Embed Size (px)
Citation preview

BEHAVIOR THERAPY 26, 643-669, 1995
Portraying Alcohol Treatment Outcomes: Different Yardsticks of Success
MARK B. SOBELL
LINDA C . SOBELL
Addwtton Research Foundanon and Umverstty of Toronto
DOUGLAS R. GAVIN
Addtcnon Research Foundatton and York Umverstty
An ~mportant ~ssue m the alcohol field is how to present treatment outcome findings m a way that conveys the nature of the full range of outcomes (1.e., how indwlduals fared). Results should also be presented so as to be readily understood by practlnoners. To illustrate how treatment outcome reports can be enriched by graphic portrayals of outcome findings, previously unpublished results from a study of Graded Self-Change treatment for problem drinkers are first presented in a tradmonal manner. Then, sup- plemental graphic methods of data reporting, including the use of frequency distribu- tions and scatter plots, are presented. These portrayals are shown to address issues that receive little attennon in reports hmited to stansncal analyses. It is also shown that reported success rates, "yardsncks of success," are highly dependent on small changes m the criteria used to define success.
A longstanding but seldom addressed issue in the alcohol field is how to present treatment outcome findings in a way that conveys the nature of the full range of outcomes (i.e., how individuals fared) and the relationships be- tween different outcome dimensions. In one of the few articles to seriously address these issues, Taylor and his colleagues (1985) presented 10-year drinking outcome data for 68 male alcoholic patients who were treated in the well known "treatment" versus "advice" trial (Edwards et al., 1977), The authors used sur- vival curves and life charts to depict group outcomes on a yearly basis and
The authors would hke to express their thanks to the staff of the former Assessment Follow-Up Umt at the Chnlcal Research and Treatment Insntute who conducted all of the assessments for this study and many of the follow-up interviews, and to Wayne Skinner, Joanne Spratt, Juhe Henderson, and Slmonne LeBreton who served as therapists. Gloria Leo was tremendously helpful m conducting the study, and Even Kwan and Gfl Sitaremos assisted with the statlsncal analyses Curtis Breshn provided valuable comments on the manuscript. Also, sm anonymous reviewers provided highly valuable comments.
Requests for reprints should be addressed to M.B. Sobell, Center for Psychological Studies, Nova Southeastern University, 3301 College Ave., Fort Lauderdale, Florida 33314
643 0005-7894/95/0643-066951 00/0 Copyright 1995 by Assoclanon for Advancement of Behavior Therapy
All rights of reproducnon m any form reserved

644 SOBELL ET AL.
used a barycentrlc coordinate plot to present individual variation in amount of time spent in three drinking categories (abstinent, social drinking, trou- bled drinking) over the 10 years. Although subjects showed stable patterns over time, the patterns were composed of "a patchwork of drinking and absti- nence" (p. 50), leading the authors to conclude that outcome is most usefully conceived as a "dynamic rather than a static concept" (p. 50). The article by Taylor and his colleagues clearly shows that presentations of treatment out- come reports can be far more informative than typically is the case. For example, innovative methods such as graphical portrayals of outcomes can convey more information and in a more comprehensible manner than can be communicated by statistical analyses alone. Such methods have not yet been applied, however, to the presentation of outcome findings for shorter intervals.
The nature of outcomes over shorter intervals is ~mportant not just from the standpoint of knowing how treated indwiduals fare, but also because shorter term outcomes are more likely to reflect treatment effects than outcomes over extended intervals (Moos & Finney, 1985). More specific knowledge of the na- ture of outcomes might suggest treatment improvements or shed light on treat- ment mechanisms. For example, assessing multiple dimensions of drinking behavior might reveal that one method of treatment leads to a reduction in the frequency of drinking but not in the amount consumed, whereas another method might affect the magnitude rather than the frequency of drinking. Reasons why this occurred could be explored, and the different methods could be matched to specific client subgroups. For instance, binge drinkers might benefit more from a treatment that affected the magnitude of consumption versus the frequency of drinking.
Because the ultimate objective of treatment research is to influence clinical practice, results should be presented in such a way that they can be readily understood by practitioners. Unfortunately, many practitioners lack the time and background to disentangle complicated statistical presentations of results (Dies, 1983). Thus, it would be valuable to present findings in a way that facili- tates readers' comprehension of the nature of treatment outcomes.
This article uses an existing data set to present ways of supplementing statistical outcome reports with graphic portrayals that present a great deal of information in a relatively easily understood format. These data have not been presented elsewhere, although the treatment procedures have been de- scribed in detail as part o f a clinical guidebook (M. B. Sobell & Sobell, 1993a). Because the study has not been presented previously in the empirical litera- ture, this article includes a brief description of the treatment rationale and procedures before discussing methods of data presentation. Findings, along with a discussion of the main conclusions emanating from that analysis, are then first presented in the traditional statistical manner. Building on this back- ground, the remainder of the paper then explores supplemental methods of portraying outcome findings. The treatment study, therefore, can be thought of as constituting a paper within a paper, with a larger purpose than a simple research report.

PORTRAYING TREATMENT OUTCOMES 645
Methods Guided Self-Change Treatment
Problem drinkers, persons who have low severity alcohol problems (M. B. Sobell & Sobell, 1993a, 1993b), are abundant in number, greatly outnumbering those who are severely dependent on alcohol (Institute of Medicine, 1990). Historically, behavioral treatments for alcohol problems have emphasized skills training based on the assumption that individuals engage in excessive drinking as an inappropriate coping response (M. B. Sobell, Wilkinson, & Sobell, 1990). However, it has been found that problem drinkers respond well to brief inter- ventions involving, at the most, a few sessions (Bien, Miller, & Tonigan, 1993). The success of brief treatments calls into question whether skills training is necessary for problem drinkers. A parsimonious explanation of the efficacy of brief treatments is that the major effect of such interventions is motiva- tional: if problem drinkers want to change, they already have the necessary skills and resources to do so. Miller (1985, 1986/87; Miller & Rollnick, 1991) has suggested that motivation can be conceptualized as a state of readiness to engage in behaviors intended to achieve some goal, rather than as a person- ality trait. Viewed as a state, motivation can be influenced by several factors. In a motivationally based treatment, a major objective is to help individuals use their existing skills to solve their problems.
Guided Self-Change (GSC) is a short-term motivationally based treatment specifically designed to appeal to and be appropriate for problem drinkers. The data presented in this article are from a randomized trial that compared the effectiveness of GSC treatment with and without a cognitive relapse preven- tion component. The relapse prevention component was tested as a supple- ment to GSC because it was hypothesized that the relapse prevention perspec- tive would help maintain treatment gains. Because strong ties between the therapist and client would not be expected to occur in a brief treatment, an important treatment component should be to prepare clients for dealing with problems encountered after treatment. Relapse prevention, which focuses on the maintenance of treatment effects (Marlatt & George, 1984), is an obvious candidate for maintaining behavior change. The cognitive component of re- lapse prevention tested in this study involved encouraging the client to adopt the perspective that relapses may occur following treatment, and that how one deals with relapses is important: (1) relapses should be interrupted as soon as possible in order to minimize consequences; (2) relapses should be consid- ered as learning experiences that identify previously unrecognized high risk situauons or inadequate methods of coping; and (3) relapses should not be attributed to personal failings (which would promote low self-efficacy), but rather to situational factors that can be dealt with in the future.
Subjects Persons seeking treatment for alcohol problems at the Addiction Research
Foundation (Toronto) who volunteered to participate in a treatment study in- volving a GSC treatment (M. B. Sobell & Sobell, 1993a) were screened at a

646 SOBELL ZZ At.
centralized Assessment/Follow-Up Unit. Clients were eligible if they: (1) had a primary alcohol problem; (2) read and wrote English; (3) were between 19 and 60 years of age; (4) had an Alcohol Dependence Scale (ADS; Skinner & Allen, 1982) score of ~< 21; (5) were not legally coerced to participate in treatment; (6) passed a screening to exclude possible organic brain damage; (7) lived within 100 km of Toronto; (8) had not participated in formal alcohol or drug treatment within the past year; (9) were not currently receiving psy- chiatric treatment or medications for major psychiatric problems; (10) had not changed residence more than four times in the preceding year; (I1) reported never having experienced major alcohol withdrawal symptoms; (12) provided the name of a collateral to be contacted for follow up; (13) reported average alcohol consumption no greater than 12 standard drinks (13 g ethanol each) on >i 5 days per week during the 6 months prior to assessment; and (14) signed an informed consent.
Eligible clients were randomly assigned to one of two GSC treatment con- ditions: Behavioral Counseling Only (Group BC), or Behavioral Counseling plus Cognitive Relapse Prevention (Group RP). Four female and two male experienced outpatient therapists conducted the individual treatment sessions. Randomization was blocked so that each therapist saw an equal number of subjects in each treatment condition, and gender was balanced across condi- tions. I f a subject failed to complete treatment, a new subject was substituted to maintain the balance among therapists, gender, and conditions.
To obtain 100 subjects (50 in each group), 129 subjects entered the study. Of the 29 who did not complete the treatment, 17 were in Group BC and 12 in Group RP. This difference between groups was not significant (p > .05), nor were there any significant differences in demographic and drinking his- tory variables between dropouts and treatment completers. For describing the sample, data from all 100 completers have been combined.
Treatment completers had a mean (SD) age of 37.3 (8.82) years and a mean (SD) education of 14.8 (3.5) years, 49% were married, 89% were employed, and for 83% it was their first treatment experience. They had a mean (SD) ADS score of 12.8 (4.6). Their drinking was not extremely heavy, especially compared with studies of severely dependent alcohol abusers (e.g., Foy, Nunn, & Rychtarik, 1984; Ito, Donovan, & Hall, 1988; Kuchipudi, Hobein, Flick- inger, & Iber, 1990). Collectively, subjects drank on 68.2% of all days during the pretreatment year. When they drank, 38.7% of the days involved ~< 4 drinks (1 drink = 13.6g absolute ethanol), and only 16.8% of the days involved >/10 drinks. Subjects' mean (SD) drinks consumed per drinking day was 6.2 (2.7). However, subjects reported a substantial number of alcohol-related conse- quences. The percentages of subjects reporting various types of consequences were as follows: 21% legal, 27% health, 37% affective, 47% financial, 47.5% vocational, 56% aggression, 78°70 cognitive, and 81% interpersonal. Subjects were also asked to provide a subjective evaluation of the severity of their drinking problem over the previous year: 78% evaluated their problem as "major" or "very major," which was defined as having suffered at least one or more serious alcohol-related consequence. It should be noted that although the terms "major" and "very major" are used here because those terms were

PORTRAYING TREATMENT OUTCOMES 647
used in the question posed to clients, the types of consequences described by these problem drinkers typically were far less serious than consequences reported by severely dependent individuals (e.g., relationship dissolutions, mul- tiple job losses, liver disease).
Procedures
Treatment procedures are only summarized here because they have been de- scribed in great detail elsewhere (M. B. Sobell & Sobell, 1993a). The treatment protocols were specified in a therapist manual prepared for the study. They consisted of a 2-hour assessment, followed by two 90-minute structured ses- sions, and supplemented by readings and homework assignments. The assess- ment was conducted by staff uninformed about subjects' group assignments. Assessment information gathered included (a) demographic and substance abuse history information, (b) the Inventory of Drinking Situations (IDS; measures the extent to which subjects report that they drank heavily in certain types of situations in the past year; Annis, Graham, & Davis, 1987), (c) the Situational Confidence Questionnaire (SCQ; a state measure of self-efficacy or confidence to resist the urge to drink heavily for the same situations as in the IDS; Annis & Graham, 1988), (d) a Timeline Followback interview (TLFB; collected subjects' estimates of their drinking over the past year; L. C. Sobell & Sobell, 1992), and (e) a medical screening. At the assessment and at each treatment session subjects specified a self-selected goal (i.e., abstinence or re- duced drinking) on a Goal Statement form. Subjects with medical contraindi- cations to drinking (n -- 4) were told that they should not drink at all. Sub- jects selecting a reduced drinking goal (n = 80) had to specify limits for quantity and frequency of consumption and had to list situations in which drinking would not occur. Although subjects choosing a reduced drinking goal initially specified their own limits for drinking, in the first treatment session advice on specific low risk drinking guidelines was provided.
At the assessment, subjects were given a short reading and a homework as- signment. The reading described drinking from a behavioral perspective (e.g., antecedents, consequences) and provided a framework for subjects to orga- nize information they had reported during the assessment. The homework asked subjects to functionally analyze their three most serious problem drinking situations by identifying triggers (high-risk situations) associated with the drinking and evaluating the consequences of the drinking (good and bad, im- mediate and delayed). Thus, before the first session, subjects were familiar with the treatment orientation and had begun a detailed analysis of their problem drinking.
At the first session, subjects' homework assignment answers and their un- derstanding of the reading were discussed. When subjects' goal statements were discussed, they were advised of the following recommendations for a re- duced drinking goal: (1) consume not more than three standard drinks on any given day (Babor, Kranzler, & Lauerman, 1987); (2) drink on not more than 4 days per week (Sanchez-Craig, 1986) in order to help avoid developing ex- cessive tolerance or habitual components to the drinking; (3) never drink in high-risk circumstances; (4) drink at a rate no faster than one drink per hour

648 SOBELL ET AL.
if there was a possibility of driving; and (5) consider imposing a 15-20 minute delay period between making a decision to drink and acting on that decision (Cummings, Gordon, & Marlatt, 1980).
At the end of the first session, subjects were given a second brief reading and a homework assignment and asked to bring the completed homework to their next session. The reading described behavioral problem solving proce- dures. The homework required clients to develop "options" (alternatwe ways of responding) for the problem drinking situations identified in their first home- work. After identifying options, they evaluated each for its feasibility and potential effectiveness and selected the best and second best options for which they then developed "action plans" (i.e., detailed steps to be taken in order to enact the option).
At each treatment session, the therapist reviewed the rationale for the readings and explored subjects' understanding of the material. Subjects' an- swers to the homework assignments were discussed and elaborated upon if necessary. Subjects were also asked to discuss any personal strengths and re- sources they could use in dealing with their drinking problem (e.g., how they had successfully dealt with other problems in their lives, how they had quit smoking or sustained a weight loss, or activities in which they might engage to fill rime freed up by stopping or reducing drinking). Finally, they reported their drinking since the last session using the TLFB technique.
Procedures for the RP and BC treatment conditions differed in two ways. First, the RP subjects' readings contained sections on relapse management, relapse prevention, and the importance of viewing recovery from a long-term perspective. Second, during the sessions the relapse prevention components were discussed in relation to the readings. These components were absent from all BC subjects' treatment. As a quality control procedure to assure the dis- criminability between the RP and BC treatments, all sessions were tape recorded and a randomly selected session for each subject was reviewed by a research assistant for compliance with the protocol. In only one case was a protocol violation observed (a BC subject was treated with RP procedures) and that instance had been reported by the therapist. The subject was replaced by an- other randomly selected subject.
At both sessions, subjects were told that, although the structured treatment involved two sessions, they could contact their therapist at any time they felt they needed further treatment. In response to subjects' requests, therapists were free to conduct further sessions or refer subjects to other services.
Follow-up interviews were scheduled with subjects at 1, 3, 6, 12, 18, and 24 months, and the interviewer was to be the assessment worker who had first assessed the subject. Unfortunately, considerable staffturnover in the Assess- ment/Follow-Up Unit over the course of the study resulted in most subjects being followed by a research assistant who had not conducted the assessments. The information gathered at follow-up contacts largely paralleled that gathered at the pretreatment assessment.
After about half of the subjects had entered the follow-up phase, it became apparent that the data collection for these relatively well functioning, highly stable clients was too intense for a two-session treatment. Several of the sub-

PORTRAYING TREATMENT OUTCOMES 649
jects who had withdrawn from the follow-up phase had told the interviewer that they did not have time to participate in follow-up. Thus, to gather data from as many subjects as possible, subjects who had withdrawn from follow- up were contacted and asked if they would agree to participate in an abbreviated follow-up interview. This increased the follow-up completion rate by about 10070. Follow-up interviews were also scheduled to be conducted with subjects' collaterals at 6-month intervals. Collaterals were asked to describe the sub- ject's drinking over a 30-day period using a modified TLFB procedure, which involved reporting categories of drinking (L. C. Sobell et al., 1986), and to report any alcohol-related consequences experienced by the subject.
Results and Discussion: Relapse Prevention as a Component of Guided Self-Change Treatment
To illustrate the ways in which treatment outcome reports can be enriched by graphic portrayals of outcome findings, study results are first presented and discussed in a traditional manner, summarizing the major statistical analyses. Following this, suggested supplemental methods of data presentation are con- sidered.
Follow-Up Sample At 6 months, follow up was completed on 85°7o of the subjects who com-
pleted treatment (42 in Group BC and 43 in Group RP) and on 73°7o at 12 months (37 in Group BC and 36 in Group RP). Chi-square analyses for differen- tial dropout by treatment condition indicated no significant effect. Inability to locate subjects accounted for 46.707o of the attrition at 6 months and 33.307o at 12 months; the remaining cases were located but refused to continue in follow up. Similar follow-up attrition rates have been reported in other outcome studies of problem drinkers (e.g., Alden, 1978; Anderson & Scott, 1992; Annis & Peachey, 1992; Heather, Kissoon-Singh, & Fenton, 1990; Miller, Benefield, & Tonigan, 1993; Sanchez-Craig, Annis, Bornet, & MacDonald, 1984).
A series of analyses evaluated differences between early follow-up drop outs and those for whom some follow-up data were gathered. These analyses ex- amined demographic variables, drinking history, and pretreatment and within- treatment drinking behavior. A Bonferroni procedure was applied to correct for the multiple comparisons, but using an alpha level adjusted to .25, the mid-point of the range (.20 to .30) suggested by Winer (1971) when discussing how to form conclusions of no difference. Only one significant difference was obtained. Early dropouts had a lower percentage of limited drinking days (con- sumption of ~ 4 drinks) during the pretreatment year than completers [Drop- outs Mean = 12.7407o; Completers Mean = 29.81070, t = 3.50, df = 32.61 (unequal variance), p = .001]. The reason for this difference is unknown. One possibility is that the early dropouts may have tended to be binge drinkers (i.e., either drank heavily or not at all), although it is not clear why this would affect their participation in follow up. When the same procedures were ap- plied to evaluate potential differences between the 6-month follow-up dropouts and subjects for whom 12 months of follow-up data were collected, no differ-

650 SOBELL ET AL.
ences attained statistical significance. The two groups did not differ significantly on any drinking behavior variable over the first 6 months of follow-up.
Because the 12-montfi period provides a comparison interval equivalent to the pretreatment period, the analyses presented here are for the 12-month follow-up Interval. Findings of analyses using 6-month follow-up data were consistent with those of the analyses based on 12-month follow-up.
Group Drinking Outcomes Over Time
Subjects' total number of drinks consumed over the follow-up year was 53.8% less than their reported drinking for the year prior to treatment. Similar reductions have been reported in other studies using brief interventions with problem drinkers (e.g., Graber & Miller, 1988; Sanchez-Craig, Leigh, Spivack, & Lei, 1989; Sanchez-Craig, Spivack, & Davila, 1991; M. B. Sobell et al., 1980).
Group drinking outcomes were analyzed using multivariate analyses of vari- ance (MANOVA) for repeated measures. The dependent variables were propor- tion of days abstinent, proportion of drinking days in which 1 to 4 standard drinks were consumed, the proportion of drinking days in which >1 10 stan- dard drinks were consumed and the mean number of standard drinks con- sumed per drinking day. Analyses for days when 5 to 9 drinks were consumed were not conducted because this variable would be fully determined by knowl- edge of the values of the other variables. The independent variables were oc- casion (within-subjects variable: pretreatment, treatment, follow-up) and con- dition (between-subjects variable: BC, RP). Wilk's Lambda was used as the multivariate criterion. Significant effects were probed using unlvariate tests and multiple comparison procedures, and significant interactions were ex- amined.
The MANOVA found no significant overall effects for condition (p > .05) or condition-occasion interactions, but there was a significant overall effect for occasion, Wilk's Lamda F(8,60) = 15.60, p < .001. The occasion effect was probed using univariate tests for the dependent variables; all dependent variables showed an occasion effect. The significant univariate tests were then probed using multiple comparisons that compared pretreatment to the com- bined treatment and follow-up intervals, and follow-up to the treatment in- terval. Working within the constraints on degrees of freedom available for the comparisons, this combination of tests was preferred to testing follow up against either the pretreatment or treatment interval alone. For all of the de- pendent variables, these'contrasts showed that the pretreatment interval was significantly different from the combined treatment and follow-up intervals, and that the treatment and follow up intervals did not differ significantly. Table 1 displays pretreatment, treatment, and follow-up means and standard devia- tions for the two treatment conditions and the four dependent variables in- cluded in the MANOVA.
Outcome Measures Other Than Drmking
Consequence data gathered in this study covered nine areas: work prob- lems, maj or withdrawals, physical health problems, cognitive problems, affec- tive problems, interpersonal problems, verbal or physical aggression, legal prob-

PORTRAYING TREATMENT OUTCOMES 651
T A B L E 1
MEANS (SD) FOR T w o TREATMENT CONDITIONS (BEHAVIORAL COUNSELING, BC, N = 36; BEHAVIORAL COUNSELING PLUS COGNITIVE RELAPSE PREVENTION, RP, N = 33),
OVER THREE INTERVALS (l YR PRETREATMENT, WITHIN=TREATMENT, 1 YR POSTTREATMENT) FOR FOUR OUTCOME VARIABLES
Interval
Treatment Condition Pretreatment Within-Treatment Posttreatment
Proportion of Total Days Abstinent
BC 0 32 (0 26) 0 58 (0.35) 0 61 (0.30) RP 0.33 (0 29) 0 45 (0 35) 0 50 (0.29)
Proportion of Drinking Days Consumed 1-4 Standard Drinks
BC 0 35 (0 33) 0.59 (0 39) 0.59 (0 38) RP 0.49 (0 30) 0.68 (0.27) 0.73 (0 29)
Proporuon of Drinking Days Consumed /> 10 Standard Drinks
BC 0 21 (0.31) 0 11 (0 21) 0 10 (0.16) RP 0 09 (0 19) 0.01 (0.03) 0.03 (0.06)
Mean Number of Standard Drinks Consumed per Drinking Day
BC 672 (3.03) 4 11 (295) 421 (261) RP 5 05 (2 20) 3 58 (1 41) 3 58 (1 72)
lems, and f inancial problems. For purposes o f s ta t is t ical evaluat ion, a consequence var iable was created by d icho tomiz ing subjec ts ' responses (i.e., yes, no), with scores ranging f rom 0 to 9. A n eva lua t ion o f scale rel iabi l i ty using the fol low-up sample (65 usable cases) y ie lded a Cronbach ' s a lpha o f .68. This value is acceptable for using the c o m b i n e d scores in research appl i - cat ions. Consequence scores were evalua ted using a 2 ( t rea tment condi t ion: BC, RP) × 2 (interval: p re t rea tment , pos t t r ea tmen t ) repeated measures anal- ysis o f variance. This analysis found no significant effect for t r ea tment condi - t ions, and no significant in terac t ion effect. A signif icant interval effect was ob- tained, F(1,63) = 56.73, p < .001; subjects ' mean (SD) pretreatment consequence score o f 4.1 (1.84) decreased to 1.7 (1.82) pos t t rea tment .
A n o t h e r ou t come measure consis ted o f cl ients ' rat ings o f the severity o f their d r ink ing problems. There were five categories: (1) not a p rob lem (no con- sequences or worry); (2) very m i n o r p rob lem (worry, but no consequences); (3) m i n o r p rob l em (one or more consequences but none the subject cons id- ered serious); (4) m a j o r p rob lem (one consequence cons idered serious); and (5) very m a j o r p rob lem (more than one consequence cons idered serious). For purposes o f s ta t is t ical analysis , these categor ies were considered to const i tute a 5-poin t scale and they were subjected to a 2 ( t rea tment condi t ion : BC, RP) × 2 (interval: pretreatment , pos t t rea tment) repeated measures analysis o f vari- ance. This analysis y ie lded no significant cond i t ion effect, but the effect for

652 SOBELL ET AL.
occasion was significant, F(1,65) = 48.81, p < .001, with mean (SD) subjective problem severity ratings significantly less following treatment [2.97 (0.97)] than prior to treatment [4.01 (0.74)]. It should be recalled that a score of 2 indicates that no negative consequences were actually experienced. The occasion effect was qualified by a significant condition × occasion interaction, F(1,65) = 4.19, p = .045, which appeared to reflect that group RP subjects changed less (mean change = -0 .72) than group BC subjects (mean change = 1.31). Because this was the only one of several outcome analyses to yield a significant interac- tion, and the probability attained was just below the .05 criterion, it is likely that the interaction effect was a chance occurrence.
Relattonsh(p Between Drinking and Consequences Dtmenstons
To evaluate the relationship between the number of consequences subjects experienced over the follow-up year and heavy drinking, the number of con- sequences was correlated with the percentage of days they consumed five or more drinks during that interval. Although the correlation between these vari- ables was statistically significant (r= .28, n = 64, p =.025), the relationship accounted for less than 8°7o of the variance in the data.
Predwtors o f Outcome To evaluate variables potentially predictive o f outcome, multiple regression
analyses were conducted using as dependent variables the mean frequency of abstinent days, mean drinks per drinking day, mean number of drinks per week, and mean number of consequences over the follow-up year. Babor et al. (in press), using results from four studies, found that measures of drinking frequency and intensity (drinks per drinking day) were relatively uncorrelated, suggesting that they "represent independent dimensions of drinking behavior." Predictor variables were the following pretreatment and treatment factors: age, gender, years of education, marital status, employment status, pretreatment mean drinks per drinking day, ADS score, drinking goal at assessment, pretreat- ment alcohol consequence score, frequency of abstinent days pretreatment, pretreatment SCQ score, and end of treatment SCQ score. Multiple regres- sion analysis was chosen over the use of discriminant analysis because it takes into account gradations in improvement.
Multiple regression analyses were performed in order to identify the best set of predictors for each of the outcome variables. Although initial analyses indicated possible collinearity between the ADS and consequence scale scores, both were retained because conceptually the sets have only partial overlap. It was decided, however, to perform the multiple regressions using a step-wise backward selection procedure because the presence of collinearity would have made the results of regular multiple regression analyses difficult to interpret. The regression procedure, therefore, first predicted the outcome using a full model containing all of the predictor variables. Each subsequent step removed the predictor that contributed least to the overall fit of the model, until the final model contained only variables that contributed independently and significantly to the solution. The analyses were conducted using SPSS version 6.0. The multiple Rs obtained in these analyses were significant: frequency

PORTRAYING TREATMENT OUTCOMES 653
TABLE 2 SIGNIFICANT PREDICTOR VARIABLES AS IDENTIFIED BY MULTIPLE REGRESSION
ANALYSES FOR FOUR OUTCOME VARIABLES
Predictor Variable B Beta p
Frequency of Abstinent Days Posttreatment
Higher frequency of abstinence pretreatment 240.63 .614 < 001 H~gher Alcohol Dependence Scale score 4 51 188 037 More years of education 6 20 180 049
Number of Drinks per Drinking Day Posttreatment
Higher mean drinks/drinking day pretreatment 319 404 < 001 Lower end of treatment self-efficacy score - 079 - .440 < 001 Not employed pretreatment 1 27 246 004 Older age 053 218 014 Moderanon goal at assessment 1 17 .207 017 Married pretreatment .756 181 031 Male - 759 - .172 046
Number of Drinks per Week Posttreatment
Lesser frequency of abstinence pretreatment -20 70 - 481 < 001 Older age 378 276 008 Lower end of treatment self-efficacy score - 335 - 331 < 001 Male - 5 54 - .222 021
Number of Consequences Posttreatment
Higher Alcohol Dependence Scale score 112 273 .030 Lesser frequency of abstinence pretreatment - 1 78 - 273 030
o f abs t i nen t days p o s t t r e a t m e n t , m u l t i p l e R = .76, F(5,62) = 16.89, p < .001; n u m b e r o f d r inks per d r i n k i n g day p o s t t r e a t m e n t , m u l t i p l e R = .79, F(7 ,60) = 14.70, p < .001; n u m b e r o f d r inks per week p o s t t r e a t m e n t , m u l t i p l e R = .70, F(6,61) = 9.54, p = .001; and n u m b e r o f p o s t t r e a t m e n t c o n s e q u e n c e s , m u l t i p l e R = .35, F(2,61) = 4.15, p = .021. S ign i f ican t p r ed i c to r var iab les for the fou r c r i t e r i on m e a s u r e s a p p e a r in Table 2.
Discussion of Guided Self-Change Treatment W i t h respect to G S C t r e a t m e n t , the p resen t pos i t ive results in t e rms o f im-
p rovement f r o m pre t rea tment to pos t t r ea tmen t paral le l those repor ted for o ther b r i e f o u t p a t i e n t t r e a t m e n t s used w i t h p r o b l e m dr inkers . Because a con t ro l g r o u p was n o t used, it is no t poss ib le u n e q u i v o c a l l y to a t t r i b u t e the i m p r o v e - m e n t to the G S C t r e a t m e n t . Howeve r , two s tudies o f p r o b l e m dr inke r s t ha t used wa i t ing list c o n t r o l g roups (A lden , 1978; H a r r i s & Mil ler , 1990) f o u n d Improvement only in t reated subjects. Because typical f indings for cont ro l groups have been n o i m p r o v e m e n t , it is un l ike ly tha t t he i m p r o v e m e n t o b s e r v e d in

654 S O B E L L E T A L .
this study is a function of extraneous factors such as natural recovery, or of measurement artifacts such as regression toward the mean (Kazdin, 1986).
Although both groups showed improvement, the study provided no evidence of added value for including cognitive relapse prevention procedures as part of GSC treatment for problem drinkers. In this regard, it joins the ranks of mixed results in the evaluation of relapse prevention approaches (reviewed in Rawson, Obert, McCann, & Marinelli-Casey, 1993; M. B. Sobell & Sobell, 1993a). When positive findings have occurred in relapse prevention programs, they usually included explicit skills training procedures rather than cognitive relapse prevention procedures alone as tested in the present study. One pos- sible explanation for the tack of effect in this study is that problem drinkers may already have a perspective congruent with a relapse prevention approach. That is, because their drinking typically includes many days when they con- sume just a few drinks, problem drinkers may view an excessive drinking day as unfortunate but not fateful. Although the cognitive relapse prevention com- ponent did not receive support in terms of treatment outcomes, it was incor- porated into the treatment protocol without adding additional length to the treatment. Furthermore, the therapists reported they found it slightly awk- ward and difficult to conduct treatment without reference to relapse preven- uon concepts (M. B. Sobell & Sobell).
Because the reductions in drinking found in this study are of the same general magnitude as in previous studies, an issue that must be addressed is how the GSC approach differs from other approaches. The answer lies not in differen- tial effectiveness but in appeal to clients (i.e., minimizing intrusion upon clients' lifestyles and empowering clients, rather than therapists, to take responsibility and credit for changes). As early interventions gain increasing priority in health care, an important issue in service delivery is how to devise treatments that appeal to problem drinkers. Miller et al. (1993) recently demonstrated that problem drinkers not only appear to be resistant to traditional directive and confrontational treatments versus a nonthreatening, motivational interven- tion, but that such resistance is associated with poorer outcomes. As reported elsewhere, the GSC treatment was well liked by the vast majority of subjects in this study (M. B. Sobell & Sobell, 1993, January).
As regards the role of GSC treatment as an element of the health care system, it is an early treatment approach that is likely to have appeal for self-identified problem drinkers who want to assume major responsibility for changing their behavior. Persons who do not successfully change, and those who desire a more directed approach, could be referred to treatments with other orienta- tions or to more intensive interventions. As with other health care areas, the more intensive and costly treatments would be kept in reserve for cases that do not respond to less intensive approaches, or where there are more serious treatment needs (e.g., shelter, health, vocational training). Such a tiered or stepped care approach to treatment, similar to the principles guiding provi- sion of health care for other problems (e.g., hypertension, hypercholesterol- emia), would make for a cost-effective, comprehensive, and responsive health care system that could greatly reduce the costs of alcohol problems to individ- uals and to society (M. B. Sobell & Sobell, 1993b).

PORTRAYING TREATMENT OUTCOMES 655
This traditional method of analysis thus allows at least tentative conclu- sions about the success of GSC and the need to amplify relapse reduction interventions in order to achieve additional success. It does not, however, ad- dress many of the questions that clinicians and clinical researchers might have regarding patterns of change, which can be better described graphically than statistically, as illustrated in the next section.
Results: Alternative Portrayals of Outcomes In preparing this report of a treatment trial for publication, we noted that
although traditional analyses address issues of whether statistically significant change occurs from pre- to posttreatment, or whether one treatment has a greater effect than another, they do not provide information on many aspects of outcome likely to be of interest to treatment agencies and clinicians. For example, although traditional reports may present mean values for groups of clients, they typically provide no indication of individual differences within the group. Thus, a group for which some individuals showed dramatic im- provement and a smaller number of individuals showed dramatic failure could theoretically have the same mean change score as a group where nearly all members improved somewhat. Clinically it would be useful to know whether the typical response to the treatment was likely to be either a marked improve- ment or a setback versus a smaller improvement distributed across most clients. There would also be scientific value in knowing about different patterns of outcomes because such a split outcome pattern would suggest that the overall group consisted of subgroups of good responders and poor responders. This would lead to research attempting to characterize those subgroups and, pos- sibly, to a client-treatment matching study.
In addition to leaving certain treatment outcome issues (e.g., individual differ- ences) relatively unaddressed, traditional statistical outcome analyses may also be difficult for clinicians to interpret. Although it would not be advisable to oversimplify the presentation of results, graphic portrayals of findings may facilitate readers' appreciation of how change occurs within groups of clients and for individual clients. In the remainder of this paper we present and discuss alternative ways of presenting outcome findings. These methods can be used to supplement statistical reports and to communicate the richness of an out- come data set more fully than is typically accomplished by descriptive statistics.
Yardsticks of Success
An initial example of the value of alternative portrayals of outcomes con- cerns a type of descriptive statistic often found in traditional outcome reports, the presentation of "success rates." Some experts suggest that the ability to document treatment success improves the likelihood that one will be selected for and maintained on managed health care panels (Gilson, Prince, & Mont- gomery, in press), and thus rate of success may become an important clinical as well as research entity. Calculating success rates is valued for its simplicity, but there are three notable limitations with such an approach. First, there are no consensual criteria regarding what outcome variable should be used nor the cut-off for separating successful from unsuccessful cases. Second, in the

656 SOBELL ET AL.
TABLE 3 YARDSTICKS OF SUCCESS SUCCESS RATES FOR THE PRESENT STUDY AS A FUNCTION
OF THE DEFINITION OF SUCCESS EMPLOYED
Percent of Cases Success Criterion Successful
Never > 4 Drinking Days/Week & Never > 3 Drinks/Day d'b Never > 3 Drinks/Day a'~ Never > 12 Drinks/Week a'd Never > 4 Drinking Days/Week a h Never > 17 Drinks/Week a'e Mean Drinking Days/Week ~< 4 & Mean Drinks/Drinking Day ~< 3 b Never > 21 Drinks/Week a't Mean Drinks/Drinking Day ~< 3 ~ Mean Drinks/Week ~< 12 ~
4 Drinking Days per Week b Mean Drinks/Week ~< 17 e Mean Drinks/Week ~ 21 ¢
87 116 174 24 6 29 0 30 4 39 1 42 0 60 9 66 7 75.4 82 6
a For these variables, weeks were calculated as consecuU~e 7 day blocks beginning with the day following the last treatment session b Present study
Present study, Anderson et al , 1993; Babor et al , 1987 d Addiction Research Foundation and Canadian Centre on Substance Abuse, 1993 e Hams & Miller, 1990
Anderson et al., 1993, Babor et al , 1987
a b s e n c e o f a c o n s e n s u a l s t a n d a r d , t h e p u r p o r t e d success r a t e s will ref lect t h e n a t u r e (1.e., t ype o f o u t c o m e v a r i a b l e , l e n i e n c y o r s t r i c t n e s s ) o f t h e c r i t e r i a b e i n g u s e d fo r a g iven s tudy. T h i r d , a d i c h o t o m o u s c h a r a c t e r i z a t i o n o f o u t - c o m e s conveys ve ry l i t t le i n f o r m a t i o n a b o u t w h a t c a n o t h e r w i s e be a r i ch d a t a set. M o s t i m p o r t a n t l y , u s i n g d a t a f r o m t he p r e s e n t s tudy, Table 3 i l l u s t r a t e s h o w rela t ively smal l dif ferences m cr i te r ia c a n yield m a r k e d differences in success rates .
T h e y a r d s t t c k s o f success p r e s e n t e d in Tab le 3 a re b a s e d o n g o a l c r i t e r i a p r o v i d e d to s u b j e c t s in t h e p r e s e n t s tudy, a n d o n w e e k l y c u t - o f f s t a n d a r d s t h a t have b e e n s u g g e s t e d in t he l i t e ra tu re . I n t e r m s o f q u a n t i t y a n d f r e q u e n c y o f d r i n k i n g , t he s t r i c t e s t tes t o f a d v i c e p r o v i d e d to s u b j e c t s in t he p r e s e n t s t u d y r e q u i r e d t h e m to n e v e r c o n s u m e m o r e t h a n t h r e e d r i n k s in a d a y a n d n e v e r to d r i n k o n m o r e t h a n 4 days pe r week. Al te rna t ive ly , o n e c o u l d eva lua t e genera l c o m p l i a n c e w i t h t h e r e c o m m e n d e d l imi t s by e x a m i n i n g h o w m a n y s u b j e c t s r e s t r i c t e d t h e i r average w e e k l y d r i n k i n g to n o m o r e t h a n t h r e e d r i n k s pe r d r i n k i n g day a n d n o m o r e t h a n 4 d r i n k i n g days p e r week. Also , b e c a u s e q u a n - t i t y a n d f r e q u e n c y c a n v a r y i n d e p e n d e n t l y , o n e c a n e x a m i n e t h e m as s e p a r a t e d i m e n s i o n s to e v a l u a t e s u b j e c t s ' success , as a p p e a r s in Tab le 3.
A p o p u l a r way o f e x p r e s s i n g success ra tes h a s b e e n in t e r m s o f week ly al- c o h o l c o n s u m p t i o n . Tab le 3 i n d i c a t e s h o w success ra tes c h a n g e w i t h r e l a t ive ly m i n o r c h a n g e s in t h e l imi t , a n d h o w they c h a n g e as a f u n c t i o n o f w h e t h e r

P O R T R A Y I N G T R E A T M E N T O U T C O M E S 657
100% . . . . . . . . . . . . . . . . . . . . . . . ~'" ~ " ' ~ " i . . . . . . ~ ' - - ' -
80% " / ' (/) i " I a)
O ~t~ . . . . . . . . ./..i " 80%
G,IO~ / 'If i /
"~) 40% .~ " - - pretreatment . . . . posttreatment
~ 20% )/lr
0%
0 20 40 60 80
M e a n w e e k l y s t a n d a r d d r i n k s
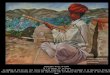
FIG. 1 Cumu]atwe frequency d]stnbunons of subjects' (n = 69) pre- and posttreatment mean number of standard dnnks consumed per week. The dotted hnes indicate improvement from pre- to posttreatment applying criteria of 12 and 40 standard drinks per week
the limit is expressed as an absolute boundary or as a mean value. For ex- ample, success can be reflected as the percentage of subjects who never ex- ceeded 12 drinks per week, or more leniently as the percentage of subjects whose average consumption did not exceed 12 drinks per week. Similarly, a cut-off value of 17 standard drinks per week could be used, as suggested by Harris and Miller (1990; 17 drinks as defined here is equivalent to 20 of Harris and Miller's standard ethanol content units). Finally, one could adopt a criterion of 21 standard drinks per week as suggested by Babor, Kranzler, and Lauerman as a limit for nonhazardous drinking (1987; see also Anderson, Cremona, Paton, Turner, & Wallace, 1993). Using these different criteria, the presenta- tion of success rates at the 12 month follow-up in Table 3 shows that rather small changes in criteria result in considerable differences in success rates. In short, the use of single criterion success rates, although convenient, requires careful attention to the specific criterion reported in order to be meaningful, and comparability among studies is limited to those that report an equivalent criterion.
An alternative to presenting a single success rate is to present a cumulative frequency distribution of clients' outcomes along various dimensions. For ex- ample, if mean weekly alcohol consumption is considered important, as with

658 SOBELL ET AL
studies referenced in Table 3, a cumulative frequency distribution of clients' outcomes along that dimension can be prepared as shown in Figure 1. Figure 1 also shows the cumulative frequency distribution for subjects' pretreatment mean weekly alcohol consumption, permitting a visual pre-posttreatment com- parison. To facilitate the presentation of results, findings for the two treat- ment conditions have been combined because there was no significant differ- ence between conditions.
An advantage of presenting frequency distributions, such as shown in Figure 1, is that this allows readers to apply whatever weekly drinks criterion they wish to evaluate success. For example, the dotted lines in Figure 1 indicate that approximately 18% of the subjects were consuming a mean of 12 or fewer drinks per week prior to treatment, whereas approximately 60% were drinking this amount or less during follow-up, more than a three-fold increase. Simi- larly, approximately 19% of the subjects were consuming more than 40 drinks per week before treatment, but only about 2% were drinking that heavily during follow-up.
Graphical presentations of outcome data can substantially enhance presen- tations of treatment outcome findings and inform readers of relationships in the data that are not apparent from statistical presentations. The shapes of the curves convey to readers how change was distributed within the group. For example, if, as in Figure I, approximately 60% of the subjects were con- suming 12 or fewer drinks per week after treatment, but most of the remaining 40% were consuming large amounts, such as 50 or more drinks per week, the frequency distribution would have an S-shape rather than the current steadily increasing curve. Such a marked difference in distributions would not be ap- parent from simply reporting a single success rate, but it could be clinically ~mportant by suggesting there was a subgroup of subjects who had little re- sponse to treatment.
Needless to say, number of drinks consumed per week is only one of several "yardsticks" of success that could be displayed in a frequency distribution format. Although distributions for other variables will not be presented here due to space considerations, visual comparison of distribution shift curves for different measures of drinking, such as percentage of days abstinent, mean drinks consumed per drinking day, and percentage of clays drinking above or below various criterion levels, would provide clinicians with a picture of how clients' drinking was most likely to change. For example, it might be found that most problem drinkers are better able to refrain from drinking entirely for a day (i.e., to reduce their frequency of drinking) than to reduce the quan- tity they consume on drinking days. Moreover, if frequency distributions were regularly presented for a standard set of outcome variables (e.g., frequency of drinking, mean drinks consumed per drinking day), this would allow meaningful comparisons of findings between studies. Lack of comparability among outcome studies has long been noted as a serious deficiency in the al- cohol treatment outcome literature (Longabaugh, 1989).
How Do Indtvldual Chents Fare Af ter Treatment?
An important matter for clinicians is how many clients actually show im- provement from pre- to posttreatment, for example in meeting a criterion of

PORTRAYING TREATMENT OUTCOMES 659
c-
"0
d "0
E
0 cO ~0 >. tO "0
E
0
I00% i @~ ~ @-- A •-- -- - - ~
l • I A ~ 8 0 % :
60% •
Improvement 4O%
Group
• RP 2O%
• • BC
0% 0% 20'% 40'% 66%0 86°1o 100%
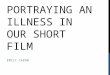
Pretreatment days consumed 0-4 drinks FIG. 2 Scatter plot showing individual subjects' (n --- 69) pre- and posttreatment mean per-
centage of days consumed 0 to 4 standard drinks for two treatment conditions. Cases to the left of the diagonal reflect ~mprovement following treatment.
consuming four or fewer drinks per day (including abstinent days). Statistical group outcome reports convey very little about what types of individual change are typical. Further, although correlational techniques can suggest the general correspondence between two or more measures, they do not communicate cer- tain features of outcomes that might be important to clinicians. For example, in statistical analyses, atypical cases, or outliers, may weaken the statistical association and may even be omitted from the analyses because they are aber- rant. From a clinical perspective, however, it can be important to know that a small proportion of cases might show a radically different response to treatment.
Distribution shift curves also convey little information about change among individual clients. However, for a given variable, change among individual clients can be illustrated using scatter plots comparing pre- and posttreatment status. For example, Figure 2 presents a scatter plot from the present study comparing the pre- and posttreatment percentage of days drinking 0 to 4 drinks for individual clients. This figure shows that on this measure only three clients (cases markedly to the right of the diagonal in Figure 2) were worse after treat- ment, with the vast majority evidencing substantial posttreatment increases. In

660 SOBELL ET AL,
100%
.~ 80%
60%
"6 40% g
20%
1 5 9 13 17 21 29 25 33 37 41 4'5 29 53 5'7 6'1 6'5 69
Cases rank ordered by percentage of days • 10 or more drinks consumed 0 to 4 drinks, posttreatment • 5 to 9 drinks
] 1 to 4 drinks
] 0 drinks
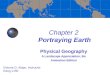
F m 3 P o s t t r e a t m e n t m d ~ l d u a l subjec t (n = 69) o u t c o m e d a t a r ank o rde red by the per-
cen tage o f da}s tha t subjec ts c o n s u m e d 0 to 4 s t a n d a r d d r inks
fact, the clumping of clients near the 100% mark posttreatment may weaken the value of statistical analyses in this case because the variance for one of the variables is highly constrained. Another facet of the outcome that would not be readily apparent from a statistical presentation, but that can be observed from Figure 2, is that many of the subjects who had relatively few abstinent or light drinking days pretreatment (e.g., from 10% to 40%) were substan- nally improved after treatment. Figure 2 also presents data by treatment con- dition, indicating that the pattern of results was similar among subjects in both conditions.
What Were Subjects" Drinking Repertowes Lzke?
Although scatter plots are useful for single variables, they cannot convey the sense of subjects' entire drinking repertoires. An important question for chnicians working with problem drinkers might be whether successful out- comes tend to consist of two distinct subgroups of individuals, some who be- come totally abstinent and some who mainly consume limited amounts of alcohol, or whether the majority of cases involve a mix of abstinent and limited drinking days. Using bars to represent each subject's posttreatment status, with drinking divided into categories (e.g., abstinent, I to 4 drinks, 5 to 9 drinks, 1> 10 drinks), individual subjects' drinking outcomes are portrayed in Figure 3. Subjects are rank ordered by their percentage of days drinking 0 to 4 drinks during the follow-up year. Figure 3 not only illustrates that most

PORTRAYING TREATMENT OUTCOMES 661
100%.
80%"
~ 80°/°. 8
Q.
~ 40%.
• 20% a.
0% 1 5 9 13 17 21 25 29 33 37 41 45 49 53 57 61 65 69
Cases in identical order as in Figure 5 [ B 10 or more drinks
5to9 drinks
] 1 to 4 drinks
] 0 drinks
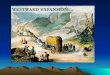
FIG. 4 Pretreatment mdiwdual subject (n = 69) data for subjects rank ordered by the per- centage of days that subjects consumed 0 to 4 standard drinks during the posttreatment year (1 e, subjects are m the same rank order as m Figure 3, but F~gure 4 displays their pretreatment data).
subjects showed a mix of light drinking and abstinent days in follow up, but also reflects the fact that light drinking constituted a substantial part of their treatment outcomes.
Were Subjects" Pretreatment Patterns o f Drinking Simdar to Their Posttreatment Patterns?
Because simultaneous presentation of pre- and posttreatment individual sub- ject data can be difficult to follow, especially when data are presented for a large number of subjects, the findings presented in Figure 3 are limited to post- treatment drinking dispositions. Clinicians might be interested, however, in how well the treatment outcomes paralleled subjects' pretreatment patterns of drinking. That is, are subjects with highly successful treatment outcomes those who already had a large number of abstinent and light drinking days in their patterns prior to treatment? Figure 4 presents a variation of Figure 3 that addresses this question. In Figure 4, instead of cases being rank ordered in terms of their pretreatment drinking, they are presented in the same order as in Figure 3. For example, case 10 in Figures 3 and 4 is the same individual, with Figure 3 presenting posttreatment data and Figure 4 presenting that same individual's pretreatment data. In this case, the subject was one of a few who were abstinent over the entire follow-up year. By comparing Figures 3 and 4, one can see that the relationship between patterns of pretreatment and post-

662
5O%
S O B E L L E T A L .
40%
0
"6
0 c 20% @
@ a. 10%
0%
F I G 5
- - p re t r ea tmen t
pos t t r ea tmen t / "
/ "
/
/
i [ i i i i i
8 7 6 5 4 3 2 1 0
N u m b e r of c o n s e q u e n c e s
Frequency dlsmbunons of subjects' (n = 69) pre- and posttreatment number of alcohol- related negative consequences reported The shaded area indicates the improvement m terms of percentage of subjects reporting zero or one consequence over follow up
t rea tment d r ink ing is not strong. H a d the re la t ionship been strong, F igure 4 would have closely resembled Figure 3 in form, a l though the overall height o f the abs t inent and l ight dr inking por t ions o f the bars would have been lower.
What Types o f Shtfts Are Seen m Drinking Consequences After Treatment?
Alternative ways of presenting outcome findings are not restricted to drinking measures. A n o t h e r var iable typica l ly repor ted m ou tcome studies involves a lcohol - re la ted consequences exper ienced pre- and pos t t rea tment . A l t h o u g h a statistical compar i son can suggest whether a reduct ion in consequences from pre- to pos t t rea tment was unl ikely to occur by chance, such a compar i son does not in fo rm cl inicians abou t whether they should expect their clients to ex- perience consequences, and, i f so, how many may remain. Figure 5 presents subjects ' pre- and pos t t r ea tmen t consequence scores as f requency d is t r ibu- nons. A l t h o u g h the figure shows tha t the curve shifts to the right, reflecting improvement , in this case the shape o f the curve also changes, reflecting a change in the relative d i s t r ibu t ion o f consequences within the sample. Dur ing the p re t rea tment interval the m o d a l number o f consequences exper ienced by subjects was a round four to five, with few subjects repor t ing only one or no consequences. In contrast, at pos t t rea tment the moda l number of consequences exper ienced was zero, with one consequence being the second mos t f requent ou tcome (the shaded area in Figure 5 indicates the increase in cases repor t ing zero or one consequence) . Figure 5 suggests that it would be reasonable for

PORTRAYING TREATMENT OUTCOMES 663
100%
O O O
D r-
£ a .
80%
60%
40%
20%
pretreatment . . . . posttreatment
"J ~ ' / f •
. J o/° •
0%
Not a Very Minor Major Very problem minor Major
Subject ive prob lem severity rating
FIG 6. Frequency dlstribuuons of subjects' (n = 68) pre- and posttreatment subjectwe ratings of their problem seventy
clinicians to expect that more than half of problem drinkers treated by GSC will experience one or no consequences during the year following treatment.
How Do Subjects Perceive Their Improvement?
Another variable that illustrates the value of distribution shift curves is sub- jects' subjective ratings of the severity of their problem. Figure 6 shows fre- quency distributions of problem severity ratings for the combined groups at pre- and posttreatment. In contrast to the frequency distribution for conse- quence scores in Figure 5, Figure 6 shows that for this variable the extent of change appears to have occurred rather evenly throughout the sample (i.e., the curve shifts to the left, but the shape is relatively unchanged). Again, al- though the earlier presented statistical comparison indicated a significant reduc- tion in perceived problem severity from pre- to posttreatment, the frequency distribution makes clear that the most likely outcome was not a full remedia- tion of the problem, but rather that individuals generally did not consider any consequences they experienced to be serious, whereas the vast majority of subjects reported that prior to treatment they had experienced one or more serious consequence of their drinking.

664
8
SOBELL ET AL.
c "
E ,~ ,
u) 0 6 "
o r - -
o- ~ 4-,, • ffl
o 1
f . . .
° I
; I
E I I
Z 0 0% 20% 40% 60'%
90 % confidence Ltrnd
RegresSio n L)ne
99% conhdence Limit
80'% 1 O0 %
Percen tage of days c o n s u m e d 5 or more dnnks, p o s t t r e a t m e n t
F]G 7 Scatter plot shorting the relauonshlp of individual subjects' (n = 64) heav:~ drinking day posttreatment and the number of consequences they experienced posttreatment The figure also ~ho~s the regression hne for the relaUonshlp and the 90% confidence limits for the hne
Did SubJects Who Drank Less Also Report Fewer Consequences?
Another aspect of individual subject outcomes that can be meaningfully examined through graphic methods is relationships between outcome dimen- sions. Figure 7 is a scatter plot showing the number of consequences subjects experienced over the follow-up year plotted against the percentage of days of heavy drinking (i.e., days when they consumed five or more drinks). What stands out in Figure 7 is that the relationship between engaging in heavy drinking and experiencing consequences is relatively weak. This conclusion is reinforced by the regression line drawn in Figure 7, which also shows the 90% confidence limits for the line. For any given value of the percentage of days subjects consumed/> 5 drinks after treatment, the corresponding point on the regression line represents the most likely number of consequences that would have occurred posttreatment. The distance between the confidence limits represents the range within which a value from the regression line would fall 90% of the time. Thus, allowing a 10% chance of error (the 95% confidence interval would have been even broader), the predicted number of consequences experienced by a person who drank >/5 drinks on 30% of the posttreatment days would range from 0 to 5, whereas the predicted range for a person who never drank /> 5 drinks posttreatment is from 0 to 4.5. In other words, one

P O R T R A Y I N G T R E A T M E N T OUTCOMES 665
would predict nearly the same amount of consequences for a person who had substantial heavy drinking days as for a person who had no heavy drinking days. This aspect of the findings would not be apparent from a correlational analysis, yet it has clinical importance because it means one cannot assume that just because a client's drinking is mostly light that the client will not en- counter drinking-related problems. In this regard, one other study has sug- gested that heaviness of drinking is not necessarily associated with conse- quences (i.e., alcohol dependence scores were lower in patients with cirrhosis than in those with precirrhotic liver disease; Wodak, Saunders, Ewusi-Mensah, Davis, & Williams, 1983). Taken together these findings suggest that the rela- tionship between consequences and drinking behavior needs further study.
Discussion The main intent of this article is to illustrate how nontraditional ways of
presenting outcome data can supplement traditional methods, provide valu- able information about the nature of outcomes, and facilitate comparisons among studies. Hypothetically, it is possible that the information conveyed in this manuscript could be more parsimoniously and appropriately commu- nicated by limiting presentations to existing statistical tools. However, it seems unlikely that available statistical methods could readily communicate the rich- ness of information contained in the graphic portrayals. Moreover, even if statistical methods could summarize the information, limiting presentations to statistics begs the following question: To whom are the findings to be com- municated, and is there a preferred way of communicating these findings?
The audience to which published clinical research is directed should include practitioners and researchers. Publication of clinical research should not only inform peers about findings, it should also serve to disseminate research. For publications to have a dissemination impact, they need to be understood by the readership. It is unreasonable to expect practitioners to be experts in ad- vanced statistical techniques. In fact, we have contended that it is the respon- sibility of clinical scientists to present issues and findings to practitioners in a manner that facilitates their understanding and assimilation of the material (L. C. Sobell, 1994). Clearly the comprehension of graphic portrayals, such as presented here, requires some thought and effort on the part o f the reader, but it does not require specialized training. Moreover, many of the graphs cap- ture in a single picture information that it would be quite complicated to ex- tract from statistical displays. It is incumbent upon authors using these tech- niques, however, to accompany the graphic presentations with sufficient linguistic interpretation to allow them to be understood by the average reader.
Predictors of outcome was the one area where we were not able to identify a method of graphical presentation of findings that would add meaningfully to the statistical presentation. However, the statistical analyses presented in Table 2 do reflect some of the subtleties of outcome analyses. In particular, the extent to which predictor variables account for variance in outcomes differs depending upon the specific outcome measure being predicted. That is, some outcomes for particular variables have varying relationships to other outcome

666 SOBELL ET AL.
variables (also see Babor et al., 1994) and to premorbid criteria. For ex- ample, ADS scores were significantly related to posttreatment consequences and posttreatment abstinent days, but not to quantitative measures of drinking, such as number of drinks per week. Lower self-efficacy scores at the end of treatment were related to quantitative measures of drinking but not to post- treatment frequency of abstinence or consequences. The fact that type of goal was only significantly related to posttreatment mean drinks per drinking day is not surprising, because subjects seeking abstinence would be expected to engage in less drinking than those seeking a reduced drinking outcome. Al- though pretreatment drinking levels tended to predict posttreatment drinking, pretreatment consequences did not significantly predict posttreatment conse- quences. Collectively, these findings demonstrate the importance of concep- tualizing treatment outcome as truly multidimensional. Such an approach has imphcatlons for research design. From a multidimensional perspectwe, it can be hypothesized that different types of patient-treatment matching might be expected to affect certain outcome dimensions more than others.
With regard to scientific communication, it is important to consider the present state of alcohol treatment research. For decades, outcome reports have been valued for the conclusions they provide about treatment effectiveness, but the field has failed to explore the richness of information that can be provided about patterns of behavior and related change over time. Jacob Cohen (1994), an eminent psychological statistician, recently asserted that before we attempt to generahze from our data, "we must seek to understand and im- prove them" (p. 1001). He also suggested that we should seek standardization of measurement, and the use of"simple, flexible, informal, and largely graphic techniques" (p. 1001) for understanding data. Although the examples provided here are not exhaustive of alternative ways of presenting findings, they exem- plify the value of supplemental data presentations for increasing our under- standing of clinical research phenomena. They also demonstrate that with some effort on the part of authors and readers, the value of treatment outcome re- search reports for clinicians can be meaningfully increased. Increased emphasis on the use of empirically based treatments as part of cost containment in the health care sector requires a greater dialogue between researchers and clini- cians, and increased accountability for research funding emphasizes the need for clinical research to have a demonstrable impact on clinical practice. This attention by researchers and clinicians to each others' needs is a foundation of behavior therapy. We hope the present paper has demonstrated that the relationship can be enhanced in our publications.
References Addiction Research Foundation and Canadian Centre on Substance Abuse (1993). Moderate
Drmkmg and Health A joint pohcy statement. Toronto Author Alden, L (1978) Evaluation ofa preventwe self-management programme for problem drinkers.
Canadtan Journal o f Behavtoural Setenee, 10, 258-263 Anderson, P, Cremona, A, Paton, A, Turner, C., & Wallace, P (1993) The risk of alcohol.
Addtctton, 88, 1493-1508 Anderson, P, & Scott, E (1992) The effect of general practmoners' advice to heavy drinking
men Brlttsh Journal o f Addlctton, 87, 891-900

PORTRAYING TREATMENT OUTCOMES 667
Anms, H M., & Graham, J. M (1988) Sttuatlonal Confidence Questtonnatre (SCO 39)." User's guide. Toronto- Addiction Research Foundation.
Anms, H M , Graham, J M., & Davis, C S (1987) Inventory o fDrmkmg Sltuattons (IDS) user's guide Toronto' Addiction Research Foundation
Annls, H M , & Peachey, J E (1992). The use of calcium carb~mlde m relapse prevention coun- sehng. Results of a randomized controlled trial Brtttsh Journal o f Addtctton, 87, 63-72.
Babor, T F, Kranzler, H. R , & Lauerman, R. J. (1987) Socml drinking as a health and psy- chosocml risk factor Anstle's hmxt revisited. In M Galanter (Ed.), Recent developments m alcohohsm Vol 5 (pp. 373-402). New York: Plenum.
Babor, T. F., Longabaugh, R., Zweben, A., Fuller, R , Stout, R , Anton, R. F , & Randall, C (1994). Issues in the definmon and measurement of drinking outcomes m alcoholism treatment research. Journal o f Studws on Alcohol, Suppl 12, 55, 101-111
Blen, T. H., Mdler, W. R., & Tonlgan, J. S. (1993). Brief interventions for alcohol problems: A review. Addtctton, 88, 315-336.
Cohen, J. (1994). The earth is round (p < .05). Amertcan Psychologist, 49, 997-1003. Cummings, C., Gordon, J. R., & Marlatt, G A. (1980). Relapse: Prevention and prediction In
W. R Mdler (Ed.), Addlcttve behavtors (pp 291-321). New York. Pergamon Press. Dies, R. R (1983). Bridging the gap between research and practice m group psychotherapy In
R R Dies & K. R. MacKenzie (Eds), Advances tn group psychotherapy: Integrating re- search and practwe (pp. 1-26) New York: International Umversmes Press.
Edwards, G., Orford, J., Egert, S , Guthrle, S., Hawker, A., Hensman, C., M~tcheson, M., Op- penheimer, E , & Taylor, C. (1977) Alcohohsm' A controlled trial of "treatment" and "ad- vice." Journal o f Studies on Alcohol, 38, 1004-1031
Foy, D. W., Nunn, L. B, & Rychtank, R. G. (1984). Broad-spectrum behavmral treatment for chromc alcoholics Effects of training controlled drinking skills. Journal o f Consulting and Chnlcal Psychology, 52, 218-230.
Gllson, M., Prince, J. E., & Montgomery, R W (m press) D~verslficatlon and consultation. Deslgmng a private group psychological pracnce m the age of health care reform Cogmtlve and Behavtoral Practwe.
Graber, R. A., & Mdler, W. R (1988). Abstinence or controlled drinking goals for problem drinkers' A randomized chmcal trml. Psychology o fAddwt tve Behavtors, 2, 20-33.
Harns , K. B., & Mdler, W. R. (1990). Behaworal self-control training for problem drinkers Com- ponents of efficacy. Psychology o f Addtcttve Behavior, 4, 82-90.
Heather, N., Klssoon-Smgh, J., & Fenton, G. W. (1990). Assisted natural recovery from alcohol problems' Effects of a self-help manual with and without supplementary telephone contact. Brtttsh Journal o f Addwtton, 85, 1177-1185
Institute of Medicine. (1990). Broadenmg the base o f treatment for alcohol problems Washington, DC National Academy Press.
Ito, R J , Donovan, D. M., & Hall, J J. (1988). Relapse prevention m alcohol aftercare: Effects on drinking outcome, change process, and aftercare attendance Brittsh Journal o f Addw- tton, 83, 171-181
Kazdln, A E (1986) Comparatwe outcome studies of psychotherapy' Methodological issues and strategies. Journal o f Consulting and Chntcal Psychology, 54, 95-105.
Kuchlpudl, V., Hobem, K., Fhckmger, A., & Iber, F L (1990). Failure of a 2-hour motlvanonal intervention to alter recurrent drinking behavior m alcoholics with gastromtestinal disease Journal o f Studies on Alcohol, 51, 356-360
Longabaugh, R (1989) Recommended research pr lonnes for the assessment of treatment out- comes Psychology o f Addtcttve Behaviors, 2, 131-141.
Marlatt, G A , & George, W. H. (1984). Relapse prevention' Introduction and overview of the model Brtttsh Journal o f Addwtton, 79, 261-273.
Miller, W. R. (1985) Motivation for treatment ' A rewew with special emphasis on alcoholism Psychologtcal Bulletm, 98, 84-107

668 SOBELL ET AL
Miller, W R (1986/87) Motivation and treatment goals. Drugs & Society, 1, 133-151 Miller, W R , Benefield, R G., & Tonlgan, J S (1993) Enhancing motivation for change in
problem drinking A controlled comparison of two therapist styles Journal of Consultmg and Chmcal P~ychology, 61, 455-461
Miller, W. R., & Rollnlck, S (1991) Motivational mtervtewmg Preparing people to change ad- dwtlve behavior New York Guilford Press
Moos, R H , & Flnney, J. W (1985) New directions in program evaluation Implications for expanding the role of alcoholism researchers. In B McCrady, N. Noel, & T D Nlrenberg (Eds), Future directions m alcohol abuse treatment research, (pp. 173-203) Washington, DC " U S Government Printing Office
Rawson, R A , Obert, J E , McCann, M. J., & Marmelh-Casey, P. (1993) Relapse prevention strategies m outpatient substance abuse treatment Psychology of Addictive Behavtom, 7, 85-96
Sanchez-Crmg, M (1986) How much is too much '~ Estimates of hazardous drinking based on clients' self-reports British Journal of Addwtlon, 81, 251-256.
Sanchez-Cralg, M , Anms, H M , Bornet, A R., & MacDonald, K R (1984) Random assign- ment to abstinence and controlled drinking' Evaluation of a cognitive-behavioral program for problem drinkers Journal of Consulting and Chmcal Psychology, 52, 390-403
Sanchez-Cralg, M , Lelgh, G., Spivak, K , & Lel, H (1989) Superior outcome of females over males after brief treatment for the reduction of heav'y drinking Brmsh Journal of Addic- tion, 84, 395-404
Sanchez-Cralg, M , Splvak, K , & Davlla, R (199l) Superior outcome of females o'~er males after brief treatment for the reduction of heavy drinking Replication and report of ther- apist effects Brmsh Journal o f Addiction, 86, 867-876
Skinner, H, A , & Allen, B A (1982). Alcohol dependence syndrome" Measurement and ~ahda- tlon Journal of Abnormal Psychology, 91, 199-209
Sobell, L C (1994, November) BrMgmg the gap between sctence and chmcal practtce. The chal- lenge before us Presentation at the 28th Annual Meeting of the Association for Advance- ment of Behavior Therapy, San Diego, CA.
Sobell, L C , & Sobell, M B. (1992) Tlmellne follow-back' A technique for assessing self-reported alcohol consumpUon. In R Z Lltten & J Allen (Eds), Measuring alcohol consumption Psychosoctal and blologtcal methods (pp 41-72). New Jersey: H u m a n a Press.
Sobell, L C , Sobell, M B, Riley, D M , Klajner, F , Leo, G. 1, Pavan, D, & Cancflla, A (1986) Effect of television programming and advemsmg on alcohol consumption m normal drinkers Journal o f Studies on Alcohol, 47, 333-340.
Sobell, M B, Malsto, S A , Sobell, L C , Cooper, A. M , Cooper, T, & Sanders, B. (1980) De,,elopmg a prototype for evaluating alcohol treatment effectiveness. In L C Sobell, M B Sobell, & E Ward (Eds), Evaluating alcohol and drug abuse treatment effecttveness. Recent advances (pp 129-150). New York" Pergamon Press
Sobell, M B, & Sobell, L. C (1993a) Problem drmkers" GuMed self-change treatment New York Guilford Press.
Sobell, M B, & Sobell, L C. (1993b) Treatment for problem drinkers A public health priority In J S Baer, G. A Marlatt, & R. J. McMahon (Eds.), Addictive behaviors across the hfespan. Prevention, treatment, andpohcy issues (pp 138-157) Beverly Hills, CA Sage Press
Sobell, M B., & Sobell, L C. (1993, January) Chents'and therapists'perceptions o fa motlva- Uonalmterventtonforproblem drinkers Poster session presented at the Sixth International Conference on Treatment of Addictive Behaviors, Santa Fe, NM
Sobell, M B, Wilkinson, D A., & Sobell, L C. (1990). Alcohol and drug problems In A. S Bellack, M Hersen, & A. E. Kazdin (Eds), International handbook ofbehavror modification and therapy (2nd ed) (pp. 415-435). New York Plenum Press.

PORTRAYING TREATMENT OUTCOMES 669
Taylor, C., Brown, D., Duckltt, A , Edwards, G., Oppenheimer, E , & Sheehan, M (1985). Pat- terns of outcome' Drinking histories over ten years among a group of alcohohcs. Brmsh Journal o f Addtctlon, 80, 45-50.
Wmer, B. J. (1971). Stat~stlcalprmctples m expertmentaldestgn (2nded) New York McGraw-Hall Wodak, A. D., Saunders, J. B, Ewusl-Mensah, I , Davis, M , & Wflhams, R. (1983). Seventy
of alcohol dependence in patients with alcoholic hver disease Brmsh Medtcal Journal, 287, 1420-1422.
RECEIVED" December 23, 1994 ACCEPTED May 15, 1995