Embed Size (px)
Citation preview

DISPATCHES FROM THE GUILD CONFERENCE, SERIES #5
46 PRACTICAL GASTROENTEROLOGY • JUNE 2017
DISPATCHES FROM THE GUILD CONFERENCE, SERIES #5
Uma Mahadevan MD, Series Editorguildconference.com
Postoperative Management of Crohn’s Disease
Jana G. Hashash, MD, MSc, Assistant Professor of Medicine, Division of Gastroenterology, Hepatology and Nutrition, University of Pittsburgh School of Medicine, Pittsburgh, PA Miguel Regueiro, MD, AGAF, FACG, FACP, Professor of Medicine and Professor, Clinical and Translational Science, University of Pittsburgh School of Medicine, Division of Gastroenterology, Hepatology, and Nutrition, Senior Medical Lead of Specialty Medical Homes, University of Pittsburgh Medical Center, IBD Clinical Medical Director, Division of Gastroenterology, Hepatology and Nutrition, Pittsburgh, PA
The majority of patients with Crohn’s disease will require an intestinal resection at some point in their life. Postoperatively, these patients are at risk for developing recurrent Crohn’s disease and medications are often required to prevent recurrence. Stratifying patients according to their risk of recurrence is important and determines postoperative management of these patients.
Jana G. Hashash Miguel Regueiro
Natural Course of Postoperative Crohn’s Disease and Recurrence RatesAfter a curative ileocecal resection, the prevention of Crohn’s disease recurrence remains a challenge. Recurrence in these patients usually occurs at the ileocolonic anastomosis and in the neo-terminal ileum.6 Studies have shown that histologic recurrence may occur as early as 1 week after surgery.7 Endoscopic recurrence of Crohn’s disease tends to follow with recurrence rates as high as 70-90% at 1 year after surgery in patients who do not receive postoperative Crohn’s disease medications.6,8-12 Crohn’s disease recurrence after resection is often silent and this accounts for the lag between endoscopic and clinical recurrence, with the latter occurring later.13 Clinical recurrence rates, as
INTRODUCTION
Crohn’s disease is a chronic inflammatory condition that affects the GI tract anywhere between the mouth and the anal verge. Approximately
780,000 people in the United States carry the diagnosis of Crohn’s disease and the incidence and prevalence have been on the rise.1,2 The majority of patients with Crohn’s disease will require an intestinal resection, most commonly an ileocecal resection. The indication for surgery is usually for medically refractory disease or complications such as strictures, abscess, fistulae, or rarely malignancy.3,4 In a recent systematic review, it was reported that the 1 year cumulative risk of surgery for Crohn’s disease patients is estimated to be 16.3%, 33.3% at 5 years, and as high as 46.6% at 10 years.5

DISPATCHES FROM THE GUILD CONFERENCE, SERIES #5
Postoperative Management of Crohn’s Disease
PRACTICAL GASTROENTEROLOGY • JUNE 2017 47
DISPATCHES FROM THE GUILD CONFERENCE, SERIES #5
was developed by Rutgeerts et al.11 Although it is not validated, this score is widely used and predicts a patient’s risk for future clinical and surgical recurrence. Based on the endoscopic appearance of the neo-terminal ileum, patients are categorized into one of 5 groups; i0, i1, i2, i3, or i4 (Table 1). Patients with a score of i0 (normal appearing neo-terminal ileum) and i1 (<5 small aphthous ulcers in the neo-terminal ileum) have a low likelihood of progression to clinical or surgical recurrence in the next 5 years and are considered to be in endoscopic remission. Specifically, 85% remain in clinical remission over a 2-year time period and are considered very low risk for requiring a second operation.11,23,24 Patients with scores of i2, i3, and i4 are at a high risk to require a second Crohn’s disease intestinal operation within the following 5 years and are designated as having endoscopic recurrence.11, 23, 24
Risk Factors for Postoperative Crohn’s Disease RecurrenceThere are several risk factors that have been shown to contribute to the postoperative recurrence of Crohn’s disease. These factors are classified as (1) patient-related factors, (2) disease-related factors, and (3) surgery-related factors.25
The only modifiable risk factor is tobacco smoking.26-30 Not only does smoking tobacco increase endoscopic and clinical recurrence rates, surgical rates were seen to increase by 2.5 fold.31 Recurrence rates were higher in females and those who were smoking greater than 15 cigarettes per day.28,32
Fistulizing or penetrating Crohn’s disease and the need for prior Crohn’s disease related intestinal resection have also been shown to be strong risk factors for postoperative recurrence.33 Data on peri-operative steroid use as a risk factor for Crohn’s disease recurrence has been inconclusive. Recently, however, a multi-centre observational study by de Barcelos et al. showed that perioperative steroid use was the only significant risk factor for early postoperative endoscopic recurrence.34 A number of other disease-related risk factors have been studied as potential risk factors and these include young age at diagnosis of Crohns’ disease, young age at initial intestinal resection, and short duration of disease prior to the need for surgery.16,17,19,25,27,28,30,35-40
Surgical risk factors pertaining to the intestinal resection itself have been extensively studied, but all have been inconclusive in identifying strong factors for postoperative recurrence of Crohn’s disease.
defined by the Crohn’s disease Activity Index (CDAI), were shown to occur in 20-40% of patients at 1 year from surgery, and 35-50% by 5 years postoperatively.6,9-11,14 It is not an uncommon scenario for patients to require yet another surgical resection once clinical symptoms ensue in the postoperative setting (i.e. clinical recurrence). A quarter (25%) of patients will require a second intestinal resection by 5 years after their initial surgery, and up to 35% of patients by 10 years.15 The indication for subsequent intestinal resection tends to be similar to the indication of the initial operation.16-19
Surveillance of Postoperative Crohn’s DiseaseThe most sensitive modality for detection of postoperative Crohn’s disease is via an ileocolonoscopy which allows for the evaluation of the neo-terminal ileum mucosa. Due to the high rates of early endoscopic recurrence, it has been recommended that ileocolonoscopy is performed 6-12 months postoperatively.13,17,20-22 This would allow for early detection and aggressive treatment of recurrent disease, if present.
Endoscopic Scoring of Postoperative Crohn’s Disease The most widely used endoscopic scoring system
Table 1. Rutgeerts Endoscopic Recurrence Scoring System11
Endoscopic Score
Definition
i0 No lesions
i1 < 5 aphthous lesions
i2 > 5 aphthous lesions with normal mucosa between the lesions or skip areas of larger lesions or lesions confined to the ileocolonic anastomosis
i3 Diffuse aphthous ileitis with diffusely inflamed mucosa
i4 Diffuse inflammation with already larger ulcers, nodules, and/or narrowing
i0 and i1 imply endoscopic remission while i2-i4 imply recurrent endoscopic disease

Postoperative Management of Crohn’s Disease
DISPATCHES FROM THE GUILD CONFERENCE, SERIES #5
48 PRACTICAL GASTROENTEROLOGY • JUNE 2017
the use of immunomodulators,45-47 nitroidimazole,48,49 budesonide,50,51 5-aminosalicylic acid52-55 and placebo. The lowest endoscopic recurrence rates were seen with immunomodulators (azathioprine and 6 mercaptopurine) at 42-44%. Postoperative recurrence rates were further decreased with the widespread use of anti-tumor necrosis factors (anti-TNF) medications. Table 3 summarizes the postoperative endoscopic rates reported with these medications.56-64
Most recently, data from the PREVENT trial65 showed that the clinical recurrence rates in patients on infliximab was less than the rates on placebo at week
Variables that were explored include: length of resected bowel, width of surgical margins, type of anastomosis, perioperative complications, and presence of granulomas in the surgical specimen.4,24,25,28,36,39,41-44
Medications Studied for the Management of Postoperative Crohn’s DiseaseThere have been many studies on the early use of different medication classes for the prevention of postoperative Crohn’s disease after resective surgery. Table 2 displays the 1 year clinical and endoscopic recurrence rates that have been reported in various randomized controlled studies of patients after an ileocecal resection and (continued on page 50)
Table 2. One Year Clinical and Endoscopic Recurrence Rates Reported in Randomized Controlled Studies20,22
Medication Clinical Recurrence Endoscopic Recurrence
Placebo 25% – 77% 53% - 79%
5-ASA 24% - 58% 63% - 66%
Budesonide 19% - 32% 52% - 57%
Nitroidimazole 7% - 8% 52% - 54%
AZA/6MP 34% – 50% 42 – 44%
5-ASA: 5-aminosalicylic acid; AZA: azathioprine; 6MP: 6-mercaptopurine
Table 3. Postoperative Endoscopic Recurrence (≥i2) Rates Reported in Anti-TNF Studies56-64
Anti-TNF Control
Sorrentino (MTX/IFX vs 5-ASA 2yr) 0% 100% (5-ASA)
Regueiro (IFX vs PBO RCT 1 yr) 9% 85% (PBO)
Yoshida (IFX vs PBO Open 1 yr) 21% 81% (5-ASA)
Armuzzi (IFX vs AZA Open 1 yr) 9% 40% (AZA)
Fernandez-Blanco (ADA) 10% N/A
Papamichael (ADA 6m) 0% N/A
Savarino (ADA 3yr) 0% N/A
Aguas (ADA 1 yr) 21% N/A
Savarino (ADA vs AZA vs 5-ASA 2 yrs) 6% 65% (AZA), 83%(5-ASA)
anti-TNF: anti-tumor necrosis factor; MTX: methotrexate; IFX: infliximab; 5-ASA: 5-aminosalicylic acid; PBO; placebo; RCT: randomized controlled trial; AZA: azathioprine; ADA: adalimumab

50 PRACTICAL GASTROENTEROLOGY • JUNE 2017
DISPATCHES FROM THE GUILD CONFERENCE, SERIES #5
Postoperative Management of Crohn’s Disease
76 or less, however this difference was not statistically significant (12.9% vs 20%; p=0.097). Endoscopic recurrence rates, however, were significantly lower in patients receiving infliximab compared to placebo (22.4% vs 51.3%; p<0.001).
In the POCER trial, endoscopic recurrence rates at 18 months after surgery compared those who underwent an ileocolonoscopy at 6 months after an ileocecal resection (active care arm) and who subsequently received medication escalation if needed (endoscopic ileal score ≥i2), to those patients who did not get a 6 month ileocolonoscopy (standard care arm).66 All patients received metronidazole 400 mg by mouth twice daily for the first 3 months postoperatively. Additionally patients who were classified as high risk (smokers, penetrating disease, and/or prior intestinal resection) received azathioprine. Those who were intolerant of azathioprine were given adalimumab instead. At 18 month follow up, endoscopic recurrence rates were significantly lower amongst patients in the active care arm compared to those in the standard arm (60/122=49% vs 35/52=57%; p=0.03). It was also noted that within the high-risk active arm patients, those who received adalimumab had lower 6 month endoscopic recurrence rates when compared to those who received azathioprine (6/28=21% vs 33/73=45%).66
Management of Postoperative Crohn’s Disease – Technical Review and GuidelinesRecently, the American Gastroenterological Association (AGA) published a technical review on the management of postoperative Crohn’s disease.67 This review addressed clinical questions pertaining to the different management strategies for postoperative Crohn’s disease patients and their role in reducing recurrence. For instance, this review addressed if routine early pharmacologic prophylaxis was superior to endoscopy-guided treatment in reducing long-term recurrence in postoperative Crohn’s disease patients. Another question related to the comparative effectiveness of the different medications used amongst Crohn’s disease patients who are receiving early postoperative pharmacological prophylaxis. Similarly, comparative effectiveness of the different medications used to decrease endoscopic recurrence in patients who already developed postoperative asymptomatic endoscopic recurrence. Additionally, this review compared whether routine endoscopic monitoring at 6-12 months postoperatively
is superior to no endoscopic monitoring.67 This technical review informed AGA Guidelines for the management of postoperative Crohn’s disease.68 (Table 4)
The authors provide two approaches to patients with postoperative Crohn’s disease (Figures 1, 2). Based on individuals’ risk factors, patients are stratified in to groups to aid physicians in their further management. Some physicians prefer to practice the ‘watchful waiting’ approach, while other physicians are more proactive and initiate medications postoperatively for
(continued from page 48)
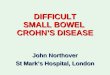
Figure 2. Algorithm for postoperative management of Crohn’s disease - Watchful Waiting
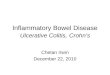
Figure 1. Algorithm for postoperative management of Crohn’s disease - Author’s Practice

DISPATCHES FROM THE GUILD CONFERENCE, SERIES #5
Postoperative Management of Crohn’s Disease
PRACTICAL GASTROENTEROLOGY • JUNE 2017 51
prophylaxis and secondary prevention of recurrent Crohn’s disease. Despite the published algorithms, deciding the best option for patients often remains a dilemma.
It is the authors’ personal practice to initiate postoperative Crohn’s disease prophylaxis to prevent recurrence. Almost all patients receive a medication postoperatively, whether using an immunomodulator or combination therapy with a biologic agent and an immunomodulator. Depending on a patient’s risk factors, he/she is categorized in to a low-risk, moderate-risk, or high-risk group (Figure 1). All patients regardless of their group will receive an ileocolonoscopy for surveillance of endoscopic recurrence, 6-12 months postoperatively. The authors stratify patients into risk categories when approaching postoperative management. Low risk patients include those who are undergoing their first intestinal resection for a short stricture and those who have had long standing disease (>10 years). Patients in the low risk group are not administered medications, however, if there is evidence of recurrent Crohn’s disease (ileal score of ≥i2), treatment with an immunomodulator and/or anti-TNF is initiated.
Otherwise, they would remain off of any medications, but should continue to have surveillance colonoscopies every 1-3 years. Patients who are in the moderate risk group are those who are undergoing their first intestinal resection for a long stricture (>10 cm) or for inflammatory Crohn’s disease and who have had disease for shorter than 10 years. Patients in this moderate risk group start thiopurines in the postoperative setting +/- metronidazole. While the authors still believe there is a role for immunomodulators in patients not previously receiving this type of medication, there has been a recent trend to only use thiopurines in combination with biologics rather than monotherapy. Nonetheless, we still use immunomodulators for this moderate risk group naïve to treatment, but escalate to an anti-TNF if there is evidence of subsequent recurrence. Patients in the high-risk group include those with penetrating disease, more than 2 intestinal resection surgeries, and who are smokers. In these high-risk patients, we recommend a combination of an immunomodulator with anti-TNF. Whether therapeutic drug monitoring of biologic therapy would allow for monotherapy anti-TNF (without an immunomodulator) for postoperative
Table 4. Summary of the Recently Published AGA Clinical Guidelines for the Management of Postoperative Crohn’s Disease68
Statement Strength of Recommendation
Quality of Evidence
1. In patients with surgically induced remission of CD, the AGA suggests early pharmacological prophylaxis over endoscopy-guided pharmacological treatment
Conditional Very Low
2. In patients with surgically induced remission of CD, the AGA suggests using anti-TNF therapy and/or thiopurines over other agents
Conditional Moderate
3. In patients with surgically induced remission of CD, the AGA suggests against using mesalamine (or other 5-aminosalicylates), budesonide, or probiotics
Conditional Low; Very Low
4. In patients with surgically induced remission of CD receiving pharmacological prophylaxis, the AGA suggests postoperative endoscopic monitoring at 6 to 12 months after surgical resection over no monitoring
Conditional Moderate
5. In patients with surgically induced remission of CD not receiving pharmacological prophylaxis, the AGA recommends postoperative endoscopic monitoring at 6 to 12 months after surgical resection over no monitoring
Strong Moderate
6. In patients with surgically induced remission of CD with asymptomatic endoscopic recurrence, the AGA suggests initiating or optimizing anti-TNF and/or thiopurine therapy over continued monitoring alone
Conditional Moderate
AGA: American Gastroenterological Association; CD: Crohn’s Disease

Postoperative Management of Crohn’s Disease
DISPATCHES FROM THE GUILD CONFERENCE, SERIES #5
52 PRACTICAL GASTROENTEROLOGY • JUNE 2017
Crohn’s disease management is unknown.Another approach to the management of
postoperative Crohn’s disease is to stratify patients by risk of recurrence but utilize endoscopic recurrence to guide therapy (Figure 2).66 In this approach, patients are separated in to a high-risk group and a low risk group for recurrence where only patients in the high-risk group would receive Crohn’s disease medications. The medication of choice is a thiopurine agent, but in cases of thiopurine intolerance, anti-TNF medications are used instead. Again, similar to the algorithm in Figure 1, all patients would undergo an ileocolonoscopy at 6 months postoperatively, and depending on evidence of endoscopic recurrence, medication escalation is made. Of note, the authors of POCER have also reported the potential for fecal calprotectin as a surrogate marker for Crohn’s disease recurrence and may be a noninvasive method to measure recurrence.69
CONCLUSIONThe majority of patients with Crohn’s disease will require an intestinal resection at some point in their lifetime. Postoperative management of these patients remains a challenge. It is important to identify high-risk patients who exhibit risk factors for recurrence and to aggressively treat these patients to prevent or ameliorate recurrence of their Crohn’s disease. All patients regardless of their risk should have an ileocolonoscopy 6-12 months postoperatively to initiate or adjust medications in cases of endoscopic recurrence (ileal score ≥i2). The authors provide the algorithm that they utilize in their practice when approaching postoperative Crohn’s disease patients (Figure 1).
References
1. http://www.ccfa.org/what-are-crohns-and-colitis/what-is-crohns-disease/ - last accessed 1.20.2017
2. Molodecky NA, Soon IS, Rabi DM, et al. Increasing incidence and prevalence of the inflammatory bowel diseases with time, based on systematic review. Gastroenterology. 2012;142: 46–54.e42 quiz e30.
3. Cosnes J, Nion-Larmurier I, Beaugerie L, et al. Impact of the increasing use of immunosuppressants in Crohn’s disease on the need for intestinal surgery. Gut. 2005;54(2):237–41.
4. Bernell O, Lapidus A, Hellers G. Risk factors for sur-gery and postoperative recurrence in Crohn’s disease. Ann Surg. 2000 Jan;231(1):38-45.
5. Frolkis AD, Dykeman J, Negron ME, et al. Risk of surgery for inflammatory bowel diseases has decreased over time: a sys-tematic review and meta-analysis of population-based studies. Gastroenterology. 2013;145:996–1006.
6. Olaison G, Smedh K, Sjodahl R. Natural course of Crohn’s disease after ileocolic resection: endoscopically visualised ileal ulcers preceding symptoms. Gut. 1992;33(3):331–5.
7. D’Haens GR, Geboes K, Peeters M, et al. Early lesions of recur-
rent Crohn’s disease caused by infusion of intestinal contents in excluded ileum. Gastroenterology. 1998;114(2):262–7.
8. Buisson A, Chevaux JB, Allen PB, et al. Review article: the natuP-ral history of postoperative Crohn’s disease recurrence. Aliment Pharmacol Ther. 2012; Mar;35(6):625-33.
9. Rutgeerts P, Geboes K, Vantrappen G, et al. Natural hisb-tory of recurrent Crohn›s disease at the ileocolonic anastomoe-sis after curative surgery. Gut. 1984;25(6):665-72.
10. Sachar DB. The problem of postoperative recurrence of Crohn’s disease. Med Clin N Am. 1990;74(1):183–8.
11. Rutgeerts P, Geboes K, Vantrappen G, et al. Predictability of the postoperative course of Crohn’s disease. Gastroenterology. 1990;99(4):956–63.
12. Tytgat GN, Mulder CJ, Brummelkamp WH. Endoscopic lesions in Crohn’s disease early after ileocecal resection. Endoscopy. 1998; 20: 260-262.
13. Rutgeerts P. Review article: recurrence of Crohn’s disease after surgery—the need for treatment of new lesions. Aliment Pharmacol Ther. 2006;24 Suppl 3:29–32.
14. Greenstein AJ, Sachar DB, Pasternack BS, et al. Reoperation and recurrence in Crohn’s colitis and ileocolitis Crude and cumulative rates. N Engl J Med. 1975 Oct 2;293(14):685-90.
15. Frolkis AD, Lipton DS, Fiest KM. Cumulative incidence of second intestinal resection in Crohn’s disease: a systematic review and meta-analysis of population-based studies. Am J Gastroenterol. 2014; 109 :1739–1748.
16. Greenstein AJ, Lachman P, Sachar DB, et al. Perforating and non-perforating indications for repeated operations in Crohn’s disease: evidence for two clinical forms. Gut. 1988;29(5):588–92.
17. Ng SC, Kamm MA. Management of postoperative Crohn’s dis-ease. Am J Gastroenterol. 2008;103(4):1029–35.
18. D’Haens GR, Gasparaitis AE, Hanauer SB. The length of recur-rent ileitis after ileocolonic resection correlates with presurgical extent of Crohn’s disease. Gastroenterology. 1993;104:A692.
19. Lautenbach E, Berlin JA, Lichtenstein GR. Risk factors for early postoperative recurrence of Crohn’s disease. Gastroenterology. 1998;115(2):259–67.
20. Hashash JG, Regueiro M. A Practical Approach to Preventing Postoperative Recurrence in Crohn’s Disease. Curr Gastroenterol Rep. 2016 May;18(5):25.
21. Cottone M, Orlando A, Modesto I. Postoperative maintenance therapy for inflammatory bowel disease. Curr Opin Gastroenterol. 2006; 22(4):377-381.
22. Hashash JG, Regueiro MD. The evolving management of postop-erative Crohn’s disease. Expert Rev Gastroenterol Hepatol. 2012 Sep;6(5):637-48.
23. Katz JA. Postoperative endoscopic surveillance in Crohn’s disease: bottom up or top down? Gastrointest Endosc. 2007;66(3):541-3.
24. Blum E, Katz JA. Postoperative therapy for Crohn’s disease. Inflamm Bowel Dis. 2009; 15(3):463-72.
25. Terdiman JP. Prevention of postoperative recurrence in Crohn’s disease. Clin Gastroenterol Hepatol. 2008 Jun;6(6):616-20.
26. Cottone M, Rosselli M, Orlando A, et al. Smoking habits and recurrence in Crohn’s disease. Gastroenterology. 1994; 106(3):643-648.
27. Sutherland LR, Ramcharan S, Bryant H, et al. Effect of cigarette smoking on recurrence of Crohn’s disease. Gastroenterology. 1990 May;98(5 Pt 1):1123-8.
28. Yamamoto T. Factors affecting recurrence after surgery for Crohn’s disease. World J Gastroenterol. 2005 Jul 14;11(26):3971-9.
29. Kane SV, Flicker M, Katz-Nelson F. Tobacco use is associated with accelerated clinical recurrence of Crohn’s disease after surgi-cally induced remission. J Clin Gastroenterol. 2005 Jan;39(1):32-5.
30. Avidan B, Sakhnini E, Lahat A, et al. Risk factors regarding the need for a second operation in patients with Crohn’s disease. Digestion. 2005;72(4):248-53.
31. Reese GE, Nanidis T, Borysiewicz C, et al. The effect of smoking after surgery for Crohn’s disease: a meta-analysis of observational
(continued on page 54)

Postoperative Management of Crohn’s Disease
DISPATCHES FROM THE GUILD CONFERENCE, SERIES #5
54 PRACTICAL GASTROENTEROLOGY • JUNE 2017
studies. Int J Colorectal Dis. 2008 Dec;23(12):1213-21.32. Cosnes J, Carbonnel F, Beaugerie L, et al. Effects of ciga-
rette smoking on the long-term course of Crohn’s disease. Gastroenterology. 1996 Feb;110(2):424-31.
33. Simillis C, Yamamoto T, Reese GE, et al. A meta-analysis com-paring incidence of recurrence and indication for reoperation after surgery for perforating versus nonperforating Crohn’s disease. Am J Gastroenterol. 2008 Jan;103(1):196-205.
34. de Barcelos IF, Kotze PG, Spinelli A, et al. Factors affecting the incidence of early endoscopic recurrence after ileocolonic resection for Crohn’s disease: a multicentre observational study. Colorectal Dis. 2017 Jan;19(1):O39-O45.
35. Mekhjian HS, Switz DM, Watts HD, et al. National Cooperative Crohn’s Disease Study: factors determining recurrence of Crohn’s disease after surgery. Gastroenterology. 1979 Oct;77(4 Pt 2):907-13.
36. Poggioli G, Laureti S, Selleri S, et al. Factors affecting recurrence in Crohn’s disease. Results of a prospective audit. Int J Colorectal Dis. 1996;11(6):294-8.
37. Chardavoyne R, Flint GW, Pollack S, et al. Factors affecting recurrence following resection for Crohn’s disease. Dis Colon Rectum. 1986;29(8):495-502.
38. Michelassi F, Balestracci T, Chappell R, et al. Primary and recur-rent Crohn’s disease. Experience with 1379 patients. Ann Surg. 1991;214(3):230-8.
39. Caprilli R, Corrao G, Taddei G, et al. Prognostic factors for postoperative recurrence of Crohn’s disease. Gruppo Italiano per lo Studio del Colon e del Retto (GISC). Dis Colon Rectum. 1996;39(3):335-41.
40. Unkart JT, Anderson L, Li E, et al. Risk factors for surgical recurrence after ileocolic resection of Crohn’s disease. Dis Colon Rectum. 2008;51(8):1211-6.
41. Ewe K, Herfarth C, Malchow H, et al. Postoperative recurrence of Crohn’s disease in relation to radicality of operation and sulfasala-zine prophylaxis: a multicenter trial. Digestion. 1989;42(4):224-32.
42. Scarpa M, Ruffolo C, Bertin E, et al. Surgical predictors of recurrence of Crohn’s disease after ileocolonic resection. Int J Colorectal Dis. 2007;22(9):1061-9.
43. Bergamaschi R, Pessaux P, Arnaud JP. Comparison of conven-tional and laparoscopic ileocolic resection for Crohn’s disease. Dis Colon Rectum. 2003;46(8):1129-33.
44. Yamamoto T, Bain IM, Mylonakis E, et al. Stapled functional end-to-end anastomosis versus sutured end-to-end anastomosis after ileocolonic resection in Crohn disease. Scand J Gastroenterol. 1999;34(7):708-13.
45. D’Haens GR, Vermeire S, Van Assche G, et al. Therapy of metro-nidazole with azathioprine to prevent postoperative recurrence of Crohn’s disease: a controlled randomized trial. Gastroenterology. 2008;135(4):1123-9.
46. Herfarth H, Tjaden C, Lukas M, et al. Adverse events in clinical trials with azathioprine and mesalamine for prevention of postop-erative recurrence of Crohn’s disease. Gut. 2006;55(10):1525-6.
47. Hanauer SB, Korelitz BI, Rutgeerts P, et al. Postoperative maintenance of Crohn’s disease remission with 6-mercaptopu-rine, mesalamine, or placebo: a 2-year trial. Gastroenterology. 2004;127(3):723-9.
48. Rutgeerts P, Hiele M, Geboes K, et al. Controlled trial of metro-nidazole treatment for prevention of Crohn’s recurrence after ileal resection. Gastroenterology. 1995;108(6):1617-21.
49. Rutgeerts P, Van Assche G, Vermeire S, et al. Ornidazole for pro-phylaxis of postoperative Crohn’s disease recurrence: a random-ized, double-blind, placebo-controlled trial. Gastroenterology. 2005;128(4):856-61.
50. Hellers G, Cortot A, Jewell D, et al. Oral budesonide for preven-tion of postsurgical recurrence in Crohn’s disease. The IOIBD Budesonide Study Group. Gastroenterology. 1999;116(2):294-300.
51. Ewe K, Bottger T, Buhr HJ, et al. Low-dose budesonide treat-ment for prevention of postoperative recurrence of Crohn’s disease: a multicentre randomized placebo-controlled trial.
German Budesonide Study Group. Eur J Gastroenterol Hepatol. 1999;11(3):277-82.
52. Florent C, Cortot A, Quandale P, et al. Placebo-controlled clinical trial of mesalazine in the prevention of early endoscopic recur-rences after resection for Crohn’s disease. Groupe d’Etudes Therapeutiques des Affections Inflammatoires Digestives (GETAID). Eur J Gastroenterol Hepatol. 1996;8(3):229-33.
53. Caprilli R, Andreoli A, Capurso L, et al. Oral mesalazine (5-ami-nosalicylic acid; Asacol) for the prevention of post-operative recurrence of Crohn’s disease. Gruppo Italiano per lo Studio del Colon e del Retto (GISC). Aliment Pharmacol Ther. 1994;8(1):35-43.
54. Caprilli R, Cottone M, Tonelli F, et al. Two mesalazine regimens in the prevention of the post-operative recurrence of Crohn’s disease: a pragmatic, double-blind, randomized controlled trial. Aliment Pharmacol Ther. 2003;17(4):517-23.
55. Brignola C, Cottone M, Pera A, et al. Mesalamine in the preven-tion of endoscopic recurrence after intestinal resection for Crohn’s disease. Italian Cooperative Study Group. Gastroenterology. 1995;108(2):345-9.
56. Sorrentino D, Terrosu G, Avellini C, et al. Infliximab with low-dose methotrexate for prevention of postsurgical recurrence of ileocolonic Crohn disease. Arch Intern Med. 2007;167(16):1804-7.
57. Regueiro M, Schraut W, Baidoo L, et al. Infliximab prevents Crohn’s disease recurrence after ileal resection. Gastroenterology. 2009;136(2):441-50. e1; quiz 716.
58. Yoshida K, Fukunaga K, Ikeuchi H, et al. Scheduled infliximab monotherapy to prevent recurrence of Crohn’s disease following ileocolic or ileal resection: A 3-year prospective randomized open trial. Inflamm Bowel Dis. 2012;18(9):1617-23.
59. Armuzzi A, Felice C, Papa A, et al. Prevention of postopera-tive recurrence with azathioprine or infliximab in patients with Crohn’s disease: an open-label pilot study. J Crohns Colitis. 2013;7(12):e623-9.
60. Fernández-Blanco I MJ, Martinez B, Cara C, Taxonera C. Adalimumab in the Prevention of Postoperative Recurrence of Crohn’s Disease. Gastroenterology. 2010;138(5):Supplement 1, page S-692.
61. Papamichael K, Archavlis E, Lariou C, et al. Adalimumab for the prevention and/or treatment of post-operative recurrence of Crohn’s disease: a prospective, two-year, single center, pilot study. J Crohns Colitis. 2012;6(9):924-31.
62. Savarino E, Dulbecco P, Bodini G, et al. Prevention of postopera-tive recurrence of Crohn’s disease by Adalimumab: a case series. Eur J Gastroenterol Hepatol. 2012;24(4):468-70.
63. Aguas M, Bastida G, Cerrillo E, et al. Adalimumab in preven-tion of postoperative recurrence of Crohn’s disease in high-risk patients. World J Gastroenterol. 2012;28;18(32):4391-8.
64. Savarino E, Bodini G, Dulbecco P, et al. Adalimumab is more effective than azathioprine and mesalamine at preventing post-operative recurrence of Crohn’s disease: a randomized controlled trial. Am J Gastroenterol. 2013;108(11):1731-42.
65. Regueiro M, Feagan BG, Zou B, et al. Infliximab Reduces Endoscopic, but Not Clinical Recurrence of Crohn’s Disease After Ileocolonic Resection. Gastroenterology. 2016 Jun; 150(7):1568-78.
66. De Cruz P, Kamm MA, Hamilton AL, et al. Crohn’s disease management after intestinal resection: a randomised trial. Lancet. 2015;11;385(9976):1406-17.
67. Regueiro M, Velayos F, Greer JB, et al. American Gastroenterological Association Institute Technical Review on the Management of Crohn’s Disease After Surgical Resection. Gastroenterology. 2017;15:277-295.
68. Geoffrey C. Nguyen, Edward V. Loftus Jr., et al. American Gastroenterological Association Institute Guideline on the Management of Crohn’s Disease After Surgical Resection. Gastroenterology. 2017;15:271-275.
69. Wright EK, Kamm MA, De Cruz P, et al. Measurement of fecal calprotectin improves monitoring and detection of recur-rence of Crohn’s disease after surgery. Gastroenterology. 2015 May;148(5):938-947.
(continued from page 52)