Embed Size (px)
Citation preview
Positive Rechallenge: What Clinical Trial Data Tell Us Julie Papay, Pharm.D. UCB BioSciences Global Patient Safety Drug-Induced Liver Injury (DILI) Conference XVI Wednesday 23 March 2016
The comments provided here are solely those of the presenter and are not necessarily reflective of the positions, policies, or practices of UCB BioSciences
2
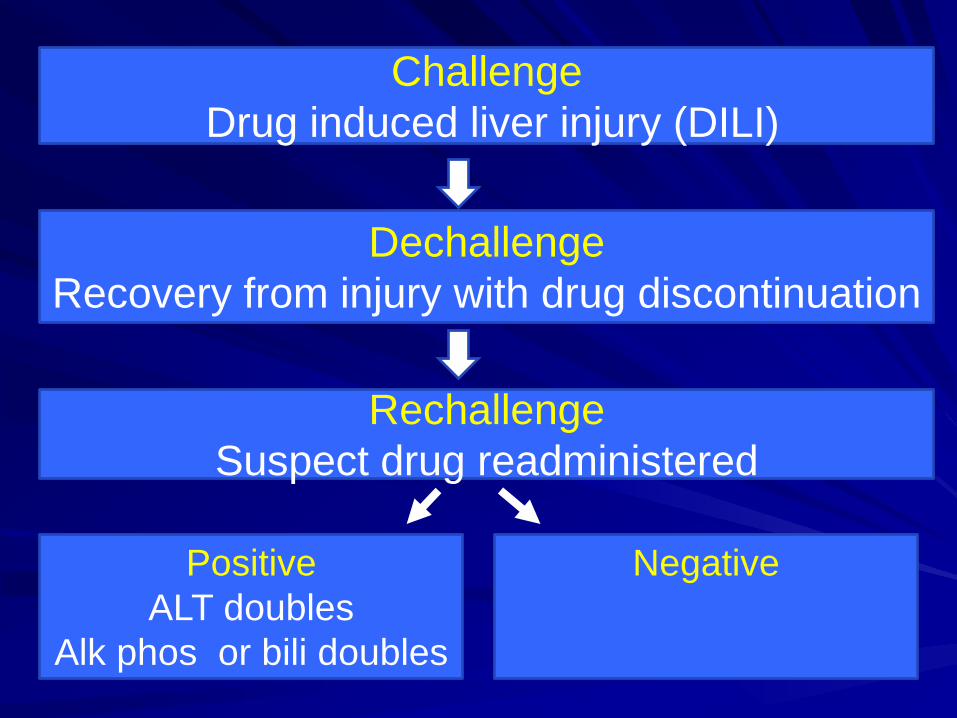
Challenge Drug induced liver injury (DILI)
Dechallenge Recovery from injury with drug discontinuation
Rechallenge Suspect drug readministered
Negative
Positive ALT doubles
Alk phos or bili doubles
Rechallenge Points to Consider
Pros Enables lifesaving drug
use Positive rechallenge can
confirm DILI diagnosis Negative rechallenge may
imply adaptation (e.g., isoniazid, statins, tacrine)
Clinical trial data may inform which subjects more safely rechallenged
Cons 2-13% fatal (e.g., halothane) FDA advises avoidance1 Rapid onset of liver injury Frequently inadvertent High risk without rigorous
clinical monitoring
1FDA Guidance for Industry, July 2009, http://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/UCM174090.pdf
Drug Induced Liver Injury (DILI) and Rechallenge in Clinical Trials: Sparse Data
Sparse information
Rechallenge Criteria
Clinical Monitoring/ Stopping
Criteria
Preclinical Screening
Positive Rechallenge in Clinical Trials:
Recent New Drug Approvals
Improved preclinical screening/testing yields safer therapeutics Rigorous safety with drug stopping criteria Provides most optimistic data on drug rechallenge
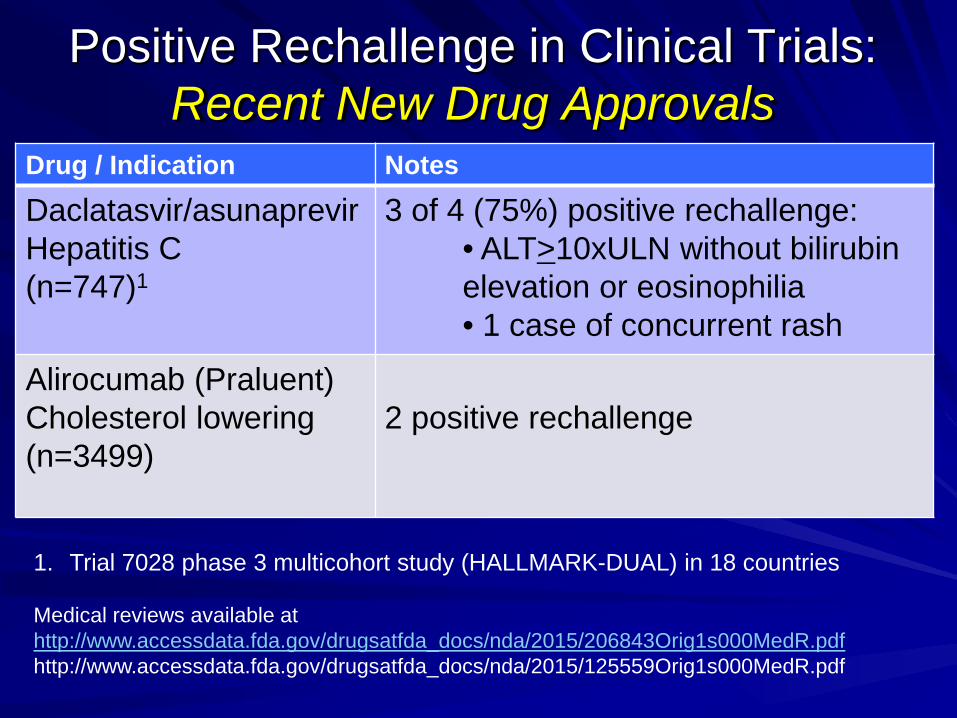
Positive Rechallenge in Clinical Trials: Recent New Drug Approvals
Drug / Indication Notes
Daclatasvir/asunaprevir Hepatitis C (n=747)1
3 of 4 (75%) positive rechallenge: • ALT>10xULN without bilirubin elevation or eosinophilia • 1 case of concurrent rash
Alirocumab (Praluent) Cholesterol lowering (n=3499)
2 positive rechallenge
1. Trial 7028 phase 3 multicohort study (HALLMARK-DUAL) in 18 countries Medical reviews available at http://www.accessdata.fda.gov/drugsatfda_docs/nda/2015/206843Orig1s000MedR.pdf http://www.accessdata.fda.gov/drugsatfda_docs/nda/2015/125559Orig1s000MedR.pdf
All re-administration occurred within 24 days
ALT>10xULN with rechallenge in 3 subjects – 1 case of concurrent rash – no bilirubin elevations or eosinophilia
2 of 4 recovered; 2 recovery unreported
Daclatasvir/Asunaprevir: 75% Positive Rechallenge
Event 1: Mean 66 days (42-84 days)
Event 2: Mean 5 days (3-6 days)
Medical review for Daklinza available at http://www.accessdata.fda.gov/drugsatfda_docs/nda/2015/206843Orig1s000MedR.pdf
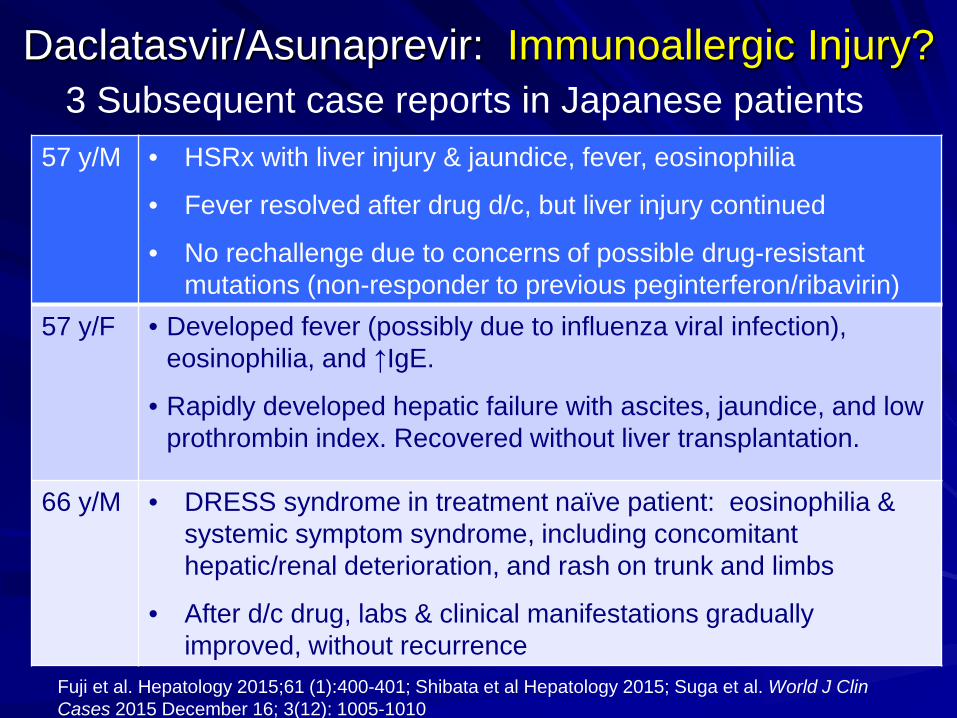
57 y/M • HSRx with liver injury & jaundice, fever, eosinophilia
• Fever resolved after drug d/c, but liver injury continued
• No rechallenge due to concerns of possible drug-resistant mutations (non-responder to previous peginterferon/ribavirin)
57 y/F • Developed fever (possibly due to influenza viral infection), eosinophilia, and ↑IgE.
• Rapidly developed hepatic failure with ascites, jaundice, and low prothrombin index. Recovered without liver transplantation.
66 y/M • DRESS syndrome in treatment naïve patient: eosinophilia & systemic symptom syndrome, including concomitant hepatic/renal deterioration, and rash on trunk and limbs
• After d/c drug, labs & clinical manifestations gradually improved, without recurrence
Daclatasvir/Asunaprevir: Immunoallergic Injury? 3 Subsequent case reports in Japanese patients
Fuji et al. Hepatology 2015;61 (1):400-401; Shibata et al Hepatology 2015; Suga et al. World J Clin Cases 2015 December 16; 3(12): 1005-1010
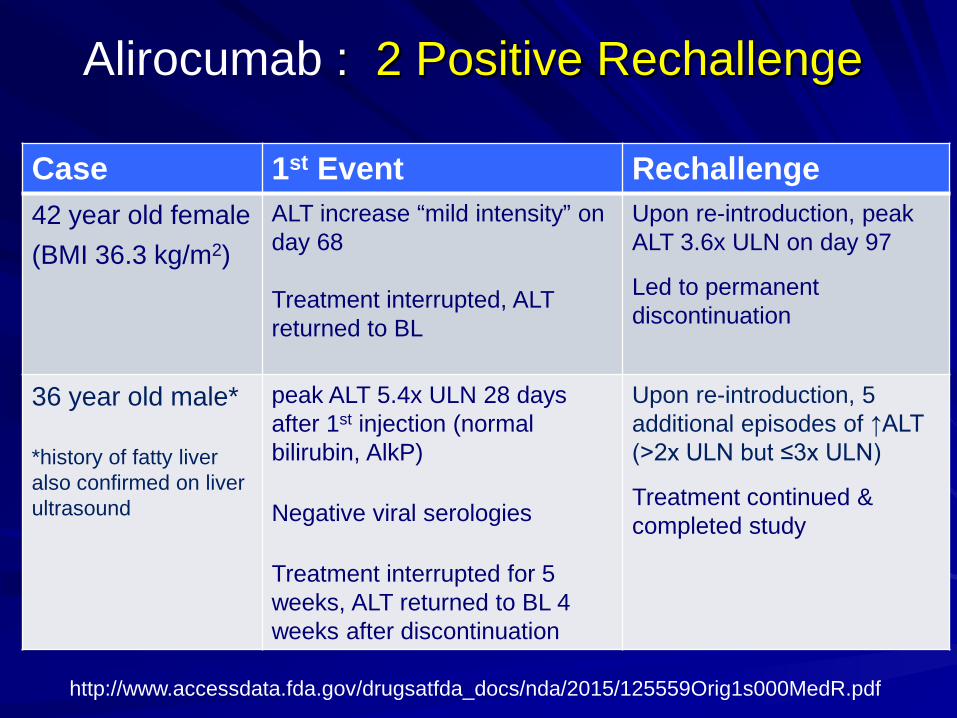
Alirocumab : 2 Positive Rechallenge
Case 1st Event Rechallenge 42 year old female (BMI 36.3 kg/m2)
ALT increase “mild intensity” on day 68 Treatment interrupted, ALT returned to BL
Upon re-introduction, peak ALT 3.6x ULN on day 97
Led to permanent discontinuation
36 year old male*
*history of fatty liver also confirmed on liver ultrasound
peak ALT 5.4x ULN 28 days after 1st injection (normal bilirubin, AlkP)
Negative viral serologies
Treatment interrupted for 5 weeks, ALT returned to BL 4 weeks after discontinuation
Upon re-introduction, 5 additional episodes of ↑ALT (>2x ULN but ≤3x ULN)
Treatment continued & completed study
http://www.accessdata.fda.gov/drugsatfda_docs/nda/2015/125559Orig1s000MedR.pdf
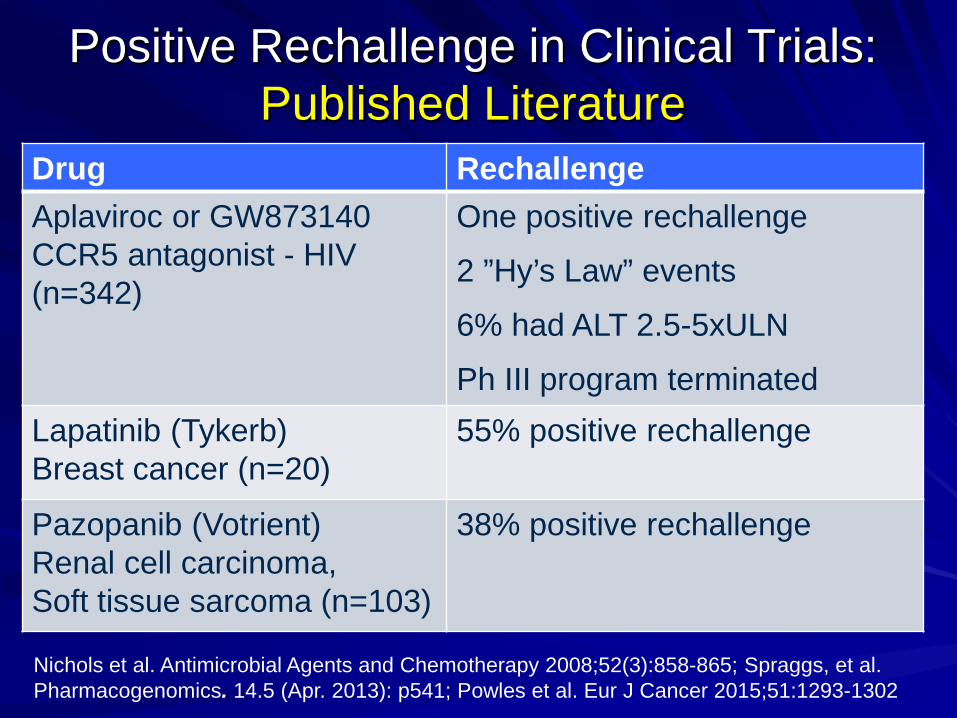
Positive Rechallenge in Clinical Trials: Published Literature
Drug Rechallenge Aplaviroc or GW873140 CCR5 antagonist - HIV (n=342)
One positive rechallenge
2 ”Hy’s Law” events
6% had ALT 2.5-5xULN
Ph III program terminated Lapatinib (Tykerb) Breast cancer (n=20)
55% positive rechallenge
Pazopanib (Votrient) Renal cell carcinoma, Soft tissue sarcoma (n=103)
38% positive rechallenge
Nichols et al. Antimicrobial Agents and Chemotherapy 2008;52(3):858-865; Spraggs, et al. Pharmacogenomics. 14.5 (Apr. 2013): p541; Powles et al. Eur J Cancer 2015;51:1293-1302
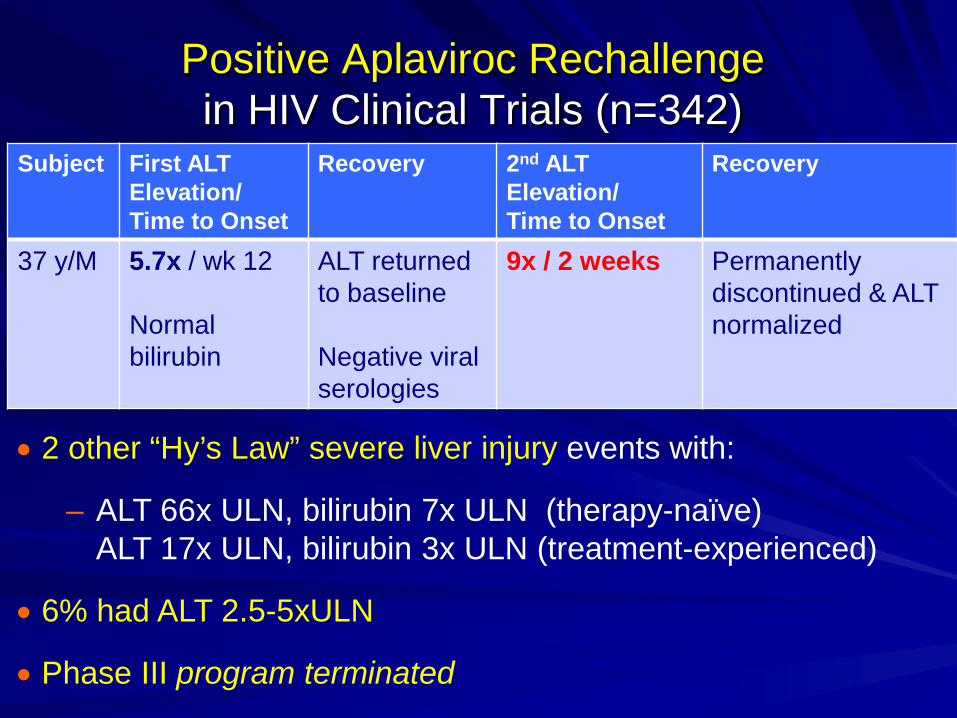
Subject First ALT Elevation/ Time to Onset
Recovery 2nd ALT Elevation/ Time to Onset
Recovery
37 y/M
5.7x / wk 12 Normal bilirubin
ALT returned to baseline Negative viral serologies
9x / 2 weeks Permanently discontinued & ALT normalized
Positive Aplaviroc Rechallenge in HIV Clinical Trials (n=342)
• 2 other “Hy’s Law” severe liver injury events with:
– ALT 66x ULN, bilirubin 7x ULN (therapy-naïve) ALT 17x ULN, bilirubin 3x ULN (treatment-experienced)
• 6% had ALT 2.5-5xULN
• Phase III program terminated
Liver chemistry: – Entry criteria: ALT/AST ≤2.5ULN and total
bilirubin ≤ 1.5ULN – Post-baseline liver chemistry tests every 3 or 4
weeks Rechallenge considered for isolated ALT >8x ULN …
Pazopanib: 103 Patients Rechallenged in 9 Prospective Phase II/III Studies (n=2080)
Powles et al. Eur J Cancer 2015;51:1293-1302 and http://www.accessdata.fda.gov/drugsatfda_docs/nda/2009/022465s000_MedR.pdf
Rechallenged only if clinical benefit was observed and all criteria were met: – ALT ≤ 2.5x ULN – Total bilirubin <1.5xULN or direct bilirubin
≤35% – No hypersensitivity signs or symptoms – Subject reconsented
Required reduced dose & close monitoring Powles et al. Eur J Cancer 2015;51:1293-1302 and http://www.accessdata.fda.gov/drugsatfda_docs/nda/2009/022465s000_MedR.pdf
Pazopanib: 103 Patients Rechallenged in 9 Prospective Phase II/III Studies (n=2080)
• 38% positive rechallenge suggests adaptation?
• Recurrence of transaminitis happened soon after reintroduction of treatment (median 9 days)
• Upon rechallenge: • no ALT >20 ULN • ALT elevation >8 ULN noted in 21% • ALT>5-8x ULN noted in 79%
• No cases of liver failure after rechallenge
• Rechallenge should only be undertaken with close monitoring of liver chemistry
15
Pazopanib Positive Rechallenge Occurs More Rapidly: Injury More Common with HLA-B*57:01
HLA-B*57:01 associated with liver injury
• Lapatinib monotherapy study in breast cancer (n=1194): – 2% developed ALT >5x ULN
– 55% positive rechallenge with lapatinib reinitiation (n=20)
• HLA DQA1*02:01 and DRB1*07:01 markers increase risk of liver injury events with:
– 8% developing ALT >5x ULN when carrying HLA alleles vs. 0.5% exhibiting ALT >5x ULN without HLA markers
• HLA markers present in 15-25% of Caucasian, Asian, African and Hispanic; 1% in Japanese
Spraggs C, et al. Pharmacogenomics. 2013:14(5):541.
Lapatinib: 55% Positive Rechallenge: Immunoallergic Injury
• U.S. Prescribing information has boxed warning:
• Hepatotoxicity may be severe and deaths have been reported
• “Hy’s Law” severe liver injury in clinical trials (<1%)
• Immunoallergic and autoimmune features are uncommon, but linked to specific HLA alleles
17
Lapatinib: 55% Positive Rechallenge: Immunoallergic Injury
Tykerb U.S. Prescribing information. Revised March 2015
High positive rechallenge rates in recent clinical trials Despite rigorous monitoring and “state of the art” preclinical, clinical, & genetic understanding of a drug
Physician
Sponsor Regulator Patient
“Real world” rechallenge
• higher morbidity/mortality likely in uncontrolled rechallenge • even fatal positive rechallenge could be unknown by
physician, sponsor, regulators
Patient
?
? ?
“Real World” Positive Rechallenge (n=88)
• 73% serious adverse events, including 2 fatalities
• Most exhibited symptomatic jaundice or hepatitis, hepatocellular injury, < 1 month from initial DILI (many <1wk)
• 14% Hy’s Law events with jaundice on DILI or rechallenge
– Most recurred upon rechallenge
• Most (82%) received multiple meds besides suspect drug
Papay JI. Regul Toxicol Pharmacol 2009;54:84-90
“Real World” Positive Rechallenge (n=88)
• “Real world” drug rechallenge can be prevented with: – recognition of initial drug-induced liver injury &
communication to patient – record DILI in electronic health records (as per
allergies) and prevent possible rechallenge Papay JI. Regul Toxicol Pharmacol 2009;54:84-90
Summary Up to 75% positive rechallenge in recent clinical trials & many with immunoallergic injury Rechallenge requires a systematic benefit:risk assessment: – Has efficacy been observed in this patient? – Are there other therapeutic alternatives? – Has dechallenge occurred? – Key drug safety liabilities relevant to this
patient: HLA markers, hypersensitivity, other meds?
– Patient well-informed of benefit:risks & consents?
Conclusions
Rechallenge should generally be avoided due to potential for – serious injury and fatalities
Rechallenge of critical medications requires use of – a standardized rechallenge benefit:risk checklist
Acknowledgements
John Senior, Lana Pauls, FDA Hepatotoxicity Meeting
Christine Hunt, Nancy Yuen, Dawn Clines, Rezvan Rafi, Susan Britt, John Walsh, Roger Brown
Thank you
Recent New Drug Approvals: Rechallenge in the Label
Kynamro: cholesterol lowering agent for *rare, severe disorder
– ↑ hepatic fat 10%
– Available via REMS program
Esbriet- idiopathic pulmonary fibrosis
*prevalence 1:160,000 to 1:1,000,000). Most individuals with HoFH experience severe CHD by their mid-20s. The rate of either death or coronary bypass surgery by the teenage years is high. Severe aortic stenosis is also common.
26
27
Subject First ALT Elevation/ Time to Onset
Recovery 2nd ALT Elevation/ Time to Onset
Recovery
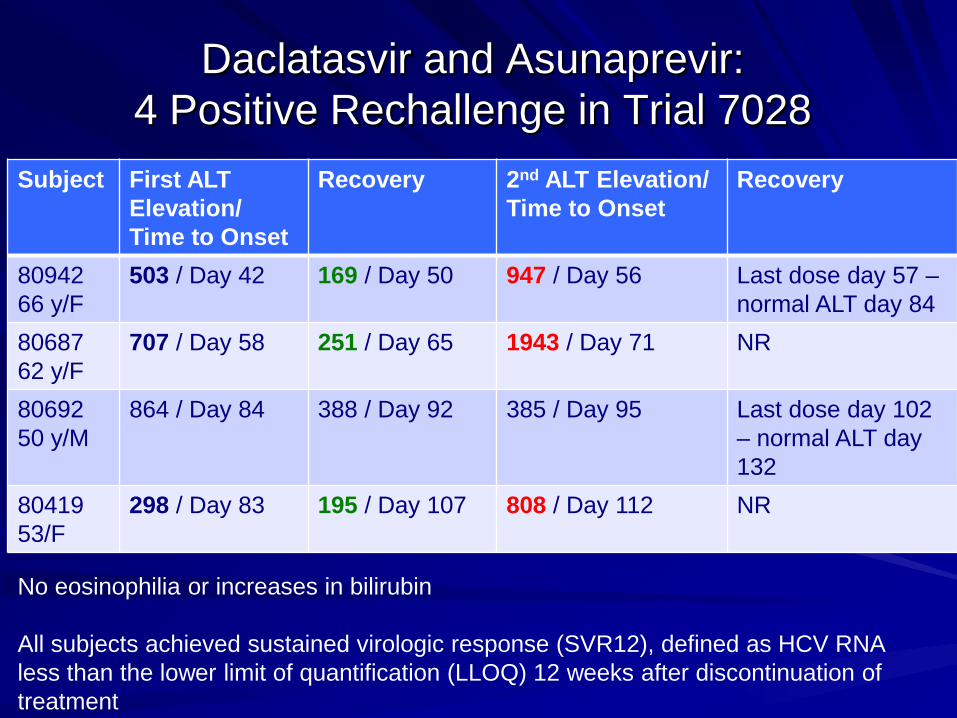
80942 66 y/F
503 / Day 42 169 / Day 50 947 / Day 56 Last dose day 57 – normal ALT day 84
80687 62 y/F
707 / Day 58 251 / Day 65 1943 / Day 71 NR
80692 50 y/M
864 / Day 84 388 / Day 92 385 / Day 95 Last dose day 102 – normal ALT day 132
80419 53/F
298 / Day 83 195 / Day 107 808 / Day 112 NR
Daclatasvir and Asunaprevir: 4 Positive Rechallenge in Trial 7028
No eosinophilia or increases in bilirubin All subjects achieved sustained virologic response (SVR12), defined as HCV RNA less than the lower limit of quantification (LLOQ) 12 weeks after discontinuation of treatment
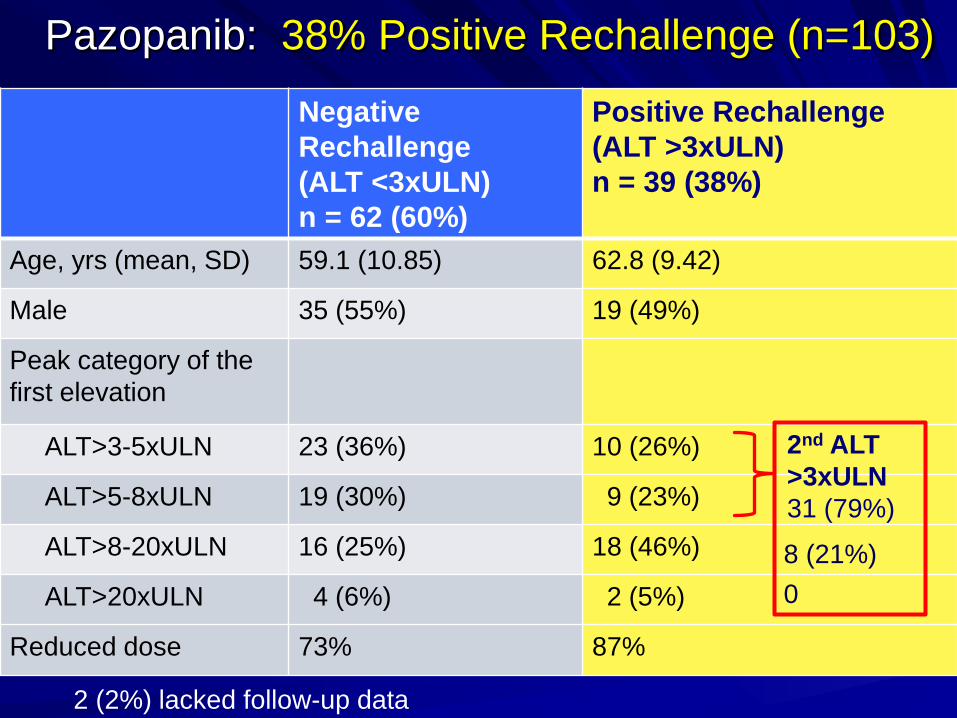
Negative Rechallenge (ALT <3xULN) n = 62 (60%)
Positive Rechallenge (ALT >3xULN) n = 39 (38%)
Age, yrs (mean, SD) 59.1 (10.85) 62.8 (9.42)
Male 35 (55%) 19 (49%)
Peak category of the first elevation
ALT>3-5xULN 23 (36%) 10 (26%)
ALT>5-8xULN 19 (30%) 9 (23%)
ALT>8-20xULN 16 (25%) 18 (46%)
ALT>20xULN 4 (6%) 2 (5%)
Reduced dose 73% 87%
Pazopanib: 38% Positive Rechallenge (n=103)
2 (2%) lacked follow-up data
2nd ALT >3xULN 31 (79%)
8 (21%) 0
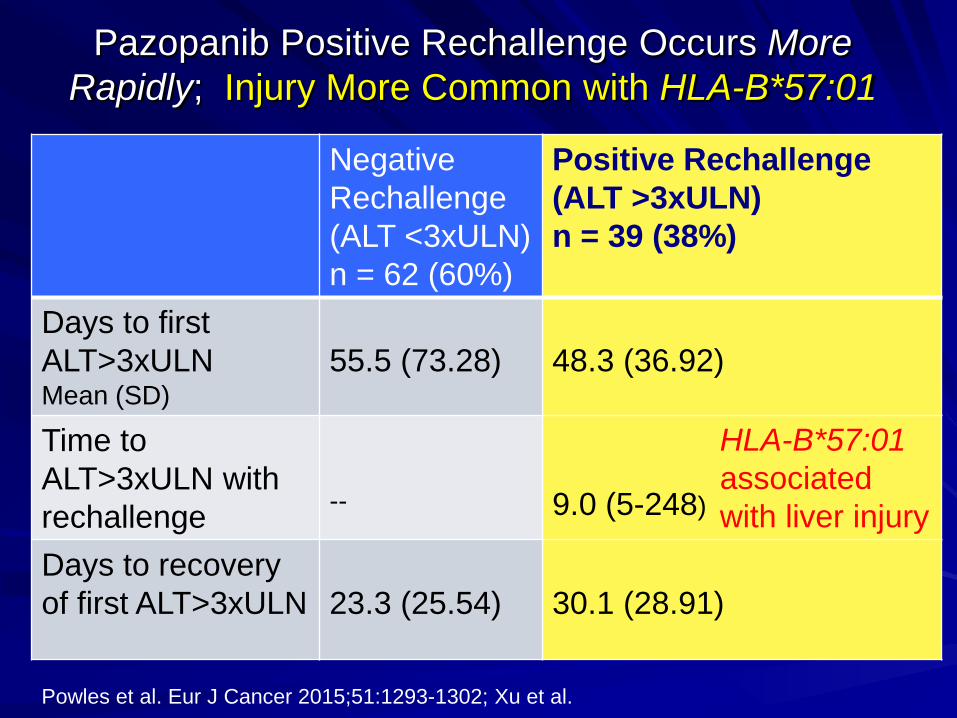
Negative Rechallenge (ALT <3xULN) n = 62 (60%)
Positive Rechallenge (ALT >3xULN) n = 39 (38%)
Days to first ALT>3xULN Mean (SD)
55.5 (73.28)
48.3 (36.92)
Time to ALT>3xULN with rechallenge
--
9.0 (5-248)
Days to recovery of first ALT>3xULN
23.3 (25.54)
30.1 (28.91)
Pazopanib Positive Rechallenge Occurs More Rapidly; Injury More Common with HLA-B*57:01
Powles et al. Eur J Cancer 2015;51:1293-1302; Xu et al.
HLA-B*57:01 associated with liver injury



























![Overview: Treatment of TBnid]/04... · with smear+ TB Started on INH/RIF/PZA/EMB Diffuse rash developed by day 7 and all drugs held. Rash resolves after 3 days Start serial rechallenge](https://img.pdfslide.us/doc/110x75/5e51def1b6449e13f20a548b/overview-treatment-of-tb-nid04-with-smear-tb-started-on-inhrifpzaemb.jpg)