Embed Size (px)
Citation preview
1
In the efforts to comply with the appropriate boards/associations, I declare that I do not have any affiliations with or financial interest in a commercial organization that could pose a conflict of interest with my
presentation.
Evidence Based Rehabilitation of Individuals with Stroke
Jeremy Simmons, PT
Cross Country EducationLeading the Way in Professional Development.
www.CrossCountryEducation.com
Evidence Based Rehabilitation of Individuals with Stroke
Written and Presented by:
Jeremy K. Simmons, MPT
Section 1Stroke Statistics
• Cerebral vascular accidents are the number 3 cause of death in the United States
• Cerebral vascular accidents are the most common and lethal neurologic disorder and the number one cause of disability in adults.
• Each year 700,000 people experience a new or recurrent stroke
• 500,000 are first attacks, 200,000 are recurrent attacks
2
Risk factors
• Primary (non-modifiable)– Age
• Number one risk factor, nearly 75% of individuals who suffer a stroke are over the age of 65
• Adults over the age of 55 have a risk of stroke greater than 1 in 6.
– Race • Blacks have twice the risk of a first ever stroke compared to
whites.– Sex
• Male/female incidence rates are 1.25 for the ages 55-64, 1.5 for ages 65-74, 1.07 for ages 75-84, and .76 for 85 and older
• Because women live longer than men, more women than men die from stroke each year.
Risk Factors
• Secondary (modifiable)– Obesity
• Number 2 preventable cause of death in the United States, second only to smoking.
• Prevalence has increased by 75% since 1991
– Elevated cholesterol– HTN
• Individuals with blood pressure <120/80 have about half the lifetime risk of stroke compared those with hypertension.
– Adult onset diabetes mellitus
Risk Factors
• Smoking– Heavy smokers (>40 per day) are twice as
likely to have strokes as light smokers (<10 per day).
– After quitting, the risk level for a stroke is at the level of non-smokers by 5 years.
• Heavy Alcohol use
• Drug use
3
Risk Factors
• Physical Activity– Vigorous physical activity has been shown to
decrease risk of stroke for male and females of all racial/ethnic groups.
• A-fib– Increases risk of stroke by 5 fold
Types of strokes incidence rates
• Ischemic (88%)
• Intracerebral hemorrhage (9%)
• Subarachnoid hemorrhage (3%)
Section 2Evidence Based Treatment of
Individuals with Stroke
• Evidence for Lower Extremity Bracing• Latest research addressing spasticity
management• Up to date research regarding the most
commonly used treatments for individuals with stroke
• Functional exercise • Anatomy of the shoulder complex• Proper range of motion of the shoulder complex
4
Lower Extremity Bracing
Lower Extremity Bracing
• Objective is to provide support for weakened muscles to decrease stress on ligamentoussupport structures. In patients with spasticity the goal is to limit the movement of the joint, thus reducing the tonal response which interferes with gait.
• Wearing an Ankle Foot Orthosis (AFO) can significantly reduce body sway and increase maximum walking speed (J.A.P. Mojica et al.).
Lower Extremity Bracing
• Most patients with ankle foot orthoses feel more self-confident and experience less difficulty with a Timed Up and Go Test, Stair Test, and increased walking speed (DCM de Wit et al.)
• In mildly impaired hemiparetic patients, immediate effects of an individually designed AFO are; reduced postural sway, more weight bearing on the affected leg in stance, and reduced double limb stance time (Pohl and Mehrholz).
5
Lower Extremity Bracing
• Patient should wear the recommended braces with supportive and properly fitted footwear. Assessment of the fit of the footwear while the patient is wearing the brace is imperative to decreasing the likelihood of skin breakdown of the foot.
• After the brace has been initially fit, regular monitoring should be done by the therapist to ensure proper fit. The brace should be comfortable and create no areas of redness on the foot and ankle. IF redness develops, the patient should be referred to the orthotist immediately to have the necessary modifications completed.
Pharmacological Management of Spasticity
Pharmacological Management of Spasticity
• Benzodiazapines (Valium [Diazepam])– Benzodiazepines (ben-zoe-dye-AZ-e-peens) belong to
the group of medicines called central nervous system (CNS) depressants (medicines that slow down the nervous system).
– Diazepam is used to help relax muscles or relieve muscle spasm.
– Benzodiazepines may be habit-forming (causing mental or physical dependence), especially when taken for a long time or in high doses (http://drugs.com).
6
Pharmacological Management of Spasticity
• Tizanidine (Zanaflex)– Tizanidine is an agonist at (alpha) 2 -adrenergic
receptor sites and presumably reduces spasticity by increasing presynaptic inhibition of motor neurons. In animal models, tizanidine has no direct effect on skeletal muscle fibers or the neuromuscular junction, and no major effect on monosynaptic spinal reflexes. The effects of tizanidine are greatest on polysynaptic pathways. The overall effect of these actions is thought to reduce facilitation of spinal motor neurons (http://drugs.com).
Pharmacological Management of Spasticity
• Dantrolene (Dantrium)– Dantrium has been shown to produce relaxation by
affecting the contractile response of the skeletal muscle at a site beyond the myoneural junction, directly on the muscle itself. In skeletal muscle, Dantrium dissociates the excitation-contraction coupling, probably by interfering with the release of Ca ++ from the sarcoplasmic reticulum. This effect appears to be more pronounced in fast muscle fibers as compared to slow ones, but generally affects both. A central nervous system effect occurs, with drowsiness, dizziness, and generalized weakness occasionally present. Although Dantriumdoes not appear to directly affect the CNS, the extent of its indirect effect is unknown (http://drugs.com).
Pharmacological Management of Spasticity
• Baclofen– Baclofen selectively affects GABA-B receptors in the
CNS, inhibiting neurotransmitter release. In humans with spinal cord injuries, a defect in the GABA-B receptors is presumably involved in the production of both involuntary spasms and increased tone. Baclofen reduces the influx of calcium in presynapticterminals of afferent fibers and can affect the postsynaptic membrane by increasing the membrane potential to inhibit neuron firing (Campbell, et al.).
– Can be taken orally or administered through intrathecal catheter.
7
Pharmacological Management of Spasticity
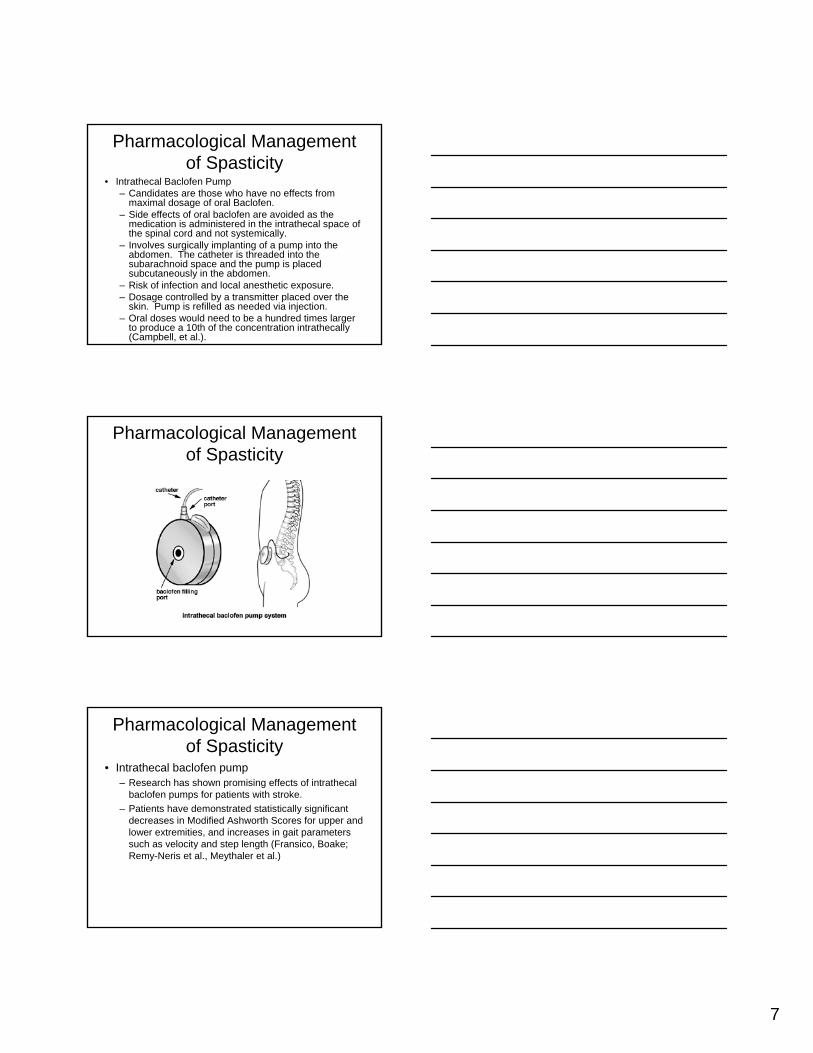
• Intrathecal Baclofen Pump– Candidates are those who have no effects from
maximal dosage of oral Baclofen.– Side effects of oral baclofen are avoided as the
medication is administered in the intrathecal space of the spinal cord and not systemically.
– Involves surgically implanting of a pump into the abdomen. The catheter is threaded into the subarachnoid space and the pump is placed subcutaneously in the abdomen.
– Risk of infection and local anesthetic exposure.– Dosage controlled by a transmitter placed over the
skin. Pump is refilled as needed via injection.– Oral doses would need to be a hundred times larger
to produce a 10th of the concentration intrathecally(Campbell, et al.).
Pharmacological Management of Spasticity
Pharmacological Management of Spasticity
• Intrathecal baclofen pump– Research has shown promising effects of intrathecal
baclofen pumps for patients with stroke.
– Patients have demonstrated statistically significant decreases in Modified Ashworth Scores for upper and lower extremities, and increases in gait parameters such as velocity and step length (Fransico, Boake; Remy-Neris et al., Meythaler et al.)
8
Pharmacological Management of Spasticity
• Botulinum Toxin type A (Botox)– BOTOX® blocks neuromuscular transmission by binding to
acceptor sites on motor or sympathetic nerve terminals, entering the nerve terminals, and inhibiting the release of acetylcholine. This inhibition occurs as the neurotoxin cleaves SNAP-25, a protein integral to the successful docking and release of acetylcholine from vesicles situated within nerve endings.
– When injected intramuscularly at therapeutic doses, BOTOX®produces partial chemical denervation of the muscle resulting in a localized reduction in muscle activity. In addition, the muscle may atrophy, axonal sprouting may occur, and extrajunctional acetylcholine receptors may develop. There is evidence that reinnervation of the muscle may occur, thus slowly reversing muscle denervation produced by BOTOX®(http://drugs.com).
Pharmacological Management of Spasticity
• Botox– Peak reduction of tone is typically obtained 4-
6 weeks following injection and effects return to baseline between 10 and 16 weeks (Cardoso et al.)
Therapeutic Treatment Interventions
9
Therapeutic Treatment Interventions
• There are numerous options for the treatment of patients who have suffered a stroke. Research has shown strong evidence that patients benefit from exercise programs in which functional tasks are directly and intensively trained (RPS Van Peppen, et al.).
Neuro Developmental Treatment (Bobath Method)
• Emphasis on the therapist normalizing tone and facilitating automatic and volitional movements through specific handling techniques of key points.
• There is no evidence that interventions based on the Bobath concept are more or less effective than other approaches for upper limb rehabilitation following stroke. The small number of studies comparing the difference between the Bobath method to other treatment interventions were found to have major design flaws (Luke et al).
Neuro Developmental Treatment (Bobath Method)
• The review performed by Luke et al. suggested that the Bobath Method was more effective than Proprioceptive Neuromuscular Facilitation in reducing muscle tone. When compared against a functional approach, the Bobath showed no significant advantage in decreasing tone.

10
Neuro Developmental Treatment (Bobath Method)
• Luke et al. went on to note that the Bobathmethod showed no advantage in improving active wrist range of motion when compared with PNF and functional approaches.
• There was limited evidence that combining wrist strengthening with Bobath interventions were more effective that the Bobath interventions alone in improving upper limb activity on the Rivermead Motor Assessment Scale (Luke et al.)
Proprioceptive Neuromuscular Facilitation (PNF)
• Uses proprioceptive, cutaneous, and auditory input to produce functional improvement of motor output.
• Characterized by rotational movements in specific patterns with manual resistance by the therapist.
• There was no recent literature found to demonstrate the effectiveness of PNF as a treatment of persons with stroke.
Partial Body Weight Supported Treadmill (PBWSTT)
11
Partial Body Weight Supported Treadmill (PBWSTT)
• Based on the model of specificity of training where the patient is suspended over a treadmill with a harness.
• Body weight is typically offloaded 20-40% and gradually decreased as the patient’s functional level improves.
• Allows patients who would not other wise be able to ambulate to have the necessary support to begin gait training earlier in their rehabilitation.
• The only inclusion criteria is that the patient be able to sit at the edge of the bed independently, standing ability is not required (Teasel et al.)
Partial Body Weight Supported Treadmill (PBWSTT)
• Conflicting evidence exists regarding the efficacy of PBWSTT with three random controlled trials showing no benefit (Teasel et al.)
• PBWSTT has not been proven more effective than Aggressive Brace Assisted Walking (ABAW) (Kosak and Reding).
• Equipment is very costly initially and requires multiple staff members to be involved when treating patients with severe impairment.
Partial Body Weight Supported Treadmill (PBWSTT)
• The STEPS Randomized Clinical trial compared assessed combined interventions and the effects of short term and long term outcomes for chronic stroke.
• Groups were PBWSTT/UE ergometry, PBWSTT/LE muscle specific exercise, Limb-loaded resisted cycling/UE ergometry, and PBWSTT/Cycling.
• PBWSTT was more effective than non-task specific training cycling.
• PBWSTT/LE muscle specific exercise did not show added benefit compared to PBWSTT alone (Sullivan, et al.).
12
Partial Body Weight Supported Treadmill (PBWSTT)
• When comparing traditional body weight supported treadmill training where the therapist assist the affected limb through swing vs. a facilitated technique where pelvic motion is controlled to limit compensatory patterns and knee flexion was assisted to initiate swing, Yagura, et al. showed no improvement in locomotor outcomes, while requiring more therapist assistance.
Early Gait Training with Orthotics
• As with PBWSTT, ABAW is based on the model of task specific training.
• The patients affected limb is supported with an AFO or KAFO while the therapist supports the patient’s pelvis. The patient ambulates using a quad cane or hemi-walker for support.
• Able to be performed by a single therapist and requires less set up time when compared to PBWSTT.
Gait training
• Functional gait training must incorporate environmental obstacles such as curbs, ramps, off camber surfaces, etc.
• When comparing numerous factors (environmental and secondary tasks) that could distract a patient during gait, it was found that unpredictable environments such as a shopping mall caused the greatest decrease in gait velocity (Lord, et al.)
13
Electrical Stimulation• Electrical Stimulation is one of the most researched
treatment techniques for individuals who are recovering from stroke.
• Two models of implementation– Cortical Plasticity
• Functional Electrical Stimulation (FES) is believed to aid in reorganization and utilization of uninvolved areas of the brain when used in conjunction with activity.
– Spasticity Reduction• The principle of the reciprocal inhibition is often
utilized by applying FES to the antagonist muscle to cause reciprocal relaxation of spastic areas (Weingarden 2006).
• Nearly all of the studies performed on upper extremity recovery required the patient have 10° active wrist and finger extension of the involved hand for inclusion.
Electrical Stimulation
• Research on functional outcomes with patients who have been treated using FES vary greatly.
• De Kroon et al. used the Ness Handmaster to improve hand function for a group of chronic stroke patients.– Two groups were studied with no control. One group was given
FES for flexion and extension, while the other group was given FES for extension only.
– No difference was noted between the groups after a 6 week treatment period and 6 week follow up.
– Over all the change from baseline was not clinically relevant.
Electrical Stimulation• Another study compared two groups receiving FES
utilizing a neural prosthesis during functional task training for 30 minutes daily times 3 weeks.
• Patients were broken into two experimental groups. Each group then acted as the control while the other received FES.– Group 1 received the training 3 weeks post CVA
– Group 2 received the training 52 weeks post CVA
• The acute stage group showed greater improvement when compared to the chronic group and controls. The researches believe that this demonstrates the idea of greater brain plasticity early in the recovery of stroke and that the higher intensity of neural traffic by utilizing FES during normal functional retraining causes greater promotion of that plasticity (Popovic)
14
Electrical Stimulation
• Ring and Rosenthal completed another research study investigating the effects of a neuroprosthetic device on upper extremity recovery for patients 3-6 mos. post stroke.
• 22 patients were divided into two groups. Both received traditional therapy based on the Bobath approach and one group received additional FES training utilizing the Ness Handmaster 3 times per day for 50 minutes. Each group was subdivided into no active motion and partial active motion of the upper extremity.
• The FES group showed statistically significant improvements in spasticity reduction for both groups and voluntary motion for the partial active motion group. Increased motion of the proximal upper extremity was noted for the no active motion group, but it was not statistically significant (Ring and Rosenthal).
Electrical Stimulation• In a large study that looked into the effects of neuromuscular
electical stimulation (NMES) on supraspinatus and posterior deltoid stimulation for patients 10 days post stroke NMES was found to have no benefit for upper extremity function at the 3 month stage of recovery.
• Two groups were studied; NMES to the shoulder 1hr, 3x/day for 4 weeks and a control group which received sham NMES for the same amount. Both groups received traditional therapies for the upper extremity.
• The researchers were surprised to find that the control group had statistically significant outcomes for favorable upper extremity movement at the 3 month reassessment.
• No change was seen in upper extremity spasticity or subluxation of the shoulder in the NMES group.
• The reason for the differences in function were theorized to be caused by excessive input to the extremity at a critical period of brain recovery interfering with re-learning processes and impeding upper limb recovery after the treatment period (Church et al.).
FES Neuroprostheses
Walk Aide
15
Bioness
Ness Handmaster
Bioness L300
Constraint Induced Therapy
• Typical exclusion criteria for Constrained Induced Therapy includes; lack of ability to extend the fingers >10°, extend the wrist 20°, bilateral CVA, balance or ambulation problems, scoring >2.5 on the motor activity log for the involved extremity, major cognitive deficits, excessive pain or spasticity, and end-stage or uncontrolled medical conditions.
• The patient’s uninvolved arm is immobilized in some way to force the patient to use only the affected arm for specific gross and fine motor tasks.
• The patient will usually be in the program 6 hours per day for 10 days, with a weekend in between. The weekend days require the patient to immobilize the unaffected arm for a set number of hours.
• Modified Constraint Induced therapy has been shown to be useful in improving the motor control of the affected extremity in stroke patients (Yen, et al.).
Strength Training
• There is moderate evidence that strength training improves the efficacy of gait post stroke (Teasell, et al.)
• Patients trained on an isokinetic exercise program for the affected lower extremity showed improvements in strength when compared against a passive range of motion group. Functional improvement was not seen between the two groups however, as there was no difference in changes in gait. Rational for the results were focused on the lack of task specificity of the exercise program (Kim et al.).
16
Strength Training
• Weiss et al. found that utilization of single joint exercise movements such as hip flexion, abduction, and extension against resistance demonstrated increased strength in the affected and unaffected lower extremities of individuals >1 year post stroke.
• The only functional performance measure that improved was sit-to-stand. Stair climbing and gait velocity did not show an improvement (Weiss et al.)
Strength Training
• A review performed by Ada et al. found that strengthening does not increase spasticity, which is a common concern.
• Strengthening appeared to be more effective early after the onset of stroke and not particularly effective in chronic stroke.
• According to Ada et al. research on the effects of strengthening limits the activity to too few muscle groups and does not examine the functional gains with specific measures. The end result is that the carryover of the strengthening done in the studies is limited (Ada et al.)
Strength Training
• When comparing a functional strengthening approach versus a traditional Bobath style approach, the functional approach showed increased weight bearing on the affected side as well as improved gait speed in the subacute phase after stroke (Bale and Strand).
• Exercises consisted of:– Step up in front by affected leg– Weight bearing by affected leg by stepping unaffected leg onto
step– Step up sideways by affected leg– Lifting affected leg up on a step– Standing to sitting to standing– Heel rise– Toe rise– Bridging
17
Strength Training• The muscles should be strengthened in the range
of motion required for specific activities. Example: Terminal hip extension must be achieved during mid-stance and terminal stance phase of gait. Positioning into maximal hip extension by the therapist during strengthening exercises causes the muscle to gain strength in the necessary range for stance limb and pelvic stability.
• Proper spotting technique is vital to the success of strengthening exercises.
• The observational skills of the therapist will determine the success or failure of the exercise
Home Exercise Program
• Emphasis should be placed on the importance of the home exercise program to increase the patient’s self responsibility in his/her rehabilitation.
• Compliance rate has shown to be low with a variety of diagnoses. Research has shown that home exercise compliance is typically 30-35% (Alexandre, et al.)
• Simplicity– The patient and/or persons caring for the patient must
understand the exercises.– Handouts should provide pictures of the exercises
and clear instructions.• Safety
– Home exercises should not put the patient or his/her caregiver at risk for injury.
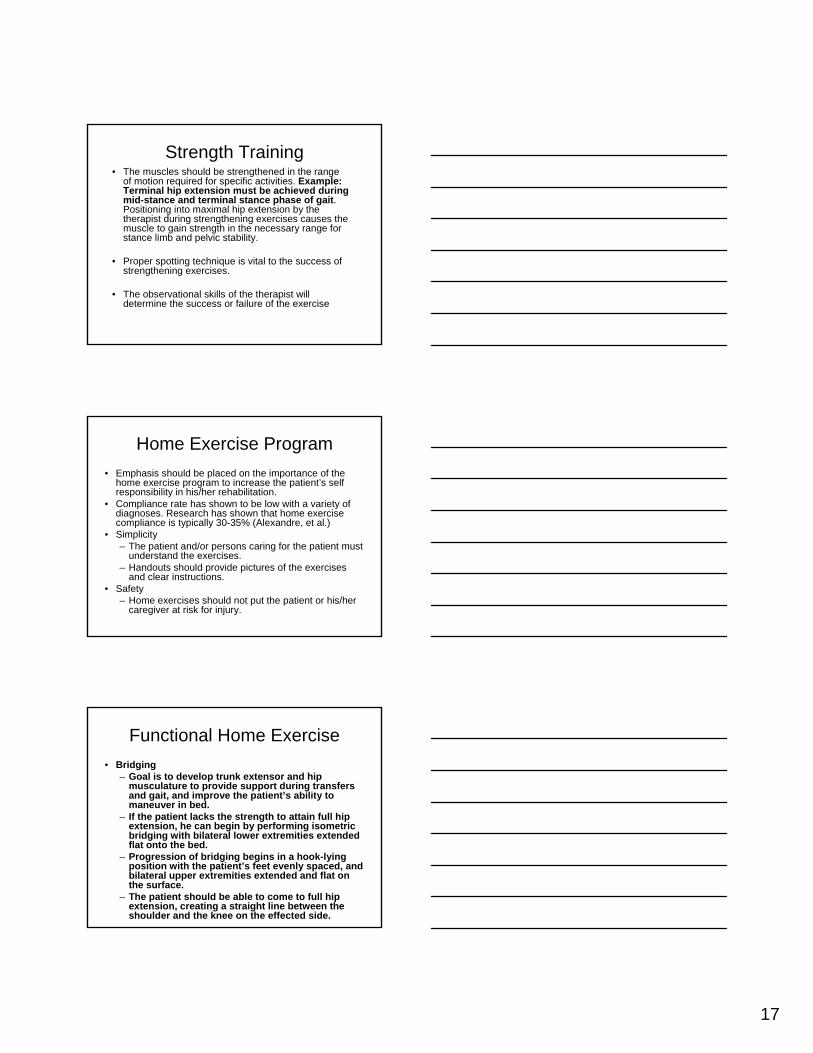
Functional Home Exercise
• Bridging– Goal is to develop trunk extensor and hip
musculature to provide support during transfers and gait, and improve the patient’s ability to maneuver in bed.
– If the patient lacks the strength to attain full hip extension, he can begin by performing isometric bridging with bilateral lower extremities extended flat onto the bed.
– Progression of bridging begins in a hook-lying position with the patient’s feet evenly spaced, and bilateral upper extremities extended and flat on the surface.
– The patient should be able to come to full hip extension, creating a straight line between the shoulder and the knee on the effected side.
18
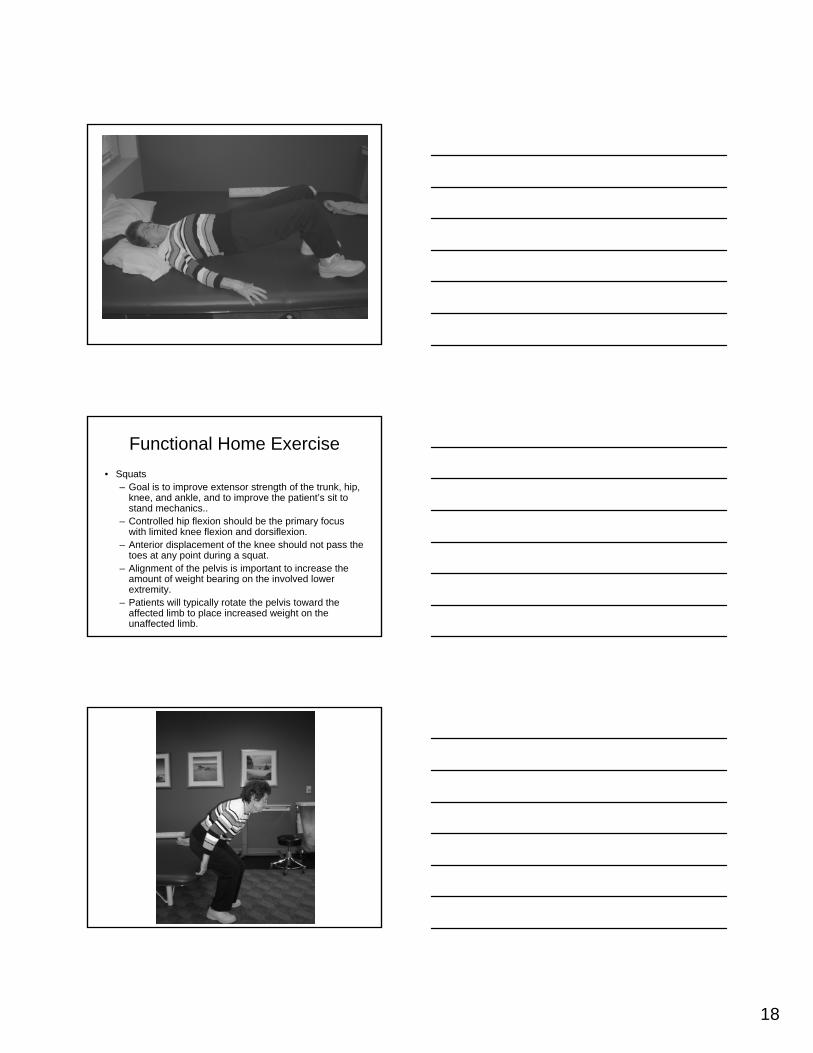
Functional Home Exercise
• Squats– Goal is to improve extensor strength of the trunk, hip,
knee, and ankle, and to improve the patient’s sit to stand mechanics..
– Controlled hip flexion should be the primary focus with limited knee flexion and dorsiflexion.
– Anterior displacement of the knee should not pass the toes at any point during a squat.
– Alignment of the pelvis is important to increase the amount of weight bearing on the involved lower extremity.
– Patients will typically rotate the pelvis toward the affected limb to place increased weight on the unaffected limb.
19
Functional Home Exercise
• Standing Weight Shift– Goal is to increase weight bearing on affected
lower extremity to improve balance and stability.
– Stand unsupported by upper extremities, and simply have the patient dorsiflex the unaffected ankle.
– Exercise can be performed with AFO donned.
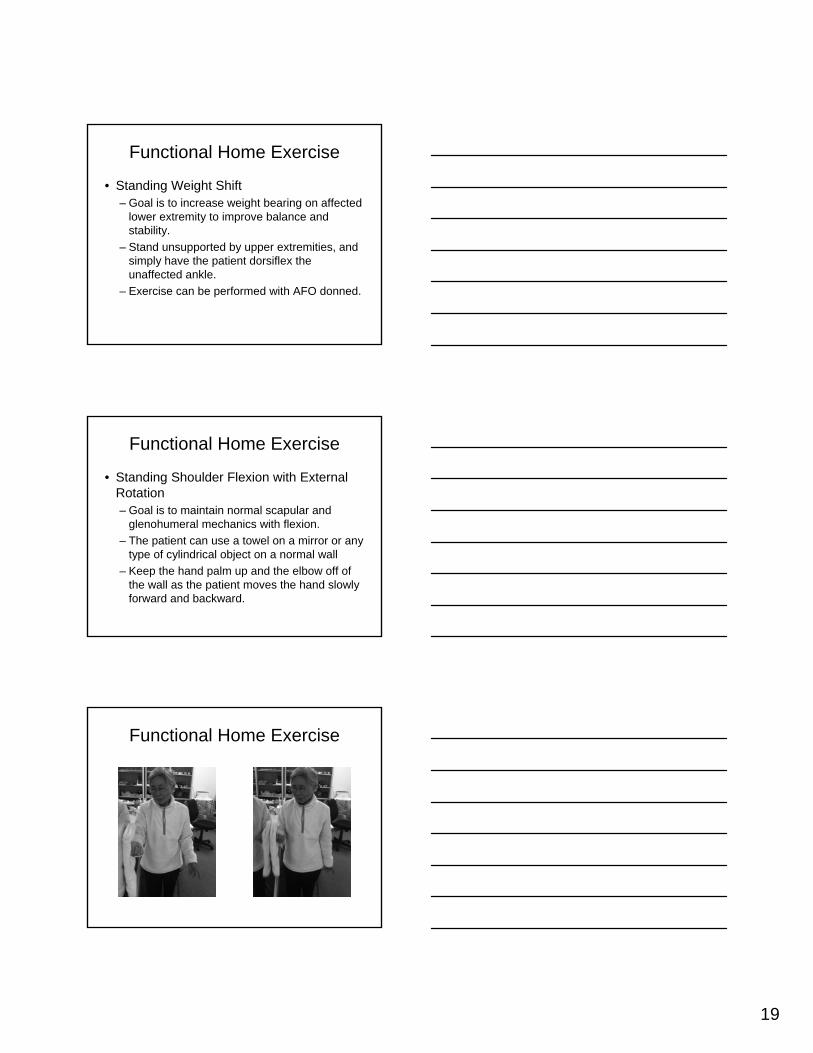
Functional Home Exercise
• Standing Shoulder Flexion with External Rotation– Goal is to maintain normal scapular and
glenohumeral mechanics with flexion.
– The patient can use a towel on a mirror or any type of cylindrical object on a normal wall
– Keep the hand palm up and the elbow off of the wall as the patient moves the hand slowly forward and backward.
Functional Home Exercise
20
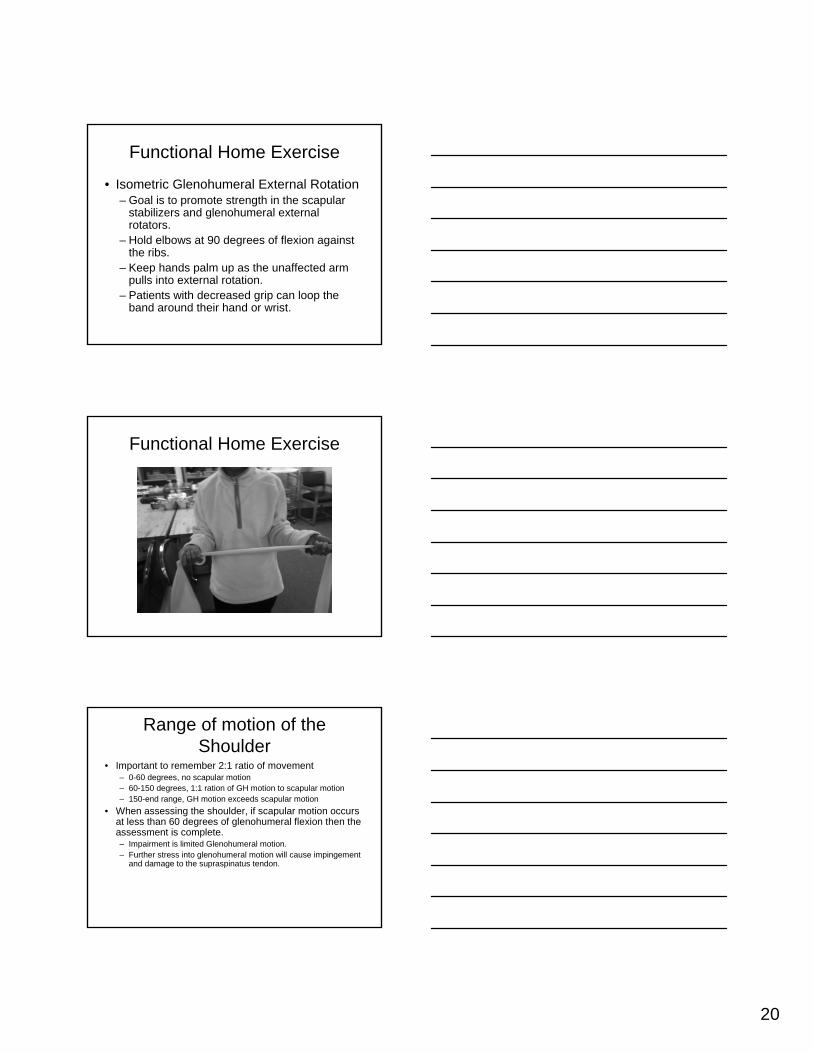
Functional Home Exercise
• Isometric Glenohumeral External Rotation– Goal is to promote strength in the scapular
stabilizers and glenohumeral external rotators.
– Hold elbows at 90 degrees of flexion against the ribs.
– Keep hands palm up as the unaffected arm pulls into external rotation.
– Patients with decreased grip can loop the band around their hand or wrist.
Functional Home Exercise
Range of motion of the Shoulder
• Important to remember 2:1 ratio of movement– 0-60 degrees, no scapular motion– 60-150 degrees, 1:1 ration of GH motion to scapular motion– 150-end range, GH motion exceeds scapular motion
• When assessing the shoulder, if scapular motion occurs at less than 60 degrees of glenohumeral flexion then the assessment is complete.– Impairment is limited Glenohumeral motion.– Further stress into glenohumeral motion will cause impingement
and damage to the supraspinatus tendon.
21
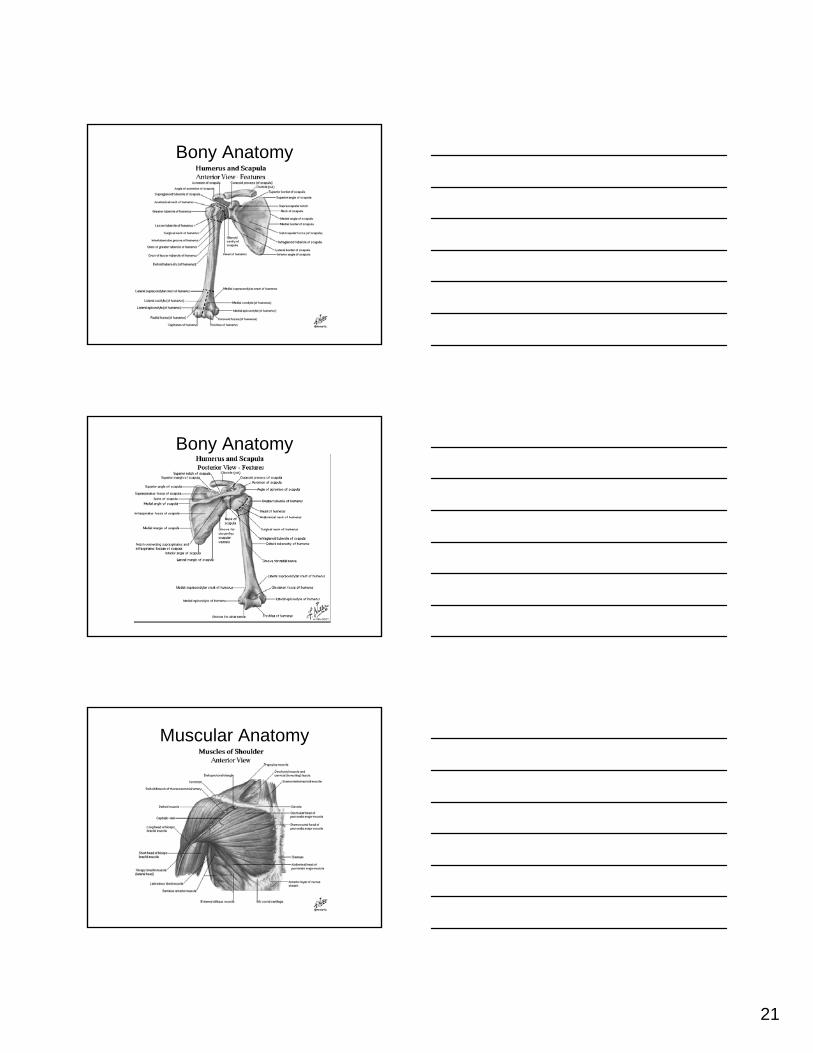
Bony Anatomy
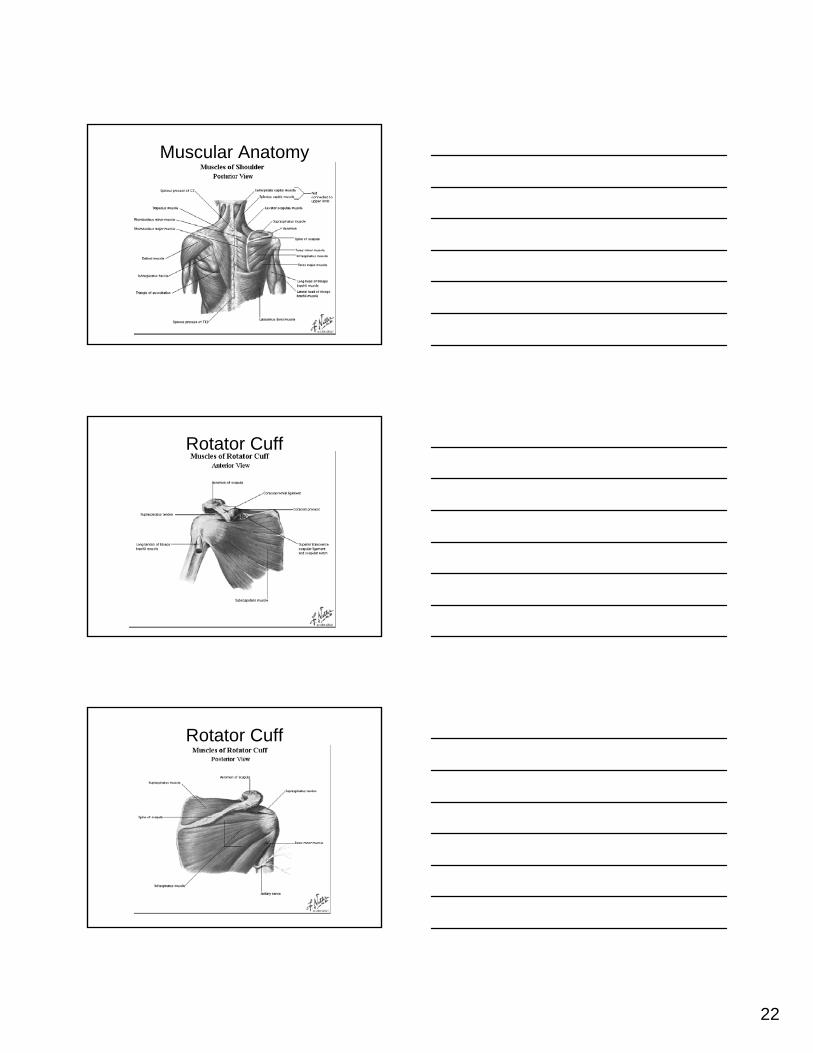
Bony Anatomy
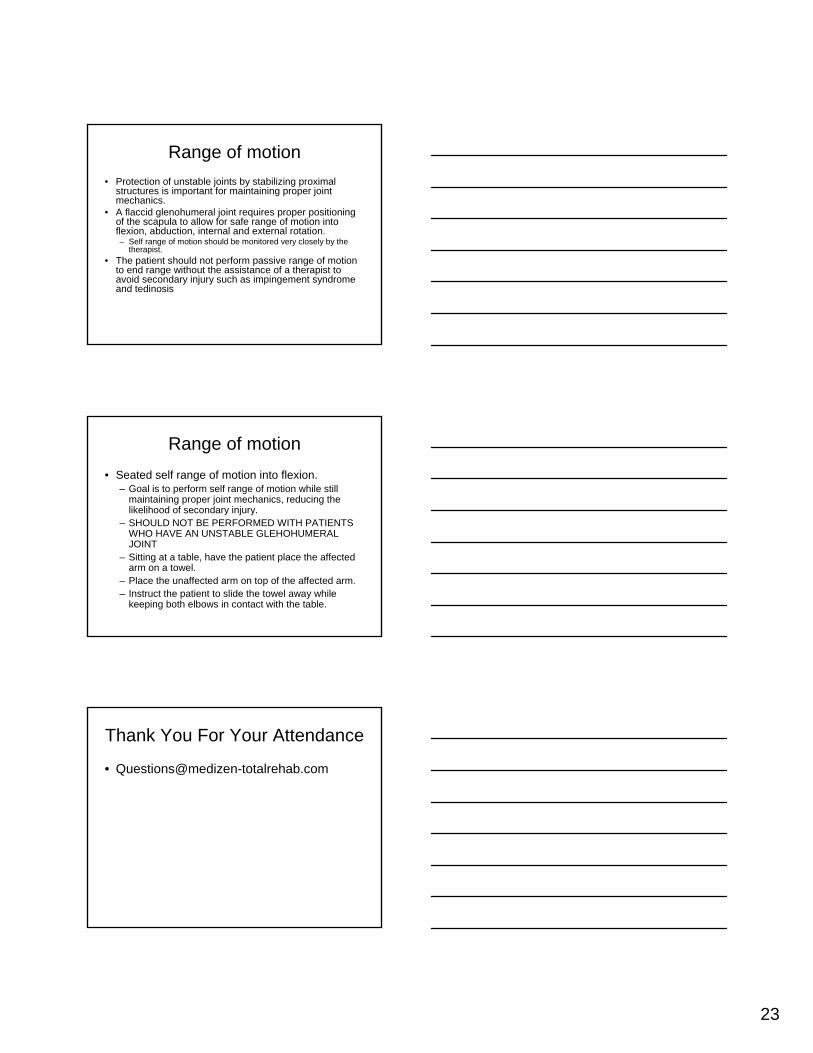
Muscular Anatomy
22
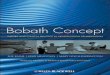
Muscular Anatomy
Rotator Cuff
Rotator Cuff
23
Range of motion
• Protection of unstable joints by stabilizing proximal structures is important for maintaining proper joint mechanics.
• A flaccid glenohumeral joint requires proper positioning of the scapula to allow for safe range of motion into flexion, abduction, internal and external rotation.– Self range of motion should be monitored very closely by the
therapist.
• The patient should not perform passive range of motion to end range without the assistance of a therapist to avoid secondary injury such as impingement syndrome and tedinosis
Range of motion
• Seated self range of motion into flexion.– Goal is to perform self range of motion while still
maintaining proper joint mechanics, reducing the likelihood of secondary injury.
– SHOULD NOT BE PERFORMED WITH PATIENTS WHO HAVE AN UNSTABLE GLEHOHUMERAL JOINT
– Sitting at a table, have the patient place the affected arm on a towel.
– Place the unaffected arm on top of the affected arm.– Instruct the patient to slide the towel away while
keeping both elbows in contact with the table.
Thank You For Your Attendance









![[PPT]PRINCIPLES OF BOBATH APPROACH - · Web viewPRINCIPLES OF BOBATH APPROACH BY – GAJANAN BHALERAO What is Bobath therapy? Bobath therapy is an interdisciplinary approach to the](https://img.pdfslide.us/doc/110x75/5aadbe627f8b9a9c2e8eb866/pptprinciples-of-bobath-approach-viewprinciples-of-bobath-approach-by-.jpg)