Embed Size (px)
Citation preview

PotassiumKate Driver BMLSc MAACB
Immunochemistry Product Manager ANZ PIDiasorin Australia
[email protected] QLD Branch Education Representative
Australasian Association of Clinical Biochemists

AACB Curriculum

AACB questions

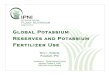
Total Body Potassium
• Potassium is the major intracellular cation ~ concentration of 150 mmol/L
• Potassium is tightly regulated in the extracellular fluid at 3.5 - 5 mmol/L
• Total body potassium concentration is ~ 3000 mmol

Fluid Space Potassium

Why is Potassium soimportant?
Potassium is the major intracellular ion and the differencebetween the ICF/ECF concentrations is responsible for thedifference in potential across the cell membrane.
This potential is referred to as the Resting Membrane Potential (RMP).Changes in the RMP cause Hyper ( K+) or Hypoexcitability ( K+) ofcells and is a significant issue in myocytes where contractionand relaxation cycles are altered (twitch).
Clinical sequalae arise mainly due to changes in ‘twitch’.


Potassium HomeostasisMajor factors in maintaining potassium homeostasis
Adequate Dietary Intake• Due to ‘compulsory’ renal and GI loss, dietary intake is important• Daily losses are more or less equal to daily dietary intake
Intracellular/Extracellular shifts• Potassium is the major intracellular cation, but is constantly redistributed.
Certain drugs, physiological conditions and acid base balance allcontribute to the ICF/ECF concentration of K.
Renal regulation• Two most important physiological determinants of potassium excretion are
the serum aldosterone concentration and the delivery of sodium tothe distal nephron.
http://hkpp.org/patients/potassium-health

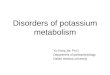
Potassium HomeostasisIntracellular/Extracellular shifts
Potassium redistributed between the ECF and ICF can occur quickly and isimportant in the daily maintenance of ECF – eg. during ingestion of K+
Potassium shifts occur in:
• Alkalosis/Acidosis• Insulin and catecholamines (Normal physiology or pathological)• Rapid Cellular proliferation disorders• Thyrotoxicosis
Via the activation of the NaKATPase pump or NaH Transporter
Electrolyte Quintet - Potassium - Mitchell L Halperin, Kamel S Kamel

Potassium HomeostasisRenal Regulation
Renal regulation of potassium is a slower acting mechanism and fine tunes theextracellular concentration
Renal Potassium reabsorption/secretion is dependent on the following factors:
• Amount of Na available for transportation or excretion
• Relative availability of Hydrogen and Potassium ions in the distalconvoluted tubules
• Ability of the distal convoluted tubules to excrete Hydrogen ions
• Circulating Concentration of Aldosterone
• The flow rate of tubular fluid - high flow rate favours transfer ofpotassium to lumen
Clinical Chemistry - William J Marshall, Stephen K Bangert

Potassium HomeostasisRenal Regulation

Potassium HomeostasisRenal Regulation
Harrisons Principles of Internal Medicine - 19th Edition
Aldosterone

Potassium HomeostasisRenin Angiotensin Aldosterone (RAA)
• The Renin, Angiotensin, Aldosterone (RAA) system is animportant regulator of Na+ and K+ and assessment of thissystem is an important part of investigating dyskalaemia
• Aldosterone is produced in response to angiotensin II, butalso in response to Hyperkalaemia.
• These two mechanisms are a ‘selective’ process to retainNaCl or to promote kaliuresis.

Potassium HomeostasisActions of Aldosterone
Electrolyte Quintet - Potassium - Mitchell L Halperin, Kamel S Kamel

Potassium HomeostasisRAA system

Urine analysis- Investigating Dyskalaemia
• The investigation of any electrolyte imbalance without anobvious cause will probably require urine analysis.
• Tests that are immediately useful are K+ Na+ Cl- Osmolality,pH (Calculate anion gap from plasma results)
• It is important to establish if the nephron’s are handling K+ appropriatelyregardless of the initial presentation.
Eg. A patient who has been sweating excessively who displayspersistent hypokalaemia after fluid correction may demonstrateinappropriate renal excretion of potassium, suggesting anunderlying renal handling issue.

Urinary Potassium tests
Electrolyte Quintet - Potassium - Mitchell L Halperin, Kamel S Kamel

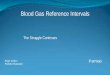
Urine Potassium TestingTrans-Tubular Potassium Gradient (TTKG)
The TTKG calculation reflects the conservation – or lack there of – of Potassium inthe CCD. It is useful in identifying the causes of hyperkalaemia or hypokalemia andindirectly assesses the action of mineralocorticoid in the CCD.
It is a ratio/index that estimates the amount of potassium in the lumen of the CCDcompared to that in peritubular capillaries.
The following is the formula for calculating the TTKG:
Note that this formula is valid only when Uosm >300 and UNa >25
The validity of this measurement falls on three assumptions:
(1) Few solutes are reabsorbed in the medullary collecting duct (MCD)
(2) Potassium is neither secreted nor reabsorbed in the MCD
(3)The osmolality of the fluid in the terminal CCD is known

Urine Potassium TestingTrans-Tubular Potassium Gradient (TTKG)Significant reabsorption or secretion of K in the MCD seldom occurs,except in profound K depletion or excess, respectively.
A typical TTKG in a normal person on a normal diet is 8-9. Duringhyperkalemia or high potassium intake, more potassium should beexcreted in the urine and the TTKG should be above 10. Low levels (<7)during hyperkalemia may indicate mineralocorticoid deficiency,especially if accompanied by hyponatremia and high urine Na.
During potassium depletion or hypokalemia, the TTKG should fall toless than 3, indicating appropriately reduced urinary excretion ofpotassium.

HypokalaemiaHypokalaemia - Results in an increase of the RMP, decreasing the excitability
• Muscle fatigue/weakness• Constipation• Paralytic Ilieus• Hypotonia• Depression• Confusion
• Changes to ECG - S,T segment changes• Potentiation of Digoxin therapy• Arrythmia
• Inability to concentrate urine - polyuria

HypokalaemiaCauses of Hypokalaemia
• Inadequate Dietary intact• Poor diet/alcoholism (Mg def)• Parental nutrition
• Intracellular shifts• Alkalosis• Insulin therapy• Excessive catecholamines• Rapid cellular proliferation
• Increased K excretion• Renal
• Renal failure - using diuretics• Acute renal failure with diuresis• Excess Mineralcorticoids/Glucocorticoids
• Primary aldosteronism• Secondary aldosteronism• Cushings• Carbenoxolone - liquorice ingestion• Renal tubular acidosis (types 1 and 2)
• Extrarenal• Laxatives/diarrhoea• Vomiting/gastric aspiration• Sweating• Villious Adenoma of the large bowel• Subcutaneous fistula
Clinical Chemistry - William J Marshall, Stephen K Bangert

HypokalaemiaIntracellular Shift
During alkalosis, H+ is retained at the kidneys to buffer the excess HCO3
Mechanism• Both the H+K+ATPase and H+ATPase both work to retain H+ ions• H+K+ATPase results in direct exchange of H+ for K+• H+ only transports H+ the K+ moves to retain electroneutrality
(refer back to slide demonstrating channels)
Important concept as this is the mechanism for hypokalaemia duringprotracted vomiting where large amounts of HCL are lost from the gut.The kidneys ‘waste’ the potassium to retain H+.
Pylori stenosis in infants requires rapid diagnosis and treatment –
Hypokalemic Hypochloremic Metabolic Alkalosis.

HypokalaemiaExcess Mineralocorticoid

Mechanisms of Highmineralocorticoid levels
1. High Renin, High AldosteroneSecondary Hyperaldosteronism
2. High Aldosterone -low reninPrimary Aldosteronism
3. Stimulation by ACTH - ectopic production - tumour
4. Exogenous steroids
5. Fast uptake of Na- increased Lumen negative potential
6. Inhibition of 11 bHSDH- continued action of Cortisol promoting
uptake of Na from the lumen7. Increased permeability/channel availabilityfor Transportation of Na
Electrolyte Quintet - Potassium - Mitchell L Halperin, Kamel S Kamel

HypokalaemiaRenal Tubular Acidosis
Characterised by hypokalaemia with a normal anion gap acidosis
Type 1: Classical Distal RTA is failure to excrete hydrogen ionsGenetic causesAutoimmune - eg. Sorjens or Lupus
Type 2: Classical Proximal RTA is failure to absorb HCO3Faconi’s DiseaseIfosfamide - chemotherapyMultiple MyelomaChronic Kidney Rejection
Type 4: Hyperkalemic RTA – inability to excrete Ammonia (results inNon-anion gap metabolic acidosis)
Many drugs in antibiotics, Diuretics, NSAIDsStructurally altered kidneyHIVDiabetic NeuropathyAmyloidTransplant

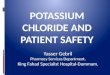
Sonic Pathology Handbook –Evaluation of Hypokalaemia


HypokalaemiaActions of Diueretics

HyperkalaemiaClinical effects
Hyperkalaemia results in a decrease in the RMP, leading to increasedexcitability of cells
Clinical consequences/effects are all about myocardial function
•sinus bradycardia•sinus arrest•slow idioventricular rhythms•ventricular tachycardia•ventricular fibrillation•asystole
Requires rapid diagnosis and treatment

HyperkalaemiaSpurious
HaemolysisDelay in separationCold samplePatient preparation
Excess intakeOral - rare - except with diureticsParental nutritionBlood transfusion - old blood
RedistributionCellular death/damageCatabolic statesSystemic acidosisInsulin lack
Decreased excretionRenal
Potassium sparing diureticsAddisons - not usually pituitaryHyporenemic hypoaldosteronismACE inhibitors
Clinical Chemistry - William J Marshall, Stephen K Bangert

Sonic Pathology Handbook –Evaluation of Hyperkalaemia


Recommended Reading

• The Electrolyte Quintet - www.oocities.org/mim_nephro/LancetK.pd
• The Utility of the Transtubular Potassium Gradient in the Evaluation of Hyperkalemia Michael J. Choi*and Fuad N. Ziyadeh† *Department of Medicine, Johns Hopkins University School of Medicine,Baltimore, Maryland; and † Departments of Internal Medicine and Physiology, Faculty of Medicine,American University of Beirut, Beirut, Lebanon
• AACB CPC 2013 Potassium disturbances - interpretation using bicarbonate
Andrea Rita Horvath, SEALS Department of Clinical Chemistry Prince of Wales Hospital, Sydney
Useful Links and Sites