Embed Size (px)
Citation preview



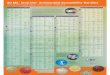
Graph 3 - Rate of Divisional Conscientious Objection from March 2003 to March 2004
0.50%
1.00%
1.50%
2.00%
2.50%
3.00%
3.50%
4.00%
4.50%
5.00%
5.50%
Mar-03 Jun-03 Sep-03 Dec-03 Mar-04
Month of calculation
Ra
te o
f c
on
sc
ien
tio
us
ob
jec
tio
n
NORTHERN RIVERS DIVISION OF GENERAL PRACTICE NSW ADELAIDE HILLS DIVISION OF GENERAL PRACTICE TWEED VALLEY DIVISION OF GENERAL PRACTICE
SUNSHINE COAST DIVISION OF GENERAL PRACTICE BLUE MOUNTAINS DIVISION OF GENERAL PRACTICE MID NORTH COAST DIVISION OF GENERAL PRACTICE
FAR NORTH QUEENSLAND DIVISION OF GENERAL PRACTICE GOLD COAST DIVISION OF GENERAL PRACTICE BRISBANE INNER SOUTH DIVISION OF GENERAL PRACTICE
GREAT SOUTHERN DIVISION OF GENERAL PRACTICE ADELAIDE CENTRAL & EASTERN DIVISION OF GENERAL PRACTICE ADELAIDE SOUTHERN DIVISION OF GENERAL PRACTICE
BENDIGO & DISTRICT DIVISION OF GENERAL PRACTICE MANLY WARRINGAH DIVISION OF GP TOOWOOMBA & DISTRICT DIVISION OF GENERAL PRACTICE
EASTERN RANGES DIVISION NORTH-EAST VICTORIAN DIVISION OF GENERAL PRACTICE PEEL & SOUTH WEST DIVISION OF GENERAL PRACTICE
NORTH-EAST VALLEY DIVISION OF GP SOUTHERN HIGHLANDS DIVISION OF GENERAL PRACTICE OTWAY DIVISION OF GENERAL PRACTICE
BAROSSA DIVISION OF GENERAL PRACTICE CAIRNS DIVISION OF GENERAL PRACTICE FREMANTLE REGIONAL GP NETWORK
SOUTH EAST NSW DIVISION OF GENERAL PRACTICE CENTRAL WHEATBELT DIVISION OF GENERAL PRACTICE BRISBANE NORTH DIVISION OF GENERAL PRACTICE
REDCLIFFE-CABOOLTURE-BRIBIE DIVISION OF GENERAL PRACTICE BAYSIDE GP DIVISION EASTERN SYDNEY DIVISION OF GENERAL PRACTICE
WIDE BAY DIVISION OF GENERAL PRACTICE ASSOCIATION INC WHITEHORSE DIVISION OF GENERAL PRACTICE CENTRAL-WEST GIPPSLAND DIVISION OF GENERAL PRACTICE
GREATER BUNBURY DIVISION OF GP , SOUTH WEST HEALTH CAMPUS INNER SOUTH EAST MELBOURNE DIVISION OF GENERAL PRACTICE
Northern Rivers
Division
Tweed Valley Division
Sunshine Coast Division
Adelaide Hills Division
Blue Mountains Division
Mid North Coast Division (NSW)

http://stopavn.com/


https://www.facebook.com/groups/nrvsgroup/

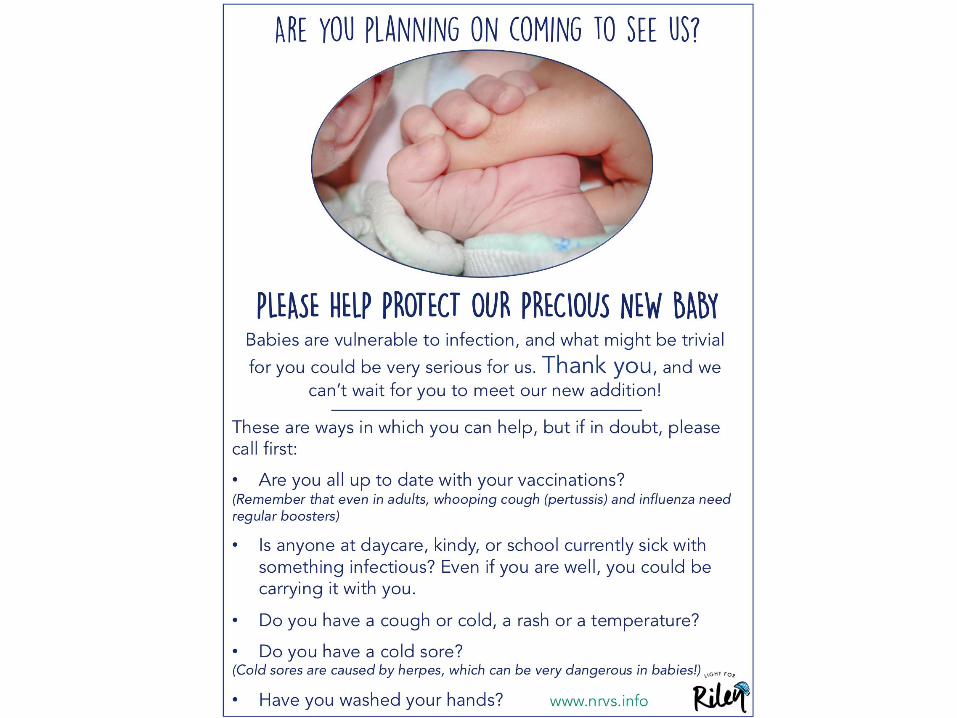
www.nrvs.info

3 years old girl with the lesion as seen in the picture. Patents not sure how long has it been there. Not certainly present 7-10 days ago. Complaining of pain but not particularly sore on examination, afebrile, no active discharge. Looks well. No rash elsewhere in the body. Recently returned from Singapore few days ago. Thoughts ? Impetigo ?

32yo food industry worker presented with 6/52 history of itchy erythematous rash on L arm, for which she had trialled terbinafibe cream. Presented due to increasing size and lesions now appearing on R arm.Well apart from chronic idiopathic neutropenia, no hx psoriasis or overseas travel, systemically well O/E scaling several erythematous lesions on upper arms with central clearing and yellow crusting, largest lesions ~2-3cm diameter with assoc/ satellite lesions. No scabies burrows. I decided to treat as secondarily infected fungal lesions with bactroban and anti fungal and advised covering lesions at work. swab neg for fungal, positive s.aureus, when presented for review 3/7 later lesions had spread down arms with some inflamed papules and pustules. Started fluclox, suggested she try a couple of bleach baths, time off work to avoid heat. Bacterial Infection cleared with oral antibiotics leaving still excruciatingly itchy desquamating rash on arms and now a few lesion on calves. Advised emollients & hydrozole + wet wraps, eventually trialled 3/7 prednisone due to severity of itch. this is the rash post steroids. currently we are pushing on with topical steroids and emollients as she returns to work

75 year old lady with multiple comorbids (DM, AF, CCF, OA, COPD). Presented with pruritus initially in the lower legs for the last 3 months. Eventually erosions and excoriations developed. Then same in the shoulder & upper arm. No recent change in medications. Tried on antihistamine, antibiotics and topical steroids. Partial response and flares up again


GPs Down Under is the online community of General Practitioners in Australia. To join the group you need to be a GP in Australia. WELCOME. PLEASE READ CONDUCT CODE This group is for all GPs working in Australia and is to provide a forum where we can respectfully network, chat with one another and provide a supportive learning environment where we can share experiences, or difficulties. Please feel free to discuss any interesting cases, share your clinical conundrums, discuss events, or anything else that you may like to! Case studies should be deidentified as much as possible. This is not a forum that constitutes medical advice legal advice financial advice and members are advised to note this carefully. All information should not be relied upon and especially treatment decisions are the responsibility of the treating practitioner.

If you have patient photos to discuss it is imperative that you have a signed consent form from the patient saying they are happy for you to discuss their picture online with other GPs. Social media Forums such as this are still subject to AHPRA legislation and it is important you are familiar and comply with that legislation. Noting too that those members of the ADF should not post with a notification of their location in accordance with ADF regulations. Mandatory reporting laws apply in each state of Australia and GP's need to be familiar with their responsibilities in this regard.


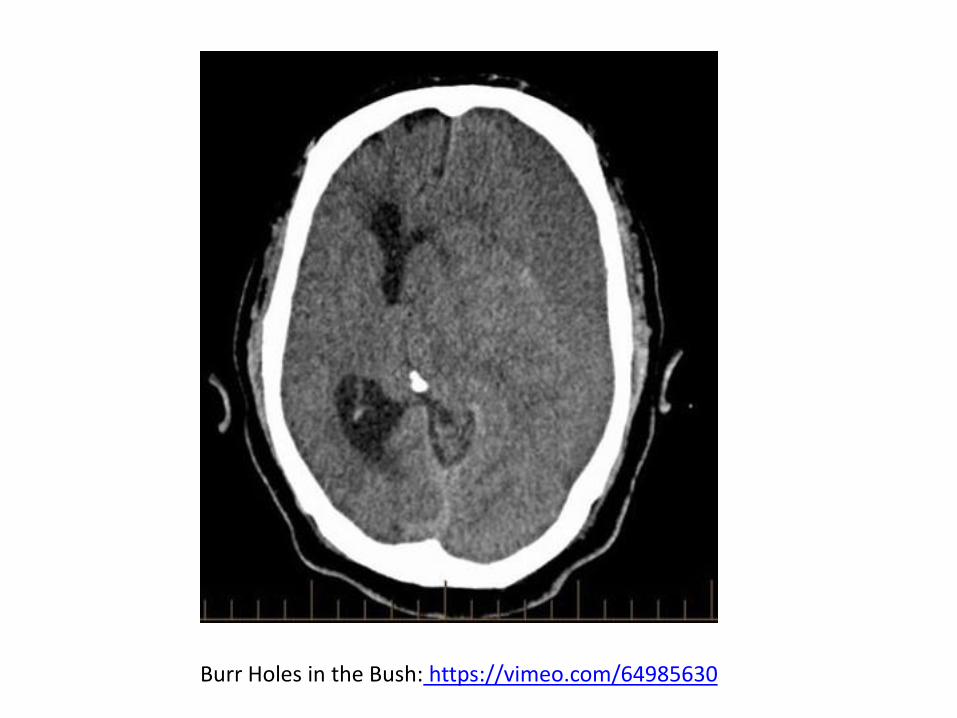
Burr Holes in the Bush: https://vimeo.com/64985630
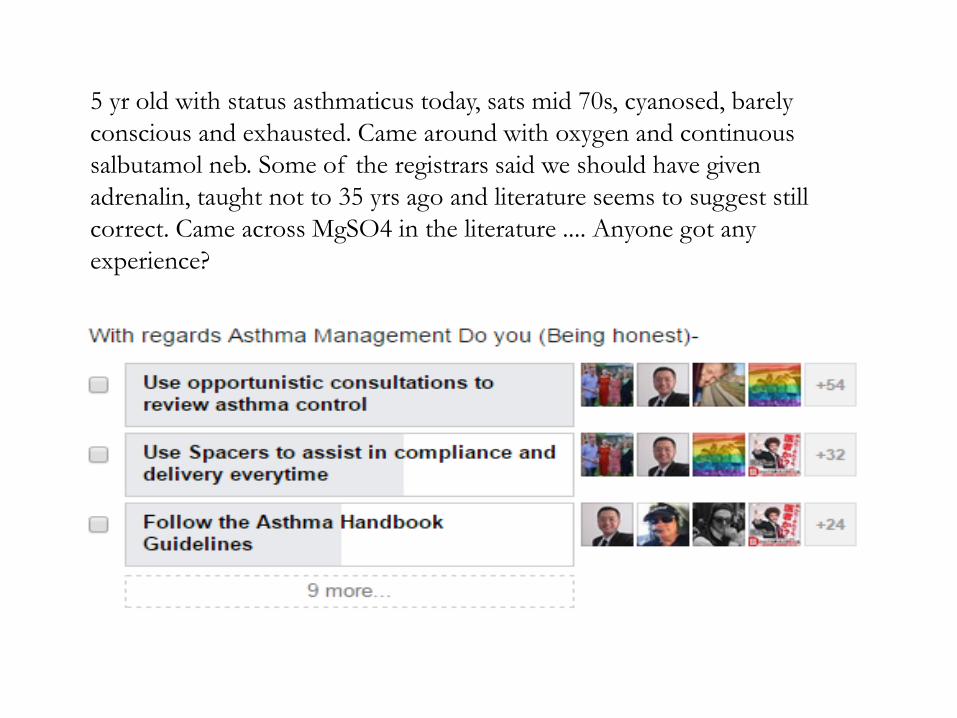
5 yr old with status asthmaticus today, sats mid 70s, cyanosed, barely
conscious and exhausted. Came around with oxygen and continuous
salbutamol neb. Some of the registrars said we should have given
adrenalin, taught not to 35 yrs ago and literature seems to suggest still
correct. Came across MgSO4 in the literature .... Anyone got any
experience?

A new pt- a lady in her late 40's presented with unilateral numbness on rt
chin and lower lip. Came on a day ago. At the same time she had some
toothache and increase sensitivity on her tooth. Saw a dentist who
thought although she had severe dental caries did not think it was dental
issue. Has localised reduced sensation to pinprick and light touch in
distribution of rt mental nerve. Not in any other distribution of
trigeminal nerve. No other focal neurology on history and examination.
No risk factors for stroke. No recent dental procedures. Did a CT scan
came back normal. I've called up the dentist who will be getting an
expert opinion from a oral dental specialist. On googling found few case
report about "numb chin" presenting as first sign of metastatic disease.
Any ideas. MS??
16 yo girl presents with Hb 77 (likely fr deficient as hypo micro but fe
studies pending). Other than being tired she's fine. Obviously I'll look
into cause but what to do in the immediate future? Not quite low
enough for a blood transfusion!
Where can I find out how long it takes for a vaccine to become
effective? The Australian Immunisation Handbook is my normal
reference but it doesn't seem to include this information.
61 year old male. Late onset type 1 diabetic 16 years ago. On
insulin and statin. Diabetes well controlled, normal BP and
bmi. His cardiovascular risk is 13% Dad stroke aged 57. Use
aspirin for primary prevention or not?
This new prostate cancer screening info sheet looks great:
http://www.racgp.org.au/…/Prostate-cancer-screening-info-sh…
In the last month or so I have seen both hypercaroteinemia and
Fox-Fordyce Disease not long after pictures were posted on
GPDU. Not sure whether the patients feel better or worse about
their GP going to FB for a diagnosis than 'Dr Google', but
thanks guys!
There seems to be quite a few self-help online CBT courses for
anxiety/depression these days. Can anyone recommend a particular
site for a good quality program that you have done or gotten good
feedback from patients? I am particularly interested in an online
CBT program that can help a patient with anxiety/social phobia
after a motor vehicle accident that rendered him with chronic pain
relating to MVA injuries.
I found out today that xxx has made it company policy that the
employee notifies them of the NATURE of their illness or injury.
I think this is a breach of privacy. The employee told me it's
company policy and they have to follow it. What do you think?
Want to know more about the MTHFR gene - perhaps a patient
handout? - Good information here -
http://www.genetics.edu.au/Professionals/mthfr-dna-test
another good resource book
http://www.genetics.edu.au/.../genetics-in-general-practice
Today I had a family of a 4 month old tell me they were going to be
taking her to a chiropractor because she didn't sleep well. Aside from the
discussion re normal sleep in infants and making sure no medical
reasons/mental health problems are going on here, what would you say
to this? I don't like to put down another profession but I really don't like
the idea of people taking young infants to a chiropractor.
What is your approach to patients talking about going to chiropractors
and osteopaths etc? Especially with children/infants?
Does anyone have any links or tips to share to help improve workloads,
waiting times and general flow of patients within a practice? Thanks.
Learnt something new today – pantoprazole can apparently cause a false
positive for THC on drug screening. I wonder if this is a problem for all
those overweight FIFO miners…often on PPIs but required to do
regular drug screens? http://www.thepoisonreview.com/…/protonix-
pantoprazole-can…/




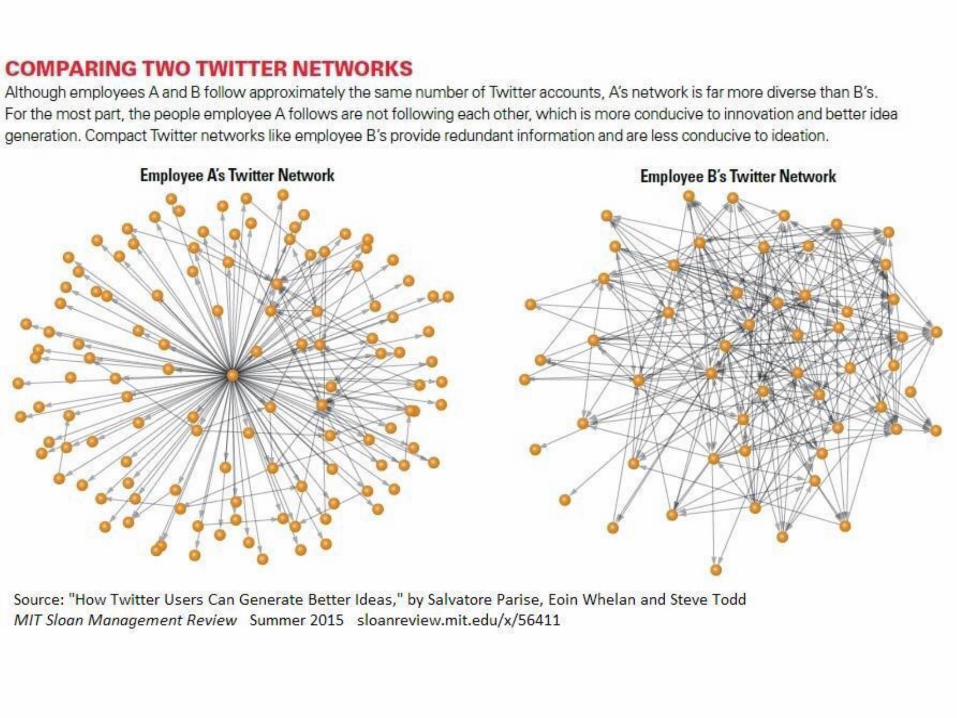
Eric Levi is an otolaryngologist in Australia who blogs at his self-titled site, Dr Eric Levi. He can be reached on Twitter @DrEricLevi. http://www.kevinmd.com/blog/2015/06/5-types-of-doctors-you-will-meet-on-social-media.html
5 types of doctors you will meet on social media: Dr Eric Levi, Social Media 27 June 2015
1. The knowledge distributor. These are the ones who frequently tweet and retweet various information, news, latest studies, guidelines, and opinions. http://www.phrp.com.au/wp-content/uploads/2015/07/PHRP-25-03-Twitter-04-FINAL-1Jul15.pdf
2. The court jester. The court jester is the one who entertains, enlightens and yet educates at the same time.
3. The social collaborator. They are fun to hang out with. They are one of the main reasons for joining social media. It is social after all.
4. The relentless commentator. The devil’s advocate. They seem to have an opinion on and a comment for anything and everything. Some of them good, some of them very critical and negative.
5. The thought leader. Here’s the one everyone wants to be. The person who leads the world with contemporary ideas and tweets their sophisticated perspective to everyone. Twitter truly adds to their impact and in some immeasurable ways, they are truly changing the world.