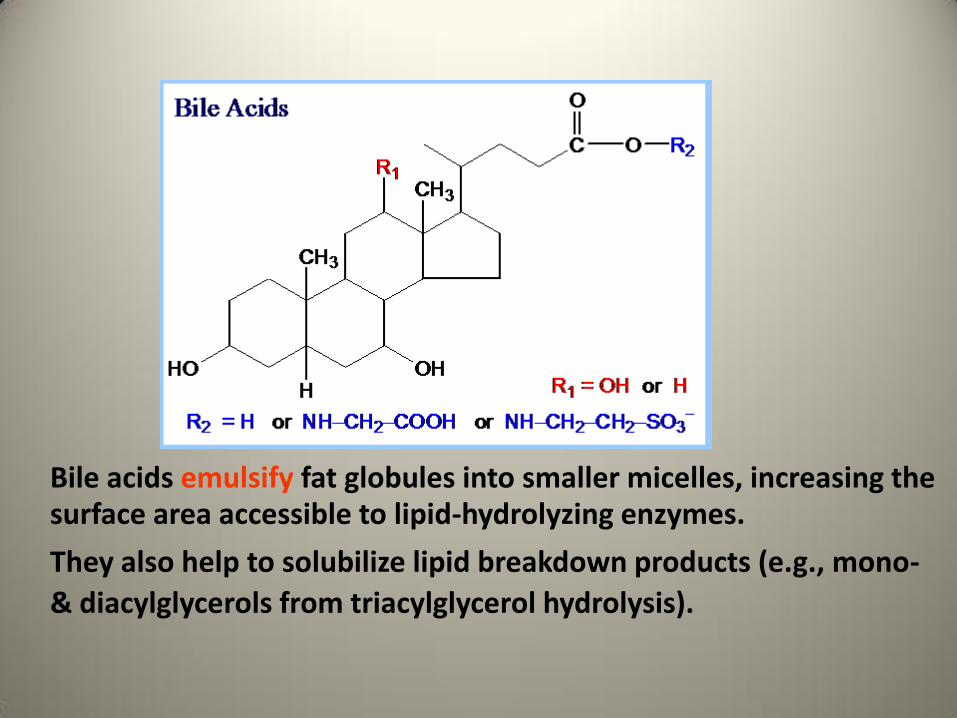
Bile acids emulsify fat globules into smaller micelles, increasing the surface area accessible to lipid-hydrolyzing enzymes.
They also help to solubilize lipid breakdown products (e.g., mono-
& diacylglycerols from triacylglycerol hydrolysis).
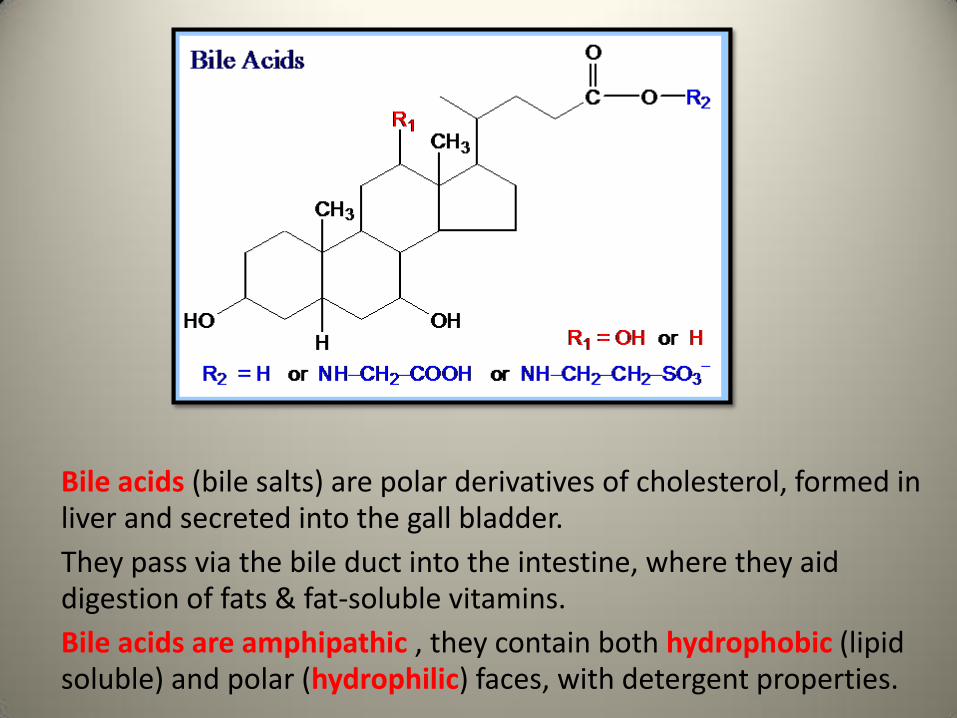
Bile acids (bile salts) are polar derivatives of cholesterol, formed in liver and secreted into the gall bladder.
They pass via the bile duct into the intestine, where they aid digestion of fats & fat-soluble vitamins.
Bile acids are amphipathic , they contain both hydrophobic (lipid soluble) and polar (hydrophilic) faces, with detergent properties.
Bile acids emulsify fat globules into smaller micelles, increasing the surface area accessible to lipid-hydrolyzing enzymes.
They also help to solubilize lipid breakdown products (e.g., mono-
& diacylglycerols from triacylglycerol hydrolysis).
Liver Physiology, Larry
Frolich, Yavapai College,
March 10, 2006
Cholesterol—one example of liver processing• Our body needs cholesterol for
– Cell membranes
– Vitamin D
– Hormones—progesterone and testosterone
– Myelin (neuron axonal “wrapping”)
– Component of bile salts
• 85% of cholesterol in our blood is “endogenous” or manufactured by our own cells (mostly liver)
• 15% comes from the food we eat
• So, is zero-cholesterol good…or even healthy?
http://www.wiley.com/college/boyer/0470003790/animations/cholesterol/cholesterol.htm
LINK to animation
Liver Physiology, Larry
Frolich, Yavapai College,
March 10, 2006
Cholesterol in the liver:Where’s it from? Where’s it go?
• Liver constantly manufactures cholesterol using acetyl-CoA as substrate
• Some cholesterol to gut via bile for emulsification of dietary fats
• Some cholesterol to blood for cell membranes, myelin, hormones, vitamins

Liver Physiology, Larry
Frolich, Yavapai College,
March 10, 2006
“Good” and “bad” cholesterol
• Two ways cholesterol is “packed”
– LDL—low density lipo-proteins (“bad”)
– HDL—high density lipo-proteins (“good”)
• LDL is component of arterial plaques that can lead to “blocked arteries”
• HDL can help to clear LDL from arterial walls

Liver Physiology, Larry
Frolich, Yavapai College,
March 10, 2006
Cholesterol in the liver:Where’s it from? Where’s it go?
• Liver constantly manufactures cholesterol using acetyl-CoA as substrate
• Some cholesterol to gut via bile for emulsification of dietary fats
• Some cholesterol to blood for cell membranes, myelin, hormones, vitamins

Liver Physiology, Larry
Frolich, Yavapai College,
March 10, 2006
“Good” and “bad” cholesterol
• Two ways cholesterol is “packed” – LDL—low density lipo-proteins (“bad”)
– HDL—high density lipo-proteins (“good”)
• LDL is component of arterial plaques that can lead to “blocked arteries”
• HDL can help to clear LDL from arterial walls
• “Packing” of cholesterol and interactions with other dietary and liver-produced fats maybe more important than cholesterol levels alone
• Trans and saturated fats (especially artificially hydrogenated fats) may be most culpable element of diet in raising LDL levels
• Mono-unsaturated fats (such as olive oil, canola oil) along with dietary fiber raise HDL levels
Liver Physiology, Larry
Frolich, Yavapai College,
March 10, 2006
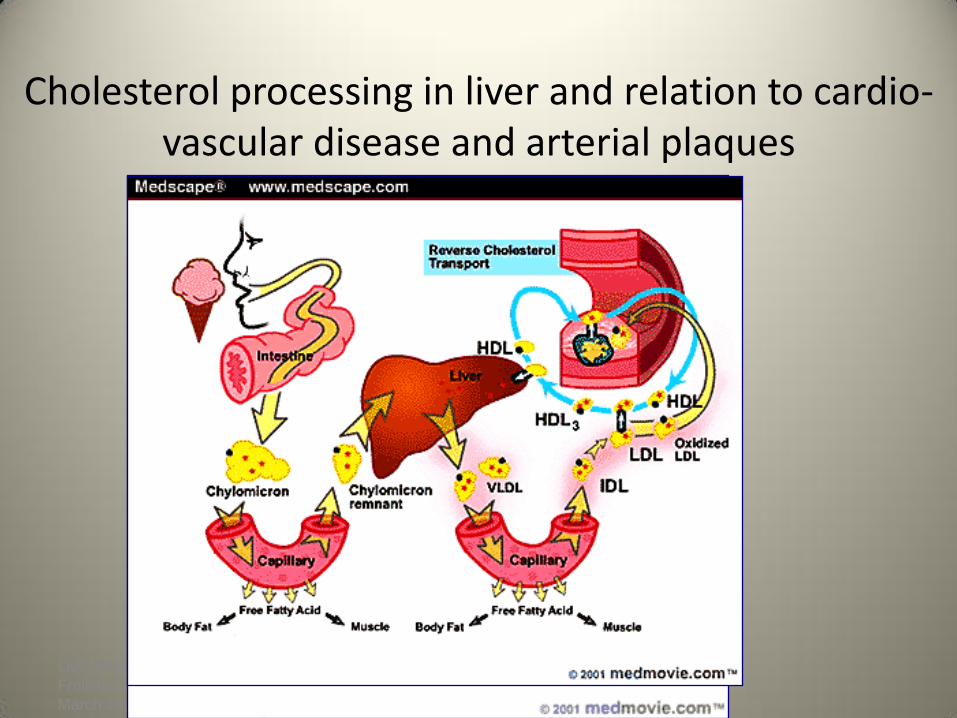
Cholesterol processing in liver and relation to cardio-vascular disease and arterial plaques

REVIEW OF LIVER FUNCTION
FUNCTIONS OF THE LIVER:Carbohydrate
metabolism Glycogenesis
Glycogenolysis
Gluconeogenesis
Fat metabolism -ketogenesis
Protein metabolism anabolism
deamination
urea formation
Secretion of bile
Detoxification
Metabolism of vitamins A,D,E,K,B
Clotting factors, espprothrombin and fibrinogen
MANIFESTATIONS OF LIVER DISORDERS
Jaundice
Hemorrhage / bleeding problems
Pruritus and itching
Ascites
Generalized Edema
Intolerance of Sedation

MANIFESTATIONS OF LIVER DISORDERS
JAUNDICECAUSES:
Prehepatic – hemolysis
Intrahepatic – liver parenchymal defect
Poshepatic – obstruction of bile ducts

MANIFESTATIONS OF LIVER DISORDERS
HEMORRHAGEDue to inadequate
prothrombin & other clotting factors
Management : Bile salts p.o.,
Vit K, p.o. & parenteral,
use of small needle with injection,
use of soft toothbrush,
check urine and stool for blood.

MANIFESTATIONS OF LIVER DISORDERS
PRURITUS & ITCHING Caused by bile pigment deposited to skin
Management:
bathing with tepid water &
use of oil-based lotion
cholestyramine – binds with bile salts and
facilitates excretion withfeces
Use soft linen
Short fingernails

MANIFESTATIONS OF LIVER DISORDERS
ASCITESCauses :
portal hypertension
decreased plasma colloid osmotic pressure
hyperaldosteronism

MANIFESTATIONS OF LIVER DISORDERS
ASCITESManagement : daily weight & abdominal girth
low Na diet, fluid restriction, diuretics
relieve symptoms from pressure of ascites :
high fowler’s
turning & positioning
IV albumin,
Paracentesis
Peritoneovenous Shunt
MANIFESTATIONS OF LIVER DISORDERS
GENERALIZED EDEMAInsufficient albumin
INTOLERANCE OF SEDATIONMost sedatives are metabolized in the liver
except phenobarbital
DISEASES OF THELIVER
• HEPATITIS
• CIRRHOSIS
• CANCER OF THE LIVER
HEPATITIS
TYPES:
• Viral Hepatitis types A, B, C
• Toxic Hepatitis – exposure to
hepatotoxin : carbon tetrachloride. Morphine, barbiturates
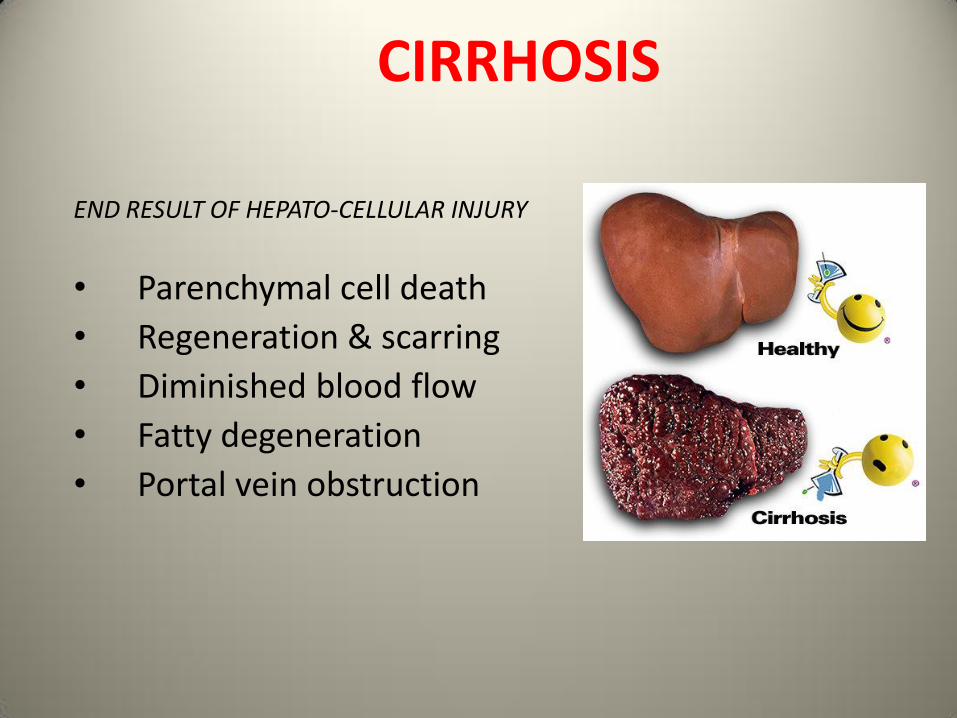
CIRRHOSIS
END RESULT OF HEPATO-CELLULAR INJURY
• Parenchymal cell death
• Regeneration & scarring
• Diminished blood flow
• Fatty degeneration
• Portal vein obstruction

One of the most
common findings with
portal hypertension is
splenomegaly.
HEPATIC COMADEGENERATIVE DISEASE OF THE BRAIN FROM LIVER FAILURE
DUE TO INABILITY OF THE LIVER TO CONVERT AMMONIA TO UREA
• CHANGES IN PERSONALITY AND BEHAVIOR
• LETHARGY
• CONFUSION
• TREMORS
• STUPOR
• DIZZINESS
• COMA
• FETOR HEPATICUS – FRUITY ODOR BREATH
• SPIDER TELANGIECTASIA
• ELEVATED SERUM AMMONIA LEVELS

LIVER FUNCTION TESTS
http://crisbertcualteros.page.tl
Liver tests- what for to do them?
1. to detect the presence of liver diseases
2. to distinguish among the different types of liver diseases
3. to follow response to treatment

TESTS BASED ON DETOXIFICATIONS
AND EXCRETORY FUNCTIONS OF LIVER:
1. SERUM BILIRUBIN – a breakdown product of porphyrin ring of heme containing proteins
(conjugated,unconjugated)
unconjugated/indirect – insouble in water; bound to albumin in the blood
conjugated/direct – water soluble; excreted in kidneys

Normal serum bilirubin concentration:
<17 micromol/L (1mg/dl)
Up to 30% of the total is direct-reacting

2. URINE BILIRUBIN:
presence of bilirubinuria liver diseases almost 100% accurate
3. BLOOD AMMONIA: elevated in advanced liver diseases with significant muscle wasting Hyperammonimea
There is a poor correlation between either the presence or the degree of acute enceph and elevation of blood ammonia
There is a poor correlation of the blood serum ammonia and hepatic function

4. SERUM ENZYMES
2 categories of serum enzymes:
Enzymes whose elevation in serum reflects
damage to hepatocytes
Enzymes whose elevation in serum reflect
cholestasis
Enzymes that do not fit precisely into either
patterns
ENZYMES THAT REFLECT DAMAGE TO HEPATOCYTES
AMINOTRANSFERASES:
sensitive indicator of liver cell injury and most helpful in recognizing acute hepatocellular diseases such as hepatitis
SERUM ENZYMES- aminotransferases
AST (Aspartate aminotransferase): liver,
cardiac, skeletal, kidneys, brain, pancreas, lungs,
leukocytes and erythrocytes
ALT (Alanine aminotransferase): found primarily
in the liver

ENZYMES THAT REFLECT CHOLESTASIS
• Alkaline phosphatase and 5’ nuleotidase: found near the bile canalicular membrane of hepatocytes
• Gamma Glutamyl Transpeptidase: Endoplasmic reticulum and in bile duct epithelial cells lacks specificity

Alkaline phosphatase: liver, bone, placenta, less
commonly small intestine

TESTS THAT MEASURE BIOSYNTHETIC
FUNCTION OF THE LIVER
SERUM ALBUMIN: synthesized exclusively by
hepatocytes
* has a slow turn over
not a good indicator of acute or mild hepatic dysfunction

• SERUM GLOBULINS: alpha and beta
globulins produced primarily in hepatocytes
• gamma globulins (immunoglobulins) produced
by B lymphocytes.
COAGULATION FACTORS:
With the exception of Factor VIII, the blood
clotting factors are made exclusively in
hepatocytes.
Because of their rapid turnover, measurement of
the clotting factors is the single best acute
measure of hepatic synthetic function and
helpful in both the diagnosis and assessing the
prognosis of acute parenchymal liver disease

• Thank you for commingand your attention
Recommended to see
• Liver anatomy and functionhttps://www.youtube.com/watch?v=P5_BxsbmXcA
• Liver Structure and the Flow of Blood and Bile https://www.youtube.com/watch?v=O71niTozP-o





























