Embed Size (px)
Citation preview
Post-MI Follow-up and Sudden Death Prevention
Steve Wilton MD
EP Cardiology
University of Calgary
ACC Rockies
March 3, 2020

Disclosures
▪ Research grants: Medtronic, Abbott, Boston Scientific

Importance of collaboration

Outline
▪ Post-MI sudden death – pathophysiology and epidemiology
▪ Risk stratification for SCD post MI – LVEF and beyond
▪ Recommendations for follow-up – how are we doing?
▪ Can beta-blockers be withdrawn post-MI?

Case vignette
▪ Case : Mrs. Blue is a 68 year-old female admitted with an inferior wall STEMI. She was successfully treated with primary PCI to the culprit RCA 9 hours after symptom onset, and had non-significant stenoses in other vessels. A left ventriculogram at the time of PCI revealed inferior and posterolateral wall severe hypokinesis and overall moderate left ventricular dysfunction (LVEF 40%). She is an obese, sedentary smoker, but has no prior cardiac history. Her course in hospital has been uneventful, and she is ready for discharge.
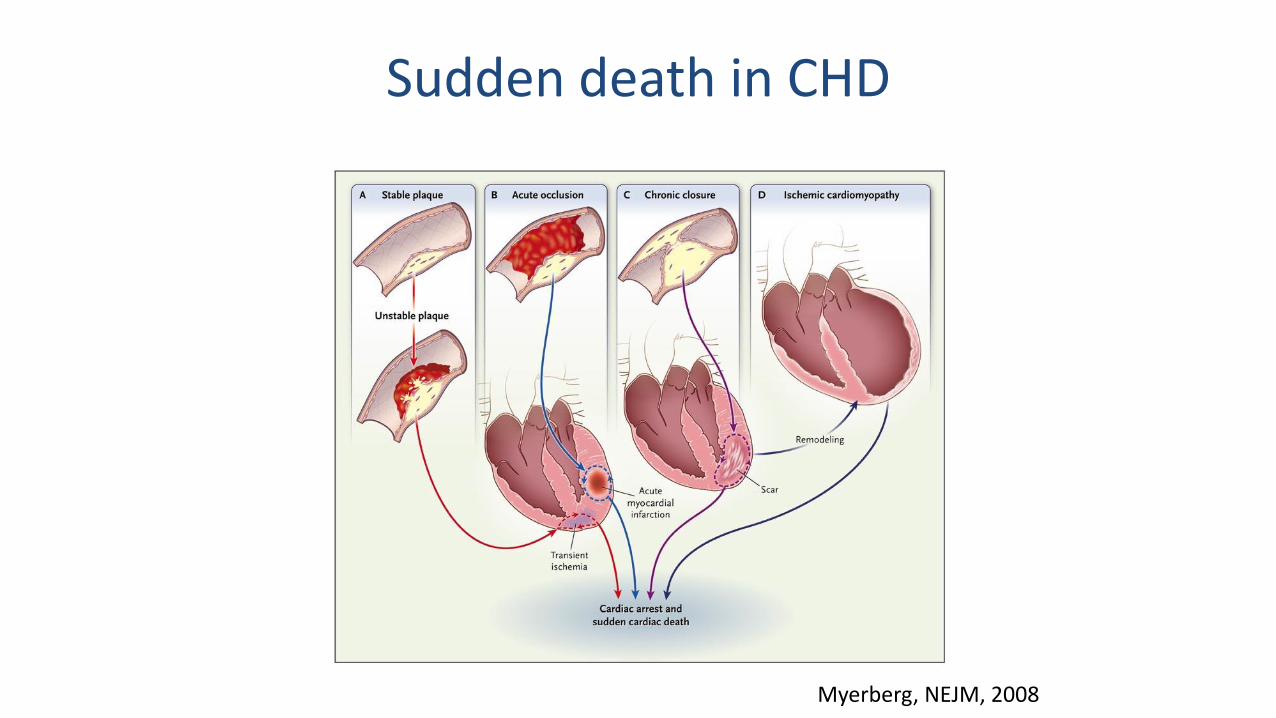
Sudden death in CHD
Myerberg, NEJM, 2008

Sudden Death Early and Late after MI
Solomon, N Engl J Med. 2005;352:2581–2588 Pouleur, Circulation. 2010;122:597–602
VALIANT Trial

Failure of Early Defibrillator Therapy
Implanted: DINAMITHohnloser SH et al. N Engl J Med 2004;351:2481-2488.
Wearable: VESTOlgin JE et el. N Engl J Med. 2018;379:1205-1215.

Problem of predicting SCD in CHD
▪ 50% of CHD deaths are sudden
▪ 80% of SCD occurs in setting of CHD
Myerberg, Circulation, 1992

0
25
50
75
100
Pro
port
ion (
%)
Limitations of LVEF
Most Identified Are Not At High Risk
Fails to Identify Most of Those at
Risk
Exner. Curr Opin Cardiol 2009, 24:61–7

Development of a Cardiac Arrest
Moss & Zareba J Electrocardiol 2003;36:101-8
Autonomic Nervous System
Underlying Fixed
Substrate
Dynamic Substrate

Combined Parameter Testing
Cardiac Death or Cardiac Arrest
Remaining
HRT + TWA& EF < 0.50
322 post-MI patientsserial assessment(2-4 & 10-14 weeks)
Later testing more accurate6-fold higher risk with abnormal HRT + TWA
Sensitivity: 55%
+ PV: 27% (NNT ~ 4)
- PV: 96%
Exner et al. JACC 2007;50:2275-84.

Risk Estimation Following InfarctionNoninvasive Evaluation: ICD efficacy
EF 0.36 to 0.50 2-60 mo. post-MI> 3 mo. post-revasc.< 80 years & without dialysis, perm AF or AAD
Holter
Abnormal TWA + HRT
Registry
Usual Care Alone
Usual Care + ICD
Minimum follow-up: 2 yearsMean follow-up: 5 years
1° outcome: mortality

Guidelines for Post-MI LVEF Reassessment
2016 CCS ICD Guideline
▪ If in-hospital LVEF ≤ 0.45, repeat in ≥3 months if revasc, or ≥40 days if no revasc
2017 ESC STEMI Guideline
▪ If pre-discharge LVEF ≤ 0.40, repeat in 6-12 weeks on OMT
Bennett M et al., Can J Cardiol. 2017;33:174-188.Ibanez B et al., Eur Heart J. 2018;39:119-177

LVEF Reassessment: Practice variability
Predictors of F/U LVEF
▪ Male sex (trend)
▪ Health insurance
▪ Cardiologist follow-up <1mo
TRIUMPH Registry
Miller, Am Heart J. 2013;166:737-43.
35%

Follow-up LVEF post-MI: How are we doing?
OBSERVATION: 2010-2011
3,318 MIs
321 (10%)LVEF
impaired
152 (47%)follow up
LVEF obtained
169 (53%)no follow up LVEF
obtained
2,997LVEF
preserved
Chew DS et al, Am. Heart J. 2018;198:91-96
INTERVENTION: 2011-2014
5,964 MIs
695 (12%)LVEF
impaired
442 (64%)follow up
LVEF obtained
253 (36%)no follow up LVEF
obtained
5,269LVEF
preserved

Post-MI follow up and SCD risk
Chew DS et al, Am. Heart J. 2018;198:91-96
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
90.0
Initial FollowUp
Moderate LVEF Reduction Group
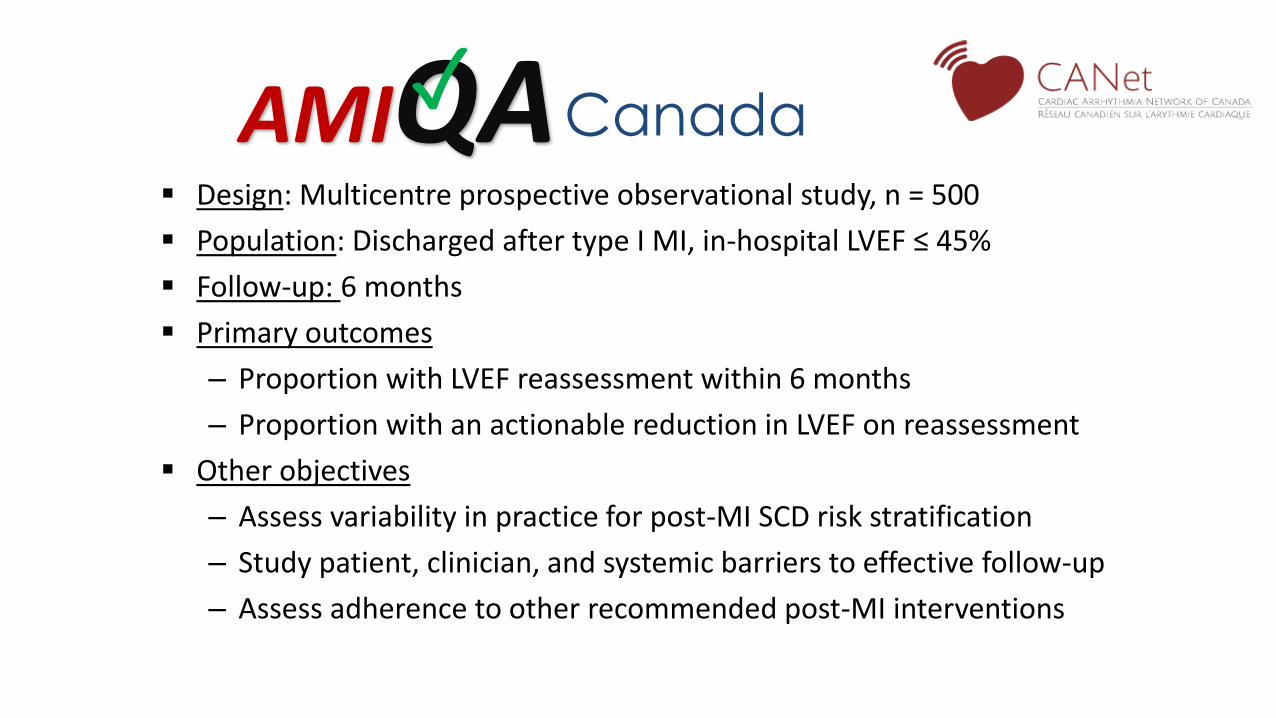
Canada ▪ Design: Multicentre prospective observational study, n = 500
▪ Population: Discharged after type I MI, in-hospital LVEF ≤ 45%
▪ Follow-up: 6 months
▪ Primary outcomes
– Proportion with LVEF reassessment within 6 months
– Proportion with an actionable reduction in LVEF on reassessment
▪ Other objectives
– Assess variability in practice for post-MI SCD risk stratification
– Study patient, clinician, and systemic barriers to effective follow-up
– Assess adherence to other recommended post-MI interventions
AMIQA✓

Canada
▪ 15 Sites – Academic and Community
▪ Enrolled, follow-up complete March 2020
▪ Synergy with REFINE ICD
AMIQA✓
Back to our case
Mrs. Blue returns for follow-up, 4 months post-MI.
▪ No angina, no HF symptoms, normal exam
▪ Notices cold hands and feet, some fatigue
▪ ECG: inferior Qs, Echo pending
▪ Has ‘nearly quit’ smoking, is participating in rehab
▪ Rx: ASA, ticagrelor 60 BID, bisoprolol 5mg, atorvastatin 80mg, perindopril 8mg
▪ Wants to know if she still needs all of these meds. . .
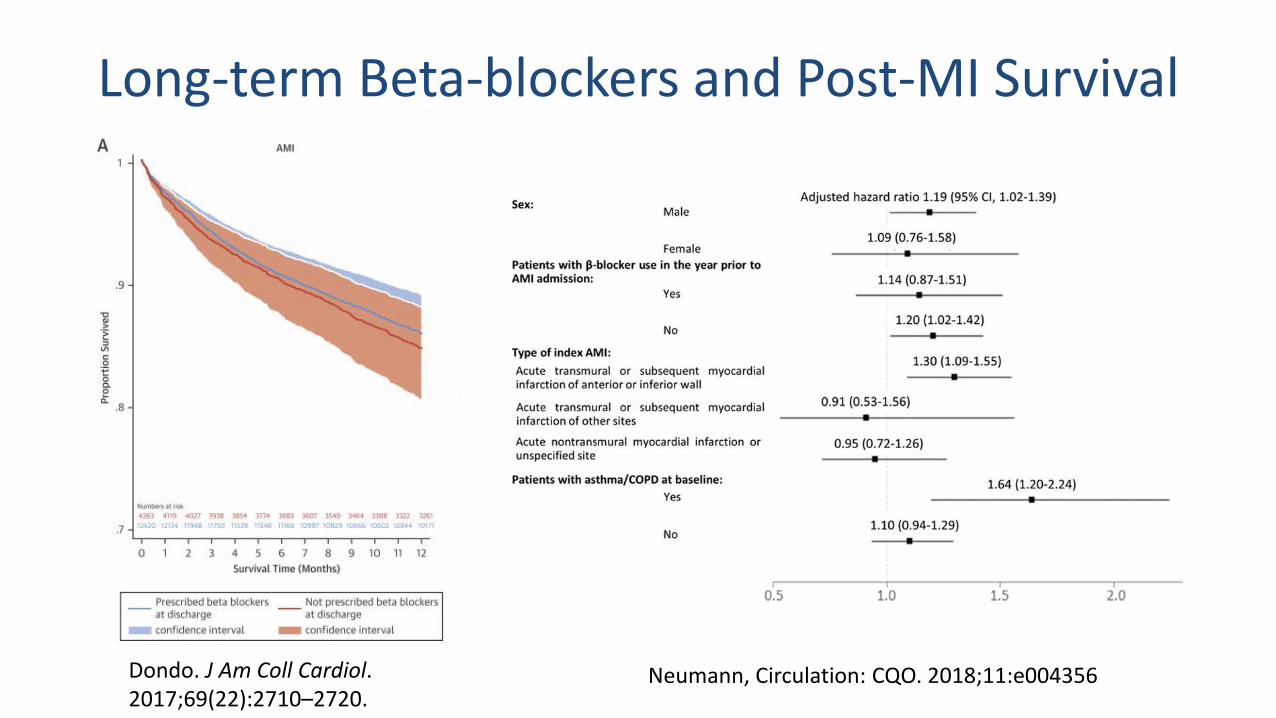
Long-term Beta-blockers and Post-MI Survival
Dondo. J Am Coll Cardiol. 2017;69(22):2710–2720.
Neumann, Circulation: CQO. 2018;11:e004356

ACE/ARB, Statin or BB: Which can be stopped?
Korhonen, J Am Coll Cardiol. 2017;70(13):1543–1554.
Take Home Points
▪ LVEF is a crude marker of SCD risk, but nothing has beat it yet.
▪ Post-MI LV function recovery is variable, and predicts outcome.
▪ Reassessment of LV function at ~3mo when in-hospital LVEF is reduced can identify patients at risk of sudden death.
▪ Long-term role of beta-blockers is unclear: Ongoing trials will help.