Embed Size (px)
Citation preview

A O R N J O U R N A L MARCH 1986, VOL. 43, NO 3
Postoperative Pain ALTERING THE PATIENT'S EXPERIENCE THROUGH EDUCATION
Cynthia A. Bray, RN
ain. The word is derived from ,the Greek poine and the Latin poene, meaning P punishment or penalty. Its mysterious
components have been problematic since prehis- toric times when ancient civilizations viewed it as the gods' retribution for mortal wrongdoings. Aristotle was the first to study pain's etiology and he believed it to be a feeling that originated in the skin (from excessive stimuli), traveled to the heart via the blood, and was interpreted by the heart. Descartes, on the other hand, postulated that pain was caused by noxious stimuli that caused vibrations in the skin, which in turn traveled to the brain via delicate threads.'
Descartes was close to the truth, for as we now know, pain is transmitted to the central nervous system (CNS) via several parallel pathways. Other CNS structures interact with those pathways and can modify the perception of any noxious stimuli. Pain is also a subjective perception and is affected by emotional, experiential, and environmental factors. Thus, pain can be thought of as a triad of independent variables: noxious stimulus, emotional input, and individual interpretations.
Acute Pain
ecause the most common cause of acute pain is surgery, postoperative pain can serve B as a model for study.* Acute pain serves
as an alarm when the body sustains tissue damage. All surgical intervention traumatizes tissues; the type of pain that results depends on the site and type of surgery.
The postoperative pain related to abdominal
surgery usually arises from trauma to the abdominal wall, not to the viscera; that of thoracic surgery arises from trauma to the thoracic wall and rib cage. All inflammatory responses to surgery mobilize histamines, serotonins, kinins, and prostaglandins, all of which lower nociceptor thresholds. In addition, nerves are cut and smooth muscles become spasmodic, causing local ischemia, acidosis, and hypoxia that further reduce the pain threshold. Lowered thresholds intensify pain sensation, increase fear and anxiety, and cause the release of more pain neurotransmitters. If unrelieved, gastrointestinal complications (eg, distention, nausea, vomiting, paralytic ileus) and
Cynthia A. Bray, RN, MSEd, CNOR, i~ a head nurse and instructor in perioperative nursing at the Hospital of the University of Pennsylvania, Philadelphia She earned her master of science degree in health education from St Joseph S University, Philadelphia, her bachelor5 degree in nursing from the University of Pennsylvania, and her diploma in nursing jrom the Hahnemnn Medical College and Hospital School of Nursing, Philadelphia
672

A O R N J O U R N A L MARCH 1986, VOL. 43, NO 3
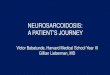
Fig 1 The Body’s Responses to Pain
Psychological Responses
Trauma/Tissue Injury
Physiological Responses
mobilization of histamines I
interpretation of kinens, etc. event
autonomic nervous anxiety system arousal emotional -
reflexive state motivational drive
+ I Pain Perception I +
Decreased
t. deep vein
t cystitis t
distention atelectasis nausea/vomiting urinary tract thrombosis hypoventilation
pneumonia ileus
t
+ I Increased Pain I
urinary problems (eg, ureteral and bladder hypomobility) may occur. Postoperative thoracic surgery complications include atelectasis and pneumonia secondary to hypoventilation, as well as the possibility of thrombosis as a result of prolonged physical immobility.
Stimuli that trigger pain can be mechanical (pressure), thermal (heat), chemical (intravenous potassium chloride), or electrical (shock). The perception of pain alerts the person to remove
himself from any life-threatening situations, and then pay attention to the extent of the injury and the alleviation of pain. Once pain has called attention to an injured area, there does not appear to be any functional value in its continuation. (Chronic pain, however, may serve a useful psychological purpose.)
The anxiety associated with acute pain is attributed to what the pain may mean: it might get worse or it might be difficult or impossible
614

A O R N J O U R N A L ___- MARCH 1986, VOL. 43, NO 3
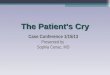
Fig 2 Major Ascending and Descending Path ways
Involved in Pain Transmission
descending control system
vasospasm
L1
to eliminate. Chronic pain is usually accompanied Anxiety usually arises from a new situation, by depression because of its continuation and effect the unknown, or from expectations of what should on the person’s lifestyle. The anxious patient and could occur. Surgery is a new experience for experiences physiological changes including many; hospital procedures constitute the unknown. increased perspiration and tachycardia. The Most patients ask, “How much will 1 hurt?” not, sympathetic response is indicative of stress (Fig “Will I hurt?” They expect the pain. Patients also 1). fear expected undignified situations (bedpans,
675

A O R N J O U R N A L ~- MARCH 1986, VOL. 43, NO 3
catheters, bodily exposure) and losing control. This anticipatory anxiety, which can occur before surgery, could have adverse effects if allowed to continue. Recent studies have shown that anticipatory anxiety is a significant predictor of postoperative pain in many ~a t i en t s .~
Concurrent anxiety occurs during situations, not after. New feelings and strange sensations are interpreted as signs of danger, infection, or deviations from the norm.
Pain Theories
arly theories of pain transmission focused on electrical rather than chemical compo- E nents: The late 1800s saw the emergence
of two opposing theories; the spenficig and the intensig theories. The specificity theory viewed pain as a specific unique sensation, independent of touch and other senses. The intensity theory emphasized stimulus intensity and central summation as determinants.
In the mid-l900s, Melzack and Wall incorpo- rated both theories into one. They also added the concept of impulse modulation occurring at various levels of the ascending afferent nerve systems. They called this theory gate contr-01.~ This outlined a more complex pain experience than the original direct-line system; it recognized pain as a net result of many interacting and dynamic neural, biochemical, physiologic, and psychologic mechanisms further influenced by culture and environment.
Four major ascending nerve pathways are involved in pain transmission. The two spinotha- lamic tracts are the main pathways (Fig 2). The lateral spinothalamic tract projects fibers that terminate in the somatosensory cortex. Before ending, they connect with the reticular nuclei of the medulla, pons, and periaqueductal gray area cells. These fibers are responsible for sensations of pain and touch. The ventral spinothalamic tract contains fibers that travel to reticular formation of the medial spinal cord, lateral pons, midbrain, and medial thalamus. Rather than discrete pain discrimination, this tract’s distal distribution to the limbic system delineates the emotional compo- nents of pain.
Neuroregulators
Acetylcholine Brad ykinin Catecholamines
Dopamine Epinephrine Norepinephrine Serotonin
B endorphins Histamine Neurotensin Prostaglandins Substance P Thyrotropin releasing hormone Vasopressin
The brain also possesses a descending system for modulation of pain transmission (Fig 2). This system is dependent on the release of neurotrans- mitters and modulators. After the discovery of the role of epinephrine and norepinephrine in neural transmission and modulation, pain theorists began researching the nervous system’s chemical components rather than its electrical aspects.
Several CNS neuroregulators alter the response to pain.6 (See “Neuroregulators.”) These secretions play an important role in our perception and response to pain, and can be modified by pharniacologic agents that block transmission to the nearby pain pathways.
Many naturally occurring neurotransmitters (endogenous opioids) and their receptors have been indentified and associated with natural pain relief. There are several types and each has a different function. The hypothesis is that an endogenous opioid system with a morphine-like substance acts as a neuroregulator. This family of endogenous opioids is commonly referred to as endorphins.
The presence of endorphins and their receptors in the CNS supports the existence of an endogenous analgesic system. This could be the reason transcutaneous electrical nerve stimulation and acupuncture reduce pain sensation for many people.
Nurses often try to separate organic and psychogenic pain, but the physiologic and
677

MARCH 1986, VOL. 43, NO 3 AORN JOURNAL
nurses to call AM admit patients to gather data and instruct them. All of these interventions take time, but we hope that through our efforts the patient may be comforted preoperatively and perceive less pain postoperatively. 0
Notes 1. R Descartes, “L‘Homme” in Lectures of the
Hktory of Physiology During the 16th, 17th, and 18th Centuries translated by M. Foster (Cambridge, England: Cambridge University Press, 1901).
2. B Stimmel, Pain, Analgesia and Addictiow The Pharmacologic Treatment of Pain (New York: Raven Press, 1983) 2.
3. L E Scott, G A Clum, J B Peoples, “Pre-operative predicators of postoperative pain,” Pain 3 (March 1983)
4. J D Barchas et al, “Behavioral neurochemistry: Neuroregulators and behavioral states,” Science 200
283-293.
(May 1978) 964-973.
(New York: Churchill Livingston, 1984) 2. 5. P D Wall and R Malzack, Textbook of Pain
6. Stimmel, Pain, Analgesia and Addiction, 18-34. 7. Stimmel, Pain, Analgesia and Addiction, 57. 8. C Lindeman, B Van Aernam, “Nursing
intervention with the presurgical patient-The effects of structured and unstructured preoperative teaching,” Nursing Research (July-August 1971) 319-332.
9. L Graham, E Conley, “Evaluation of anxiety and fear in adult surgical patients,” Nursing Research 20 (March-April 1971) 113-122; J Johnson et al, “Sensory information, instruction in a coping strategy, and recovery from surgery,” Research in Nursing and Health 1 (April 1978) 4-17.
10. D Krieger, “Therapeutic touch: The imprimatur of nursing,” American Journal of Nursing 75 (May 1975) 784.
Is Drug Substitution Worth the Price? “Whether switching from brand name to generic drug or from brand name to brand name, a physi- cian is putting the patient at risk,” was the con- cern voiced by academicians, government researchers, and research-oriented drug company representatives at a conference sponsored by Health Policy International. This controversial issue is reported in the Nov 25, 1985 issue of Medical World News.
The meeting was prompted by the recent surge of generic drugs that have small price tags, government vouchers for safety and efficacy, and state laws in their favor. The US Food and Drug Administration (FDA) has approved several generic drugs based on an abbreviated equiva- lency process based on the “75-75 rule.” That rule states than in 75% of normal healthy volun- teers tested, usually 18 to 24 men, blood levels of the generic drug must amount to at least 75% of the values achieved by the reference drug; in other words, within 25% above or below those of the reference drug.
Many participants complained that the rule allows too much variability among generic
equivalents. “The FDA is doing a good job of walking the line,” commented James T. Doluisio, MD, dean and professor of pharmacy at the Uni- versity of Texas, Austin. “The 75-75 rule is a trade-off, a judgment call.”
Some drugs contained up to 30 chemicals other than the active ingredient such as binders, sweeteners, and coloring agents. Opponents to drug substitution say it’s often one of those chem- icals that causes adverse drug reactions or inhibits drug effects.
Opponents and proponents do agree that car- diovascular drugs, such as digoxin, should not be interchanged because they have a greater poten- tial for acute morbidity.
683