Embed Size (px)
Citation preview

1
PowerPoint Slides English Brazilian Portuguese Translation
The Role of Surgery in Inflammatory Breast Cancer Patients Video Transcript
O Papel da Cirurgia em Pacientes com Carcinoma Inflamatório de Mama Transcrição de vídeo
Professional Oncology Education The Role of Surgery in Inflammatory Breast Cancer Patients Time: 22:38
Educação Profissional em Oncologia O Papel da Cirurgia em Pacientes com Carcinoma Inflamatório de Mama Duração: 22:38
Anthony Lucci, M.D., F.A.C.S. Professor of Surgery Department of Surgical Oncology The University of Texas MD Anderson Cancer Center
Dr. Anthony Lucci, M.D., F.A.C.S. Professor de Cirurgia Departamento de Oncologia Cirúrgica MD Anderson Cancer Center – Universidade do Texas
Hi, I’m Dr. Anthony Lucci from the University of Texas MD Anderson Cancer Center in Houston. And today, I’d like to talk to you about the role of surgery in inflammatory breast cancer patients.
Olá, eu sou o Dr. Anthony Lucci do MD Anderson Cancer Center da Universidade, do Texas, em Houston. Hoje gostaria de conversar com vocês sobre o papel da cirurgia em pacientes com carcinoma inflamatório de mama.
So, there’s a few learning objectives we will try to complete. And, the first one will be to determine the optimal timing and indications for surgery in the multimodal treatment of patients with inflammatory breast cancer which, throughout the talk, you’ll see abbreviated as IBC, capital IBC. We’ll also discuss optimal surgical treatments for the breast and regional lymph nodes in patients with IBC. And, we’ll identify the reconstructive and rehabilitative issues that occur after surgery in patients with IBC.
Há alguns objetivos de aprendizagem que procuraremos atingir. O primeiro será determinar o tempo e as indicações ideais para a cirurgia no tratamento multimodal de pacientes com carcinoma inflamatório de mama que, durante a palestra, vocês verão abreviado como CIM, CIM em caixa alta. Também discutiremos os tratamentos cirúrgicos ideais para a mama e linfonodos regionais em pacientes com CIM e identificaremos os problemas de reconstrução e reabilitação pós-operatórios em pacientes com CIM.
2
So, how’s IBC different from regular breast cancer? I mean, we all know about regular breast cancer, but how is IBC different? Well, inflammatory breast cancer has early dissemination, a higher recurrence rate, and still has a 50 percent mortality rate. So, even now, with improved treatments, patients still have about a 50 percent mortality rate with this disease.
Então, qual a diferença entre o CIM e o câncer de mama comum? Isto é, todos conhecemos o câncer de mama comum, mas em que se diferencia o CIM? Bem, o câncer inflamatório de mama apresenta disseminação precoce, maior índice de reincidência e, ainda, tem uma taxa de mortalidade de 50%. Então, mesmo agora, com melhores tratamentos, pacientes portadores desta doença apresentam uma taxa de mortalidade de 50%.
Now, treatment planning in IBC is really a key to success. And, so, in general, the protocol is pretty simple. Almost all patients with inflammatory breast cancer need as their primary therapy, neoadjuvant chemotherapy. And, then, if the patient has a response, meaning if the tumor responds and shrinks either partially or completely, then it’s been shown that that patient would benefit from local therapy, such as surgery. Now, breast-conserving therapy as a surgery option for breast cancer is well accepted. But, in inflammatory breast cancer, it’s not optimal, simply due to the involvement of the skin and surrounding structures, and the dermal lymphatic invasion with the tumor. So, breast conservation is not an optimal treatment option for inflammatory breast cancer and should not be offered to patients with IBC. As far as lymph nodes management, we know about sentinel node biopsies as another real great option for patients with operable stage I to III breast cancer. But, not for inflammatory breast cancer because there are several studies that have shown a high false-negative rate in patients with inflammatory breast cancer. So, generally, these patients will need an axillary dissection. And, then, following the surgical therapy, post-mastectomy radiation in the standard four fields is given, and that’s the optimal treatment modality currently for
O planejamento terapêutico do CIM é a chave para o sucesso. Em geral, o protocolo é muito simples. Quase todas as pacientes com carcinoma inflamatório de mama precisam receber quimioterapia neoadjuvante como terapia primária. Foi demonstrado que, se a paciente apresentar uma resposta, significando se o tumor responder e encolher, seja parcial ou completamente, ela se beneficiaria com uma terapia local, como a cirurgia. As terapias que preservam a mama como opção cirúrgica para o câncer de mama são bem aceitas. Mas, no carcinoma inflamatório de mama a cirurgia não é o ideal, simplesmente por causa do comprometimento da pele e estruturas adjacentes e da invasão dos vasos linfáticos da derme pelo tumor. Então, a preservação da mama não é uma opção ideal no carcinoma inflamatório de mama e não deve ser oferecida a pacientes com CIM. Quanto ao manejo de linfonodos, sabemos de biópsias de linfonodos sentinelas como sendo outra excelente opção para pacientes com câncer de mama em estágio I a III operável. Mas, não para o carcinoma inflamatório de mama, porque há vários estudos que demonstraram um alto índice de falsos-negativos em pacientes com esta doença. Geralmente, essas pacientes precisarão de uma linfadenectomia axilar. Após a terapia cirúrgica, é administrada a irradiação pós-mastectomia com
3
inflammatory breast cancer, the one that offers the best outcomes.
quatro campos padronizados, e essa é atualmente a modalidade ideal de tratamento do carcinoma inflamatório de mama, a que oferece os melhores resultados.
Now, why even do surgery? Is surgery really going to help? Well, surgery is important because you can achieve local control in the majority of patients if you perform a mastectomy. However, we said before that surgery would not be perhaps indicated in all patients suspending --- depending on the response to therapy, and we’ll talk a little bit more about that in a minute. Also, surgery allows for pathologic staging after neoadjuvant chemotherapy because there will be some patients that have a --- what appears to be a complete clinical response. But, we will find residual disease at pathologic evaluation of the mastectomy specimen and perhaps give better prognostic information and maybe even indications for additional therapy. And, finally, surgery has been a component of multimodal therapy that has been shown by several studies. And, you can see the references in the bottom right corner of the slide that offer improved disease-free and overall survival after a response to neoadjuvant chemotherapy. So, surgery is an important modality to --- for the overall protocol of --- of what we talked about of the trimodal therapy – neoadjuvant chemotherapy, surgery, and then radiation post-mastectomy to give the best outcome.
Mas, para que fazer cirurgia? A cirurgia ajuda mesmo? Bem, a cirurgia é importante porque, com a mastectomia podemos conseguir um controle local na maioria das pacientes. No entanto, já dissemos que a cirurgia talvez não fosse indicada para todas as pacientes, pois depende da resposta à terapia, e falaremos um pouco mais sobre isso num minuto. Além disso, a cirurgia permite o estadiamento patológico após a quimioterapia neoadjuvante, porque haverá pacientes que parecem ter uma resposta clínica completa. Mas, descobriremos doença residual na avaliação patológica de espécimes de mastectomias e, talvez, possamos oferecer melhores informações prognósticas e até, talvez, indicações para outras terapias. E, finalmente, a cirurgia tem sido um componente da terapia multimodal demonstrada por vários estudos. Vocês podem observar as referências no canto direito inferior do slide que oferecem melhorias quanto à ausência de doença e sobrevida global após resposta à quimioterapia neoadjuvante. Então, a cirurgia é uma modalidade importante para o protocolo global de que falamos a respeito da terapia trimodal – quimioterapia neoadjuvante, cirurgia e, depois, irradiação pós-mastectomia para conseguir o melhor resultado.

4
So, we already talked about --- a little bit about selection, but the best selection criteria are patients who response to chemotherapy are offered modified radical mastectomy. And, what we mean by response is a partial or a complete response to the chemotherapy, a clinical partial or complete response.
Já falamos um pouco sobre seleção, mas os melhores critérios de seleção são pacientes que respondem a quimioterapia, e a elas é oferecida a mastectomia radical modificada. Por resposta queremos dizer uma resposta parcial ou completa à quimioterapia, uma resposta clínica parcial ou completa.
Now, one thing I’d like to point out is that historically mastectomy alone for inflammatory breast cancer is a terrible option. And, if you look at the reason why, surgery alone, this is outcome --- this slide shows outcome after mastectomy alone for inflammatory breast cancer. And, we can see that in general, the outcomes are dismal. So, when you see here, mean survival in months, after mastectomy only, the numbers are quite low. In fact, the total or the medians are right --- somewhere around 22 months. So, surgery as a as a --- as a single modality therapy is not successful and is not recommended.
Algo que gostaria de salientar é que, historicamente, a mastectomia sozinha para o carcinoma inflamatório de mama é uma péssima opção. Se observarem a razão disso, a cirurgia isoladamente, este é o resultado – o slide mostra o resultado depois da mastectomia sozinha no carcinoma inflamatório de mama. Podemos ver que, em geral, os resultados são desanimadores. Então, se observarem aqui, os valores médios de sobrevida, em meses, são bastante baixos depois de realizar só a mastectomia. Aliás, o total ou as medianas estão mais ou menos ao redor de 22 meses. Então, cirurgia como terapia de modalidade única não é bem-sucedida e não é recomendada.

5
Now, one thing surgery is good for in part --- as part of a combined therapy, is for providing local control of the disease. And, here we see that when you look at local regional recurrence after combined modality therapy, again, systemic chemotherapy followed by mastectomy, followed by post-mastectomy radiation, we have local regional recurrences somewhere around 20 percent. So, gr--- I think that’s great that in 80 percent of the patients, we can control the local disease with --- with the use of surgery. So, again, this is why surgery is an important component of the treatment of patients with IBC.
Agora, como parte de uma terapia de combinação, a cirurgia é boa porque permite o controle local da doença. E, se observarmos aqui, a reincidência locorregional depois de uma terapia de modalidade combinada − novamente, quimioterapia sistemática seguida de mastectomia, seguida de irradiação pós-mastectomia −, as reincidências locorregionais ficam mais ou menos ao redor de 20 por cento. Acho ótimo que em 80% das pacientes possamos controlar a doença local com cirurgia. Então, novamente, é por isso que a cirurgia é um componente importante no tratamento de pacientes com CIM.
So, how is the surgeon important in diagnosis? Well, we have to remember that in general, patients with inflammatory breast cancer will be often younger aged than those with locally advanced breast cancer. Now, that’s not all, but that’s a trend. Also, we have to remember that the surgeon has a role in rec --- recognizing the signs of IBC – erythema, edema, which again can cause the peau d’orange, the characteristic peau d’orange from the enlargement of the hair follicle pits. And, we’ll see some pictures of that in just a second, for a better demonstration. Also, wheals or ridges in the skin of the breast, and then usually, that rapid progression of redness covering at least a third or more of the breast would be criteria --- diagnostic criteria for inflammatory breast cancer.
Então, qual a importância do cirurgião no diagnóstico? Temos que lembrar que, em geral, as pacientes com carcinoma inflamatório de mama são mais jovens do que aquelas com câncer de mama localmente avançado. Isso não é tudo, mas é uma tendência. Também, temos que lembrar que o cirurgião cumpre um papel em reconhecer os sinais do CIM – eritema, edema, que também pode gerar o peau d'orange, o aspecto de casca de laranja característico do aumento dos folículos pilosos. Veremos algumas imagens disso em um segundo para exemplificar melhor. Além disso, [a presença de] vergões ou rugas na pele da mama e, geralmente, a rápida progressão da vermelhidão que se estende pelo menos em uma terça parte ou mais da superfície da mama seriam critérios diagnósticos para carcinoma inflamatório da mama.
6
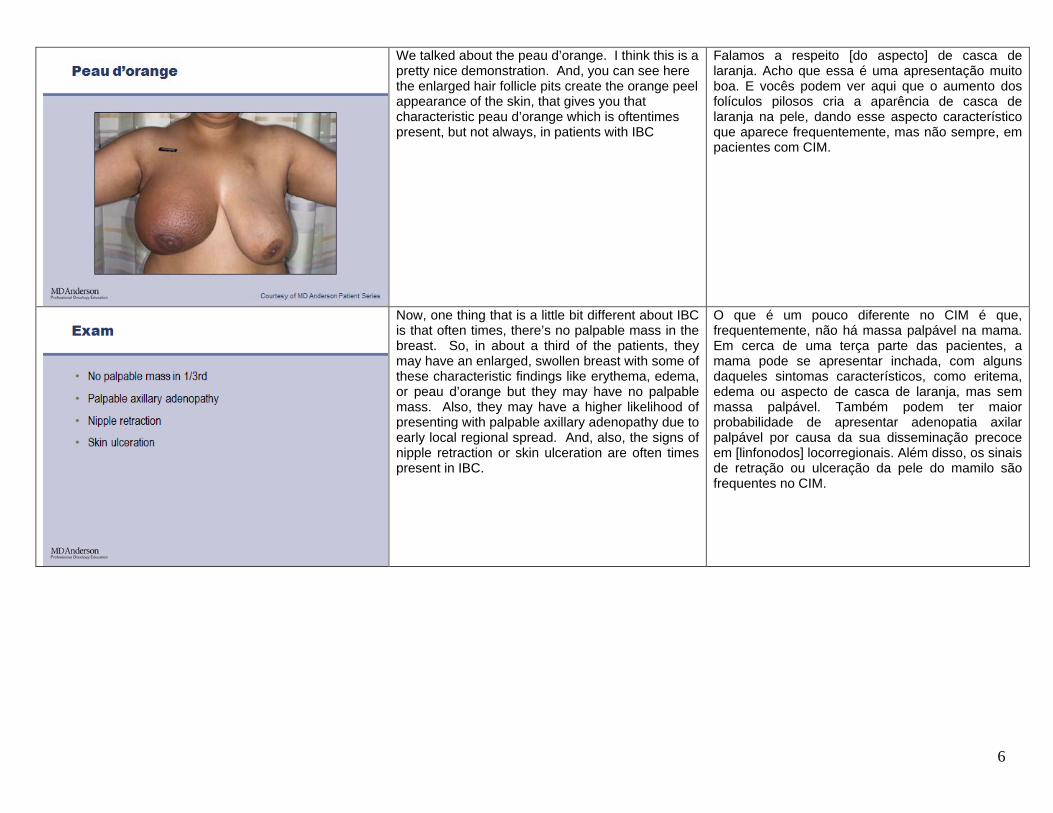
We talked about the peau d’orange. I think this is a pretty nice demonstration. And, you can see here the enlarged hair follicle pits create the orange peel appearance of the skin, that gives you that characteristic peau d’orange which is oftentimes present, but not always, in patients with IBC
Falamos a respeito [do aspecto] de casca de laranja. Acho que essa é uma apresentação muito boa. E vocês podem ver aqui que o aumento dos folículos pilosos cria a aparência de casca de laranja na pele, dando esse aspecto característico que aparece frequentemente, mas não sempre, em pacientes com CIM.
Now, one thing that is a little bit different about IBC is that often times, there’s no palpable mass in the breast. So, in about a third of the patients, they may have an enlarged, swollen breast with some of these characteristic findings like erythema, edema, or peau d’orange but they may have no palpable mass. Also, they may have a higher likelihood of presenting with palpable axillary adenopathy due to early local regional spread. And, also, the signs of nipple retraction or skin ulceration are often times present in IBC.
O que é um pouco diferente no CIM é que, frequentemente, não há massa palpável na mama. Em cerca de uma terça parte das pacientes, a mama pode se apresentar inchada, com alguns daqueles sintomas característicos, como eritema, edema ou aspecto de casca de laranja, mas sem massa palpável. Também podem ter maior probabilidade de apresentar adenopatia axilar palpável por causa da sua disseminação precoce em [linfonodos] locorregionais. Além disso, os sinais de retração ou ulceração da pele do mamilo são frequentes no CIM.

7
So, here’s again some pictures which I think will give us a much better idea of what we’re talking about. Here, we see ulceration of the skin with breast tissue. We see widespread edema and swelling. And, I think, again, this would be hard to --- to misdiagnose because it’s a fairly pronounced case. But, I think it does give a clear picture of what we’re talking about with IBC, with its rapid progression and pronounced findings.
Aqui temos, novamente, algumas ilustrações que, acredito, oferecem uma ideia muito melhor do que estamos falando. Aqui, vemos a ulceração da pele com tecido mamário. Vemos edema generalizado. E, de novo, acredito que seria difícil de emitir um diagnóstico equivocado porque é um caso bastante pronunciado. Mas, acredito que oferece um quadro claro do que viemos falando sobre o CIM, com sua progressão rápida e resultados pronunciados.
Here’s a little bit more subtle with the redness covering around the nipple areolar complex, the swelling and, again, in this patient, there was no palpable mass. It was simply an enlargement of the entire breast. And, oftentimes what happens is these cases are misdiagnosed as infection. And, the patients are treated long-term with antibiotics. So, it’s important for the surgeon and any clinician to really be aware of the fact that you can never let that diagnosis be out of your differential. IBC has always got to be considered when you see redness over a significant portion of the breast and any of those other characteristic findings.
Aqui é um pouco mais sutil, com vermelhidão cobrindo a área que circunda o complexo areolar do mamilo, o edema e, novamente, nesta paciente não havia massa palpável. Simplesmente, houve o aumento de toda a mama. O que acontece com frequência nesses casos é serem diagnosticadas equivocadamente como infecção. E as pacientes recebem tratamento com antibióticos em longo prazo. É importante para o cirurgião e todo clínico estar bem ciente do fato de que não podem jamais descartar a possibilidade desse diagnóstico diferencial. O CIM sempre deve ser considerado quando for observada vermelhidão sobre uma porção significativa da mama e qualquer um daqueles sintomas característicos.

8
Again, here’s the wheals and ridges we talked about, very obvious, almost looking like the spokes of a wheel coming out in the breast. Very clear demonstration of how IBC can cause this ridging. And, then you see the characteristic redness that’s covering a significant portion of the breast. Again, very pathognomonic, or I should say very characteristic of IBC.
Outra vez, aqui estão os vergões e rugas aos quais nos referimos, bem evidentes, quase se parecendo com os raios de uma roda saindo da mama. Exemplo muito claro de como o CIM causa essas rugas. Depois, vocês veem a vermelhidão característica que cobre uma porção significativa da mama. Outra vez, muito patognomônico, ou talvez deva dizer muito característico do CIM.
Again, more subtle, but in this patient, the patient presented initially with swelling and edema, had core biopsy, I should say core biopsies of the breast tissue which showed invasive carcinoma. And, then had punch biopsies of the skin which showed dermal lymphatic invasion tumor emboli characteristic of IBC. And, then, this patient has been treated and now has significant reduction of the redness that was present.
Outra vez, mais sutil, mas esta paciente inicialmente apresentou edema, foi submetida à biópsia por punção com agulha grossa, devo dizer biópsias por punção com agulha grossa, em que foi observado carcinoma invasivo. Depois, foi submetida a biópsias cutâneas realizadas com punch, nas que foram observados êmbolos tumorais em vasos linfáticos da derme, característicos do CIM. Depois, a paciente recebeu tratamento e, agora, a extensão da vermelhidão anterior foi reduzida significativamente.
9
So, we just talked a little bit about diagnostic techniques, such as punch biopsies. So, let’s talk about when those may be helpful. First of all, though, I’ll talk about imaging. Because obviously that’s the first step with any patient with breast cancer is they’re going have imaging of the breast. One thing to remember in inflammatory breast cancer is that many times, the imaging may be negative or difficult to interpret due to the level of edema and swelling of the breast. And, you can have patients where there’s no clear mass within the breast but they could still have inflammatory breast cancer that’s invading into the skin. It just may not show a clear mass in the breast. And, then, the thickening is often times noted as a finding on either the mammogram, the ultrasound, or even on CTs or MRIs. Core biopsy is still the best diagnostic modality. There’s really no role for incisional biopsy. There’s no role for incisional biopsy in --- in early breast cancer in any case. I think nowadays, it --- it really has to be a core biopsy or it may --- perhaps even an FNA if you’re talking about of the lymph nodes. But, open biopsy just really doesn’t have a role. It’s very limited. There’ll be rare cases where you would need that. Punch biopsy, we talked about punch biopsy of the skin. Punch biopsy of the skin can be used in cases where there’s not a clear diagnosis and you may see dermal lymphatic tumor emboli in up to 72 percent of patients. But, remember, it’s not required for diagnosis. So, there may be cases where you don’t see that in the skin, but there’s redness covering a significant portion of the skin. You have edema, you have a core biopsy showing invasive carcinoma, that can still be a diagnosis of inflammatory breast cancer. You do not have to have dermal lymphatic tumor emboli, and I think that’s an important point.
Acabamos de falar um pouco sobre técnicas diagnósticas, como as biópsias com punch. Falemos sobre quando elas podem ser úteis. Mas, primeiro, falarei sobre imaginologia. Porque, evidentemente, é o primeiro passo para pacientes com câncer de mama: serem submetidas a exames da mama por imaginologia. Algo que devemos lembrar no carcinoma inflamatório de mama é que, muitas vezes, [os resultados] das imagens podem ser negativos ou difíceis de interpretar por causa do grau de edema da mama. E pode haver pacientes sem massa evidente na mama e, mesmo assim, apresentar carcinoma inflamatório de mama que invade a pele. Só que a massa na mama pode não ser evidente. Também, o espessamento é observado frequentemente como um sinal na mamografia, ecografia ou mesmo em tomografias computadorizadas ou ressonâncias magnéticas. A biópsia por punção com agulha grossa é ainda a melhor modalidade diagnóstica. Na verdade, não há nenhum papel para a biópsia incisional. Não há nenhum papel para a biópsia incisional em câncer de mama precoce em nenhuma circunstância. Atualmente, acredito que tem que ser uma biópsia por punção com agulha grossa ou, talvez, mesmo uma punção aspirativa com agulha fina caso se trate de linfonodos. Mas, a biópsia aberta não cumpre nenhum papel mesmo. É muito limitada. Raramente precisariam dela. A biópsia com punch, já falamos a respeito da biópsia cutânea com punch. A biópsia cutânea com punch pode ser utilizada em casos onde não houver um diagnóstico claro e estiverem presentes êmbolos tumorais em vasos linfáticos na derme de até 72% das pacientes. Mas, lembrem que não é obrigatório para o diagnóstico. Pode haver casos em que não vemos isso na pele, mas sim uma vermelhidão que cobre uma porção significativa da pele. Constatamos o edema e contamos com os resultados de uma biópsia por punção com agulha grossa que demonstra a presença de carcinoma invasivo; mas isso ainda pode ser um diagnóstico de carcinoma inflamatório de mama. Não há necessidade de haver êmbolos tumorais em vasos linfáticos da derme. Para mim, isso é um ponto

10
importante.
We already talked about this. Excisional or incisional biopsy is just a terrible idea, and it’s rarely necessary. And we’ll see why in a little bit, it can actually be detrimental to the patient.
Já falamos sobre isto. A biópsia excisional ou incisional é apenas uma péssima ideia e raramente necessária. E dentro de pouco veremos por quê. De fato, pode ser prejudicial à paciente.
So, here’s a --- a patient who was seen at an outside institution, underwent an excisional biopsy, and here’s one of the problems with IBC. It’s a disease that’s often involving the skin extensively. And, many times, these excisional biopsies don’t heal and they can become open wounds that will delay the further treatment of the patient.
Temos aqui uma paciente que foi examinada numa instituição externa, foi submetida a uma biópsia excisional e eis aqui um dos problemas com o CIM. É uma doença que muitas vezes acomete a pele extensivamente. E, muitas vezes, as biópsias excisionais não curam e podem se tornar feridas abertas que atrasam o tratamento posterior da paciente.

11
Again, this patient was found to have bilateral inflammatory breast cancer, underwent an excisional biopsy unnecessarily on both sides. The one on the left side here actually didn’t heal and opened up, and delayed, again, the treatment of the patient.
Novamente, foi observado que esta paciente apresentava carcinoma inflamatório bilateral de mama e foi submetida a uma biópsia excisional em ambos os lados sem necessidade. A do lado esquerdo, aqui, não curou e se abriu, atrasando, novamente, o tratamento da paciente.
Now, what about staging? So, at --- with inflammatory breast cancer, it’s important to note that up to 30 percent of the patients can already have metastatic disease at the time of diagnosis, which is higher than your run of the mill breast can --- invasive breast cancer. So, traditionally, chest x-ray or bone scans, and in some cases, even PET scans or CT scans or PET/CTs combined can be used for imaging up front. I’ll say there’s no obvious, you know, right treatment protocol. Here, we tend to use PET/CT not only as a diagnostic, but, also, as a research tool to see if we can identify patients with disease up front. But, it is an option to use for patients with inflammatory. I would say, however, that PET/CT is generally not a good idea for staging patients with non-inflammatory early stage breast cancer. It would be not necessary in the majority of cases.
E o que dizer sobre o estadiamento? No carcinoma inflamatório de mama é importante observar que até 30% das pacientes já podem apresentar metástase no momento do diagnóstico, que é mais elevada do que a de câncer de mama invasivo comum. Tradicionalmente, a radiografia torácica ou a cintilografia óssea, e em alguns casos, mesmo TEPs ou TCs ou TEPs/TCs combinadas podem ser utilizadas como imaginologia antecipada. Eu diria que não existe um protocolo terapêutico óbvio, certo. Aqui há uma tendência a utilizar a TEP/TC não só como diagnóstico, mas como ferramenta de pesquisa para ver se podemos identificar pacientes com doença precoce. Mas, é uma opção para utilizar em pacientes com carcinoma inflamatório. No entanto, eu diria que, em geral, a TEP/TC não é uma boa ideia para estadiar pacientes com carcinoma não inflamatório de mama em estágio precoce. Não seria necessário na maioria dos casos.

12
The other reason why staging is important is IBC is more likely to recur in the soft tissue. We also have looked at research studies here, looking at circulating tumor cells in the blood and disseminated tumor cells in the bone marrow, and that research is ongoing now, to try to see if we can identify patients at additional risk who are already spreading disease hematogenously, through the bloodstream, and may give us some insight in the future as to why this disease spreads rapidly to other areas.
A outra razão de o estadiamento ser importante é que o CIM tem maior probabilidade de recidiva em tecidos moles. Também vimos estudos de pesquisa aqui que estudaram células neoplásicas circulantes no sangue e células neoplásicas disseminadas na medula óssea – e essa pesquisa está em andamento – para procurar identificar pacientes em risco adicional que já disseminam a doença do ponto de vista hematogênico pela corrente sanguínea e pode nos dar algumas ideias no futuro quanto à razão de esta doença se espalhar rapidamente a outras áreas.
So, again, we talked about the role of the surgeon. The first thing is to recognize that it’s inflammatory cancer. Keep that in mind. Don’t always consider that it’s an abscess. If you think it’s an abscess or breast mastitis, you could treat with one course of antibiotics and watch closely. But, if it doesn’t get better, I think right away, you have to start thinking about is this something else. And, hopefully there’s already been imaging obtained, and if the imaging shows a mass, then directed biopsy with core needle and perhaps, even like we said, punch biopsy of the skin may be necessary. Once the diagnosis is made, the patient needs to be referred for neoadjuvant therapy, then a modified radical mastectomy if a partial or a complete response, and then postmastectomy radiation. I keep harping back on that point simply because that’s the treatment protocol that’s going to give the best outcome.
Então, repetindo, falamos sobre o papel do cirurgião. A primeira coisa é reconhecer que é carcinoma inflamatório. Lembrem-se disso. Não pensem sempre que é um abscesso. Se pensarem que é um abscesso ou mastite, poderiam tratar com um ciclo de antibióticos e observação cuidadosa. Mas, se não melhorar, eu pensaria imediatamente de que se trata de algo mais. E, com sorte, já teriam sido obtidos exames por imagem, e se nestes for observada uma massa, então poderá ser necessária uma biópsia dirigida com agulha grossa e, talvez, mesmo como já dissemos, uma biópsia cutânea com punch. Após o diagnóstico, a paciente deve ser encaminhada para terapia neoadjuvante. Depois, uma mastectomia radical modificada, caso haja resposta parcial ou completa e, depois, irradiação pós-mastectomia. Continuo insistindo nesse ponto simplesmente porque esse é o protocolo terapêutico que dará o melhor resultado.
13
Now, what about the axillary lymph nodes? We already talked about sentinel node not being optimal. But, one other thing is that we can do imaging. We can do ultrasound of the axilla as we do here at MD Anderson, and we’ll actually do a fine needle aspiration of any suspicious lymph nodes that will give us information up front about whether or not the lymph nodes were involved with tumor. And, then, axillary lymph node dissection is still considered the gold standard for IBC patients.
O que dizer sobre os linfonodos axilares? Já comentamos que os linfonodos sentinelas não são ideais. Mas, o que podemos fazer é imaginologia. Podemos fazer ecografia da axila, como fazemos aqui no MD Anderson, e, de fato, fazemos punção aspirativa com agulha fina de qualquer linfonodo linfático suspeito que nos dê informações antecipadas sobre se o tumor comprometeu os linfonodos ou não. Por isso, a linfadenectomia axilar ainda é considerada o padrão-ouro para pacientes com CIM.
So, we already talked about that recognition is the key to optimal treatment and outcome.
Já comentamos que reconhecer é a chave para o tratamento e o resultado ideais.

14
Let’s go over a few cases that might bring this all to a more poignant kind of situation that we can all relate to. The first case would be a 48-year-old patient who presented with IBC. She was considered inoperable because of the extent of the disease. But, there was no distant metastasis and we’ll see why that was in just a second. The patient had an Er positive, Pgr negative, Her-2 negative primary tumor.
Repassemos alguns casos que talvez leve tudo isto a uma situação mais extrema à qual todos nós nos possamos relacionar. O primeiro caso seria o de uma paciente com 48 anos de idade que apresentou CIM. Seu caso foi considerado inoperável por causa da extensão da doença. Mas não havia metástase distante, e já veremos por quê. A paciente teve um tumor primário positivo para Er, negativo para Pgr e negativo para Her-2.
This is why the patient was seen at an outside institution and was told you’re not operable, we really can’t treat you. Obviously, the first thing we thought is, this is a very advanced case of IBC. We see the ulceration of the skin as we talked about, widespread redness and edema, and so, the first thought here is, again, going back to the protocol, neoadjuvant chemotherapy.
Foi por isso que a paciente foi examinada por uma instituição externa e lhe disseram que não era operável e que não podiam tratá-la. Evidentemente, o primeiro que pensamos é que era um caso muito avançado de CIM. Vemos a ulceração da pele, como comentamos antes, a vermelhidão e o edema generalizados e, então, o primeiro que pensamos, de novo, voltando ao protocolo, é a quimioterapia neoadjuvante.
15
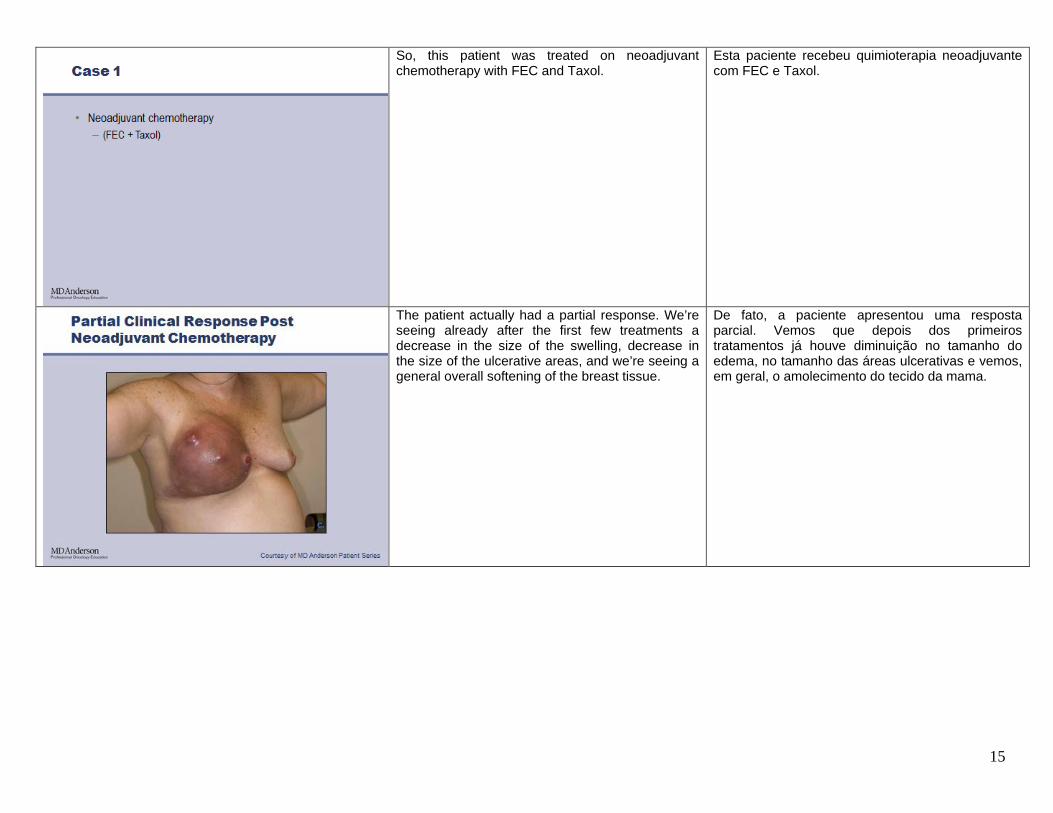
So, this patient was treated on neoadjuvant chemotherapy with FEC and Taxol.
Esta paciente recebeu quimioterapia neoadjuvante com FEC e Taxol.
The patient actually had a partial response. We’re seeing already after the first few treatments a decrease in the size of the swelling, decrease in the size of the ulcerative areas, and we’re seeing a general overall softening of the breast tissue.
De fato, a paciente apresentou uma resposta parcial. Vemos que depois dos primeiros tratamentos já houve diminuição no tamanho do edema, no tamanho das áreas ulcerativas e vemos, em geral, o amolecimento do tecido da mama.

16
The patient eventually had an excellent response and was able to go --- undergo a modified radical mastectomy with negative margins.
No fim, a paciente apresentou uma resposta excelente e pôde ser submetida a uma mastectomia radical modificada com margens negativas.
And, this patient went from, remember, advanced disease to disease that was softening and shrinking, significantly reduced, was able to have a mastectomy with negative margins, and then here, you can see the treatment planning has been done for postmastectomy radiation. So, again, even advanced cases, if they follow the protocol, can receive successful treatment.
E esta paciente, lembrem, passou de uma doença avançada a uma doença que estava amolecendo e diminuindo de tamanho, significativamente menor, e pôde ser submetida a uma mastectomia com margens negativas. E, aqui, podem ver o planejamento do tratamento feito para a irradiação pós-mastectomia. Então, novamente, mesmo em casos avançados, se o protocolo for seguido, podem receber tratamentos bem-sucedidos.
17
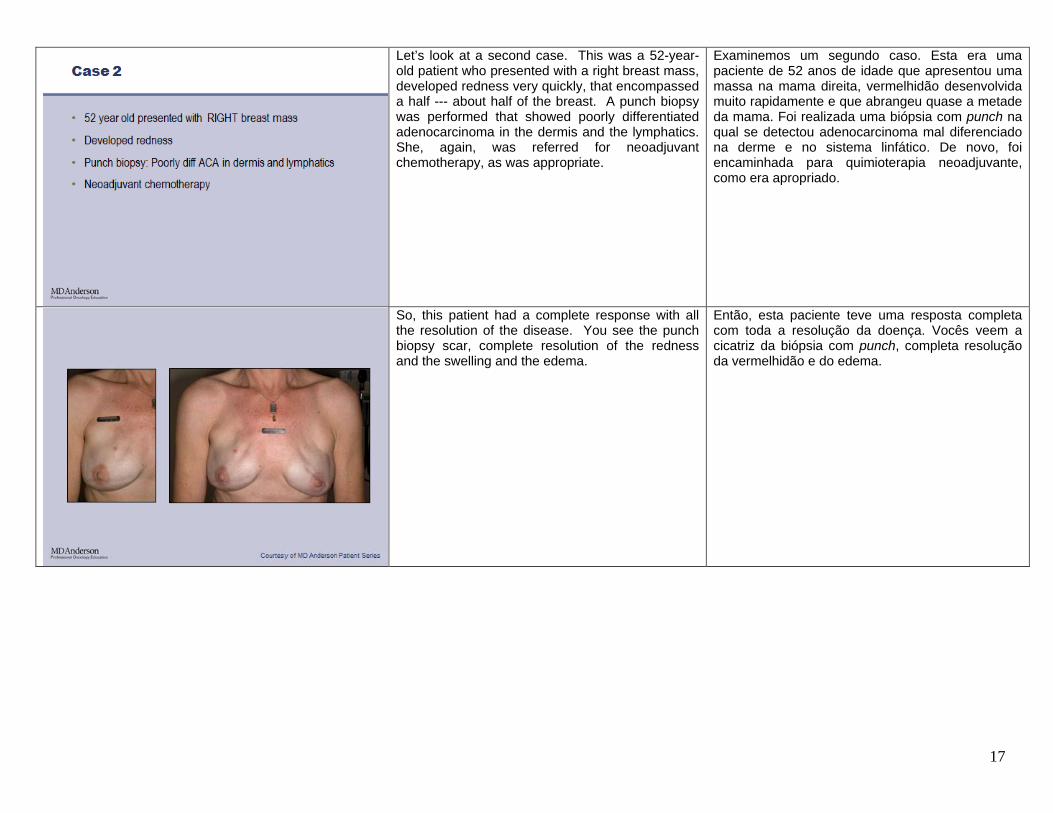
Let’s look at a second case. This was a 52-year-old patient who presented with a right breast mass, developed redness very quickly, that encompassed a half --- about half of the breast. A punch biopsy was performed that showed poorly differentiated adenocarcinoma in the dermis and the lymphatics. She, again, was referred for neoadjuvant chemotherapy, as was appropriate.
Examinemos um segundo caso. Esta era uma paciente de 52 anos de idade que apresentou uma massa na mama direita, vermelhidão desenvolvida muito rapidamente e que abrangeu quase a metade da mama. Foi realizada uma biópsia com punch na qual se detectou adenocarcinoma mal diferenciado na derme e no sistema linfático. De novo, foi encaminhada para quimioterapia neoadjuvante, como era apropriado.
So, this patient had a complete response with all the resolution of the disease. You see the punch biopsy scar, complete resolution of the redness and the swelling and the edema.
Então, esta paciente teve uma resposta completa com toda a resolução da doença. Vocês veem a cicatriz da biópsia com punch, completa resolução da vermelhidão e do edema.
18
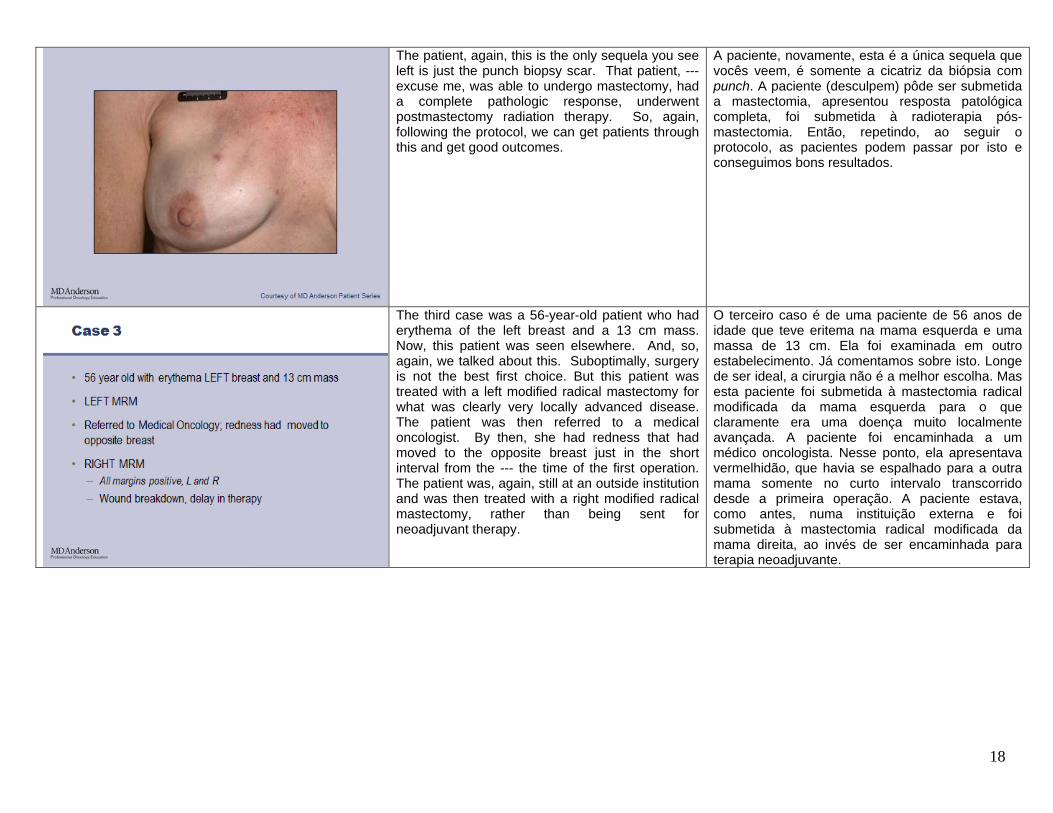
The patient, again, this is the only sequela you see left is just the punch biopsy scar. That patient, --- excuse me, was able to undergo mastectomy, had a complete pathologic response, underwent postmastectomy radiation therapy. So, again, following the protocol, we can get patients through this and get good outcomes.
A paciente, novamente, esta é a única sequela que vocês veem, é somente a cicatriz da biópsia com punch. A paciente (desculpem) pôde ser submetida a mastectomia, apresentou resposta patológica completa, foi submetida à radioterapia pós-mastectomia. Então, repetindo, ao seguir o protocolo, as pacientes podem passar por isto e conseguimos bons resultados.
The third case was a 56-year-old patient who had erythema of the left breast and a 13 cm mass. Now, this patient was seen elsewhere. And, so, again, we talked about this. Suboptimally, surgery is not the best first choice. But this patient was treated with a left modified radical mastectomy for what was clearly very locally advanced disease. The patient was then referred to a medical oncologist. By then, she had redness that had moved to the opposite breast just in the short interval from the --- the time of the first operation. The patient was, again, still at an outside institution and was then treated with a right modified radical mastectomy, rather than being sent for neoadjuvant therapy.
O terceiro caso é de uma paciente de 56 anos de idade que teve eritema na mama esquerda e uma massa de 13 cm. Ela foi examinada em outro estabelecimento. Já comentamos sobre isto. Longe de ser ideal, a cirurgia não é a melhor escolha. Mas esta paciente foi submetida à mastectomia radical modificada da mama esquerda para o que claramente era uma doença muito localmente avançada. A paciente foi encaminhada a um médico oncologista. Nesse ponto, ela apresentava vermelhidão, que havia se espalhado para a outra mama somente no curto intervalo transcorrido desde a primeira operação. A paciente estava, como antes, numa instituição externa e foi submetida à mastectomia radical modificada da mama direita, ao invés de ser encaminhada para terapia neoadjuvante.

19
This patient had margins widely positive for disease, both sides, and had, as you can see here, a wound breakdown that resulted in a significant delay in her therapy. So, again, I want to harp back to the protocol and show that surgery as a first treatment option is a bad idea. And, so, this was a case where the patient was treated with surgery up front, had an open wound, delayed therapy, suboptimal outcome.
A paciente apresentava margens amplamente positivas para a doença, em ambos os lados, e tinha, como podem ver aqui, uma ferida aberta que resultou no atraso significativo da terapia. Novamente, quero insistir no protocolo e mostrar que a cirurgia como primeira opção de tratamento é uma má ideia. Neste caso, o primeiro tratamento da paciente foi cirurgia, apresentou ferida aberta, atraso na terapia e resultado insuficiente.
Now, the good news is, is that when we see these patients early and we can get them started on neoadjuvant therapy, we can have a significant number of patients that will be treatable by --- they will be surgically operable. They will be able to come and have an operation. So, another patient who was seen had chemotherapy, had a complete clinical response with complete resolution of the redness, had a mastectomy with widely free margins, underwent postmastectomy radiation. And again, these patients do have a high risker of recurrence somewhere else, as we talked about, but if we can achieve this, we already said we’re going to get local control in 80 percent. And, we’re going to provide the optimal outcomes possible by that mo --- triple modality of chemotherapy, mastectomy, radiation.
A boa notícia é que, quando examinamos estas pacientes no início e podemos iniciar terapia neoadjuvante, poderemos ter um número significativo de pacientes que podem ser operadas. Elas poderão vir e serem submetidas a cirurgia. Outra paciente que havia sido examinada recebeu quimioterapia, apresentou uma resposta clínica completa com resolução completa da vermelhidão, foi submetida a uma mastectomia com margens amplamente livres e à irradiação pós-mastectomia. Novamente, estas pacientes apresentam um maior risco de reincidência em outras áreas, como comentamos, mas se formos bem-sucedidos, já dissemos que conseguiremos controle local em 80%. E conseguiremos os melhores resultados possíveis por meio da modalidade tríplice: quimioterapia, mastectomia, irradiação.
20
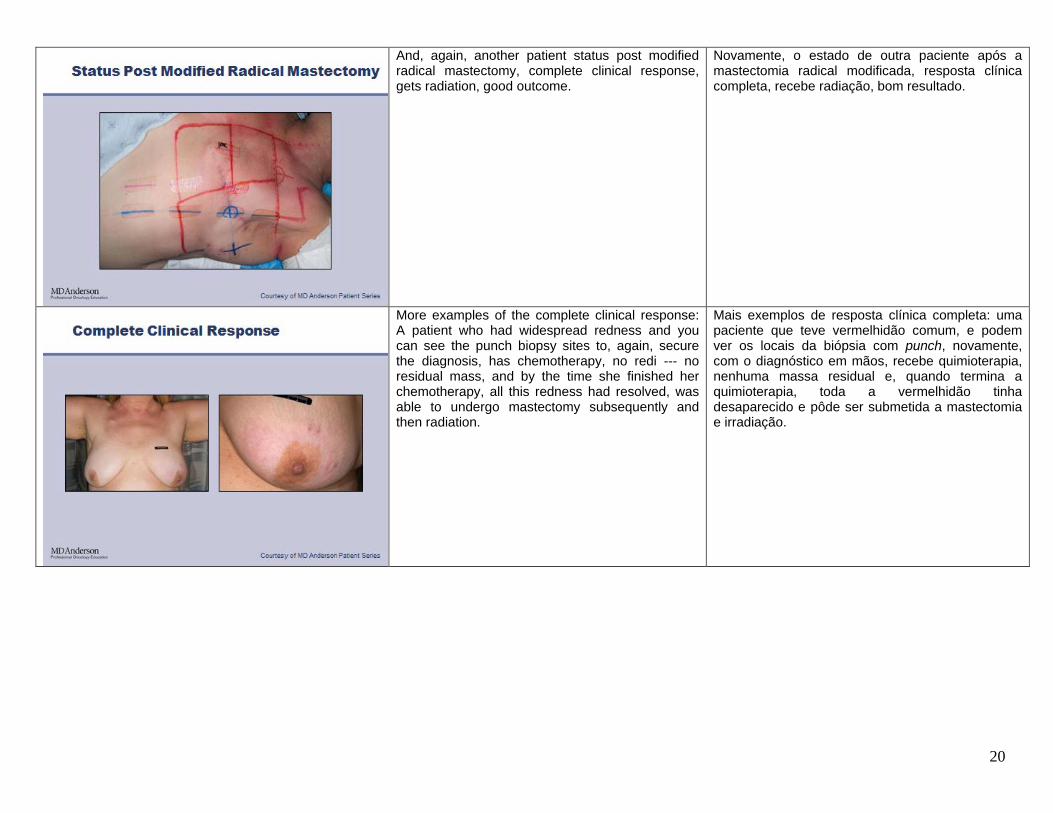
And, again, another patient status post modified radical mastectomy, complete clinical response, gets radiation, good outcome.
Novamente, o estado de outra paciente após a mastectomia radical modificada, resposta clínica completa, recebe radiação, bom resultado.
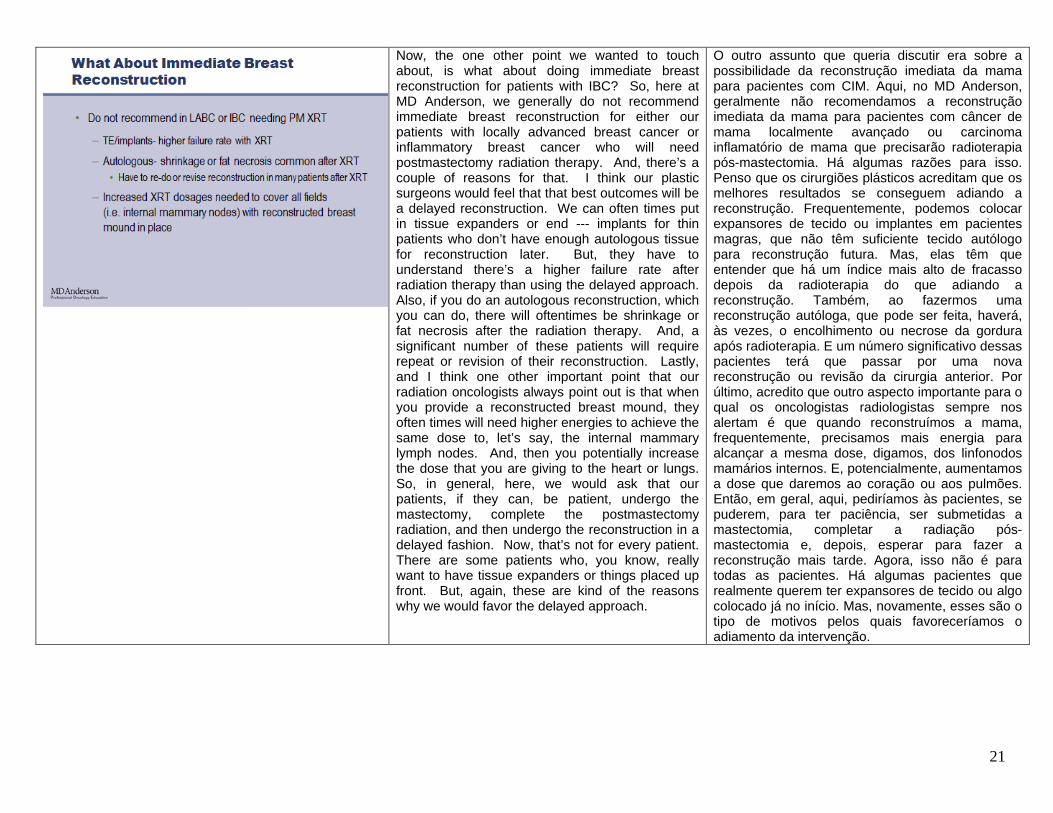
More examples of the complete clinical response: A patient who had widespread redness and you can see the punch biopsy sites to, again, secure the diagnosis, has chemotherapy, no redi --- no residual mass, and by the time she finished her chemotherapy, all this redness had resolved, was able to undergo mastectomy subsequently and then radiation.
Mais exemplos de resposta clínica completa: uma paciente que teve vermelhidão comum, e podem ver os locais da biópsia com punch, novamente, com o diagnóstico em mãos, recebe quimioterapia, nenhuma massa residual e, quando termina a quimioterapia, toda a vermelhidão tinha desaparecido e pôde ser submetida a mastectomia e irradiação.
21
Now, the one other point we wanted to touch about, is what about doing immediate breast reconstruction for patients with IBC? So, here at MD Anderson, we generally do not recommend immediate breast reconstruction for either our patients with locally advanced breast cancer or inflammatory breast cancer who will need postmastectomy radiation therapy. And, there’s a couple of reasons for that. I think our plastic surgeons would feel that that best outcomes will be a delayed reconstruction. We can often times put in tissue expanders or end --- implants for thin patients who don’t have enough autologous tissue for reconstruction later. But, they have to understand there’s a higher failure rate after radiation therapy than using the delayed approach. Also, if you do an autologous reconstruction, which you can do, there will oftentimes be shrinkage or fat necrosis after the radiation therapy. And, a significant number of these patients will require repeat or revision of their reconstruction. Lastly, and I think one other important point that our radiation oncologists always point out is that when you provide a reconstructed breast mound, they often times will need higher energies to achieve the same dose to, let’s say, the internal mammary lymph nodes. And, then you potentially increase the dose that you are giving to the heart or lungs. So, in general, here, we would ask that our patients, if they can, be patient, undergo the mastectomy, complete the postmastectomy radiation, and then undergo the reconstruction in a delayed fashion. Now, that’s not for every patient. There are some patients who, you know, really want to have tissue expanders or things placed up front. But, again, these are kind of the reasons why we would favor the delayed approach.
O outro assunto que queria discutir era sobre a possibilidade da reconstrução imediata da mama para pacientes com CIM. Aqui, no MD Anderson, geralmente não recomendamos a reconstrução imediata da mama para pacientes com câncer de mama localmente avançado ou carcinoma inflamatório de mama que precisarão radioterapia pós-mastectomia. Há algumas razões para isso. Penso que os cirurgiões plásticos acreditam que os melhores resultados se conseguem adiando a reconstrução. Frequentemente, podemos colocar expansores de tecido ou implantes em pacientes magras, que não têm suficiente tecido autólogo para reconstrução futura. Mas, elas têm que entender que há um índice mais alto de fracasso depois da radioterapia do que adiando a reconstrução. Também, ao fazermos uma reconstrução autóloga, que pode ser feita, haverá, às vezes, o encolhimento ou necrose da gordura após radioterapia. E um número significativo dessas pacientes terá que passar por uma nova reconstrução ou revisão da cirurgia anterior. Por último, acredito que outro aspecto importante para o qual os oncologistas radiologistas sempre nos alertam é que quando reconstruímos a mama, frequentemente, precisamos mais energia para alcançar a mesma dose, digamos, dos linfonodos mamários internos. E, potencialmente, aumentamos a dose que daremos ao coração ou aos pulmões. Então, em geral, aqui, pediríamos às pacientes, se puderem, para ter paciência, ser submetidas a mastectomia, completar a radiação pós-mastectomia e, depois, esperar para fazer a reconstrução mais tarde. Agora, isso não é para todas as pacientes. Há algumas pacientes que realmente querem ter expansores de tecido ou algo colocado já no início. Mas, novamente, esses são o tipo de motivos pelos quais favoreceríamos o adiamento da intervenção.

22
So, in conclusion, the really important point that I think I’ve harped on several times throughout the talk is that diagnosis is really the key. Recognizing the signs and symptoms of IBC, not treating for a prolonged time as an infection, recognizing what it is and getting it treated with systemic therapy up front is --- and then followed by surgery for the patients who respond, followed by radiation, is going to give you the best outcomes. So, really, recognition is really important. And, I think part of this whole educational program is making sure that clinicians are aware that these are patients that really do require recognition of the disease early on to provide really a chance at getting a cure.
Em conclusão, o ponto verdadeiramente importante que acredito ter insistido várias vezes durante toda a palestra é que a chave é o diagnóstico. Reconhecer os sinais e sintomas do CIM, não tratar por um tempo prolongado como infecção, reconhecer o que é e tratar inicialmente com terapia sistêmica e, depois, prosseguir com a cirurgia para as pacientes que responderem, seguida de irradiação, dará os melhores resultados. Então, reconhecer é realmente importante. Acredito que parte de todo este programa educacional é para confirmar se os clínicos têm conhecimento de que para as pacientes terem chance de cura sua doença deve ser reconhecida no início.
So, we already talked about the protocol multiple times. Neoadjuvant chemotherapy, modified radical mastectomy for partial or complete responders, followed by postmastectomy radiation. And, really, I think the way we’re going to get improved outcomes is --- is early identification, diagnosis, early institution of systemic therapy. And, then really, I think, in the future, if we can find out which patients are likely to have already disseminated disease or cell --- circulating cells that may be responsible for later recurrences, we can try to target those and improve outcomes. And, I think as we move along, patients with IBC will be a great group to study as far as targeted therapies, personalized therapies that may have a higher chance of working against these cells which generally behave a little different than your normal run of the mill and basic breast cancers. So, with that, I would just like to say thank you for your attention, and we’d really appreciate any questions or feedback you have about this educational presentation. Thank you.
Já falamos várias vezes sobre o protocolo. Quimioterapia neoadjuvante, mastectomia radical modificada para as que responderem parcial ou completamente, seguida de irradiação pós-mastectomia. De fato, acredito que a maneira que poderemos obter melhores resultados é com identificação e diagnóstico precoces e a instituição antecipada de uma terapia sistêmica. Penso que, no futuro, se pudermos descobrir quais as pacientes com probabilidade de já terem doença disseminada ou células circulantes que podem ser responsáveis pelas reincidências tardias, poderemos procurar atingi-las e melhorar os resultados. À medida que avançamos, penso, também, que as pacientes com CIM formarão um excelente grupo de estudo no que se refere a terapias dirigidas, terapias personalizadas que podem ter uma maior chance de ser contraproducentes a essas células que geralmente se comportam um pouco diferente do que as normais e dos cânceres de mama comuns. Então, com isso, gostaria de agradecer a atenção e dizer que teria o maior prazer em poder responder a perguntas ou receber suas opiniões sobre esta apresentação educacional. Obrigado.















![A Ultrassonografia na Doença Veno-Oclusiva … ARP e dos hepatócitos, alterações hemodinâmicas, desordens da coagulação e libertação de citocinas[2]. Não há exsudado inflamatório](https://img.pdfslide.us/doc/110x75/5c0a2abe09d3f2691a8b5f01/a-ultrassonografia-na-doenca-veno-oclusiva-arp-e-dos-hepatocitos-alteracoes.jpg)

![Single Secret Leader Election - Stanford Universitycrypto.stanford.edu/~saba/slides/SSLE.pdfPart 1 com(u1) com(u2) com(u3) com(u4) com(u5) Election R∈[N] com(u2) com(u5) com(u4)](https://img.pdfslide.us/doc/110x75/6049abecaf0f86461d49642a/single-secret-leader-election-stanford-sabaslidessslepdf-part-1-comu1-comu2.jpg)










