Embed Size (px)
Citation preview

Speaker NameTitle
Organization
Positioning for the Future of Managed Care
Richard S. Edley, PhDPresident and CEO
Rehabilitation and Community Providers Association

Welcome
• Purpose/ Objective– Understanding the Changing Managed Care and HealthCare
Landscape
– Transformation of the MCO Role
– Impact on and Direction for Providers
– MCO- Provider Partnerships
– And More…
• Format– Opening Presentations
– Guided Questions
– Audience Interaction and Participation
• Introductions

RCPA
• Health and Human Services Trade Association
based in PA
• 325 Members/ Agencies/ Hospital Systems
• Mental Health, Drug & Alcohol, Intellectual and
Developmental Disabilities, Criminal Justice,
Children’s Services, Medical Rehabilitation (incl.
Pediatric), Brain Injury, Long Term Services and
Supports
• Provider (Full), Associate, Business, and
Government Members

History of PA Association Managed Care
• Mid 1990’s Association Founded Community
Behavioral HealthCare Network of PA
(CBHNP)
• BH-MCO
• Commercial and Medicaid Business
• Full Risk, Shared Risk, ASO
• $300+ M Revenue; Multi-State
• Sold in 2008

Today
• IDD Managed Care- Future
• Managed Long Terms Services and Supports
(MLTSS)- Today
• RCPA has Founded the Rehabilitation and
Community Services Organization (RCP-SO)
• Brain Injury, Service Coordination Entities
(SCE), Personal Attendant Services (PAS)
• Capitalized and Incorporated
• Partnering with MCOs: Seat at the Table

Future of Managed Care
• Provider-Based Systems (ACO)
• New Risk and Risk/Reward Models
• Value-Based Payment Systems
• Payer-Provider Partnerships
• Transitioning of Traditional BH-MCO Role
• PH/BH/IDD/LTSS Coordination/Integration
• Diversification of Business Lines at the MCO
and Provider Level

• This Leads to the Panel Discussion Today

Speaker NameTitle
Organization
Positioning for the Future of Managed Care
Managed Care, Disrupted.
Dan CavePresident & CEO
Envolve PeopleCare™

We are made wise not by the recollection of our past, but by the responsibility for our future.
George Bernard Shaw

Let’s get it started
It’s about behavioral health…
6-7%of adults suffer from depression annually
5.7 million have bipolar disorder
Anxiety disorders affect
40 million1 in 5
experience mental illness in any given year
17 million dependent on or abuse alcohol
including 1 major depressive episode

…or is it physical health?
Countless undiagnosed | 1x-2x | with diabetes, heart disease and COPD
1 in every 4 DEATHS caused by heart failure
5 million with heart failure
11 million with COPD
1 in every 12 have asthma
29 million with diabetes

…wait…it’s about multiple chronic
conditions, right?
117had one or more
chronic conditions
1 in 4had two or more
million
0% 20% 40% 60% 80% 100%
45% of people with 2 or more chronic conditions have diabetes
78% have high blood pressure
Over and another
of individuals with diabetes also have coronary heart disease
20% 15% have some other form of heart disease
of people with heart disease also have arthritis
49%

Ok, so it’s physical/behavioral
integration?
of people with diabetes also have depression
27% 17% Depression occurs in 17%of people with cardiovascular disease
Rate of depression among individuals post-mi is between 40-65%
0% 20% 40% 60% 80% 100%
adults with mental illness and asthma
6.9million
with substance abuse disorders have co-occurring mental illness
40%of adults
People with substance abuse disorders are
50-300% more likely to have chronic conditions and/or HIV/AIDS

…oh…almost forgot, these are real
people…
29% personally involved in
legal matters in last 3 years
of elder caregivers were simultaneously employed while providing care2/3
Roughly half
of all marriages end in divorce
at work by personal financial matters
distracted1 in 3
hours/week
16 Median of
spent by elder caregivers on hands-on care

The Past
How’s that working out?

The Future
It starts with a question.
Why aren’t we in better health?
Be honest.
Why aren’t I in better health? Why aren’t you?
Think about it…now hold that thought.

Remember these?

What about these?

The future of managed care?
Let’s shape it…
PAST PRESENT FUTURE
• Eligibility• Claim
Adjudication• Claim Payment
• Utilization Management
• Case Management
• Medical Necessity
• Incremental Innovation
?

Environmental Trends
• Lifestyle
• Entitlement culture
• New healthcare
technologies and
treatments
Personal Factors
• Lack of knowledge
• Everyday demands
• Insufficient motivation
19© 2016 Envolve.
Back to that thought you are holding
Let’s be honest…

What gets in the way of health?
Emergence of health consumer
Consumer
Market
Choices
Information
Consequences

Toto, I’ve got a feeling we’re not in
Kansas anymore…
Seismic shifts
Selected Dynamics Implications
Government Deficits/Debts Cost-sharing, cost-control, prevention
Provider, payor consolidation Scale economies in maturing market, margin protection
Public and Private Exchanges Financing shift to defined contribution vs. defined benefit
Mobile technologies Rising consumer service expectations –“an app for that”
Obesity, Diabetes, Stress – going global Greater % of dollars spent on lifestyle-related conditions

Managed Care 2.0
The next disruption
Indemnity
• Eligibility
• Claim adjudication
• Claim payment
Managed Care 1.0
Unnecessary Supply
• Utilization
management
• Case management
• Provider networks,
discounts
• Provider risk sharing
PASTTransaction -
focus
PRESENTProvider-focus
FUTUREConsumer-
Focus
Managed Care 2.0
Preventable Demand
• Sustainable
consumer behavior
change
• Health and wellbeing
• Physical, behavioral,
legal, financial, etc.
• Motivational science
• Expert teams
• Adaptive technology

The emergence of a consumer
Igniting and sustaining behavior change
Sustainable Behavior Change
• Educate• Enable• Motivate
Modifiable or Preventable Demand

Managed Care 2.0…or,
Managed Care…disrupted. • Consumerism
– Choices
– Information
– Consequences
– Rising expectations,
consumer-centric
• The walls come tumbling down
• Defined contribution financing
• Providers as consultants to
consumers or primary
caregivers
• Re-imagined industry
– People analytics, consumer
marketing
– New entrants, strange
bedfellows
– Community involvement
– Wave of product
development, pilots, new
models
– Kodak moments
Fastest, easiest path to healthy wins

Speaker NameTitle
Organization
Positioning for the Future of Managed Care
Anne McCabePresident, Public Markets
Magellan Healthcare

The Changing Role of MCOs

Magellan: One Model of Healthcare
Evolution Serving Special Populations
Pre-2006
Behavioral health
2006-2009
Specialty solutions/ pharmacy
2013
Pharmacy benefits mgmt
2013
Integrated care-special populations
2014-2016
Special populations/ MLTSS
Acquisitions of AlphaCare, TMG
Integrated health homes, Magellan Complete Careof Florida
Acquisition of Partners Rx
Acquisitions of National Imaging Associates (NIA), First Health and ICORE specialty pharmacy
Market leader inbehavioral healthmanagement

Managed Care Trends
• Population management: Integrated care
models for specialty populations
• Member choice, direction & control/social
determinants
• Value-based purchasing
• Federal funding opportunities
• Provider challenges and potential solutions

Integrated Care ModelsIowa Integrated Health Home Initiative
An adaptation of the medical home model by creating IHH specifically aimed at
serving individuals with complex behavioral health & chronic medical conditions

Integrated Care ModelsIowa Integrated Health Home Initiative

Integrated Care ModelsIowa Integrated Health Home Initiative
Outcomes

Integrated Care Models Co-Located Integrated Health Program: Outpatient BH Provider
Within Offices of a Neighborhood Health Center
Goals
• Improved/elevated independence of individuals with mental illness while
supporting recovery and enhancing the individual’s quality of life
• Establishment and enhancement of relationships with medical providers to realize
improved overall health outcomes
• Decreased frequency, intensity, duration of negative health symptoms
Outcomes
• Increased access to care in 27% of members who had not previously received BH
services
• 50% of members had a score consistent with fewer depressive symptoms
• Self-reported improvement in provider relationship (9% increase), improved blood
pressure (9%), improved overall physical/BH (14%)
Provider Model
• Contracted BH outpatient provider co-located staff in the FQHC
• Increases access and coordination of services for members

NEW YORK
• Medicaid Managed Long-Term
Care Plan
• For those with chronic illness and
disabilities who want to continue to live
in their home
• Participant in the FIDA Duals
Demonstration
Integrated Care Models
FLORIDA
• Florida Medicaid specialty health plan
• For those living with serious mental
illness
• Results-driven, community-based
approach
• Holistically addresses all healthcare
needs
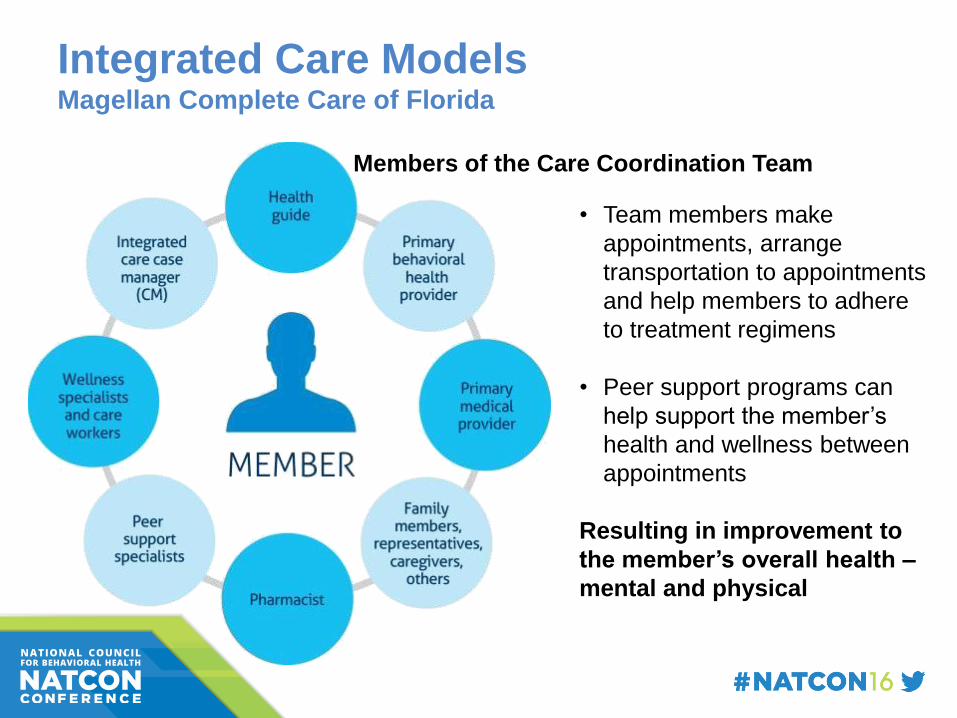
Integrated Care ModelsMagellan Complete Care of Florida
• Team members make
appointments, arrange
transportation to appointments
and help members to adhere
to treatment regimens
• Peer support programs can
help support the member’s
health and wellness between
appointments
Resulting in improvement to
the member’s overall health –
mental and physical
Members of the Care Coordination Team

Integrated Care ModelsComplete Care of Florida
Understanding
the unique mental
and physical
health needs of
individuals living
with serious
mental illness.
Members receive
personalized, high-
quality healthcare
that is tailored to
their physical
health, mental
health and social
needs.

Member Choice, Direction & Control
• Individual empowerment: Taking charge of services,
supports, and resources
• Self-directed care: Expanding real choice and control
• Decision support tools: Psychiatric advance
directives, WRAP®, life and goal-planning resources
• Empowering relationships: Built on strengths and
respect

Member Choice, Direction & Control Social Determinants of Health
Education and housing
Employment, living wages
Access to healthy foods and green spaces
Access to healthcare

Member Choice, Direction & Control Disparities and Inequities in Health
Disparities in Health
Differences in access to health services
Differences in health outcomes
Sadana and Blas, 2013
Health Inequities
are systematic, socially produced (and therefore modifiable) and unfair.
World Health Organization, 2010

Member Choice, Direction & Control Adding it all up…
Combined Healthcare Systems
Justice and Equity
Choices and
Decision Support
Social and Community Supports & Resources

Member Choice, Direction & Control Eight Dimensions of Wellness
Adapted from Swarbrick, M. (2006). A wellness approach. Psychiatric Rehabilitation Journal, 29,(4) 311- 314. (used with permission)

Member Choice, Direction & Control
• Annual Community Integration and Recovery Academy conference
attended by providers, peers, and family advocates provided
education about social inclusion and the 8 dimensions of wellness
• Peer support whole health and resiliency support groups:
– Facilitator development program
– Saw improvements in healthy eating habits among support group
participants, along with improvements in other health domains, including
better social support networks
Member Choice, Direction & Control
Invested in mini-grant initiative over 3 years:
• Community provider focused on stigma reduction and education (relates to social
determinants around rights, social justice, freedom from exclusion, etc.)
• Conducted research to support stigma reduction and education re: mental illness;
implementation of community based support groups/trainings that addressed and
counter stigma and discrimination
• Participated in collaborative trainings and meetings with partnering organizations,
peer organizations, and stakeholders in order to address and counter stigma and
discrimination; students, teachers, parents and adults attended the collaborative
meetings
• Trained college campus professors/instructors and community-based agencies
owners, administrators, managers and staff on implementing a project-based activity
to support addressing the issues centered around stigma and discrimination
• Recruited volunteers/graduate student interns to work with community-based groups
to implement the support groups
• Developed and provided a calendar of scheduled trainings, events, and/or groups;
shared with the community in various forms

Value-Based Purchasing
• Defining value through data
analytics that are transparent and
standardized to equitable measure
• Early and ongoing provider
engagement
• Transparency through sharing
provider performance
• Payment alignment by
reimbursing based on
performance and incentives
aligned with measurements of
value
Value-Based Purchasing
Defining Value Provider data
AnalyticsAlgorithms
Provider engagement
TransparencyVisualization ScorecardsDashboards
Member Choice
Payment alignment
Pay for Performance
Key Components
Value-Based PurchasingPutting the Wheels Into Motion
• Leveraging past experiences to inform
next steps
• Experience with P4P programs helps
build a solid foundation that leads to the
best outcomes for members
Value-based programs are designed to:
• Engage providers to move toward
delivering care that meets “value” criteria
• Impact the overall delivery system
• Inform next steps for other levels of care
• Provide various opportunities to engage
providers to deliver services in a cost-
effective manner
• Result in increased community tenure
Facility levels of care
Community-based
services
Traditional outpatient

Pay for PerformanceMental Health Inpatient (MH IP) Partners in Care
Goal• Entire program focused on collaboration with psychiatric inpatient facilities to improve outcomes
Outcomes/ Provider Impact• Two performance measures include follow-up after hospitalization and 30-day readmission rates
• 7-day follow-up after hospitalization (FUH) increased for providers in this program over one year
– MH IP Partners in Care providers outperformed inpatient facilities that were not part of the
program, with higher 7-day FUH in five of six quarters reviewed
• 30-day readmission rates for 10 program providers improved in a year, declining from 17% to 14%
Value-Add for Providers• More time focused on caring for members – less time on the phone doing UM
• Shared ownership in outcomes
• Facility leaders share best practices as well as discuss strategies for interventions and breaking
down barriers
• Develops transparency between providers
• Shared upside
• Good performance = good outcomes for members and success for providers
Value Based Purchasing
VBP Lowers Costs, Enhances Member Outcomes
Goal
• Improve Assertive Community Treatment (ACT) model
Actions
• Analyzed program data, worked closely with ACT provider teams to
develop a three-tiered rate structure based on overall program goals to
support recovery and wellness, as well as improve community tenure.
Outcomes
• 21% decrease in inpatient admissions, 24% decrease in the inpatient
readmission rate

Value-Based Purchasing
Inpatient
• Reduced 30-day readmissions from 11.9 to 9.8 for large hospital system in network
• Increased 30-day AFU from 79.8% to 83.88% for large hospital system in network
Assertive Community Treatment (ACT)
• Reduced from 7% to 1% acute inpatient readmissions for largest provider team in
network
• Increased from 52% to 81% medical care coordination for largest provider team in
network
Dual-diagnosis adult residential pilot project, stretch goals: 7% and 80%
• 5.26% annual program readmission rate
• 84.21% successful program completion rate

Value-Based Purchasing Key Components of Magellan’s VBP Model(s)
The use of data, algorithms,
standardized equitable measures
and actionable information to
identify and define provider value
Early and ongoing engagement
through data and an
understanding of what is being
measured, and why and how it’s
being measured
Public reporting to drive
performance improvement
Consumer transparency for
selection of highest quality
providers
Reimbursement is based upon
performance
Incentives are aligned with
definition of value
Defined value Provider engagement
Payment alignment
High-performance networks
Care coordination member-facing provider profiles Member outcomes data
Transparency Informed choice
Consumers, customers and
payers have the right
information to make informed
decisions about choice of care,
network and contracting.

Commonwealth of Pennsylvania: Pay-
for-Performance
• Program: PA DHS began Integrated Care Pay for Performance Program (P4P) 1/1/16
for all primary contractors. $10m funding pool. Incentive paid based on combined
PH/BH MCO performance
• Goals: Greater integration between BH and PH services; quality of care improvement
for Medicaid recipients with SPMI and SUD; enhanced care coordination to reduce
Medical Assistance expenditures
• Provider requirements: Meet three process measures for financial incentive
eligibility: Stratification of members with SPMI; use integrated care plans/member
profiles with BH/PH information; and hospital notification to PHMCO within one
business day of acute inpatient hospitalization/discharge notification
• Five outcome measures: 1) Initiation and engagement of alcohol/other drug
treatment; 2) adherence to antipsychotic medications for individuals with schizophrenia;
3) combined BH/PH inpatient 30-day readmission rate for individuals with SPMI; 4)
emergency dept utilization for individuals with SPMI; and 5) combined BH/PH inpatient
admission utilization for individuals with SPMI

State of Virginia: Governor’s Access Plan
(GAP)
Goal
• To help more uninsured Virginians with a serious mental illness (SMI) access needed
BH services (serves 6,000 members; projected to increase to 20,000 at peak)
• Provides limited benefit plan for individuals with SMI covering BH, medical and Rx
with a focus on community-based care
• Includes peer specialist services (F2F, warmline) provided by Magellan employees
and care coordination
Progress/Provider Impact
• No reductions of State General Funding to providers as a result of this program
• Prior to GAP, providers (particularly Medicaid) provided services to the uninsured as
unreimbursed, indigent care
• Under GAP, providers bill Magellan like all other plans in VA using unique Medicaid ID
#s. Billing process mirrors that of all other claims
• Only exception: provider billing assessments bill with SSN as the member may/may
not become enrolled, but assessment from an allowed screener is payable regardless
of enrollment

Federal Funding
Substance Abuse And Mental Health Services Administration
(SAMHSA)
• $22.9 million awarded nationwide by the U.S. Substance Abuse and
Mental Health Services Administration (SAMHSA), the Centers for
Medicare & Medicaid Services
• Purpose: Strengthen community-based mental health and substance use
disorder programs through the development of new Certified Community
Behavioral Health Clinics (CCBHC) to:
– Improve health outcomes by increasing access to quality care for all
Medicaid eligible individuals
– Reduce avoidable hospital use and complications through the
development of intermediate levels of service
– Foster better partnerships between primary care and mental health
and substance use disorder providers through co-location
– Improve the fiscal outlook for mental health and substance use
disorder care providers by improving Medicaid reimbursement

Federal Funding Available to Providers
Health Resources and Services Administration (HRSA) Behavioral Health
Integration (BHI) Grants
• 210 Behavioral Health Integration (BHI) grants in 2015, worth $51.3M.
• ACA initiative at 210 health centers in 47 states, DC and Puerto Rico
• Goal: hire new mental health professionals; add substance use disorder
health services; employ integrated models of primary care
Health Resources and Services Administration (HRSA) Substance Abuse
Service Expansion Grants (Fiscal Year 2016)
• Competitive supplement for grant funds to improve and expand delivery
of SA services provided by Health Center Programs
• Focus on Medication-assisted Treatment (MAT) in opioid use disorders.
• HRSA plans to award approximately $100 million to an estimated 310
applicants in FY 2016.

Federal Funding Available to Providers
Department of Health and Human Services
• HHS included a proposal to add certain behavioral health providers to
Electronic Health Record (EHR) Incentive Programs in its FY 2017
budget submission
• Providers include psychiatric hospitals, community mental health centers,
residential and outpatient mental health and substance abuse disorder
treatments facilities and psychologists
Administration Requests Additional $1.1B to Combat Prescription
Painkiller/Heroin Abuse in FY 2017
• Opiods involved in 30,000 deaths in US in 2014
• $500M earmarked for expansion of treatment facilities – addressing
access challenges
• Remaining $600M – prevention programs; naloxone distribution
programs; other programs

Changing Role of Providers: Challenges
and Solutions
Challenges
• Multiple standalone agencies/
safety net providers
• Dependent in large part on
state general funding
• Limited infrastructure (e.g.
technology, data analytics)
• Limited expertise with
backroom functions (e.g.
billing claims)
Solutions
• Partner, collaborate, merge
with other agencies
• Diversify funding through
mergers/new service creation
• Partnership arrangements with
an MCO
• Develop an MSO
arrangement/partner with an
MCO

Thank you!

Speaker NameTitle
Organization
Positioning for the Future of Managed Care
Dr. Lawrence GoldmanSVP, Government Relations
Beacon Health Options

Beacon’s National Scope

About Beacon Health Options
• Headquartered in Boston;
more than 70 US locations
and a London office
• 225 employer clients,
including 45 Fortune 500
companies
• Partnerships with more than
95 health plans
• Leader serving dual-eligible
beneficiaries in six states
Programs serving Medicaid recipients in 26 states and the District of Columbia
Serving 8.6 million military personnel, federal civilians and their families
Accreditation by both URAC and NCQA

Discussion Issues
• Value Based Payments
• Provider collaboration models
• Outcomes
– What can we measure
– What is really important
– How is the information used
• Challenges and opportunities ahead

Value Based Payments
“ Moving to Value – Easy to Say &
Hard to do” *
* - Monica Oss, Open Minds Daily Executive Briefing, February 22, 2016

Payment Methodologies
Fee-for-service
• One service
• One payment
Case Rate
• Group of services
• Combined payment
• Monthly/weekly paymentEpisode Bundle
• Group of services
• Combined payment
• Quality goals
• Defined time period
Total Health Outcomes
• Shared risk on total
member experience
Behavioral Health Outpatient Services
Care Management
Behavioral HealthDiversion
Behavioral HealthInpatient
Social Supports
Medical Outcomes
Behavioral Health Capitation
• Risk for providers
• Full behavioral health payment
• Defined coverage set

Transactional Relationship Model is Reinforced by
Fee-for-Service Reimbursement
Barriers to Alternative Payment Methodologies
Payer
Provider
Government
Consumer
Provider
“WE’VE ALWAYS DONE IT THIS WAY”

Alternative Payment Models Currently Used in
Several Markets
1. Outpatient Case Rates with Quality Incentive (Texas)
Treatment variability, minimal MCO pre-authorization and encouraged member movement along
treatment continuum
Incentive targets include: OP visits with 7 days of discharge, time in community standard, completion
of 340B integrated care assessments
Providers must accept all patients and submit encounters equal to 90-95% of case rates received
Case rate is significantly discounted for growth above 3-5% and are prepaid on monthly basis
2. Inpatient Case Rates (New York)
Case rate developed with each provider; is some cases-separate rate for adults v. children
Incorporates targeted LOS and reimbursement rates
No additional payment if readmission occurs within 30 days of original stay
May be reduced if target population contains certain higher end diagnosis
3. Modified Block Grant (Kansas)
Each provider negotiates annual maximum budget target and are reimbursed on FFS basis up to
this target
Providers must agree to “no eject/no reject” provisions
Per state’s discretion, additional payments can be made to providers who rendered services in
excess of budget target

Alternative Payment Models (continued)
4. Provider Partner Sub Cap (Colorado)
Full risk “down stream” (CMHCs)
BHO manages care rendered by external providers
Recipients must encounter 90-95% of capitation (maintenance of effort)
CMHC’s equity holder and board member of CMHC
5. Provider Sub-Cap (New Hampshire)
Partial risk down streamed to key CMHC’s
BHO managed care rendered by external providers
Recipients must encounter 90% of payment received (maintenance of effort)
Escalating annual quality withholds tied to achievement of specific measures; hospital
remittance, follow-up after hospitalization, care planning.
6. Risk Pool (Massachusetts)
Providers can achieve additional earnings if certain targets are met
Pools limited to specific dollar amounts and target specific levels of care
65
Outcomes:
Measure Performance & Impact
“We are interested in enabling access to the right data at
the right time at every level of the health care system,
from payer to practitioner. But we struggle with knowing
what data and analytics are important and actionable at
each level. How do we ensure providers and care
managers have the right actionable data?...” *
* - Workgroup Participant, as quoted in the National Association of Medicaid Directors Issue Brief, January 2015: Driving Innovation on
the Ground: Key issues for state Medicaid agencies in payment and delivery system reform

One solution – Outcomes Management
System (Maryland)
• Beacon Health Options (working with the Department of Mental
Hygiene) developed programming for the Outcomes Measurement
System (OMS)
– which collects information from individuals, age 6-64,
– receiving outpatient mental health treatment services in the Public
Behavioral Health System.
• OMS interviews are conducted by the clinician at the beginning of
treatment and approximately every six months during the course of
treatment.
• OMS data is displayed in the OMS Datamart and either statewide or
local jurisdiction information can be selected.
• This outcome information is integral data to informing policy and
improving consumer engagement and outcomes.




What is the future in
performance measures?
As Monica Oss wrote:
“Is one set of performance
measures possible?” *
• Can information be shared across payers?
• Will this lead to increased transparency?
• Will this allow consumer choice?
• And more….
* - Monica Oss, Open Minds Daily Briefing, February 22, 2016

The Future State of Managed
(Behavioral Health) Care
Consolidations MCO and/or Provider
Payment Reform Budget vs capitation vs global vs prospective
Outcomes Social determinants, clinical, life style, evidence based
Care integration Primary care and the specialty system
Care Coordination Connectivity to care – data analytics
The success of the Future State will be enhanced alignment of all stakeholders in the system, with transparency and collaboration around the main mission:
improve the life and health of those we serve

Thank [email protected]

Speaker NameTitle
Organization
Positioning for the Future of Managed Care
Ken AndersonVP Business Development, Government Solutions
OPTUM
Consolidation
• MCOs owning and operating BH-MCOs
• Larger and more diverse organizations –
maintain flexibility
• Positioning for the future
• Diversification
• Owning and operating direct services
• Focus on consumer and families
• Net Promoter Scores
• Provider Consolidation and diversification

Integration
• Point of Service integration
• MCO integration – single case plans and record
systems
• Population Health Management – view of the
member(s)
• Promotion and prevention
• Care Coordinator roles – linked to risk stratification
• New alignment models with provider organizations

Single Payer
• 3 Ms --- Medicaid – Medicare – Marketplace
• Dual Eligibles
• Waiver consolidation
• Population Inclusion– IDD
– LTSS
– Corrections and justice involved
– Foster Care
• Social Determinants of Health

Technology and Data
• Data, data, and more data collection and
sharing
• Aps, aps and more aps
• Multi-party service plans
• Cloud technology and telehealth
• Redesigning networks
• New payment and reimbursement models
• New integrated quality measures

Workforce
• Lack of prescribers
• Expanding roles for Peers, family members
and non-traditional providers
• Integrated health teams
• Focus on whole person
• Working with varied populations
• Community services and resources