Embed Size (px)
Citation preview

PowerPoint® Lecture Slides prepared by Janice Meeking, Mount Royal College
C H A P T E R
Copyright © 2010 Pearson Education, Inc.
17
Blood

Copyright © 2010 Pearson Education, Inc.
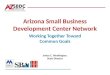
Figure 17.1
1 Withdrawblood and placein tube.
2 Centrifuge theblood sample.
Plasma• 55% of whole blood• Least dense componentBuffy coat• Leukocytes and platelets• <1% of whole bloodErythrocytes• 45% of whole blood• Most dense component
Formedelements
• Hematocrit• Percent of blood volume that is RBCs • 47% ± 5% for males• 42% ± 5% for females

Copyright © 2010 Pearson Education, Inc.
Physical Characteristics and Volume
•Sticky, opaque fluid
•Color scarlet to dark red
•pH 7.35–7.45
•38C
•~8% of body weight
•Average volume: 5–6 L for males, and 4–5 L for females

Copyright © 2010 Pearson Education, Inc.
Functions of Blood
1. Distribution of
• O2 and nutrients to body cells
• Metabolic wastes to the lungs and kidneys for elimination
• Hormones from endocrine organs to target organs

Copyright © 2010 Pearson Education, Inc.
Functions of Blood
2. Regulation of
• Body temperature by absorbing and distributing heat
• Normal pH using buffers
• Adequate fluid volume in the circulatory system

Copyright © 2010 Pearson Education, Inc.
Functions of Blood
3. Protection against
• Blood loss
• Plasma proteins and platelets initiate clot formation
• Infection
• Antibodies
• Complement proteins (small proteins that amplify other immune cells ability to kill pathogens)
• WBCs defend against foreign invaders

Copyright © 2010 Pearson Education, Inc.
Blood Composition
•Blood: a fluid connective tissue composed of
• Plasma
• Formed elements
•Erythrocytes (red blood cells, or RBCs)
•Leukocytes (white blood cells, or WBCs)
•Platelets

Copyright © 2010 Pearson Education, Inc.
Blood Plasma
•90% water
•Proteins
•mostly produced by the liver
•60% albumin
•36% globulins
•4% fibrinogen

Copyright © 2010 Pearson Education, Inc.
Blood Plasma
•Nitrogenous by-products of metabolism—lactic acid, urea, creatinine
•Nutrients—glucose, carbohydrates, amino acids
•Electrolytes—Na+, K+, Ca2+, Cl–, HCO3–
•Respiratory gases—O2 and CO2
•Hormones

Copyright © 2010 Pearson Education, Inc.
Formed Elements (WBC, RBC, platelets)

Copyright © 2010 Pearson Education, Inc.
Formed Elements
•Only WBCs are complete cells
•RBCs have no nuclei or organelles
•Platelets are cell fragments
•Most formed elements survive in the bloodstream for only a few days
•Most blood cells originate in bone marrow and do not divide

Copyright © 2010 Pearson Education, Inc. Figure 17.2
Platelets
Neutrophils Lymphocyte
Erythrocytes Monocyte

Copyright © 2010 Pearson Education, Inc.
RBCs or Erythrocytes

Copyright © 2010 Pearson Education, Inc.
Erythrocytes
•Biconcave discs, anucleate, essentially no organelles
•Filled with hemoglobin (Hb) for gas transport

Copyright © 2010 Pearson Education, Inc. Figure 17.3
2.5 µm
7.5 µm
Side view (cut)
Top view

Copyright © 2010 Pearson Education, Inc.
Erythrocytes
•Structural characteristics contribute to gas transport
• Biconcave shape—huge surface area relative to volume
• >97% hemoglobin (not counting water)
•No mitochondria; ATP production is anaerobic; no O2 is used in generation of ATP
•A great example of how structure and function work together!

Copyright © 2010 Pearson Education, Inc.
Erythrocyte Function
•Hemoglobin structure
• Protein globin: two alpha and two beta chains
•Heme pigment bonded to each globin chain (4)
•Iron atom in each heme can bind to one O2 molecule; binds reversibly
•Each Hb molecule can transport four O2
•Normal Hb: 12-16 in women, 13-18 in men

Copyright © 2010 Pearson Education, Inc. Figure 17.4
Hemegroup
(a) Hemoglobin consists of globin (two alpha and two beta polypeptide chains) and four heme groups.
(b) Iron-containing heme pigment. Globin chains
Globin chains

Copyright © 2010 Pearson Education, Inc.
Hemoglobin (Hb)
•O2 loading in the lungs
• Produces oxyhemoglobin (ruby red)
•O2 unloading in the tissues
• Produces deoxyhemoglobin or reduced hemoglobin (dark red)
•CO2 loading in the tissues
• Produces carbaminohemoglobin (carries 20% of CO2 in the blood)

Copyright © 2010 Pearson Education, Inc.
Hematopoiesis
•Hematopoiesis (hemopoiesis): blood cell formation
• Formed in red marrow
•Red marrow is found mainly in the flat bones, such as pelvis, sternum, cranium, ribs, vertebrae, and scapula. Also in the spongy epiphyseal plates of long bones like the femur and humerus.

Copyright © 2010 Pearson Education, Inc. Figure 17.5
Stem cell
HemocytoblastProerythro-blast
Earlyerythroblast
Lateerythroblast Normoblast
Phase 1Ribosomesynthesis
Phase 2Hemoglobinaccumulation
Phase 3Ejection ofnucleus
Reticulo-cyte
Erythro-cyte
Committedcell
Developmental pathway

Copyright © 2010 Pearson Education, Inc.
Regulation of Erythropoiesis
•Too few RBCs leads to tissue hypoxia
•Too many RBCs increases blood viscosity
•Balance between RBC production and destruction depends on
•Hormonal controls
• Adequate supplies of iron, amino acids, and B vitamins

Copyright © 2010 Pearson Education, Inc.
Hormonal Control of Erythropoiesis
•Erythropoietin (EPO)
•Direct stimulus for erythropoiesis
•Released by the kidneys in response to hypoxia

Copyright © 2010 Pearson Education, Inc.
Hormonal Control of Erythropoiesis
•Causes of hypoxia
•Hemorrhage or increased RBC destruction reduces RBC numbers
• Insufficient hemoglobin (e.g., iron deficiency)
•Reduced availability of O2 (e.g., high altitudes)

Copyright © 2010 Pearson Education, Inc.
Hormonal Control of Erythropoiesis
•Effects of EPO
•More rapid maturation of committed bone marrow cells
• Increased circulating reticulocyte count in 1–2 days
•Testosterone also enhances EPO production, resulting in higher RBC counts in males

Copyright © 2010 Pearson Education, Inc. Figure 17.6, step 5
Kidney (and liver toa smaller extent)releaseserythropoietin. Erythropoietin
stimulates redbone marrow.
Enhancederythropoiesisincreases RBCcount.
O2- carryingability of bloodincreases.
Homeostasis: Normal blood oxygen levels
Stimulus:Hypoxia (low bloodO2- carrying ability)
due to• Decreased
RBC count• Decreased amount
of hemoglobin• Decreased
availability of O2
1
2
3
4
5
IMBALANCE
IMBALANCE

Copyright © 2010 Pearson Education, Inc.
Dietary Requirements for Erythropoiesis
•Nutrients—amino acids, lipids, and carbohydrates
• Iron
• Stored in Hb (65%), the liver, spleen, and bone marrow
• Stored in cells as ferritin and hemosiderin
•Vitamin B12 and folic acid—necessary for DNA synthesis for cell division

Copyright © 2010 Pearson Education, Inc.
Fate and Destruction of Erythrocytes
•Life span: 100–120 days
•Old RBCs become fragile, and Hb begins to degenerate
•Macrophages engulf dying RBCs in the spleen

Copyright © 2010 Pearson Education, Inc. Figure 17.7, step 1
Low O2 levels in blood stimulatekidneys to produce erythropoietin.1

Copyright © 2010 Pearson Education, Inc. Figure 17.7, step 2
Low O2 levels in blood stimulatekidneys to produce erythropoietin.1
Erythropoietin levels risein blood.2

Copyright © 2010 Pearson Education, Inc. Figure 17.7, step 3
Low O2 levels in blood stimulatekidneys to produce erythropoietin.1
Erythropoietin levels risein blood.2
Erythropoietin and necessaryraw materials in blood promoteerythropoiesis in red bone marrow.
3

Copyright © 2010 Pearson Education, Inc. Figure 17.7, step 4
Low O2 levels in blood stimulatekidneys to produce erythropoietin.1
Erythropoietin levels risein blood.2
Erythropoietin and necessaryraw materials in blood promoteerythropoiesis in red bone marrow.
3
New erythrocytesenter bloodstream;function about 120 days.
4

Copyright © 2010 Pearson Education, Inc.
Fate and Destruction of Erythrocytes
•Heme and globin are separated
• Iron is salvaged for reuse
•Heme is degraded to yellow the pigment bilirubin
• Liver secretes bilirubin (in bile) into the intestines
•Degraded pigment leaves the body in feces as stercobilin
•Globin is metabolized into amino acids

Copyright © 2010 Pearson Education, Inc. Figure 17.7, step 5
Aged and damaged redblood cells are engulfed bymacrophages of liver,spleen, and bonemarrow; thehemoglobin isbroken down.
5 Hemoglobin
Aminoacids
GlobinHeme
Circulation
Iron storedas ferritin,hemosiderin
Bilirubin
Bilirubin is picked up from bloodby liver, secreted into intestine inbile, metabolized to stercobilin bybacteria, and excreted in feces.

Copyright © 2010 Pearson Education, Inc. Figure 17.7, step 6
Aged and damaged redblood cells are engulfed bymacrophages of liver,spleen, and bonemarrow; thehemoglobin isbroken down.
5
Raw materials aremade available in bloodfor erythrocyte synthesis.
6
Hemoglobin
Aminoacids
Globin
Iron is bound totransferrin and releasedto blood from liver asneeded for erythropoiesis.
Food nutrients,including amino acids,Fe, B12, and folic acid,are absorbed fromintestine and enterblood.
Heme
Circulation
Iron storedas ferritin,hemosiderin
Bilirubin
Bilirubin is picked up from bloodby liver, secreted into intestine inbile, metabolized to stercobilin bybacteria, and excreted in feces.

Copyright © 2010 Pearson Education, Inc. Figure 17.7
Low O2 levels in blood stimulate kidneys to produce erythropoietin.
1
Erythropoietin levels risein blood.2
Erythropoietin and necessaryraw materials in blood promoteerythropoiesis in red bone marrow.
3
Aged and damagedred blood cells areengulfed by macrophagesof liver, spleen, and bonemarrow; the hemoglobinis broken down.
5
New erythrocytesenter bloodstream;function about 120 days.
4
Raw materials aremade available in bloodfor erythrocyte synthesis.
6
Hemoglobin
Aminoacids
Globin
Iron is bound totransferrin and releasedto blood from liver asneeded for erythropoiesis.
Food nutrients,including amino acids,Fe, B12, and folic acid,are absorbed fromintestine and enterblood.
Heme
Circulation
Iron storedas ferritin,hemosiderin
Bilirubin
Bilirubin is picked up from bloodby liver, secreted into intestine inbile, metabolized to stercobilin bybacteria, and excreted in feces.

Copyright © 2010 Pearson Education, Inc.
Erythrocyte Disorders
•Anemia: blood has abnormally low O2-carrying capacity
• A sign rather than a disease itself
• Accompanied by fatigue, paleness, shortness of breath, and chills

Copyright © 2010 Pearson Education, Inc.
Causes of Anemia
1. Insufficient erythrocytes
• Hemorrhagic anemia: acute or chronic loss of blood
• Hemolytic anemia: RBCs rupture prematurely
• Aplastic anemia: destruction or inhibition of red bone marrow

Copyright © 2010 Pearson Education, Inc.
Causes of Anemia
2. Low hemoglobin content
• Iron-deficiency anemia
• Secondary result of hemorrhagic anemia or
• Inadequate intake of iron-containing foods or
• Impaired iron absorption
• Heavy menstruation

Copyright © 2010 Pearson Education, Inc.
Causes of Anemia
• Pernicious anemia
•Deficiency of vitamin B12
•Lack of intrinsic factor needed for absorption of B12
•Treated by intramuscular injection of B12 or application of Nascobal
•Common in elderly and those with GI disorders that cause malabsorption, like Crohn’s, IBD, etc.

Copyright © 2010 Pearson Education, Inc.
Causes of Anemia
3. Abnormal hemoglobin
• Thalassemias
• Absent or faulty globin chain
• RBCs are thin, delicate, and deficient in hemoglobin

Copyright © 2010 Pearson Education, Inc.
Causes of Anemia
• Sickle-cell anemia
•Defective gene codes for abnormal hemoglobin (HbS)
•Causes RBCs to become sickle shaped in low-oxygen situations

Copyright © 2010 Pearson Education, Inc. Figure 17.8
1 2 3 4 5 6 7 146
1 2 3 4 5 6 7 146
(a) Normal erythrocyte has normal hemoglobin amino acid sequence in the beta chain.
(b) Sickled erythrocyte results from a single amino acid change in the beta chain of hemoglobin.

Copyright © 2010 Pearson Education, Inc.
Erythrocyte Disorders
•Polycythemia: excess of RBCs that increase blood viscosity
•Results from:
• Polycythemia vera—bone marrow cancer
• Secondary polycythemia—when less O2 is available (high altitude) or when EPO production increases

Copyright © 2010 Pearson Education, Inc.
Leukocytes or WBCs

Copyright © 2010 Pearson Education, Inc.
Leukocytes
•Make up <1% of total blood volume
•Can leave capillaries via diapedesis
•Move through tissue spaces by ameboid motion and positive chemotaxis (toward a chemical stimulus)
•Normal range: 4-11,000/mm3
•Leukocytosis: WBC count over 11,000/mm3
•Normal response to bacterial or viral invasion

Copyright © 2010 Pearson Education, Inc. Figure 17.9
Formedelements
Platelets
Leukocytes
Erythrocytes
DifferentialWBC count(All total 4800 –10,800/l)
Neutrophils (50 – 70%)
Lymphocytes (25 – 45%)
Eosinophils (2 – 4%)
Basophils (0.5 – 1%)
Monocytes (3 – 8%)
Agranulocytes
Granulocytes

Copyright © 2010 Pearson Education, Inc.
Granulocytes
•Granulocytes: neutrophils, eosinophils, and basophils
•Cytoplasmic granules stain specifically with Wright’s stain
• Larger and shorter-lived than RBCs
• Lobed nuclei
• Phagocytic

Copyright © 2010 Pearson Education, Inc.
Neutrophils
•Most numerous WBCs
•Aka polymorphonuclear leukocytes (PMNs)
•Granules contain hydrolytic enzymes or defensins
•Very phagocytic—“bacteria slayers”
•THE MARINES “FIRST ONES IN”

Copyright © 2010 Pearson Education, Inc.
Eosinophils
•Red to crimson (acidophilic) coarse, lysosome-like granules
•Allergies and digest parasitic worms that are too large to be phagocytized

Copyright © 2010 Pearson Education, Inc.
Basophils
•Rarest WBCs
•Large, purplish-black (basophilic) granules contain histamine
•Histamine: an inflammatory chemical that acts as a vasodilator and attracts other WBCs to inflamed sites
•Are functionally similar to mast cells

Copyright © 2010 Pearson Education, Inc. Figure 17.10 (a-c)
(a) Neutrophil; multilobed nucleus
(b) Eosinophil; bilobed nucleus, red cytoplasmic granules
(c) Basophil; bilobed nucleus, purplish-black cytoplasmic granules

Copyright © 2010 Pearson Education, Inc.
Agranulocytes
•Agranulocytes: lymphocytes and monocytes
• Lack visible cytoplasmic granules
•Have spherical or kidney-shaped nuclei

Copyright © 2010 Pearson Education, Inc.
Lymphocytes
•Large, dark-purple, circular nuclei with a thin rim of blue cytoplasm
•Mostly in lymphoid tissue; few circulate in the blood
•Crucial to immunity

Copyright © 2010 Pearson Education, Inc.
Lymphocytes
•Two types
• T cells act against virus-infected cells and tumor cells (cell mediated immune response)
• B cells give rise to plasma cells, which produce antibodies (humoral immune response)

Copyright © 2010 Pearson Education, Inc.
Monocytes
•The largest leukocytes
•Abundant pale-blue cytoplasm
•Dark purple-staining, U- or kidney-shaped nuclei

Copyright © 2010 Pearson Education, Inc.
Monocytes
•Leave circulation, enter tissues, and differentiate into macrophages
• Actively phagocytic cells; crucial against viruses, intracellular bacterial parasites, and chronic infections
•Activate lymphocytes to mount an immune response

Copyright © 2010 Pearson Education, Inc. Figure 17.10d, e
(d) Small lymphocyte; large spherical nucleus
(e) Monocyte; kidney-shaped nucleus

Copyright © 2010 Pearson Education, Inc. Table 17.2 (1 of 2)

Copyright © 2010 Pearson Education, Inc.
Leukopoiesis
•Production of WBCs
•Stimulated by chemical messengers from bone marrow and mature WBCs
• Interleukins (e.g., IL-1, IL-2)
•All leukocytes originate from hemocytoblasts

Copyright © 2010 Pearson Education, Inc. Figure 17.11
Hemocytoblast
Myeloid stem cell Lymphoid stem cell
Myeloblast Myeloblast MonoblastMyeloblast Lymphoblast
Stem cells
Committedcells
Promyelocyte PromyelocytePromyelocyte Promonocyte Prolymphocyte
Eosinophilicmyelocyte
Neutrophilicmyelocyte
Basophilicmyelocyte
Eosinophilicband cells
Neutrophilicband cells
Basophilicband cells
Developmentalpathway
Eosinophils NeutrophilsBasophils
Granular leukocytes
(a) (b) (c) (d) (e)Monocytes Lymphocytes
Agranular leukocytes
Some becomeSomebecome

Copyright © 2010 Pearson Education, Inc.
Leukocyte Disorders
•Leukopenia
• Abnormally low WBC count—drug/toxin induced
•Leukemias
• Cancerous conditions involving WBCs
• Named according to the abnormal WBC clone involved
• Myelocytic leukemia involves myeloblasts
• Lymphocytic leukemia involves lymphocytes
•Acute leukemia involves blast-type cells and primarily affects children
•Chronic leukemia is more prevalent in older people

Copyright © 2010 Pearson Education, Inc.
Leukemia
•Bone marrow totally occupied with cancerous leukocytes
•Immature nonfunctional WBCs in the bloodstream
•Death caused by internal hemorrhage and overwhelming infections
•Treatments include irradiation, antileukemic drugs, and stem cell transplants

Copyright © 2010 Pearson Education, Inc.
Platelets

Copyright © 2010 Pearson Education, Inc.
Platelets
•Form a temporary platelet plug that helps seal breaks in blood vessels
•Circulating platelets are kept inactive and mobile by NO (nitric oxide) and prostacyclin from endothelial cells of blood vessels

Copyright © 2010 Pearson Education, Inc. Figure 17.12
Stem cell Developmental pathway
Hemocyto-blast Megakaryoblast
PromegakaryocyteMegakaryocyte Platelets

Copyright © 2010 Pearson Education, Inc.
Hemostasis

Copyright © 2010 Pearson Education, Inc.
Hemostasis
• Fast series of reactions for stoppage of bleeding
1. Vascular spasm
2. Platelet plug formation
3. Coagulation (blood clotting)

Copyright © 2010 Pearson Education, Inc.
Vascular Spasm
•Vasoconstriction of damaged blood vessel
•Triggers
•Direct injury
•Chemicals released by endothelial cells and platelets
• Pain reflexes

Copyright © 2010 Pearson Education, Inc. Figure 17.13
Collagenfibers
Platelets
Fibrin
Step Vascular spasm• Smooth muscle contracts, causing vasoconstriction.
Step Platelet plugformation
• Injury to lining of vessel exposes collagen fibers; platelets adhere.
• Platelets release chemicals that make nearby platelets sticky; platelet plug forms.
Step Coagulation• Fibrin forms a mesh that traps red blood cells and platelets, forming the clot.
1
2
3

Copyright © 2010 Pearson Education, Inc.
Coagulation
• A set of reactions in which blood is transformed from a liquid to a gel
• Reinforces the platelet plug with fibrin threads

Copyright © 2010 Pearson Education, Inc.
Coagulation

Copyright © 2010 Pearson Education, Inc.
Coagulation
• Three phases of coagulation
1. Prothrombin activator is formed (intrinsic and extrinsic pathways)
2. Prothrombin is converted into thrombin
3. Thrombin catalyzes the joining of fibrinogen to form a fibrin mesh

Copyright © 2010 Pearson Education, Inc. Figure 17.14 (1 of 2)
Vessel endothelium ruptures,exposing underlying tissues(e.g., collagen)
PF3
released byaggregated
platelets
XII
XI
IX
XIIa
Ca2+
Ca2+
XIa
IXa
Intrinsic pathwayPhase 1Tissue cell traumaexposes blood to
Platelets cling and theirsurfaces provide sites formobilization of factors
Extrinsic pathway
Tissue factor (TF)
VII
VIIa
VIII
VIIIa
Ca2+
X
Xa
Prothrombinactivator
PF3
TF/VIIa complexIXa/VIIIa complex
V
Va

Copyright © 2010 Pearson Education, Inc. Figure 17.14 (2 of 2)
Ca2+
Phase 2
Phase 3
Prothrombinactivator
Prothrombin (II)
Thrombin (IIa)
Fibrinogen (I)(soluble)
Fibrin(insolublepolymer) XIII
XIIIa
Cross-linkedfibrin mesh

Copyright © 2010 Pearson Education, Inc.
CLOTTING PATHWAYS
Measured by: PTT
Drugs: Heparin
Measured by PT/INRDrugs: Warfarin, ASA, Vitamin-E, EFA’sFactor
s 2-7-9-10
PROTHROMBIN ACTIVATOR made up of V&X: Started by X alone and V becomes active with + feedback
Extrinsic Pathway: Damage outside of blood vessels.
Intrinsic Pathway:Blood trauma (turbulence and viscosity) or collagen and blood contact.

Copyright © 2010 Pearson Education, Inc. Figure 17.15

Copyright © 2010 Pearson Education, Inc.
Clot Retraction
•Actin and myosin in platelets contract within 30–60 minutes
•Platelets pull on the fibrin strands, squeezing serum from the clot

Copyright © 2010 Pearson Education, Inc.
Clot Repair
•Platelet-derived growth factor (PDGF) stimulates division of smooth muscle cells and fibroblasts to rebuild blood vessel wall
•Vascular endothelial growth factor (VEGF) stimulates endothelial cells to multiply and restore the endothelial lining

Copyright © 2010 Pearson Education, Inc.
Fibrinolysis
•Begins within two days
•Plasminogen in clot is converted to plasmin by tissue plasminogen activator (tPA), factor XII and thrombin
•Plasmin is a fibrin-digesting enzyme

Copyright © 2010 Pearson Education, Inc.
Factors Preventing Undesirable Clotting
•Platelet adhesion is prevented by
• Smooth endothelial lining of blood vessels
• Antithrombic substances nitric oxide and prostacyclin secreted by endothelial cells
• Vitamin E quinine, which acts as a potent anticoagulant

Copyright © 2010 Pearson Education, Inc.
Disorders of Hemostasis
•Thromboembolytic disorders: undesirable clot formation
•Bleeding disorders: abnormalities that prevent normal clot formation

Copyright © 2010 Pearson Education, Inc.
Thromboembolytic Conditions
•Thrombus: clot that develops and persists in an unbroken blood vessel
•May block circulation, leading to tissue death
•Embolus: a thrombus freely floating in the blood stream
• Pulmonary emboli impair the ability of the body to obtain oxygen
•Cerebral emboli can cause strokes

Copyright © 2010 Pearson Education, Inc.
Thromboembolytic Conditions
• Prevented by
• Aspirin
•Antiprostaglandin that inhibits thromboxane A2
• Heparin
•Anticoagulant used clinically for pre- and postoperative cardiac care
• Warfarin
•Used for those prone to atrial fibrillation

Copyright © 2010 Pearson Education, Inc.
Disseminated Intravascular Coagulation (DIC)
•Widespread clotting blocks intact blood vessels
•Severe bleeding occurs because residual blood unable to clot
•Most common in pregnancy, septicemia, or incompatible blood transfusions

Copyright © 2010 Pearson Education, Inc.
Bleeding Disorders
•Thrombocytopenia: deficient number of circulating platelets
• Petechiae appear due to spontaneous, widespread hemorrhage
•Due to suppression or destruction of bone marrow (e.g., malignancy, radiation)
• Platelet count <50,000/mm3 is diagnostic
• Treated with transfusion of concentrated platelets

Copyright © 2010 Pearson Education, Inc.
Bleeding Disorders
•Impaired liver function
• Inability to synthesize procoagulants
•Causes include vitamin K deficiency, hepatitis, and cirrhosis
• Liver disease can also prevent the liver from producing bile, impairing fat and vitamin K absorption

Copyright © 2010 Pearson Education, Inc.
Bleeding Disorders
•Hemophilias include several similar hereditary bleeding disorders
• Hemophilia A: most common type (77% of all cases); due to a deficiency of factor VIII
• Hemophilia B: deficiency of factor IX
• Hemophilia C: mild type; deficiency of factor XI
•Symptoms include prolonged bleeding, especially into joint cavities
•Treated with plasma transfusions and injection of missing factors

Copyright © 2010 Pearson Education, Inc.
Transfusions
•Whole-blood transfusions are used when blood loss is substantial
•Packed red cells (plasma removed) are used to restore oxygen-carrying capacity
•Transfusion of incompatible blood can be fatal

Copyright © 2010 Pearson Education, Inc.
Blood Types

Copyright © 2010 Pearson Education, Inc.
Blood Groups
•Humans have 30 varieties of naturally occurring RBC antigens
•Antigens of the ABO and Rh blood groups cause vigorous transfusion reactions
•Other blood groups (MNS, Duffy, Kell, and Lewis) are usually weak agglutinogens

Copyright © 2010 Pearson Education, Inc.
ABO Blood Groups
•Types A, B, AB, and O
•Based on the presence or absence of two agglutinogens (A and B) on the surface of the RBCs
•Blood may contain anti-A or anti-B antibodies (agglutinins) that act against transfused RBCs with ABO antigens not normally present
•Anti-A or anti-B form in the blood at about 2 months of age

Copyright © 2010 Pearson Education, Inc. Table 17.4

Copyright © 2010 Pearson Education, Inc.
Rh Blood Groups
•There are 45 different Rh agglutinogens (Rh factors)
•C, D, and E are most common
•Rh+ indicates presence of D
•Rh+ = 85% of the population
•Rh- = 15% of the population

Copyright © 2010 Pearson Education, Inc.
Rh Blood Groups
•Anti-Rh antibodies are not spontaneously formed in Rh– individuals
•Anti-Rh antibodies form if an Rh– individual receives Rh+ blood
•A second exposure to Rh+ blood will result in a typical transfusion reaction

Copyright © 2010 Pearson Education, Inc.
Homeostatic Imbalance: Hemolytic Disease of the Newborn
•Also called erythroblastosis fetalis
•Rh– mother becomes sensitized when exposure to Rh+ blood causes her body to synthesize anti-Rh antibodies
•Anti-Rh antibodies cross the placenta and destroy the RBCs of an Rh+ baby

Copyright © 2010 Pearson Education, Inc.
Homeostatic Imbalance: Hemolytic Disease of the Newborn
•The baby can be treated with prebirth transfusions and exchange transfusions after birth
•RhoGAM serum containing anti-Rh can prevent the Rh– mother from becoming sensitized

Copyright © 2010 Pearson Education, Inc.
ABO Blood Typing
Blood Type Being Tested
RBC Agglutinogens
Serum Reaction
Anti-A Anti-B
AB A and B + +
B B – +
A A + –
O None – –

Copyright © 2010 Pearson Education, Inc. Figure 17.16
SerumAnti-A
RBCs
Anti-B
Type AB (containsagglutinogens A and B;agglutinates with bothsera)
Blood being tested
Type A (containsagglutinogen A;agglutinates with anti-A)
Type B (containsagglutinogen B;agglutinates with anti-B)
Type O (contains noagglutinogens; does notagglutinate with eitherserum)

Copyright © 2010 Pearson Education, Inc.
Restoring Blood Volume
•Death from shock may result from low blood volume
•Volume must be replaced immediately with
• Normal saline or multiple-electrolyte solution that mimics plasma electrolyte composition
• Plasma expanders (e.g., purified human serum albumin, hetastarch, and dextran)
•Mimic osmotic properties of albumin
•More expensive and may cause significant complications

Copyright © 2010 Pearson Education, Inc.
Diagnostic Blood Tests
•Hematocrit
•Blood glucose tests
•Microscopic examination reveals variations in size and shape of RBCs, indications of anemias
•RBCs too big = macrocytic anemia (B12/folic acid deficiency, etc.)
•RBCs too small = microcytic anemia (iron deficiency, thalassemia, etc.)

Copyright © 2010 Pearson Education, Inc.
Diagnostic Blood Tests
•Differential WBC count
•Prothrombin time (PTT) and platelet counts assess hemostasis
•SMAC (or CMP), a blood chemistry profile
•Complete blood count (CBC)

Copyright © 2010 Pearson Education, Inc.
Developmental Aspects
•Fetal blood cells form in the fetal yolk sac, liver, and spleen
•Red bone marrow is the primary hematopoietic area by the seventh month
•Blood cells develop from mesenchymal cells called blood islands
•The fetus forms HbF, which has a higher affinity for O2 than hemoglobin A formed after birth

Copyright © 2010 Pearson Education, Inc.
Developmental Aspects
•Blood diseases of aging
•Chronic leukemias, anemias, clotting disorders
•Usually precipitated by disorders of the heart, blood vessels, and immune system

Copyright © 2010 Pearson Education, Inc.
QUESTIONS TO TEST WHAT YOU NOW KNOW!!!

Copyright © 2010 Pearson Education, Inc.
Which of the following comprise a logical sequence of vessels as blood exits the heart?
A. Capillaries, arteries, veins
B. Veins, capillaries, arteries
C. Arteries, capillaries, veins
D. Arteries, veins, capillaries

Copyright © 2010 Pearson Education, Inc.
After centrifuging, of the listed blood components, which contains the components of immune function?
A. Plasma
B. Buffy coat
C. Erythrocytes
D. Hematocrit

Copyright © 2010 Pearson Education, Inc.
The major function of the most common plasma protein, albumin, is __________.
A. maintenance of plasma osmotic pressure
B. buffering changes in plasma pH
C. fighting foreign invaders
D. both a and b

Copyright © 2010 Pearson Education, Inc.
Red blood cells are efficient oxygen transport cells. Of the following characteristics, which is the major contributor to the significant oxygen-carrying capacity of a red blood cell?
A. Red blood cells lack mitochondria.
B. Red blood cells don’t divide.
C. Red blood cells are biconcave discs.
D. Red blood cells contain myoglobin.

Copyright © 2010 Pearson Education, Inc.
Each hemoglobin can transport ________ oxygen atoms.
A. 4
B. 40
C. 400
D. 4000

Copyright © 2010 Pearson Education, Inc.
Oxygen binds to the _______ portion of hemoglobin.
A. globin
B. oxyhemoglobin
C. iron atom
D. amino acid

Copyright © 2010 Pearson Education, Inc.
A patient with low iron levels would experience which of the following symptoms?
A. An increased white blood cell count
B. An increase in energy level
C. An increase in fatigue
D. A decreased white blood cell count

Copyright © 2010 Pearson Education, Inc.
A hematopoietic stem cell will give rise to __________.
A. erythrocytes
B. leukocytes
C. platelets
D. all of the above

Copyright © 2010 Pearson Education, Inc.
Predict the outcome of an overdose of the hormone erythropoietin.
A. The blood viscosity increases to levels that may induce heart attacks or strokes.
B. The oxygen-carrying capacity remains unchanged despite elevated red blood cell counts.
C. Red blood cell counts remain unchanged, but the number of reticulocytes increases.
D. Blood viscosity levels decrease while oxygen-carrying capacity increases.

Copyright © 2010 Pearson Education, Inc.
What response would you expect after traveling to high altitude for two weeks?
A. Blood levels of oxygen would remain depressed for the duration.
B. A surge in iron release from the liver would occur.
C. The kidneys would secrete elevated amounts of erythropoietin.
D. There would be no change in blood composition.

Copyright © 2010 Pearson Education, Inc.
If a patient has pernicious anemia, the inability of the body to absorb vitamin B12, the patient __________.
A. would have reduced blood iron levels
B. would have a decreased number of red blood cells
C. would have increased levels of hemoglobin
D. would not experience any effects on red blood cells

Copyright © 2010 Pearson Education, Inc.
Which of the following statements is true regarding the mechanism controlling movement of white blood cells into damaged areas?A. White blood cells exit the capillary and move
through the tissue spaces with cytoplasmic extensions by following a trail of chemicals produced by other white blood cells.
B. Capillaries break open, flooding a damaged area with white blood cells.
C. The damaged tissues synthesize their own white blood cells.
D. None of the statements are true.

Copyright © 2010 Pearson Education, Inc.
An elevated neutrophil count would be indicative of ________.
A. an allergic reaction
B. a cancer
C. an acute bacterial infection
D. a parasitic infection

Copyright © 2010 Pearson Education, Inc.
Antihistamines counter the actions of which white blood cells?
A. Neutrophils
B. Lymphocytes
C. Basophils
D. Eosinophils

Copyright © 2010 Pearson Education, Inc.
Leukemia is a general descriptor for which of the following disorders?
A. An abnormally low white blood cell count
B. Overproduction of abnormal leukocytes
C. Elevated counts of normal neutrophils
D. Overproduction of abnormal erythrocytes

Copyright © 2010 Pearson Education, Inc.
A __________ is the progenitor of platelets.
A. thrombopoietin
B. thrombocyte
C. megakaryocyte
D. thrombocytoblast

Copyright © 2010 Pearson Education, Inc.
Why don’t platelets form plugs in undamaged vessels?
A. Platelets aren’t formed until vessel damage occurs.
B. Only contact of platelets with exposed collagen fibers and von Willebrand factor causes them to be sticky and form plugs.
C. Plugs do form, but are removed by macrophages.
D. Platelets don’t form plugs, it is the megakaryocytes that form the plugs.

Copyright © 2010 Pearson Education, Inc.
Activation of the extrinsic pathway of coagulation requires exposure of the blood to _________.
A. collagen
B. tissue factor III
C. prothrombin activator
D. serotonin

Copyright © 2010 Pearson Education, Inc.
Why doesn’t a clot fill the entire vasculature system once it has started forming?
A. Rapid blood flow washes away and dilutes activated clotting factors.
B. Thrombin is inactivated by antithrombin III if it enters the general circulation.
C. Both a and b occur.
D. Neither a nor b occurs.

Copyright © 2010 Pearson Education, Inc.
An oral heparin medication might be prescribed for a patient who:
A. is at risk for embolism (clots that spontaneously form and wedge in blood vessels).
B. has thrombocytopenia.
C. is a hemophiliac.
D. has a deficiency in a clotting factor.

Copyright © 2010 Pearson Education, Inc.
Why is it possible for a person with type A negative blood to have a negative reaction when receiving a transfusion of whole type O negative blood?
A. Some type O cells possess B agglutinogens on their surface.
B. The Rh factor would cross-react.
C. Blood transfusions can only occur within the same blood group.
D. The type O blood may have high enough levels of anti-A antibodies that could cross-react with the recipient’s cells.