Embed Size (px)
DESCRIPTION
postural hypotension
Citation preview

postural hypotension:causesadministration of drugsprolonged recumbencyinadequate posttural reflexlate stage pregnancyadvanced agevenous defects in legaddison s diseaseexhauustionchronic postural hypotension or shy drager syndrome
In general, drugs produce postural hypotension by diminishing the body�s ability to maintain blood pressure (and in turn adequate cerebral perfusion) in response to the increased influence of gravity that occurs when the patient rises suddenly. An exaggerated blood pressure response is observed
during pregnancy" In the first, the woman experiences postural hypotension during the first trimester; this usually occurs when she rises from bed in the morning but does not recur during the day. The precise cause of this phenomenon is not known.The second form, known as the supine hypotensive syndrome of pregnancy,occurs late in the third trimester if the woman remains in the supine position for more than 3 to 7 minutes.
In the first, the woman experiences postural hypotension during the first trimester; this usually occurs when she rises from bed in the morning but does not recur during the day. The precise cause of this phenomenon is not known.The second form, known as the supine hypotensive syndrome of pregnancy,occurs late in the third trimester
if the woman remains in the supine position for more than 3 to 7 minutes.
Postural hypotension may be detectable if the patient�s blood pressure and heart rate are recorded in both the supine and standing positions, something that is rarely done in most medical or dental practices. The doctor should record the first blood pressure reading after the patient has been in a supine position for 2 to 3 minutes and the second after the patient has been standing for 1 minute.
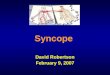
PATHOPHYSIOLOGYNormal regulatory mechanismsWhen the patient changes from a supine to an upright position, the influence of gravity on the cardiovascular system intensifies. Blood pumped from the heart must now move upward, against gravity, to reach the cerebral

circulation to supply the brain with the O2and glucose it needs to maintain consciousness. On the other hand, with the patient in the supine position the force of gravity is distributed equally over the entire body and blood flows more readily from the heart to the brain. With other positions (e.g., semisupine, Trendelenburg), gravity�s effect is usually such that systolic blood pressure decreases by 2 mm Hg for each 25 mm (1 inch) that the patient�s head is situated above the level of the heart; for each 25 mm (1 inch) that the head is situated below the level of the heart, blood pressure increases by 2 mm Hg (Figure 7-1).A number of intricate mechanisms have evolved to protect the brain and ensure that it receives an adequate supply of O2and glucose.24These include the following:¦A reflex arteriolar constriction mediated through baroreceptors (pressure receptors) located in the carotid sinus and aortic arch¦A reflex increase in heart rate, which occurs simultaneously with the increase in arteriolar tone and is mediated through the same mechanisms¦A reflex venous constriction that increases the return of venous blood to the heart, mediated both intrinsically and sympathetically¦ An increase in muscle tone and contraction in the legs and abdomen�the so-called venous pump�facilitating the return of venous blood (of vitalimportance because at least 60% of circulating blood volume at any given moment is in venous circulation)¦A reflex increase in respiration, which also aids in the return of blood to the right side of the heart via changes in intraabdominal and intrathoracic pressures¦ The release into the blood of various neurohumoral substances, such as norepinephrine, antidiuretic hormone, renin, and angiotensin
management:Step 1:assessment of consciousnessStep 2:activation of the office emergency system.Step 3:P (position)tep 4: A?B?C (airway-breathing-circulation
Step 5:D (definitive care).Step 5a:administration of O2Step 5b:monitoring of vital signsStep 6:subsequent managementStep 6a:delayed recovery'Step 7:discharge