Embed Size (px)
Citation preview
1
Gram Positive Bacteria
Dental Optometry MicrobiologyKen B. Waites, M.D., F(AAM)
September, 2008
Objectives• To review and discuss:
• microbiological characteristics• epidemiology• virulence factors• associated diseases• laboratory detection
of clinically important gram-positive cocci and gram-positive bacilli.
• Organisms to be discussed include:– Staphylococcus– Streptococcus– Enterococcus– Listeria– Corynebacterium– Bacillus
2
Staphylococcus• Most important
genus in FamilyMicrococcaceae
• Other genera– Stomatococcus– Micrococcus
Habitat• S. aureus
– anterior nares 50-75% healthy people– skin & mucous membranes– hospital environment
• S. epidermidis & others– resident skin flora, gut, upper
respiratory tract• S. saprophyticus
– Urinary tract in young women
3
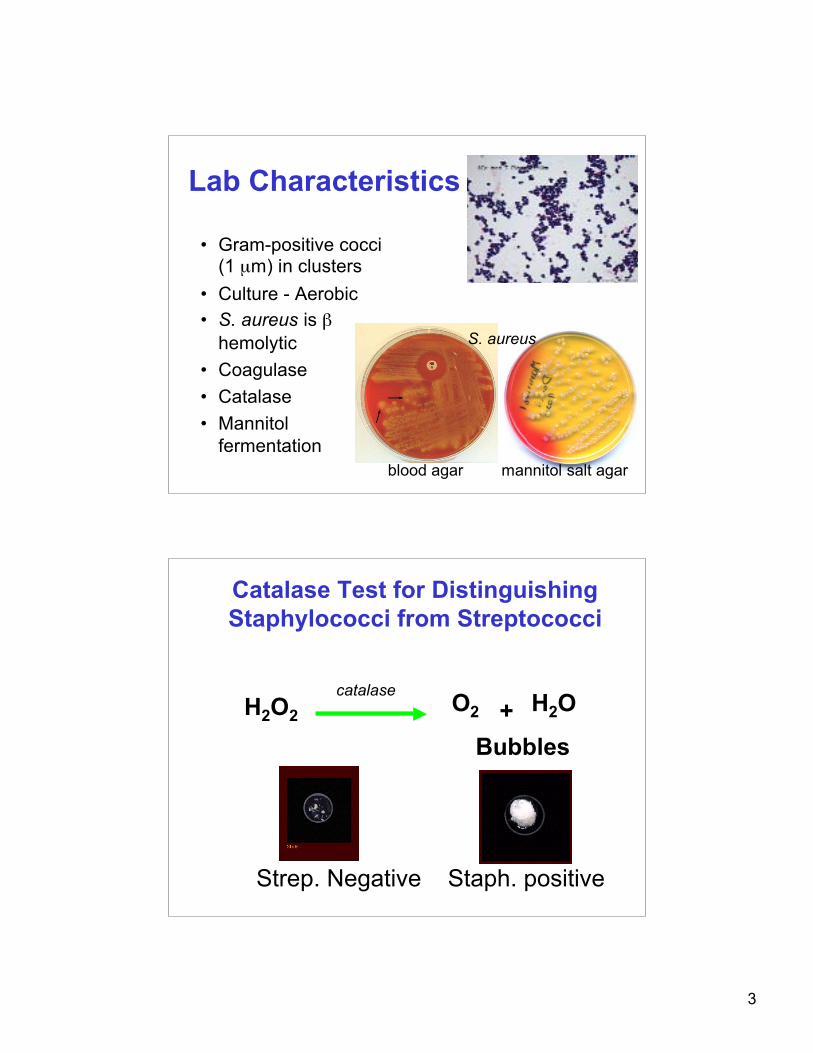
Lab Characteristics
• Gram-positive cocci(1 µm) in clusters
• Culture - Aerobic• S. aureus is β
hemolytic• Coagulase• Catalase• Mannitol
fermentation
S. aureus
blood agar mannitol salt agar
Catalase Test for DistinguishingStaphylococci from Streptococci
H2O2 catalase O2 + H2O
Bubbles
Strep. Negative Staph. positive
4
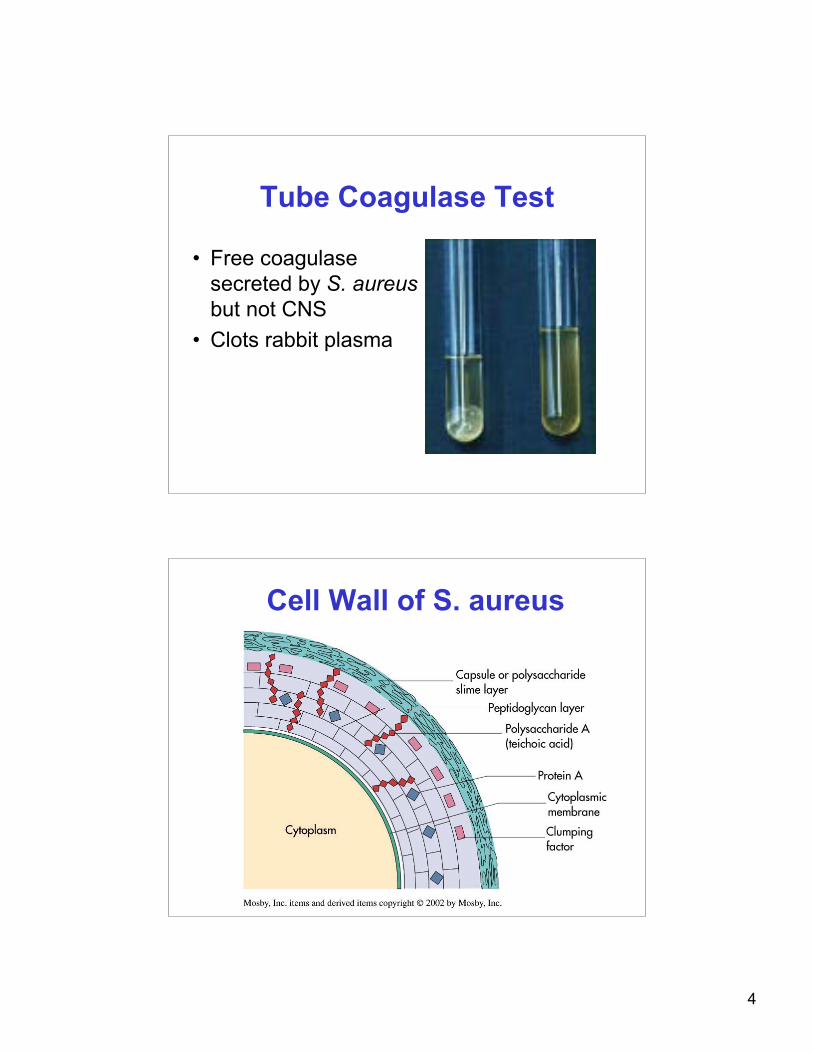
Tube Coagulase Test
• Free coagulasesecreted by S. aureusbut not CNS
• Clots rabbit plasma
Cell Wall of S. aureus
5
Antigenic Structures & VirulenceFactors of S. aureus
• Cell wall peptidoglycan– elicits production of IL-1 and opsonic antibody– PMN chemotaxis “pyogenic”– induces sepsis– activates complement– teichoic acid binds fibronectin on host cells
• Protein A - binds Fc of IgG• Capsule (some strains) antiphagocytic
S. aureus Soluble Virulence Factors
• Catalase - reduce phagocyte killing - remove H2O2
• Coagulase - clots plasma (free & bound)• Hyaluronidase - destroys connective tissue• Beta lactamase - destroys beta lactam drugs• Altered Penicillin binding proteins (PBP2’)• Fibrinolysin• Lipases• Nucleases
6
S. aureus Soluble Virulence Factors• Cytotoxins & leukocidins
– lyse white blood cells (Panton-Valentine)– release lysosomal enzymes → damage tissue
• Exfoliatin– interrupts intercellular skin junctions– “Scalded Skin Syndrome”
• Toxic Shock Toxin – stimulates T cells → cytokines,– endothelial damage → rash– “Toxic Shock Syndrome”
• Enterotoxins– stimulate vomiting by interaction with GI neural
receptors (food poisoning)
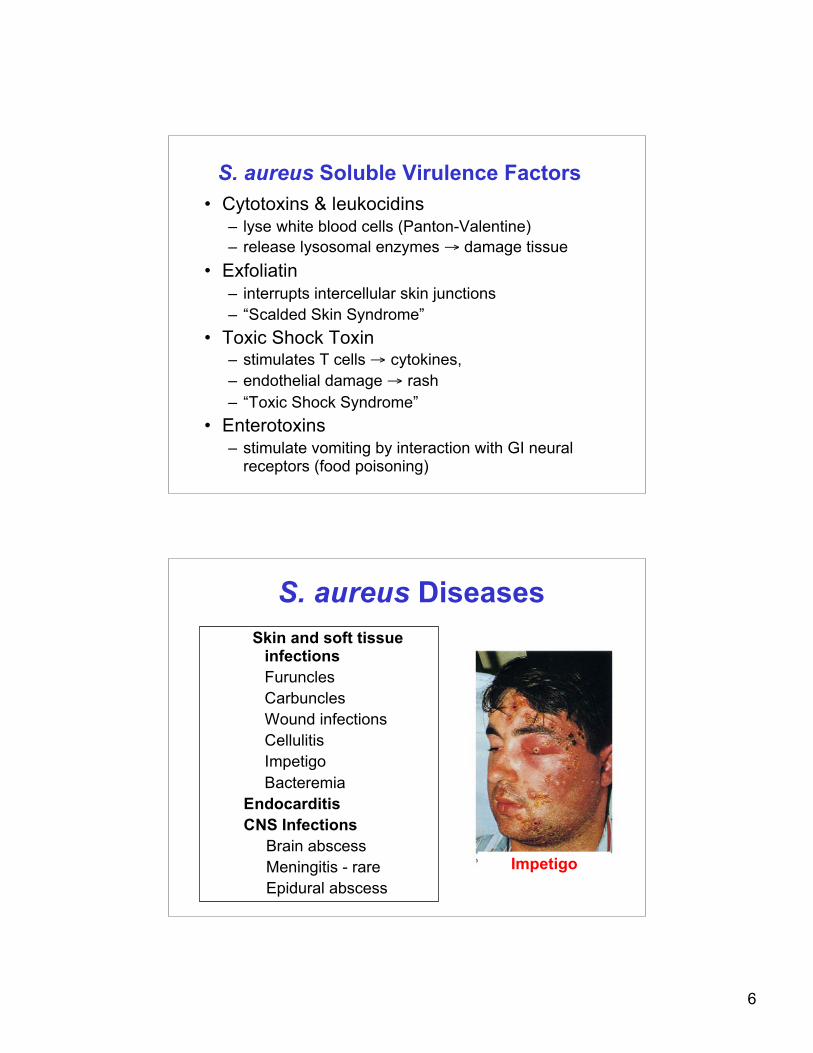
S. aureus DiseasesSkin and soft tissue
infectionsFurunclesCarbunclesWound infectionsCellulitisImpetigoBacteremia
EndocarditisCNS Infections
Brain abscess Meningitis - rare Epidural abscess
Impetigo
7
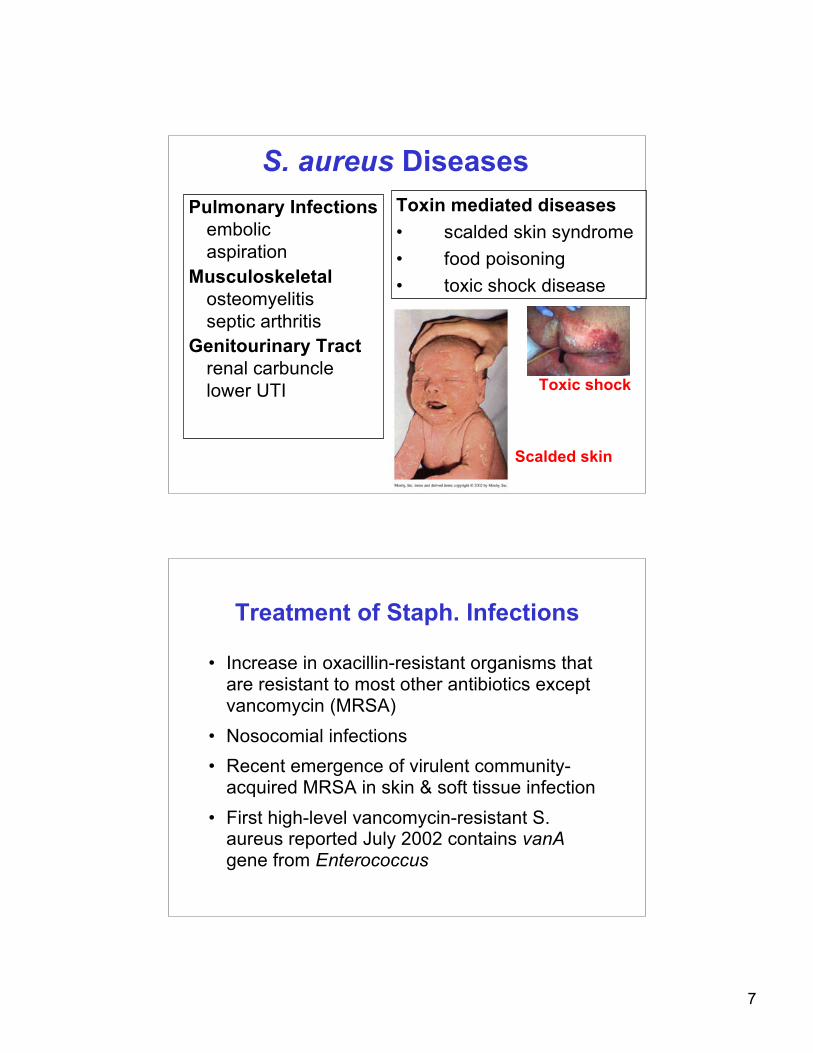
S. aureus DiseasesPulmonary Infections
embolicaspiration
Musculoskeletalosteomyelitisseptic arthritis
Genitourinary Tractrenal carbunclelower UTI
Toxin mediated diseases• scalded skin syndrome• food poisoning• toxic shock disease
Toxic shock
Scalded skin
Treatment of Staph. Infections
• Increase in oxacillin-resistant organisms thatare resistant to most other antibiotics exceptvancomycin (MRSA)
• Nosocomial infections• Recent emergence of virulent community-
acquired MRSA in skin & soft tissue infection• First high-level vancomycin-resistant S.
aureus reported July 2002 contains vanAgene from Enterococcus
8
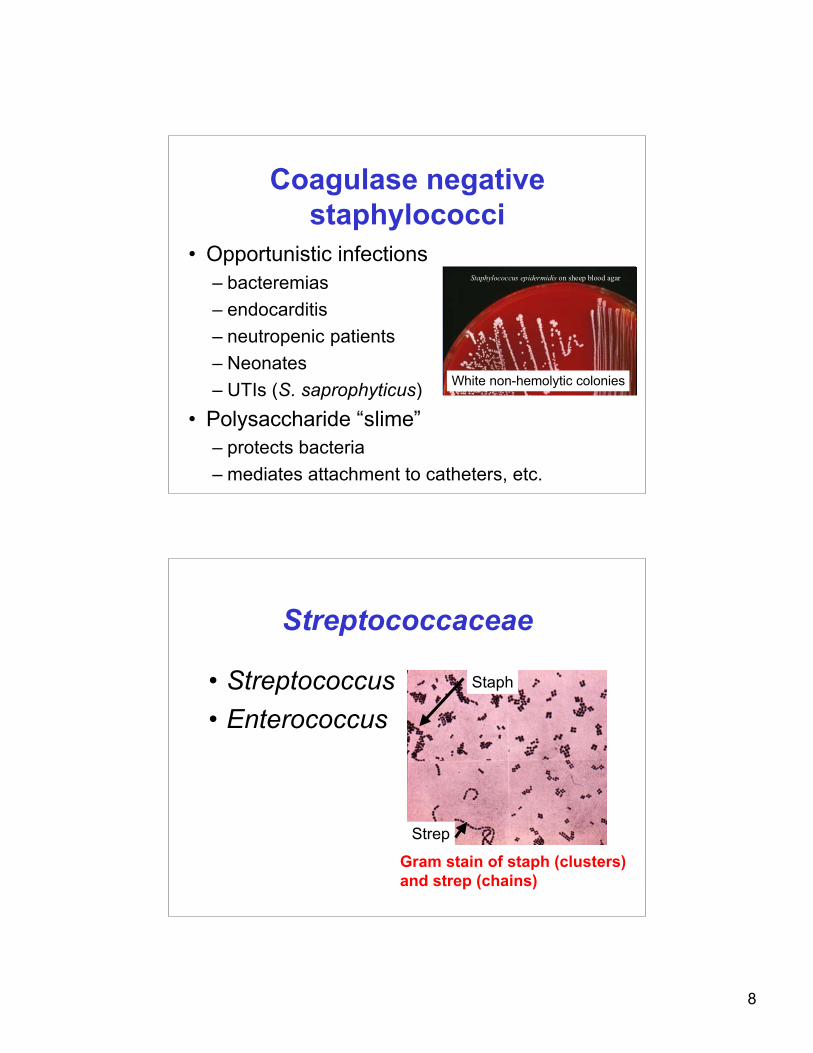
Coagulase negativestaphylococci
• Opportunistic infections– bacteremias– endocarditis– neutropenic patients– Neonates– UTIs (S. saprophyticus)
• Polysaccharide “slime”– protects bacteria– mediates attachment to catheters, etc.
Staphylococcus epidermidisStaphylococcus epidermidis on sheep blood agar on sheep blood agar
White non-hemolytic colonies
Streptococcaceae
• Streptococcus• Enterococcus
Gram stain of staph (clusters)and strep (chains)
Staph
Strep
9
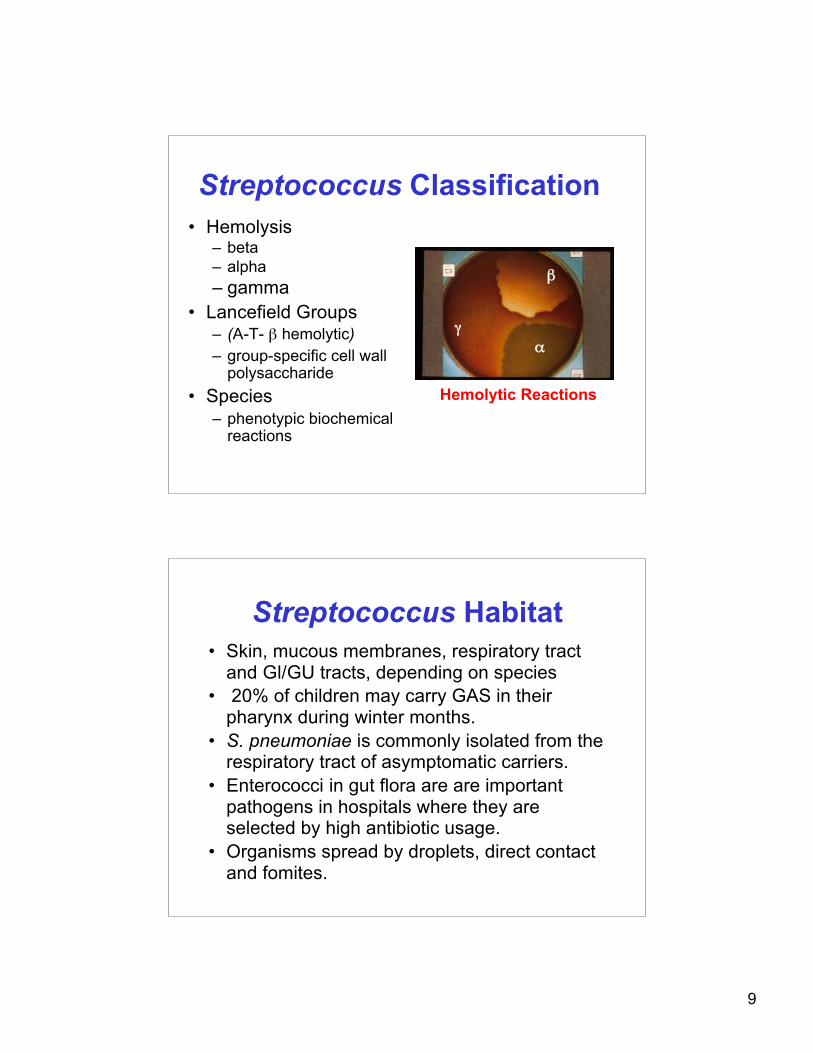
Streptococcus Classification• Hemolysis
– beta– alpha– gamma
• Lancefield Groups– (A-T- β hemolytic)– group-specific cell wall
polysaccharide• Species
– phenotypic biochemicalreactions
Hemolytic Reactions
β
αγ
Streptococcus Habitat• Skin, mucous membranes, respiratory tract
and Gl/GU tracts, depending on species• 20% of children may carry GAS in their
pharynx during winter months.• S. pneumoniae is commonly isolated from the
respiratory tract of asymptomatic carriers.• Enterococci in gut flora are are important
pathogens in hospitals where they areselected by high antibiotic usage.
• Organisms spread by droplets, direct contactand fomites.
10
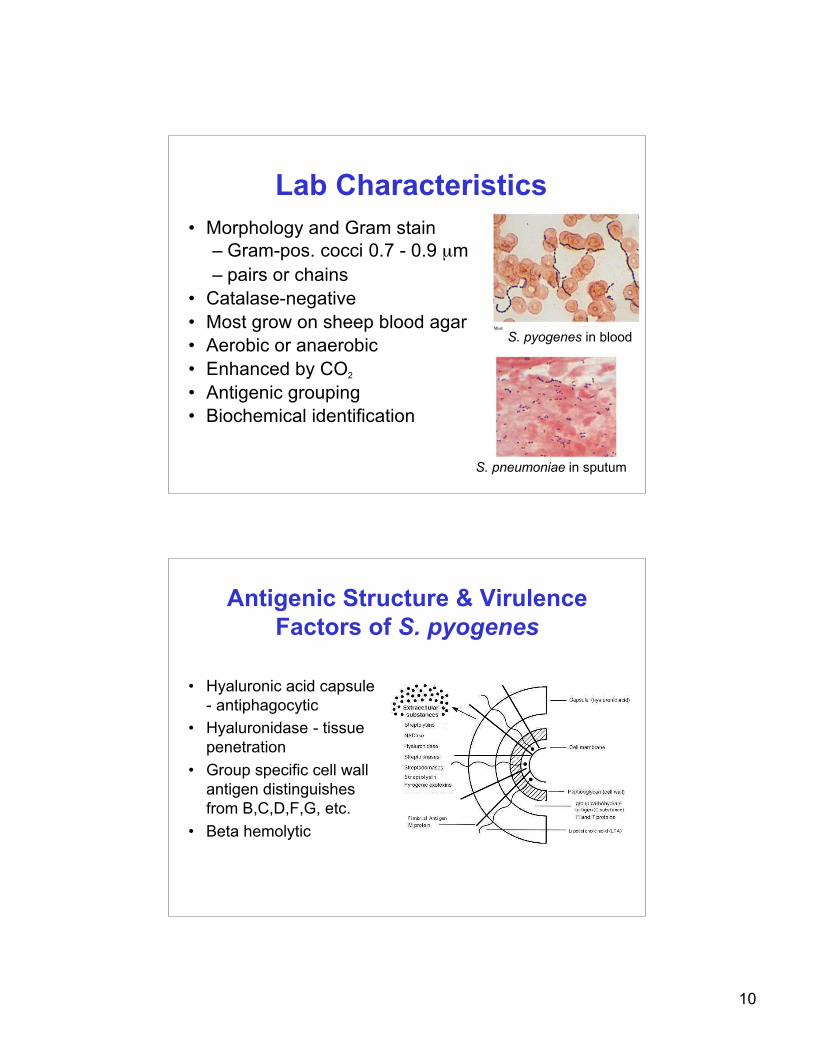
Lab Characteristics• Morphology and Gram stain
– Gram-pos. cocci 0.7 - 0.9 µm– pairs or chains
• Catalase-negative• Most grow on sheep blood agar• Aerobic or anaerobic• Enhanced by CO2
• Antigenic grouping• Biochemical identification
S. pyogenes in blood
S. pneumoniae in sputum
Antigenic Structure & VirulenceFactors of S. pyogenes
• Hyaluronic acid capsule- antiphagocytic
• Hyaluronidase - tissuepenetration
• Group specific cell wallantigen distinguishesfrom B,C,D,F,G, etc.
• Beta hemolytic
11
Antigenic Structure & VirulenceFactors of S. pyogenes
• M Protein– Virulence factor present on pilus with teichoic acid– Organisms lacking it are readily opsonized and
phagocytized– Binds fibrinogen, fibrin & degradation products
forming dense coating on the organism's surface,blocking complement
– Antibody against M protein is an importantprotective mechanism, but repeated infections withstrains possessing one of over 80 differentserotypes can occur
– Autoantibody target-Acute Rheumatic Fever
Antigenic Structure & VirulenceFactors of S. pyogenes
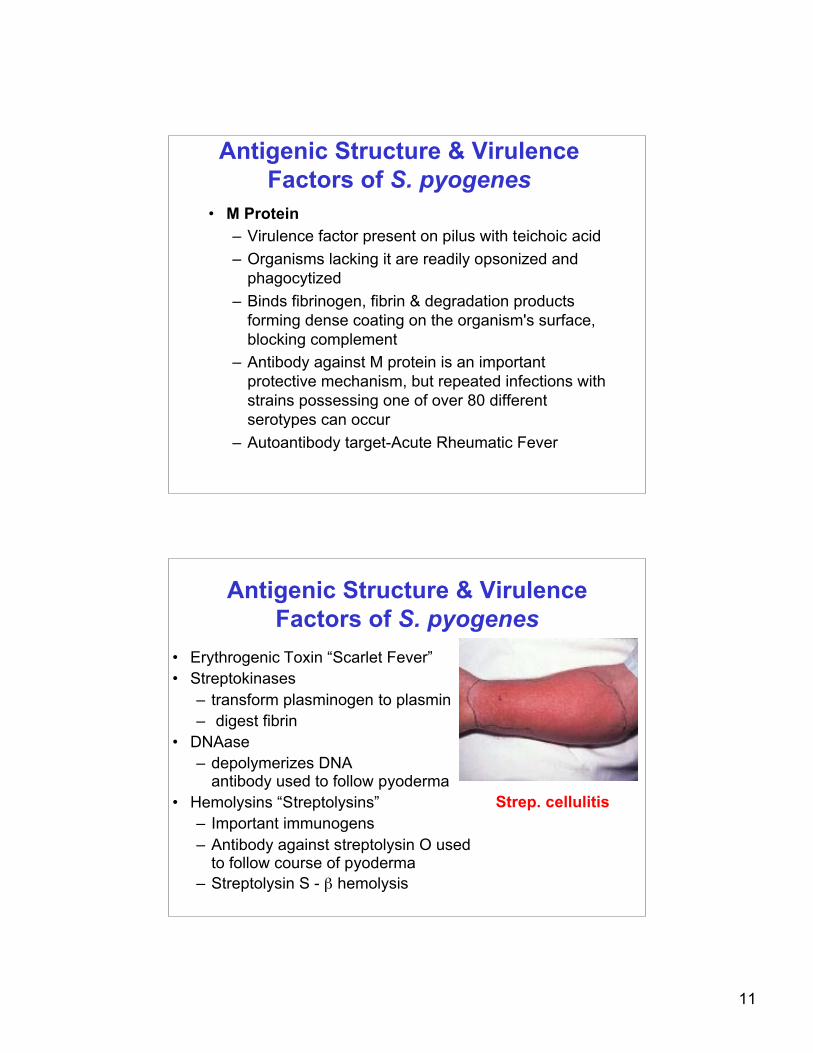
• Erythrogenic Toxin “Scarlet Fever”• Streptokinases
– transform plasminogen to plasmin– digest fibrin
• DNAase– depolymerizes DNA
antibody used to follow pyoderma• Hemolysins “Streptolysins”
– Important immunogens– Antibody against streptolysin O used
to follow course of pyoderma– Streptolysin S - β hemolysis
Strep. cellulitis
12
Antigenic Structure & VirulenceFactors of S. pyogenes
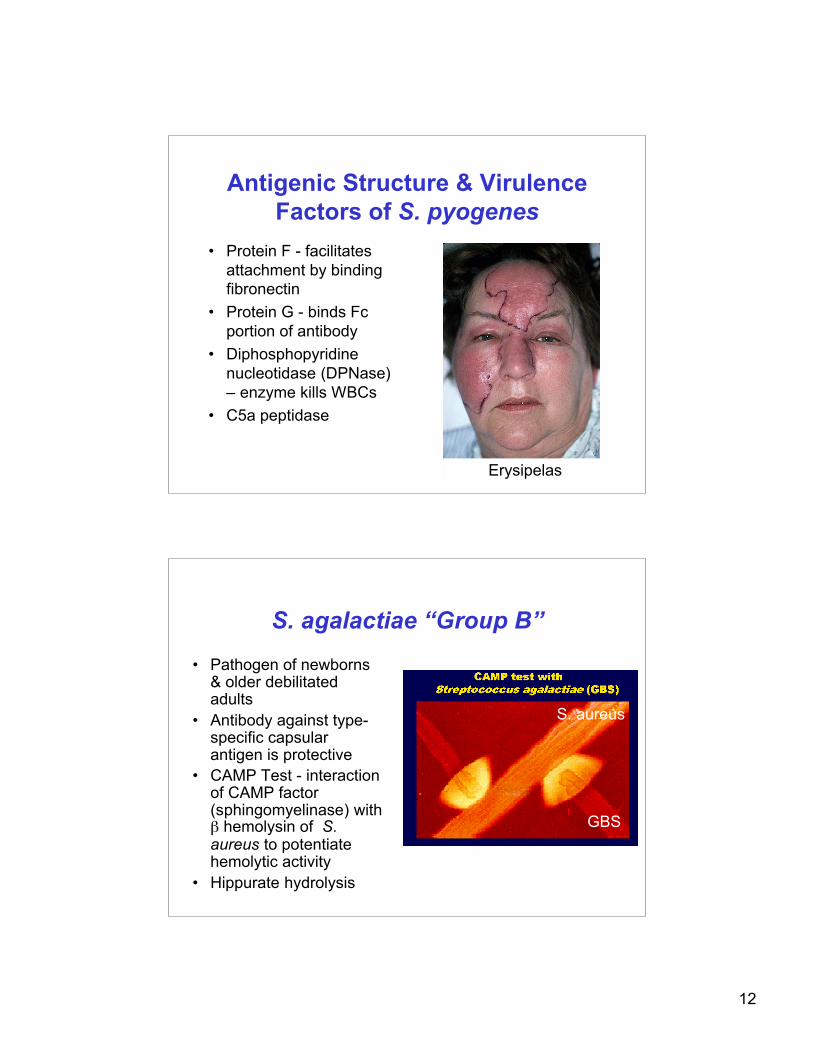
• Protein F - facilitatesattachment by bindingfibronectin
• Protein G - binds Fcportion of antibody
• Diphosphopyridinenucleotidase (DPNase)– enzyme kills WBCs
• C5a peptidase
Erysipelas
S. agalactiae “Group B”
• Pathogen of newborns& older debilitatedadults
• Antibody against type-specific capsularantigen is protective
• CAMP Test - interactionof CAMP factor(sphingomyelinase) withβ hemolysin of S.aureus to potentiatehemolytic activity
• Hippurate hydrolysis
GBS
S. aureus
13
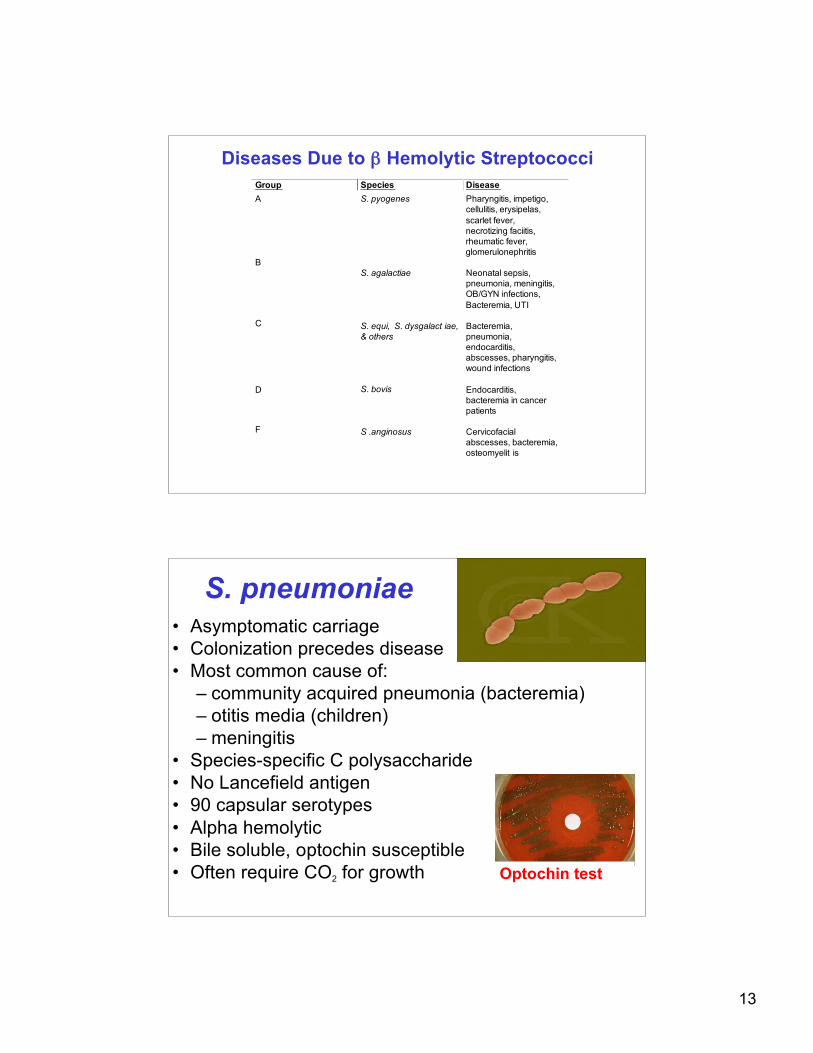
Diseases Due to β Hemolytic StreptococciGroup Species Disease
A S. pyogenes Pharyngitis, impetigo,
cellulitis, erysipelas,
scarlet fever,
necrotizing faciitis,
rheumatic fever,
glomerulonephritis
B
S. agalactiae
Neonatal sepsis,
pneumonia, meningitis,
OB/GYN infections,
Bacteremia, UTI
C
S. equi, S. dysgalact iae,
& others
Bacteremia,
pneumonia,
endocarditis,
abscesses, pharyngitis,
wound infections
D
S. bovis
Endocarditis,
bacteremia in cancer
patients
F
S .anginosus
Cervicofacial
abscesses, bacteremia,
osteomyelit is
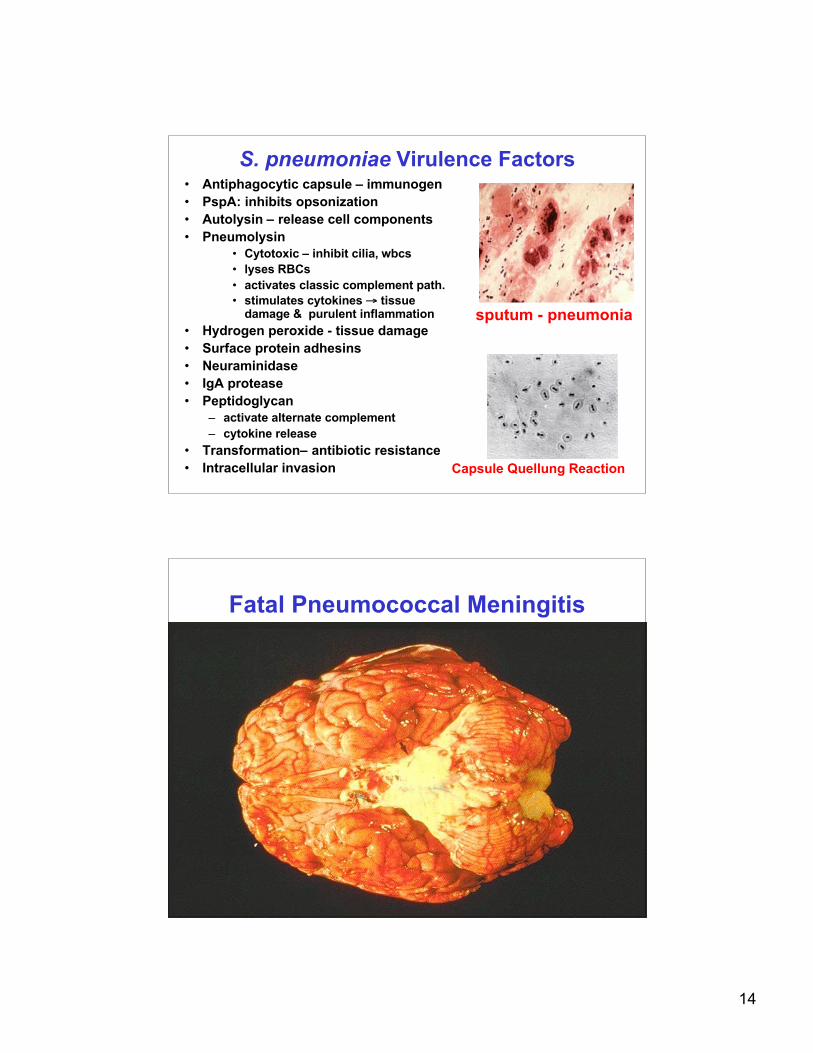
S. pneumoniae• Asymptomatic carriage• Colonization precedes disease• Most common cause of:
– community acquired pneumonia (bacteremia)– otitis media (children)– meningitis
• Species-specific C polysaccharide• No Lancefield antigen• 90 capsular serotypes• Alpha hemolytic• Bile soluble, optochin susceptible• Often require CO2 for growth Optochin test
14
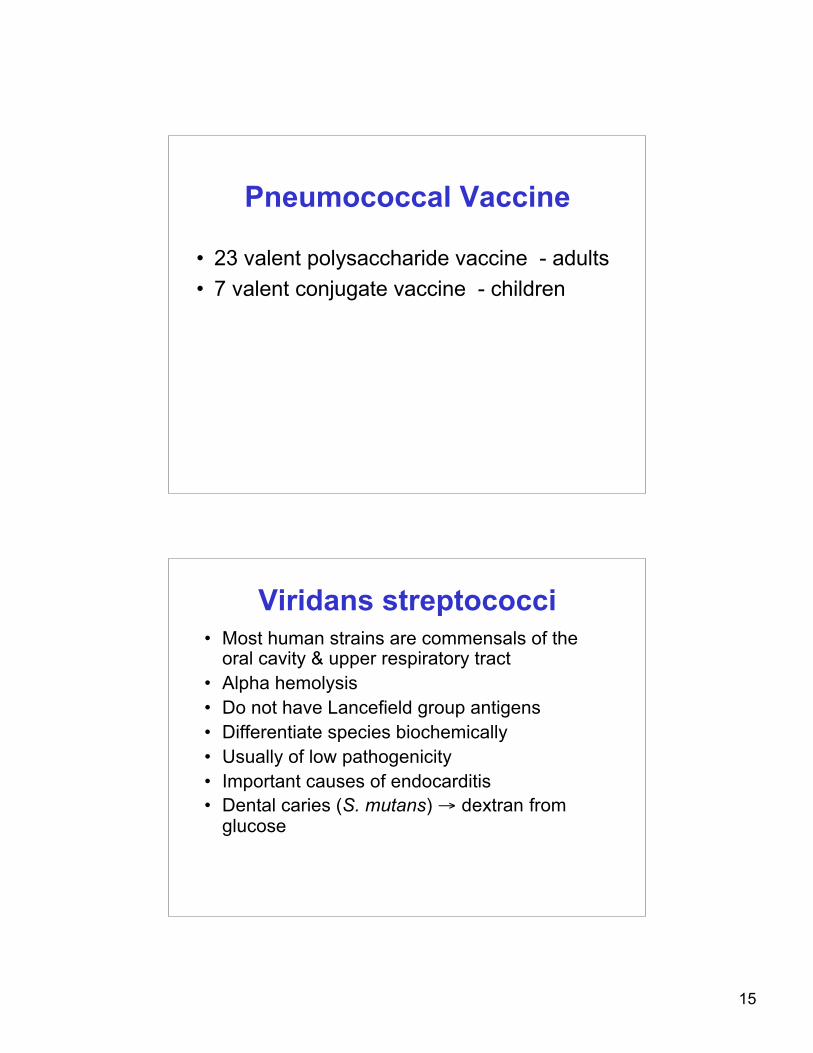
S. pneumoniae Virulence Factors• Antiphagocytic capsule – immunogen• PspA: inhibits opsonization• Autolysin – release cell components• Pneumolysin
• Cytotoxic – inhibit cilia, wbcs• lyses RBCs• activates classic complement path.• stimulates cytokines → tissue
damage & purulent inflammation• Hydrogen peroxide - tissue damage• Surface protein adhesins• Neuraminidase• IgA protease• Peptidoglycan
– activate alternate complement– cytokine release
• Transformation– antibiotic resistance• Intracellular invasion Capsule Quellung Reaction
sputum - pneumonia
Fatal Pneumococcal Meningitis
15
Pneumococcal Vaccine
• 23 valent polysaccharide vaccine - adults• 7 valent conjugate vaccine - children
Viridans streptococci• Most human strains are commensals of the
oral cavity & upper respiratory tract• Alpha hemolysis• Do not have Lancefield group antigens• Differentiate species biochemically• Usually of low pathogenicity• Important causes of endocarditis• Dental caries (S. mutans) → dextran from
glucose
16
Enterococcus• At least 12 species• Usually non-hemolytic• E. faecalis most common• Distinguish from streptococci by:
– esculin hydrolysis– growth in 6.5% NaCl– PYR hydrolysis (Group A β strep. are +)
• Enteric flora• Opportunist - nosocomial pathogen• Intrinsic antimicrobial resistance• E. faecium - vancomycin-resistance• Abscesses, urinary tract, endocarditis,
abdominal/pelvic, bacteremia, wound infections
Listeria monocytogenes• Gram-positive coccobacilli• Catalase positive• Weakly β hemolytic• Facultatively intracellular• Motile• Attachment factors,
hemolysins, phospholipases• Diseases
– foodborne (dairyproducts)
– meningitis– neonatal infections
17
Key PointsListeria monocytogenes
• Gram-positivebacilli/coccobacilli
• Catalase-positive• Motile• Esculin positive• β hemolytic
Positive motility test
Corynebacterium• Gram-positive, curved pleomorphic rods• “Chinese Letters”• Aerobic/facultatively anaerobic• Grow readily on SBA• Need selective media (cystine-tellurite)
to detect and ID• Catalase & oxidase positive• Usually non-motile• Commensals on skin• Pathogens
– C. jeikeium– C. diphtheriae
18
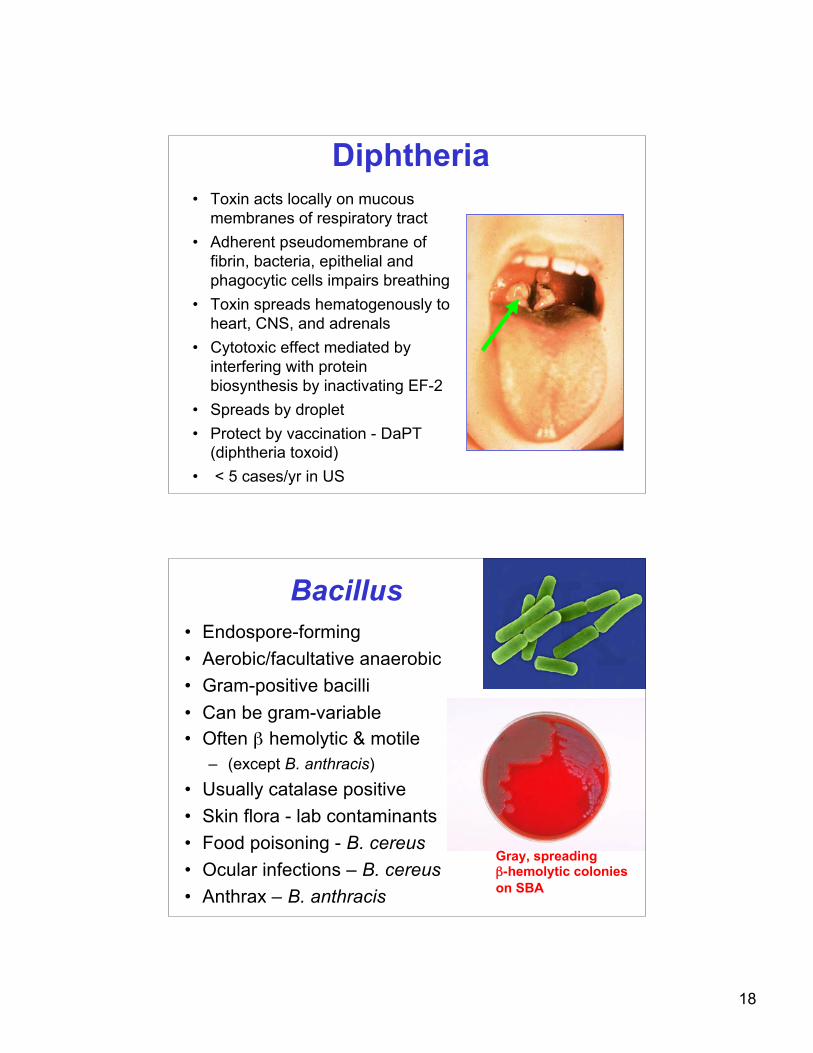
Diphtheria• Toxin acts locally on mucous
membranes of respiratory tract• Adherent pseudomembrane of
fibrin, bacteria, epithelial andphagocytic cells impairs breathing
• Toxin spreads hematogenously toheart, CNS, and adrenals
• Cytotoxic effect mediated byinterfering with proteinbiosynthesis by inactivating EF-2
• Spreads by droplet• Protect by vaccination - DaPT
(diphtheria toxoid)• < 5 cases/yr in US
Bacillus• Endospore-forming• Aerobic/facultative anaerobic• Gram-positive bacilli• Can be gram-variable• Often β hemolytic & motile
– (except B. anthracis)• Usually catalase positive• Skin flora - lab contaminants• Food poisoning - B. cereus• Ocular infections – B. cereus• Anthrax – B. anthracis
Gray, spreading β-hemolytic colonies on SBA
19
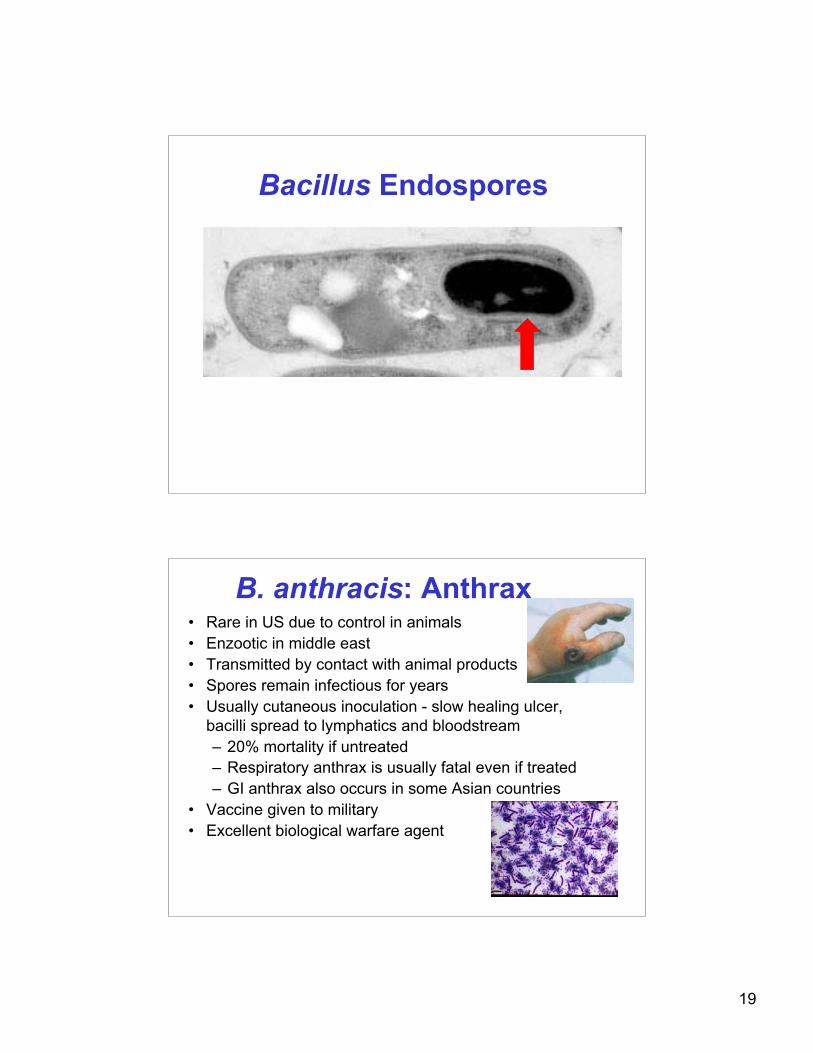
Bacillus Endospores
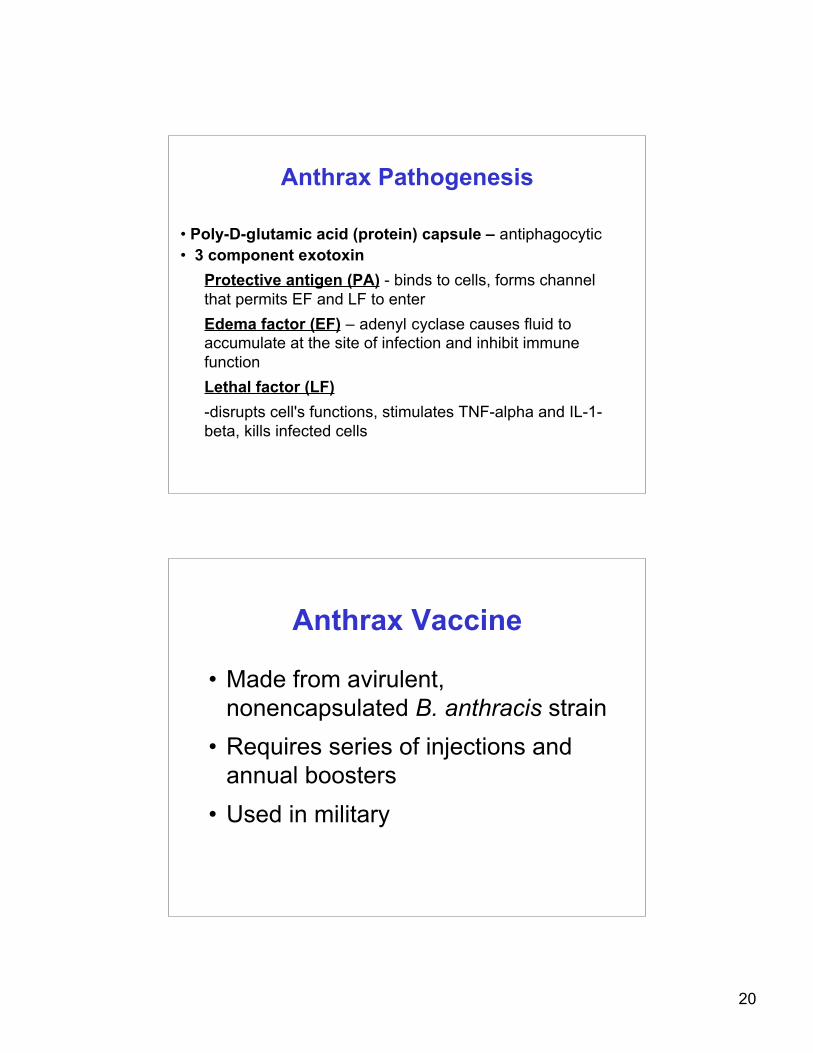
B. anthracis: Anthrax• Rare in US due to control in animals• Enzootic in middle east• Transmitted by contact with animal products• Spores remain infectious for years• Usually cutaneous inoculation - slow healing ulcer,
bacilli spread to lymphatics and bloodstream– 20% mortality if untreated– Respiratory anthrax is usually fatal even if treated– GI anthrax also occurs in some Asian countries
• Vaccine given to military• Excellent biological warfare agent
20
Anthrax Pathogenesis
• Poly-D-glutamic acid (protein) capsule – antiphagocytic• 3 component exotoxin
Protective antigen (PA) - binds to cells, forms channelthat permits EF and LF to enterEdema factor (EF) – adenyl cyclase causes fluid toaccumulate at the site of infection and inhibit immunefunctionLethal factor (LF)-disrupts cell's functions, stimulates TNF-alpha and IL-1-beta, kills infected cells
Anthrax Vaccine
• Made from avirulent,nonencapsulated B. anthracis strain
• Requires series of injections andannual boosters
• Used in military





























