Embed Size (px)
Citation preview
1
PREGNANT &
LOVING IT!
EFFECTIVELY TREATING
THE PREGNANT PATIENT
DR. NATALIE J. SEBBA,
PT, DPT, WCS, CLT
* Slides or material not to be reproduced or used without written consent of author
Provider Disclaimer
Allied Health Education and the presenter of this webinar
do not have any financial or other associations with the
manufacturers of any products or suppliers of commercial
services that may be discussed or displayed in this
presentation.
There was no commercial support for this presentation.
The views expressed in this presentation are the views and
opinions of the presenter.
Participants must use discretion when using the
information contained in this presentation.
Objectives:
1.Participant will understand the typical physiological changes associated with
pregnancy.
2. Clinician will properly identify common spinal and pelvic alignment impairments of
the pregnant woman.
3. Clinician will understand how to assess a pregnant woman and effectively prescribe
therapeutic exercises associated with this presentation.
4. Following the webinar the clinician will effectively instruct women in proper body
mechanics associated with pregnancy.
5. Learner will verbalize the importance of core and pelvic floor muscle function and
understand the progression of strength development in the pregnant client.
6. The learner will be able to properly educate women on exercise considerations
during pregnancy and how to reduce the risk of diastasis rectus.
7. Participant will understand educational concepts for pregnant women related to
childbirth, positioning during labor and immediate post-partum considerations.
8. Participant will identify proper assessment scales to utilize with this patient
population to improve effectiveness of documentation and reimbursement.
2
Normal Physiological Changes
Pregnancy is divided into 3 trimesters.
Each trimester is a little longer than 13 weeks.
Normal Physiological Changes
1st Trimester
Fatigue
Increased urination
Nausea/vomitting
Generalized malaise
Breast tenderness
Increased abdominal
girth
About 25% of pregnant
women experience slight
bleeding during their first
trimester.
1st Trimester Red Flags
Hyperemesis Gravidarum
Serious medical condition that can result in dehydration, weight loss
and nutritional deficiencies
Management suggestions:
Add fresh ginger to foods
Drink ginger root tea
Blood loss
Significant bleeding, cramping, or sharp pain = CALL doctor
3
Normal Physiological Changes
2nd Trimester:
Noticeable increase weight
Fatigue
Fluid retention
Indigestion
Food cravings
Light-headedness
Heart burn
Constipation/gas
Stretch marks
Braxton Hicks contractions
2nd Trimester Red Flags
Gestational Diabetes:
40% of pregnant women
Risk factors: overweight, >age 35, hx of larger babies
Management suggestions:
Regular mild to moderate exercise
Nutritional counseling: monitoring carbohydrate and fat intake
Preeclampsia:
Combination of symptoms: fluid retention, severe headaches, blurred
vision, edema
Management suggestions:
Doctors orders: often bed rest
Normal Physiological Changes
3rd Trimester:
Braxton Hicks contractions
Painful rib subluxations
Indigestion
Difficulty sleeping
Difficulty breathing
Frequent urination
Low back pain
Symphysis pubis pain
Groin/back pain
Swelling
Spotting
4
3rd Trimester Red Flags
Placenta Previa: When the placenta covers the opening in the
mother's cervix.
Previous delivery
> 35 yo
history of previous surgeries, such as a cesarean section (C-section) or
uterine fibroid removal
Management suggestions:
Doctors orders: often bed rest
Rapid weight gain
Severe abdominal cramps
Transient osteoporosis
Normal Physiological Changes
Cardiovascular system:
Volume increases 35-50%
Plasma increase>red blood cell increase = “physiologic anemia”
Increased venous pressure in LE
Heart size increases and is elevated
HR increases by 10-20 bpm
Cardiac output increases 30-60%; increased in L side lying
Metabolic system:
Additional 300 calories/day
Expected gain: 25-30 lbs/ 50-60 lbs for multiples
Normal fasting blood glucose levels are lower than standard
Normal Physiological Changes
Hormonal changes
Estrogen
Levels increase 30x
Relaxin & progesterone: increases ligamentous laity, softens cartilage
Significantly affects pelvic joints, sacrum, coccyx etc.
Peaks at week 14 and prior to delivery
Connective Tissue
Thoracolumbar fascia: position of extreme length reducing ability to
stabilize trunk
Joint hypermobility
Increase risk of injury to back, pelvic, and LE
5
Normal Physiological Changes
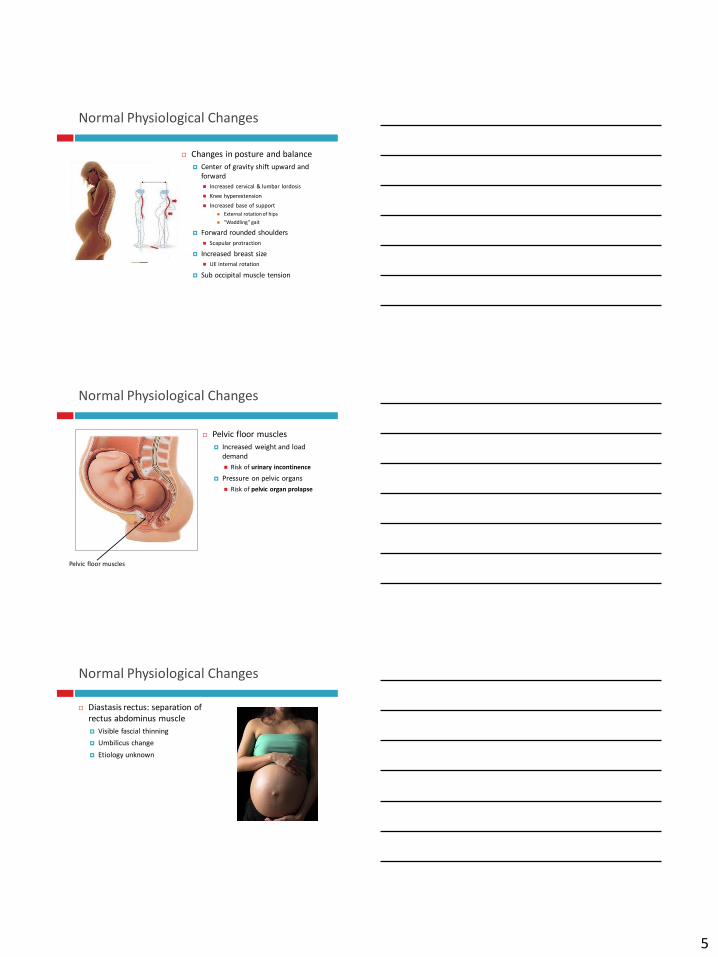
Changes in posture and balance
Center of gravity shift upward and
forward
Increased cervical & lumbar lordosis
Knee hyperextension
Increased base of support
External rotation of hips
“Waddling” gait
Forward rounded shoulders
Scapular protraction
Increased breast size
UE internal rotation
Sub occipital muscle tension
Normal Physiological Changes
Pelvic floor muscles
Increased weight and load
demand
Risk of urinary incontinence
Pressure on pelvic organs
Risk of pelvic organ prolapse
Pelvic floor muscles
Normal Physiological Changes
Diastasis rectus: separation of
rectus abdominus muscle
Visible fascial thinning
Umbilicus change
Etiology unknown
6
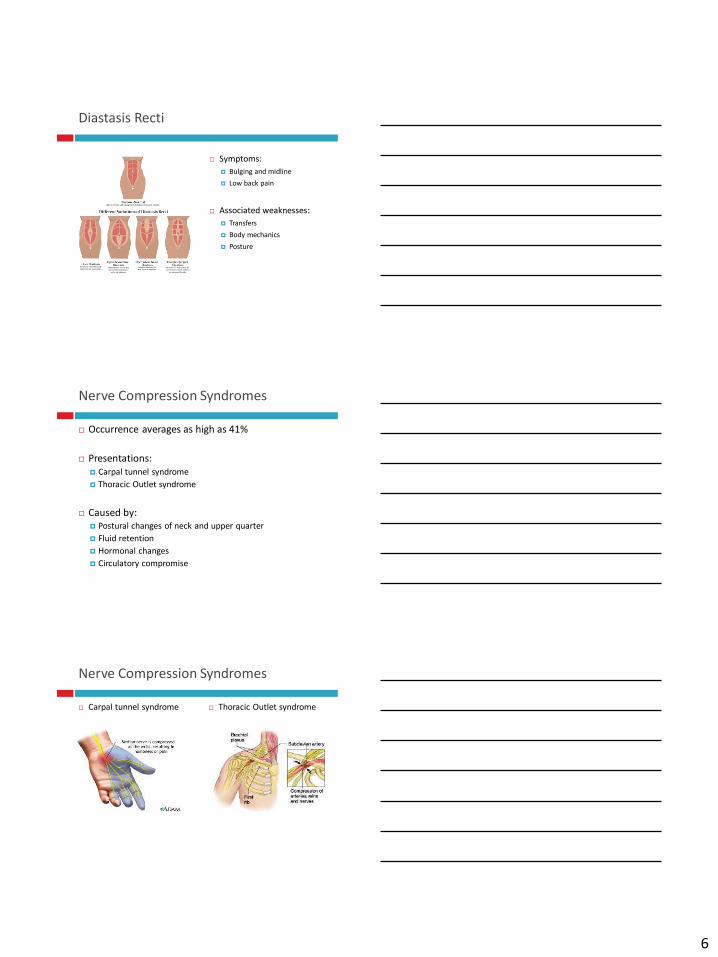
Diastasis Recti
Symptoms:
Bulging and midline
Low back pain
Associated weaknesses:
Transfers
Body mechanics
Posture
Nerve Compression Syndromes
Occurrence averages as high as 41%
Presentations:
Carpal tunnel syndrome
Thoracic Outlet syndrome
Caused by:
Postural changes of neck and upper quarter
Fluid retention
Hormonal changes
Circulatory compromise
Nerve Compression Syndromes
Carpal tunnel syndrome Thoracic Outlet syndrome
7
Nerve Compression Syndromes
Interventions:
Postural correction
Manual release
Ergonomic assessment
Splints for CTS
Symptoms often persist into postpartum and
increased presentation severity with breastfeeding
Common Spine Symptoms
Postural back pain
50-70% pregnant women experience this pain
Continues into postpartum period for 68% of these women
Symptoms worsen with:
Fatigue
As day progresses
Static postures
Common Spine Symptoms
Sacroiliac/Pelvic Girdle Pain
Pelvic girdle pain: localized to posterior pelvis and radiates into
buttocks and posterior thigh
Symptoms increased with:
Prolonged sitting
Standing/walking
Climbing stairs
Unilateral standing
Torsion activity
Increased with activity
Not often relieved with rest
8
Common Spine Symptoms
Pubic Symphysis Dysfunction
Often in combination with pelvic girdle pain (PGP)
Symptoms:
Tenderness at symphysis joint
Radiating pain into groin, medial thigh
Increased pain with weight bearing
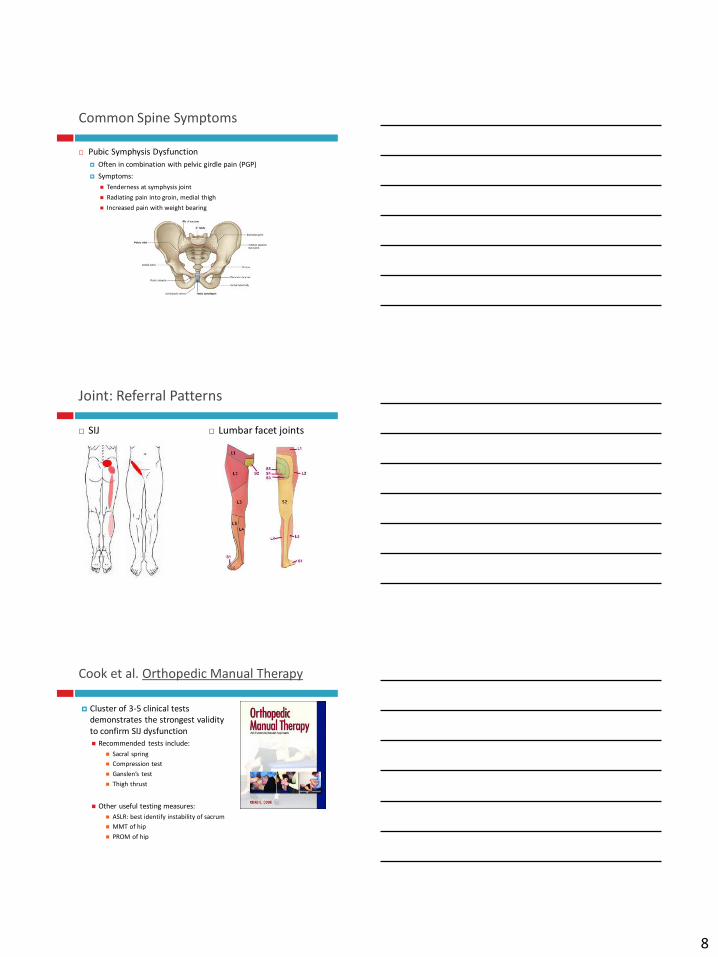
Joint: Referral Patterns
SIJ Lumbar facet joints
Cook et al. Orthopedic Manual Therapy
Cluster of 3-5 clinical tests
demonstrates the strongest validity
to confirm SIJ dysfunction
Recommended tests include:
Sacral spring
Compression test
Ganslen’s test
Thigh thrust
Other useful testing measures:
ASLR: best identify instability of sacrum
MMT of hip
PROM of hip
9
Pelvic Girdle Pain Clinical Practice Guidelines:
July 2017
Clinton, S. et al. Pelvic girdle pain in the antepartum population:
Physical Therapy Clinical Practice Guidelines Linked to the
International Classification of Functioning, Dias ability and Health
From the Section of Women’s Health and the Orthopedic Section of the APTA. Journal of Women’s Health Physical Therapy. Volume 41 (2). July 2017.
Clinical Course:
Common presentation of PGP: 14-30 wks
Presents of LBP or PGP in early pregnancy indicate high
likelihood of increased pain in late pregnancy
Persistent pain in postpartum period presents in7-25% of
women
Pelvic Girdle Pain Clinical Practice Guidelines:
July 2017
5 Diagnostic categories:
Pelvic girdle syndrome (6%)
Both SIJ and pubic symphysis
Symphysiolysis (2.3%)
Pain only in pubic symphysis
One sides SI syndrome (5.5%)
Double sided SI syndrome
(6.3%)
Constant variation (1.6%)
Pelvic Girdle Pain Clinical Practice Guidelines:
July 2017
Postural changes:
Magnitude of postural changes during pregnancy is not related to PGB
Pathophysiology:
Changes in ability to manage load transfer due to joint laxity may account for development of PGP
Current studies do not support relationship of relaxinand PGP
Pubic symphysis has been shown to widen as early at 8-10 wks and continues to average of 7mm
PGP more likely to present in women with >10mm separation
10
Pelvic Girdle Pain Clinical Practice Guidelines:
July 2017
Differential Diagnosis
History of trauma, unexplained weight loss, steroid use, drug abuse, HIV, fever, systemically unwell
Special consideration:
Symptoms due to uterine abruption, referred pain from UTI
Hip dysfunction:
Femoral neck fracture, bursitis, impingement, labral irritation
Ensure proper test interpretation based on location of pain
Lumbar spine:
Spondylolisthesis, discal patterns that fail to centralize, diminished reflexes, lumbar disk
Pelvic Girdle Pain Clinical Practice Guidelines:
July 2017
Examination
Pelvic Girdle Syndrome
Separation
Compression
Hip abduction/adduction
One sided/double sided
SI Syndromes
Thigh trust
Menell’s test
FABER
Pubic Symphysis
Palpation
Trendelenburg
Pelvic Girdle Examination
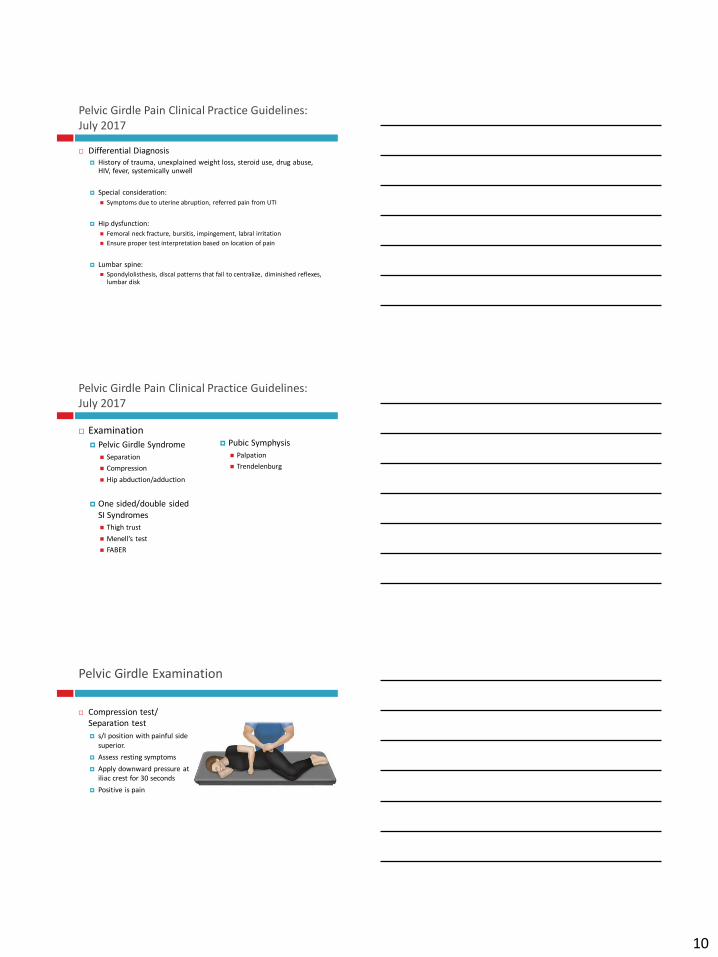
Compression test/
Separation test
s/I position with painful side
superior.
Assess resting symptoms
Apply downward pressure at
iliac crest for 30 seconds
Positive is pain
11
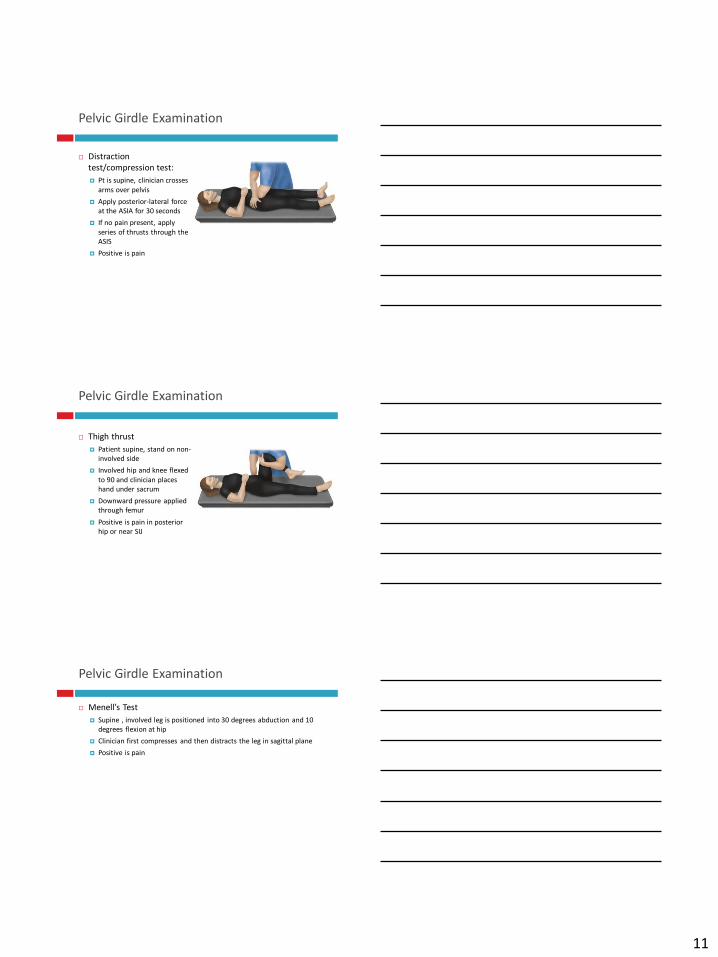
Pelvic Girdle Examination
Distraction
test/compression test:
Pt is supine, clinician crosses
arms over pelvis
Apply posterior-lateral force
at the ASIA for 30 seconds
If no pain present, apply
series of thrusts through the
ASIS
Positive is pain
Pelvic Girdle Examination
Thigh thrust
Patient supine, stand on non-
involved side
Involved hip and knee flexed
to 90 and clinician places
hand under sacrum
Downward pressure applied
through femur
Positive is pain in posterior
hip or near SIJ
Pelvic Girdle Examination
Menell’s Test
Supine , involved leg is positioned into 30 degrees abduction and 10
degrees flexion at hip
Clinician first compresses and then distracts the leg in sagittal plane
Positive is pain
12
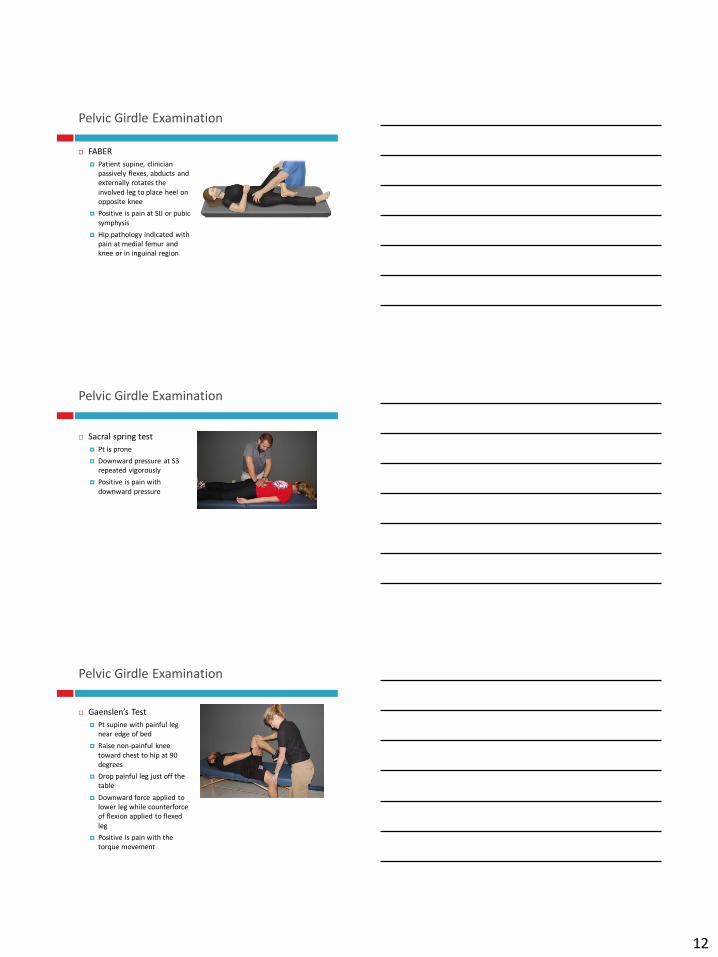
Pelvic Girdle Examination
FABER
Patient supine, clinician
passively flexes, abducts and
externally rotates the
involved leg to place heel on
opposite knee
Positive is pain at SIJ or pubic
symphysis
Hip pathology indicated with
pain at medial femur and
knee or in inguinal region
Pelvic Girdle Examination
Sacral spring test
Pt is prone
Downward pressure at S3
repeated vigorously
Positive is pain with
downward pressure
Pelvic Girdle Examination
Gaenslen’s Test
Pt supine with painful leg
near edge of bed
Raise non-painful knee
toward chest to hip at 90
degrees
Drop painful leg just off the
table
Downward force applied to
lower leg while counterforce
of flexion applied to flexed
leg
Positive is pain with the
torque movement
13
Pelvic Girdle Examination
Active Straight Leg Raise:
Pt is supine and asked to
raise involved leg 6” above the table
Then clinician stabilizes pelvis
and pt repeats
Perform B if B involvement
suspected
Positive is pain without
support, relieved with
support
Trendelenburg:
Patient stands with back to
clinician and actively flexes
hip and knee to 90 degrees
Positive is flexed hip
descends and pain at pelvic
joint
Pelvic Girdle Examination
Hip PROM
Flexion
Abduction/Adduction
Internal/External rotation
Positive is increased pain
Lunge
Patient asked to step forward
and shift weight over forward
leg.
Then flex forward hip and
knee to 90 degrees
Positive is increased pain
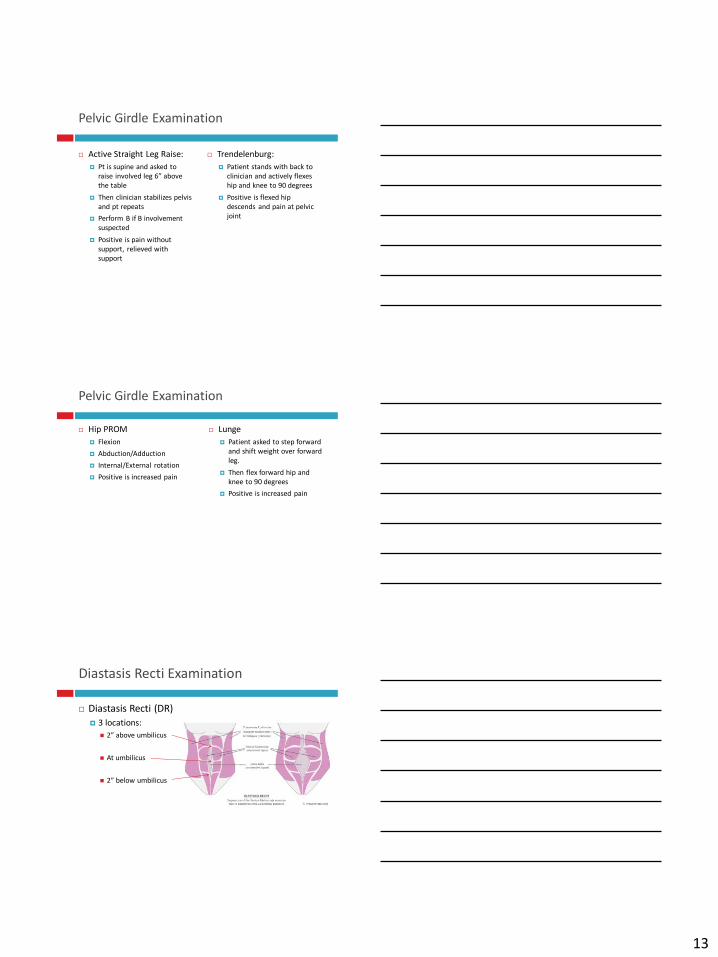
Diastasis Recti Examination
Diastasis Recti (DR)
3 locations:
2” above umbilicus
At umbilicus
2” below umbilicus
14
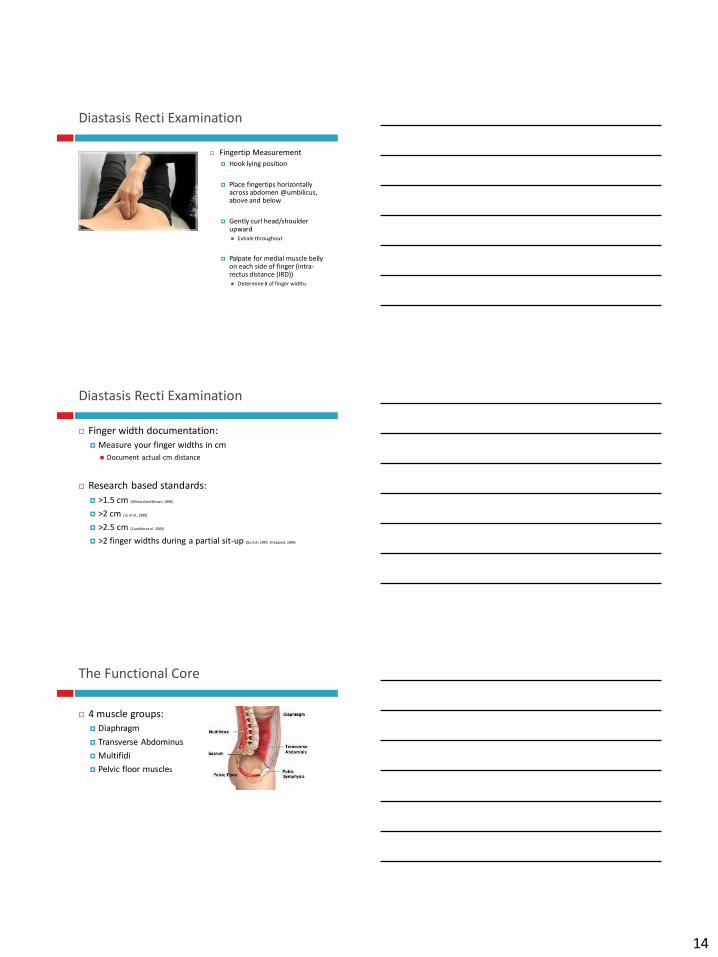
Diastasis Recti Examination
Fingertip Measurement
Hook lying position
Place fingertips horizontally across abdomen @umbilicus, above and below
Gently curl head/shoulder upward
Exhale throughout
Palpate for medial muscle belly on each side of finger (intra-rectus distance (IRD))
Determine # of finger widths
Diastasis Recti Examination
Finger width documentation:
Measure your finger widths in cm
Document actual cm distance
Research based standards:
>1.5 cm (Gilleard and Brown, 1996)
>2 cm (Lo et al.,1999)
>2.5 cm (Candido et al., 2005)
>2 finger widths during a partial sit-up (Bursch, 1987; Sheppard, 1996)
The Functional Core
4 muscle groups:
Diaphragm
Transverse Abdominus
Multifidi
Pelvic floor muscles
15
Functional Core Weakness
Common symptoms of weakness include:
Mid and low back pain with movement
Instability through pelvis, pelvic girdle, hips and lumbar
spine
Urinary and/or fecal incontinence
Poor balance reactions
Abnormal breathing patterns with movement
Carrying low during pregnancy
Increased waddling gait with pregnancy
Alignment Interventions
Clinton et el:
NO evidence that spinal manipulation and/or mobilization is harmful
to the antepartum female or fetus
Normal movement in all directions if advocated despite hypermobility
or laxity
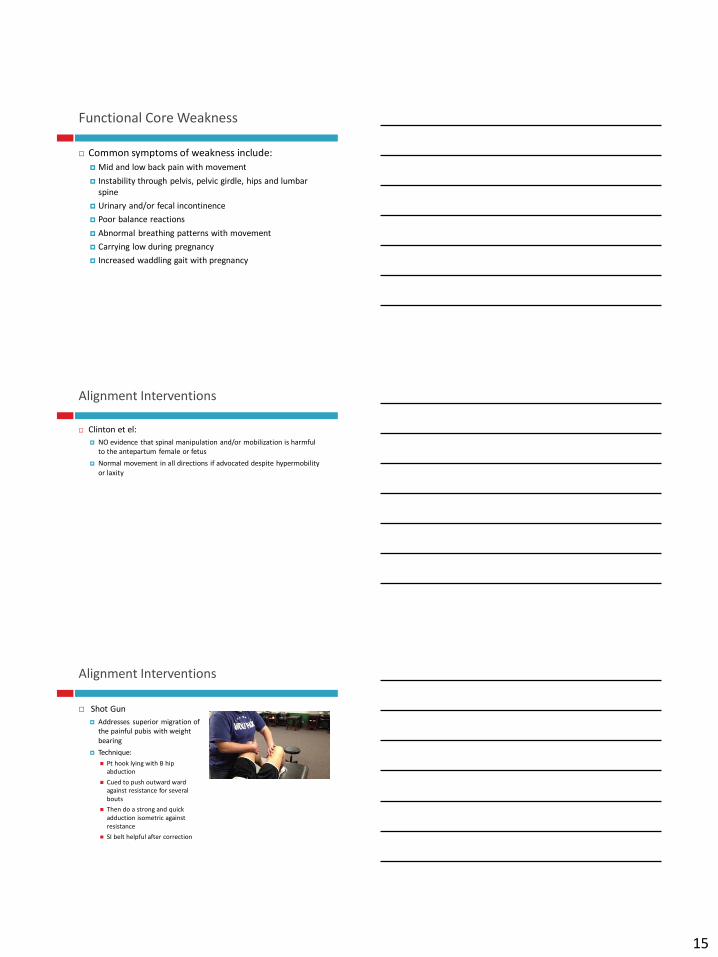
Alignment Interventions
Shot Gun
Addresses superior migration of
the painful pubis with weight
bearing
Technique:
Pt hook lying with B hip
abduction
Cued to push outward ward
against resistance for several
bouts
Then do a strong and quick
adduction isometric against
resistance
SI belt helpful after correction
16
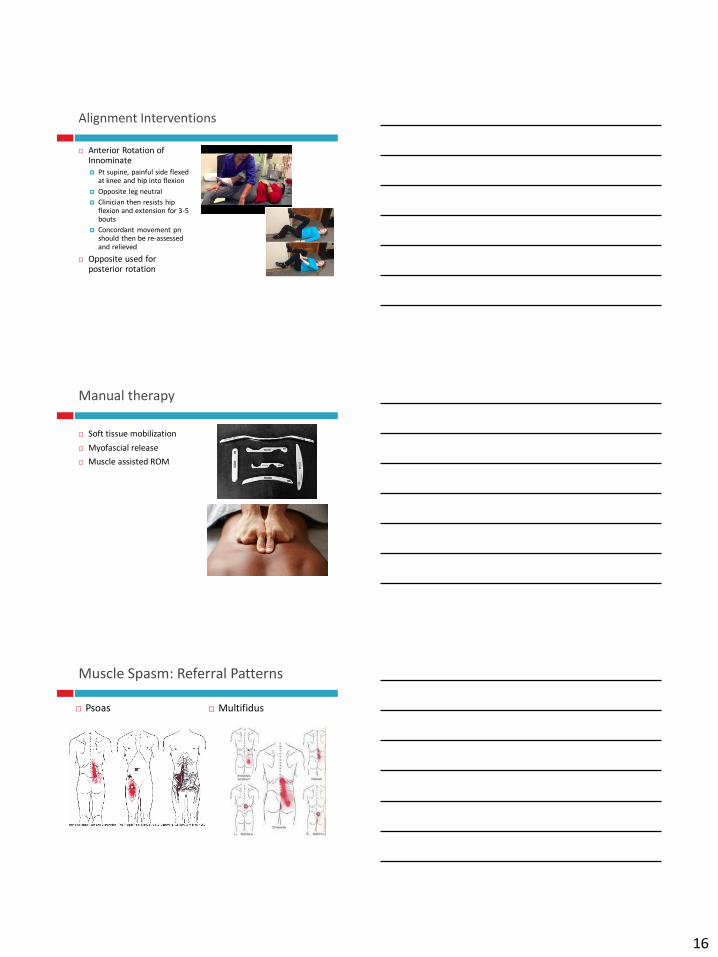
Alignment Interventions
Anterior Rotation of Innominate
Pt supine, painful side flexed at knee and hip into flexion
Opposite leg neutral
Clinician then resists hip flexion and extension for 3-5 bouts
Concordant movement pnshould then be re-assessed and relieved
Opposite used for posterior rotation
Manual therapy
Soft tissue mobilization
Myofascial release
Muscle assisted ROM
Muscle Spasm: Referral Patterns
Psoas Multifidus
17
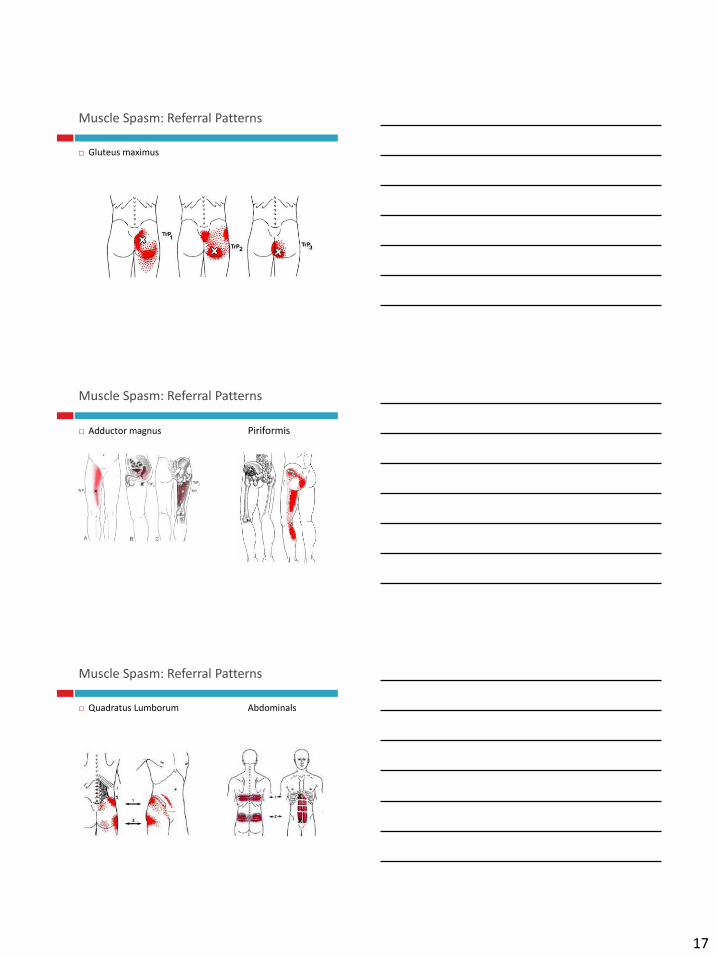
Muscle Spasm: Referral Patterns
Gluteus maximus
Muscle Spasm: Referral Patterns
Adductor magnus Piriformis
Muscle Spasm: Referral Patterns
Quadratus Lumborum Abdominals
18
Muscle Spasm: Referral Patterns
Pelvic floor muscle tension:
Results in pelvic pain
Referred abdominal pain
Unsafe Postures & Exercises
Prone with knees at the chest and buttocks elevated
Risk: Air embolism
B straight leg raises
Risk: Risk of diastasis and low back pain
Elevated fire hydrant exercise
Risk: Risk of SIJ and lumbar vertebrae stress
Elevated quadruped hip extension
Risk: Hyperextension of lumbar spine
Unilateral weight bearing exercise
Risk: SIJ irritation
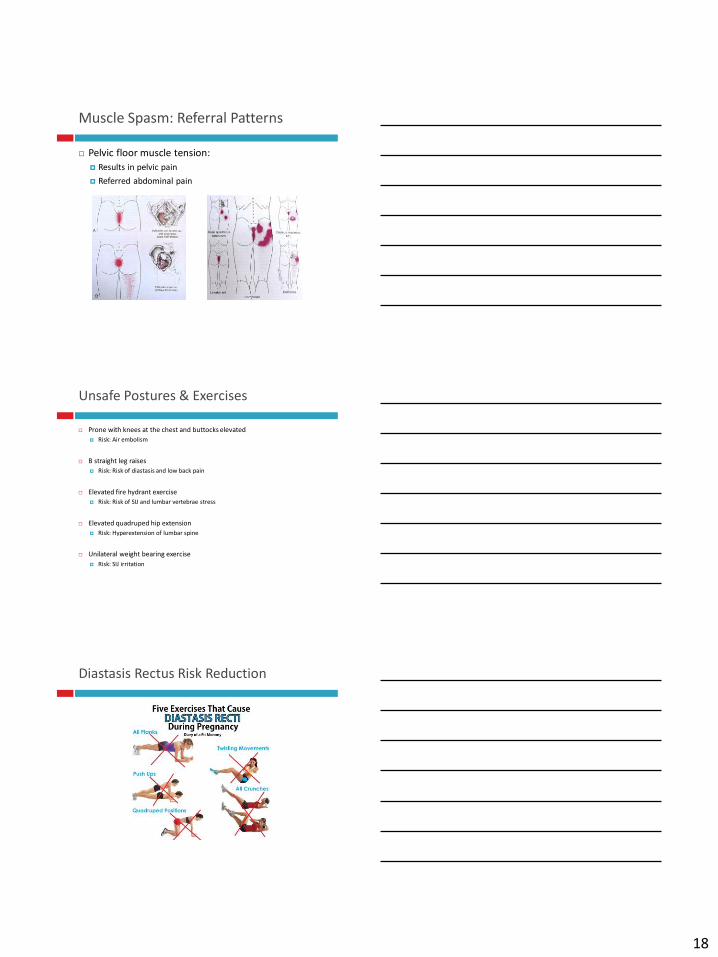
Diastasis Rectus Risk Reduction
19
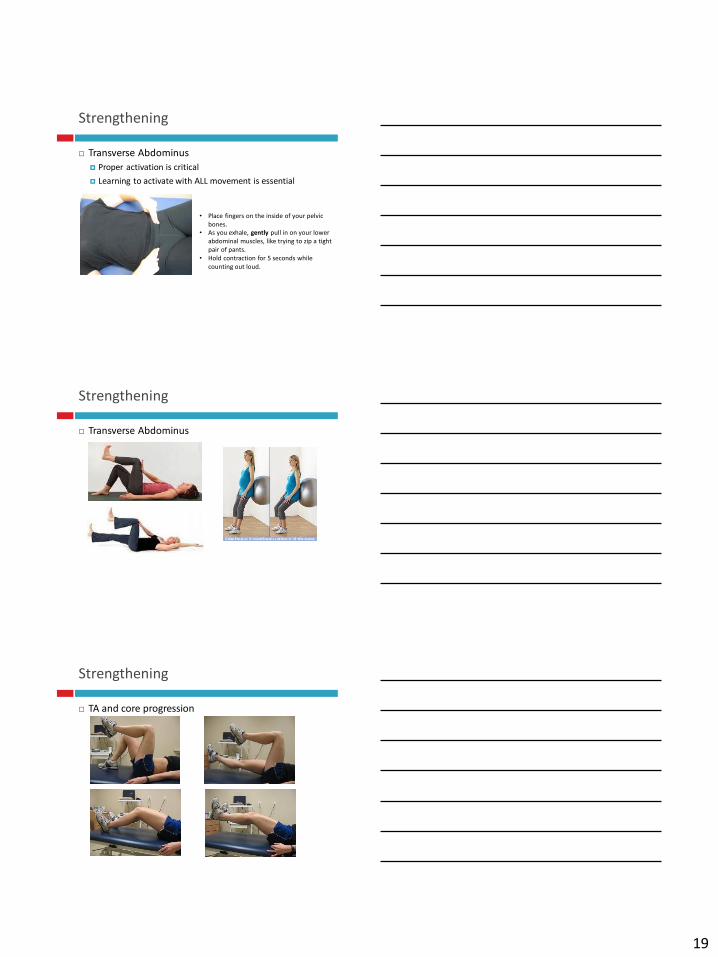
Strengthening
Transverse Abdominus
Proper activation is critical
Learning to activate with ALL movement is essential
• Place fingers on the inside of your pelvic
bones.
• As you exhale, gently pull in on your lower
abdominal muscles, like trying to zip a tight
pair of pants.
• Hold contraction for 5 seconds while
counting out loud.
Strengthening
Transverse Abdominus
Strengthening
TA and core progression
20
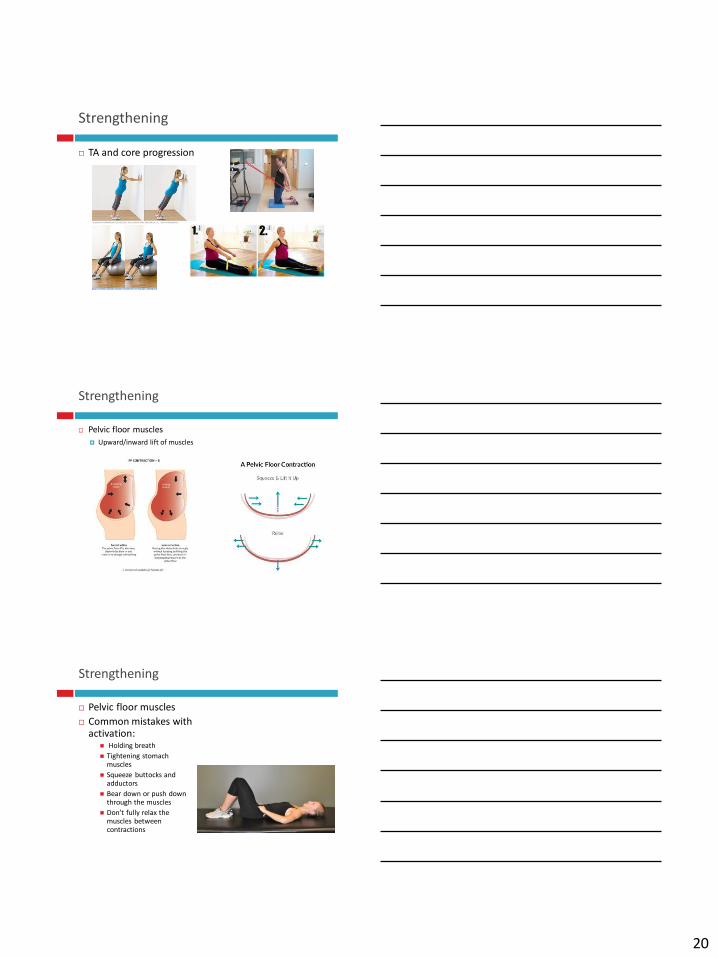
Strengthening
TA and core progression
Strengthening
Pelvic floor muscles
Upward/inward lift of muscles
Strengthening
Pelvic floor muscles
Common mistakes with activation:
Holding breath
Tightening stomach muscles
Squeeze buttocks and adductors
Bear down or push down through the muscles
Don’t fully relax the muscles between contractions
21
Strengthening
Pelvic floor muscles
Endurance activation: target slow twitch fibers
Sustained contraction, adequate rest duration
Exercise ideas:
Begin with 3 sec hold, 10 sec rest x 5
Increase reps to 10 as able
Slowly increase duration of hold, maintain 10 sec rest
Goal 10 sec hold
Quick activation: targets fast twitch fibers
Quick activation, full contract and relax
Exercise ideas:
Begin with cadence of 1 sec contract: 3 sec relax
10 quick activations at 1:3 cadence
Slowly increase speed to 1:2 cadence
Ex progression: 5 quick contractions, 10 sec rest x 3-5
Stretching
Cervical region:
Cervical, levator scapulae, upper traps, pectoralis
Mid spine:
Pectoralis, rhomboids, latissimus dorsi, upper trap, levator scapulae
Lumbar spine/pelvis:
Abdominals, hip flexion, gluteals, piriformis
LE:
TFL/IT band, quadriceps, adductors, abductors, gastroc/soleus
Body Mechanics: Getting out of Bed
DO follow these steps:
1. Bend your knees and scoot to side opposite
which you will get out of bed.
3. Roll on your side toward the side you are getting
out on.
4. Drop your legs off the bed.
5. Cross your arms as shown in the picture with
your bottom arm bent at the elbow and your upper
crossed so your palm is on the bed.
6. Exhale as you push up to sitting using your elbow
and hand.
REVERSE these steps to safely get into bed.
Do NOT: Sit straight up in bed from a laying doing
position. This puts a high amount of stress on your
back!!
1 2 3
4 5 6
22
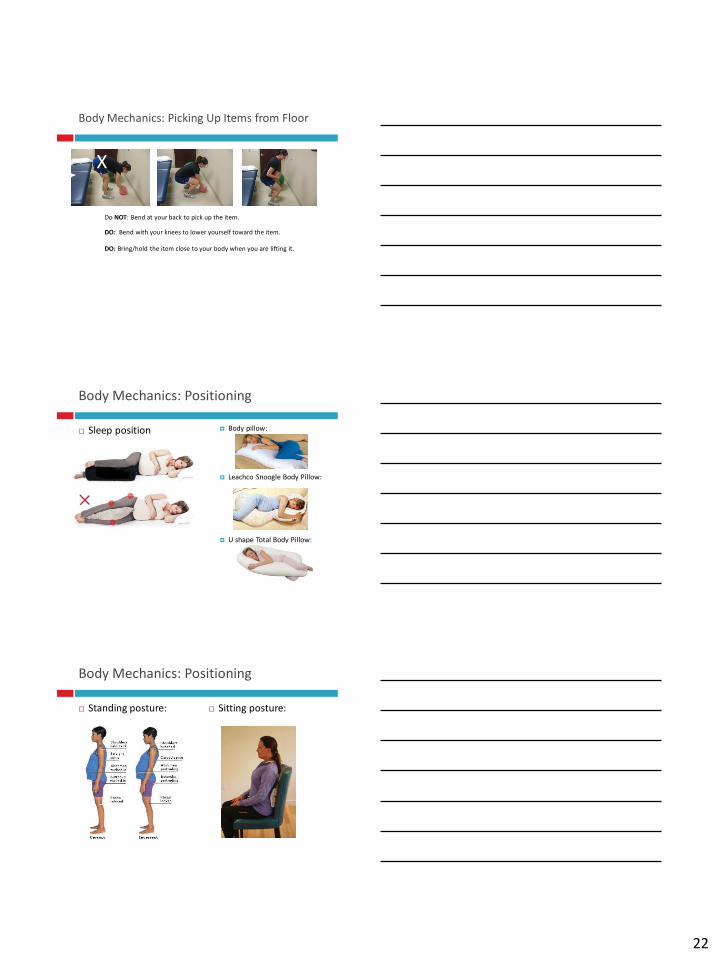
Body Mechanics: Picking Up Items from Floor
X
DO: Bend with your knees to lower yourself toward the item.
Do NOT: Bend at your back to pick up the item.
DO: Bring/hold the item close to your body when you are lifting it.
Body Mechanics: Positioning
Sleep position Body pillow:
Leachco Snoogle Body Pillow:
U shape Total Body Pillow:
Body Mechanics: Positioning
Standing posture: Sitting posture:
23
Support Devices
SIJ support
Serola SI Belt: $44
SIJ/abdominal support
Mother to Be: $39
Support Devices
Compression stockings
Over the counter is typically 12-15 mmHg
Ideally 20-30 mmHg
SmartWool PhD Graduated Compression Socks
Panty hose: no compression at abdomen
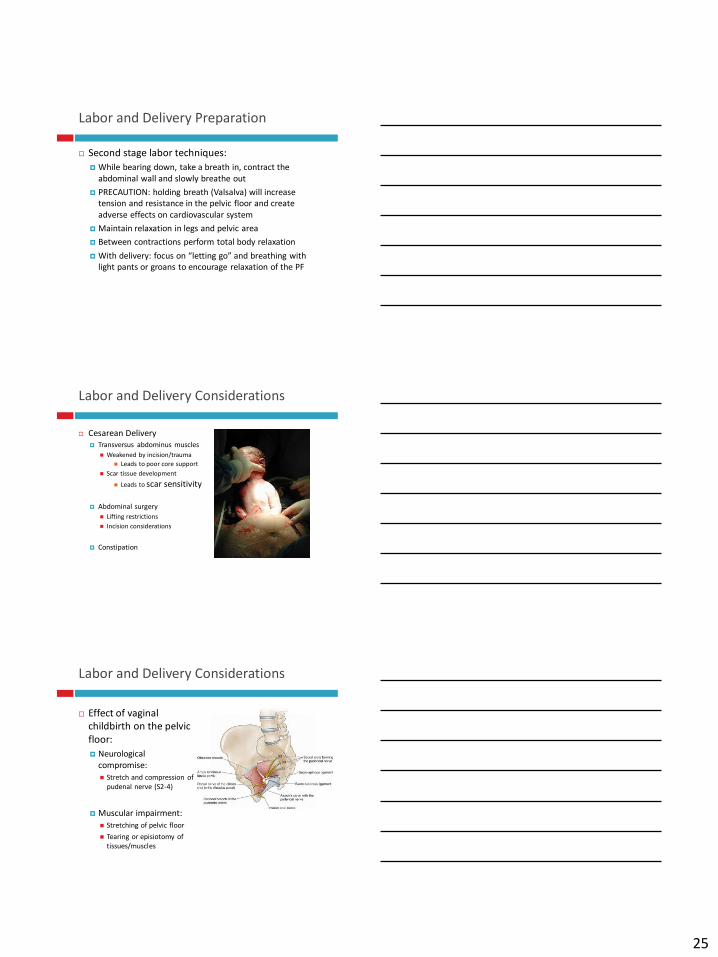
Generalized Exercise Recommendations
Strongly recommended that women
continue mild to moderate exercise based
on pre-pregnancy fitness levels.
No evidence indicating need to reduce
intensity but should be aware that heart
rate with vary as well as respiratory rate.
Use Borg scale of perceived exertion:
between 12-14
Never exercise to exhaustion
24
Exercise Contraindications
Incompetent cervix/early
dilation
Vaginal bleeding
Placenta previa
Pre-eclampsia
Maternal heart disease
Maternal Type 1 diabetes
Gestational diabetes
Severe anemia
Extreme fatigue
Overheating
Diastasis recti
Absolute: Precaution:
Labor and Delivery Considerations
Cesarean is indicated with:
Placenta previa
Placenta abruption
Transient osteoporosis
Severe pubic symphysis separation
Breech position
Labor and Delivery Preparation
Vaginal birth preparation exercise:
Visual imagery: concentrate on a relaxing image throughout pregnancy for use later with delivery
Muscle setting: guided contract/relax from feet to head
Focus on the contrasting sensations
Add deep breathing
Selective tension: progression of muscle setting by focusing on relaxing one area while the other is contracting
Breathing: slow, deep diaphragmatic breathing
25
Labor and Delivery Preparation
Second stage labor techniques:
While bearing down, take a breath in, contract the
abdominal wall and slowly breathe out
PRECAUTION: holding breath (Valsalva) will increase
tension and resistance in the pelvic floor and create
adverse effects on cardiovascular system
Maintain relaxation in legs and pelvic area
Between contractions perform total body relaxation
With delivery: focus on “letting go” and breathing with light pants or groans to encourage relaxation of the PF
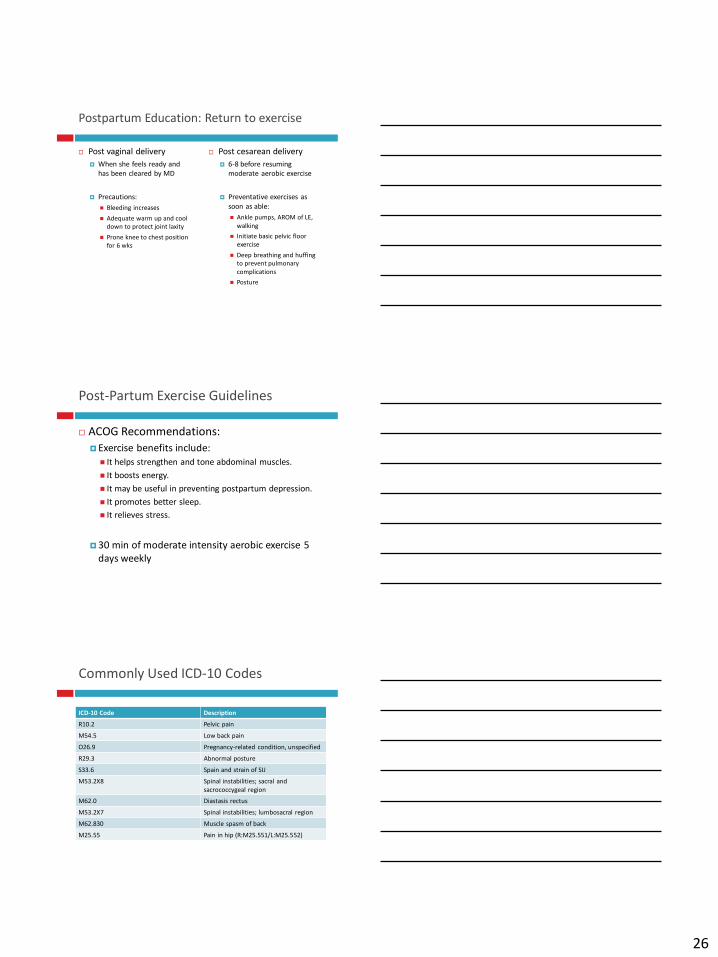
Labor and Delivery Considerations
Cesarean Delivery
Transversus abdominus muscles
Weakened by incision/trauma
Leads to poor core support
Scar tissue development
Leads to scar sensitivity
Abdominal surgery
Lifting restrictions
Incision considerations
Constipation
Labor and Delivery Considerations
Effect of vaginal
childbirth on the pelvic
floor:
Neurological
compromise:
Stretch and compression of
pudenal nerve (S2-4)
Muscular impairment:
Stretching of pelvic floor
Tearing or episiotomy of
tissues/muscles
26
Postpartum Education: Return to exercise
Post vaginal delivery
When she feels ready and
has been cleared by MD
Precautions:
Bleeding increases
Adequate warm up and cool
down to protect joint laxity
Prone knee to chest position
for 6 wks
Post cesarean delivery
6-8 before resuming
moderate aerobic exercise
Preventative exercises as
soon as able:
Ankle pumps, AROM of LE,
walking
Initiate basic pelvic floor
exercise
Deep breathing and huffing
to prevent pulmonary
complications
Posture
Post-Partum Exercise Guidelines
ACOG Recommendations:
Exercise benefits include:
It helps strengthen and tone abdominal muscles.
It boosts energy.
It may be useful in preventing postpartum depression.
It promotes better sleep.
It relieves stress.
30 min of moderate intensity aerobic exercise 5
days weekly
Commonly Used ICD-10 Codes
ICD-10 Code Description
R10.2 Pelvic pain
M54.5 Low back pain
O26.9 Pregnancy-related condition, unspecified
R29.3 Abnormal posture
S33.6 Spain and strain of SIJ
M53.2X8 Spinal instabilities; sacral and
sacrococcygeal region
M62.0 Diastasis rectus
M53.2X7 Spinal instabilities; lumbosacral region
M62.830 Muscle spasm of back
M25.55 Pain in hip (R:M25.551/L:M25.552)
27
Assessment Scale Recommendations
Pelvic Girdle/SIJ Pain
Pelvic Girdle Questionnaire
Low Back Pain
Oswestry Questionnaire
General Function:
SF-8
Questions?
Also, make plans to join us
for:
Postpartum Recovery:
Improving Function for
Mothers
November 30th