Embed Size (px)
Citation preview
1
To comply with professional boards/associations standards:
I declare that I or my family do not have any financial relationship in any amount, occurring in the last 12 months with a commercial interest whose
products or services are discussed in my presentation. Additionally, all planners involved do not have any financial relationship.
Requirements for successful completion are attendance for the full session along with a completed session evaluation form.
Cross Country Education and all current accreditation statuses does not imply endorsement of any commercial products displayed in conjunction with this
activity.
POSITIONAL RELEASE session 203THERESA A. SCHMIDT,
DPT,MS,OCS,LMT,CEAS,CHy Cross Country Education
Leading the Way in Continuing Education and Professional Development. www.CrossCountryEducation.com
POSITIONAL RELEASE:Strain-Counterstrain
Theresa A. Schmidt, DPT,MS,OCS,LMT,CEAS,CHy
www.educise.com
Sponsored by CROSS COUNTRY EDUCATIONCopyright c 2012 Theresa A. Schmidt
2
INTRODUCTION: NEUROPHYSIOLOGY
We treat muscle problems: stiffness, weakness, pain, etc.
MUSCLE LENGTH influenced by:• Our security system:
•MONOSYNAPTIC REFLEXES•PROPRIOCEPTIVE REFLEXES
MUSCLE SPINDLEExtrafusal & Intrafusal Fibers
Extrafusal: Alpha motorneuronmonitors length of muscle
Intrafusal: Gamma motorneuronmonitors length and rate of change in length
Spindle bias is the present sensitivityto changes in length and rate of change
3
Golgi Tendon Organ
GTOs monitor tone, when stretched, GTOs fire 1B, results: inhibits alpha motorneuron
Inhibits contraction
If sensitized, may weaken muscle
ABNORMAL FACILITATION Stress overexcites nerves, lowers
threshold for stimulation, facilitates afferents, overloads adjacent segments: FACILITATED REFLEXES
Local: at the myofascial level: TPs, taut bands, tension
Segmental: at spinal nerve level, spasm, edema, ANS dysfunction in several spinal levels
4
TRIGGER POINTS: TPs
Dr. Janet Travell: “hyperirritable foci lying within taut bands of muscle which are painful on compression and which refer pain or other symptoms at a distal site”
Indicators of joint dysfunction
(Chaitow, p.59)
TRIGGER POINTS: EMGs
Persistent contraction Calcium buildup Oxygen deficit, can’t pump out
Ca++ Selective shortening of sarcomeres Must clear TPs to relax muscle(Chaitow/Headley)
Trigger Points
• Barbara Headley, PT showed trigger points can also be areas of abnormal electrical silence on EMG studies, where the muscle has too little activity, also causing a trigger point
• (Headley, Barbara.Myofascial Exams and Biofeedback: Can EMG Validate Trigger Points? ISBN 0929538080 (0-929538-08-0)
5
POSITIONAL RELEASE OR STRAIN/COUNTERSTRAIN:
Technique using tender points as diagnostic indicators of joint
dysfunction
and position of comfort to release abnormal muscle
tension and pain
INDIRECT RELEASE
Moving the joint through a range of motion
in the direction of ease
“Passive treatment” per Jones
6
JONES’ THEORY
Abnormal firing of proprioceptors
Elevated spindle sensitivity based on position of relative stretch, load and velocity
7
COUNTER STRAIN:JONES DEFINITION:
Mild strain (overstretching) applied in a direction opposite to that false and continuing message of strain from which the body is suffering: SHORTENING!
8
STRAIN/COUNTERSTRAIN JONES’ RULES
Pain is position orientedJoint dysfunction is due to abrupt reaction to strain
POC is held still for 90 seconds
the rate of return to the neutral position must be slow for
success
Joint dysfunction behaves as if it is constantly
strained:
muscle spindle is the culprit
9
Dr. Jones said: Position the tender point muscle
in its maximally shortened position:
Dr. Schmidt says: this is NOT necessary in practice
OUTCOMES OF PRT:
Decreased tissue tension
Decreased pain
Increased strength (Wong, 2004)
10
EFFECT ON PAIN & STRENGTH
Wong and Schauer: RCT of subjects with hip muscle TPs and weakness, n=49
Outcomes: VAS, HHD MMT post intervention
3 groups: SCS, EX, combined SCS+EX
Intervention: SCS hip TPs 2x/wk for 2 wks
Signif. Increase in strength in SCS and SCS+EX group
All groups had TP pain reduced and greater strength 2-4 wks post intervention(Wong & Schauer, Jnl Man Manip Ther 2004)
EFFECT ON CHRONIC ANKLE INSTABILITY
Collins, doc. dist. RCT n=27 with instability
Outcomes: isokinetic strength, dynamic balance (Ft Ank Ability Measure),
Instability (Star excursion balance test and global rating of change)
1x/wk for 4 wks with home exercise for all groups
2 groups: PRT+EX and sham+EX
NO effect on strength or subjective ankle function but dynamic stability improved
(Nova Univ., 2010)
EFFECT ON MASSETER TP PAIN AND ROM OF TMJ
Ibanez Garcia et al, RCT, n=71, 3 groups
NM technique, PRT, and control groups 1x/wk: 3 wks
Outcomes: Pressure pain threshold, AROM open jaw, VAS with 2.5kg/cm2
1 wk post intervention: No signif. diff. between tx groups, small diff compared to control(Ibanez Garcia, Jnl Man Manip Ther 1/09)
11
EFFECT ON LOCAL PAIN UPPER TRAPEZIUS
Meseguer RCT n+54 with upper trap TPs
3 groups: classic PRT, PRT with stroking, and control
Outcomes: VAS with 4.5kg/cm2 2 min after tx.
2 groups had significant pain reduction but no difference between PRT alone or PRT with stroking the TP(Meseguer et al., Clin Chiropractic 9/06)
PRECAUTION WITH PRT
As you shorten the TP muscle, you stretch the antagonist, may create delayed onset muscle soreness, let clients know to use ice!
12
PRT - INDICATIONS
Muscle guarding
Acute injury
Joint hyper/hypomobility
Fascial tension
Painful tender/trigger points
Structural dysfunction
ADL restoration
CONTRAINDICATIONS TO PRT
InfectionNonunited fractureOpen woundHematomaHealing SuturesHypersensitivity precautions
When motion is contraindicatedObtain medical clearance!
EVALUATION OF TPPerform a full exam
Document TP location, pain scale
Prioritize per severity, treat worst first
PRT is part of the Plan of treatment, may relax muscle to allow for ROM or contraction with ease
13
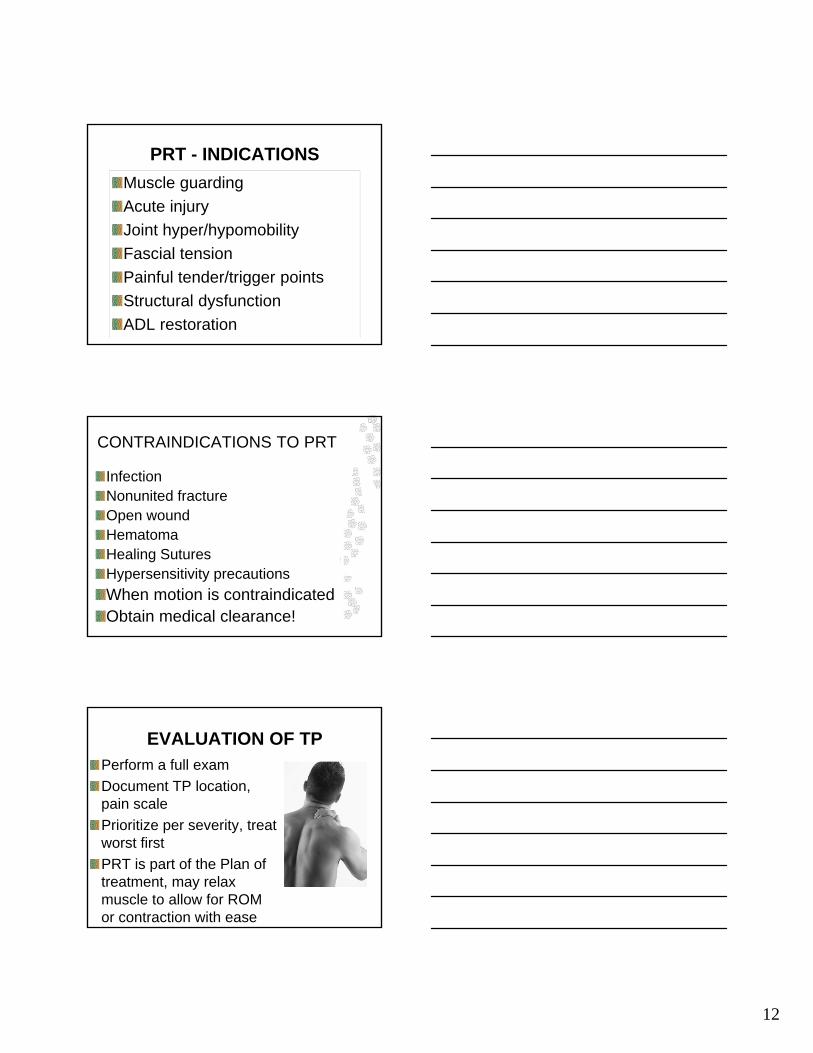
UPPER TRAPEZIUSExtend/ sidebend neck to affected side, rotate contralaterally, & elevate scapula
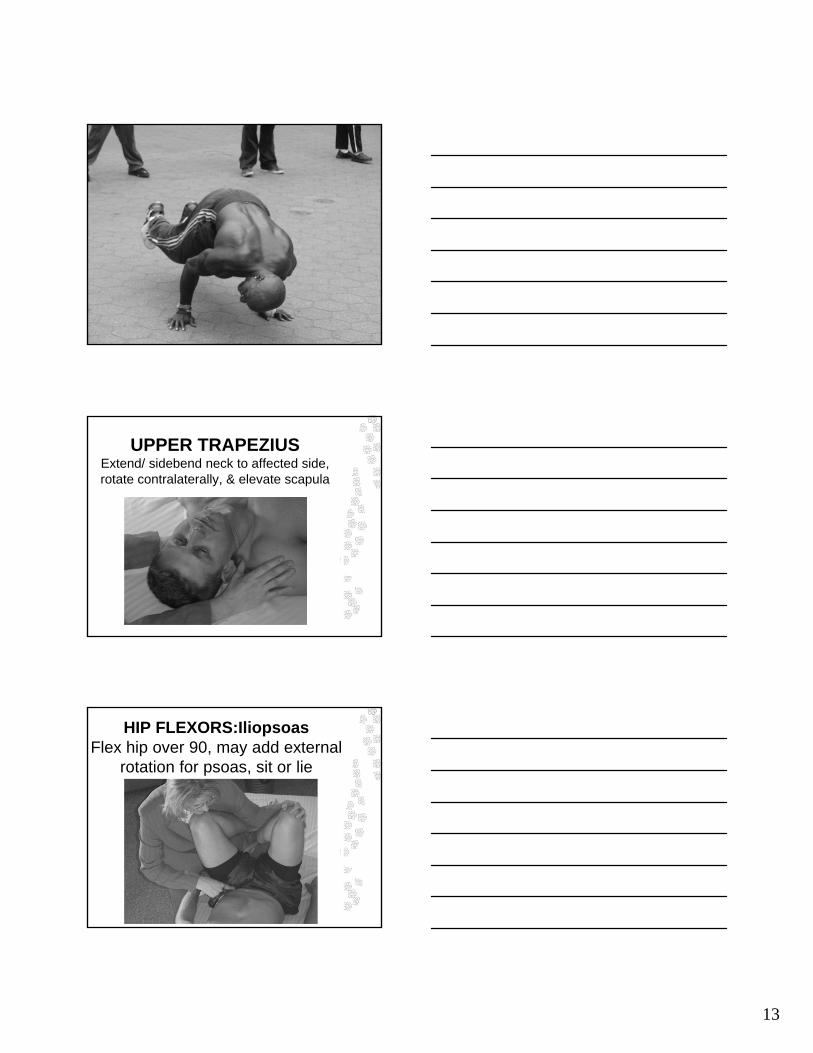
HIP FLEXORS:IliopsoasFlex hip over 90, may add external
rotation for psoas, sit or lie
14
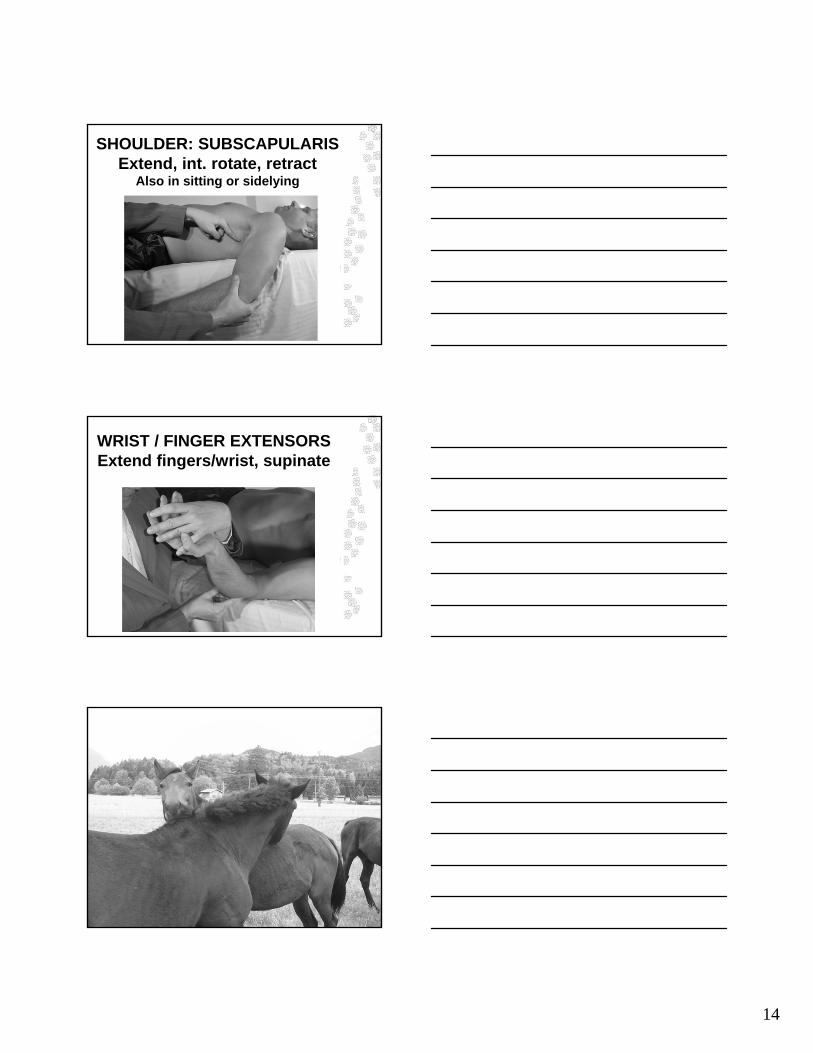
SHOULDER: SUBSCAPULARISExtend, int. rotate, retract
Also in sitting or sidelying
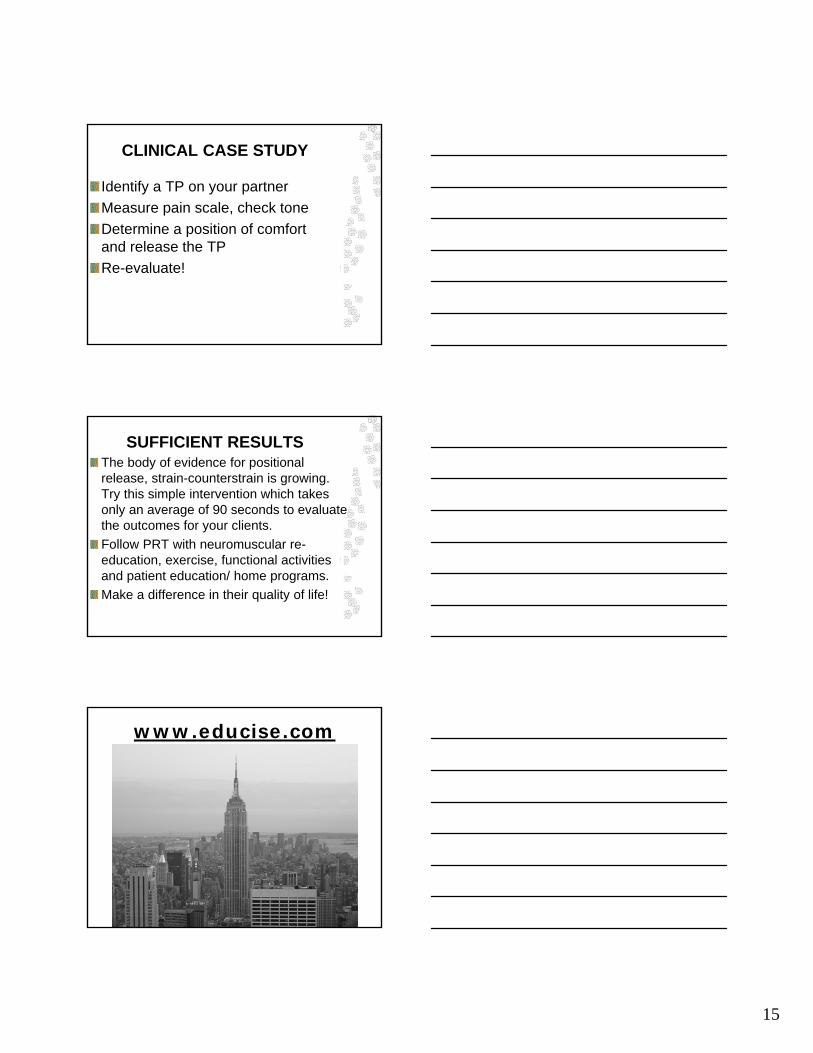
WRIST / FINGER EXTENSORSExtend fingers/wrist, supinate
15
CLINICAL CASE STUDY
Identify a TP on your partner
Measure pain scale, check tone
Determine a position of comfort and release the TP
Re-evaluate!
SUFFICIENT RESULTSThe body of evidence for positional release, strain-counterstrain is growing. Try this simple intervention which takes only an average of 90 seconds to evaluate the outcomes for your clients.
Follow PRT with neuromuscular re-education, exercise, functional activities and patient education/ home programs.
Make a difference in their quality of life!
www.educise.com
16
THANK YOU!