Embed Size (px)
Citation preview
PC
S
PgFvnaoctimoteiavdep
©3
T
olyoma Virus-Associated Nephropathy and Concurrentytomegalovirus Infection in the Kidney Transplant Recipients
.B. Park, J.H. Kwak, K.T. Lee, E.A. Hwang, S.Y. Han, H.T. Kim, W.H. Cho, M.S. Choi, and H.C. Kim
ABSTRACT
Introduction. Cytomegalovirus (CMV) and polyoma virus BK (BKV) may both establishlatency following primary infection. Frequent reactivation of these viruses can occur in thekidney transplant recipients. BKV may induce CMV gene expression by stimulatingcellular regulator proteins or by its own gene regulator proteins. A high rate of concurrentCMV infections has been noted in kidney transplant recipients with polyoma virus-associated nephropathy (PVAN).Methods. PVAN was identified in 10 of 191 patients who received kidney transplantsbetween October 1998 and September 2003. PVAN was confirmed by allograft kidneybiopsy. Four of the 10 patients were complicated by concurrent CMV infection.Results. Two patients had only serological evidence of CMV infection and one patienthad CMV gastritis. These three patients were treated with intravenous ganciclovir withgood results. Disseminated ganciclovir-resistant CMV disease was demonstrated in theremaining patient. This 34-year-old kidney transplant recipient with PVAN died ofmultiorgan failure despite antiviral therapy with both ganciclovir and foscarnet.Conclusion. PVAN with concurrent CMV infection in kidney transplant recipientsshowed variable clinical courses including mortality. Further studies are needed to
elucidate the influence of PVAN on the pathogenesis of CMV infection.P
WmSriTctcmpi
KPK
o1
OLYOMA VIRUS-ASSOCIATED NEPHROPATHY(PVAN) has emerged as an important cause of allo-
raft dysfunction and loss in kidney transplant recipients.ollowing primary infection in early childhood, polyomairus preferentially establishes latency within the genitouri-ary tract. The setting of immunosuppression may stimulatesymptomatic viral reactivation of latent infection in solidrgan transplant recipients. Cytomegalovirus (CMV) isapable of establishing lifelong persistent infection. Reac-ivation of CMV infection is an important cause of diseasen solid organ transplant recipients. Coinfection of two or
ore viruses may occur in humans. Recently, coinfectionf polyoma virus and CMV has been reported in kidneyransplant recipients. Polyoma virus may induce CMV genexpression by stimulating cellular regulator proteins or byts own gene regulator proteins.1 However, a significantssociation or direct relationship to reactivation of theseiruses in kidney transplant recipients is not yet wellocumented. In this study, we reviewed our clinical experi-nce with four kidney transplant patients who had biopsy-
roven PVAN with concurrent CMV infections. d2006 by Elsevier Inc. All rights reserved.60 Park Avenue South, New York, NY 10010-1710
ransplantation Proceedings, 38, 2059–2061 (2006)
ATIENTS AND METHODS
e included 191 patients whose graft functioned more than 6onths after kidney transplantation between October 1998 and
eptember 2003. PVAN was identified in 10 of 191 patients whoeceived kidney transplants. Four patients had concurrent CMVnfections among the 10 kidney transplant recipients with PVAN.he diagnosis of PVAN was based on the presence of the viralytopathic effects in the urine cytology specimen (decoy cells) andhe characteristic intranuclear inclusion in renal tubular epithelialells identified in the allograft kidney biopsy. In addition, electronicroscopy and detection of polyoma virus DNA in plasma were
erformed for PVAN diagnosis. The presence of concurrent CMVnfection was confirmed on polymerase chain reaction (PCR)
From the Departments of Internal Medicine (S.B.P., J.H.K.,.T.L., E.A.H., S.Y.H., H.C.K.), Surgery (H.T.K., W.H.C.), andathology (M.S.C.), Keimyung University School of Medicine,eimyung University Kidney Institute, Daegu, Korea.Address reprint requests to Dr Sung Bae Park, Department
f Internal Medicine, Keimyung University School of Medicine,94 Dong San Dong, Daegu, 700-712, Korea. E-mail: sbpark@
smc.or.kr0041-1345/06/$–see front matterdoi:10.1016/j.transproceed.2006.06.107
2059
a(
R
Fitfpmaa
iPiCygrtokbh
svawwggmm
D
CiolttmoSbtd
i
AGDONHDRIBTFS
nor; Cm
1234
c
2060 PARK, KWAK, LEE ET AL
nalysis of CMV DNA, serology for CMV immunoglobulin MIgM), and immunohistochemical analysis of tissue biopsies.
ESULTS
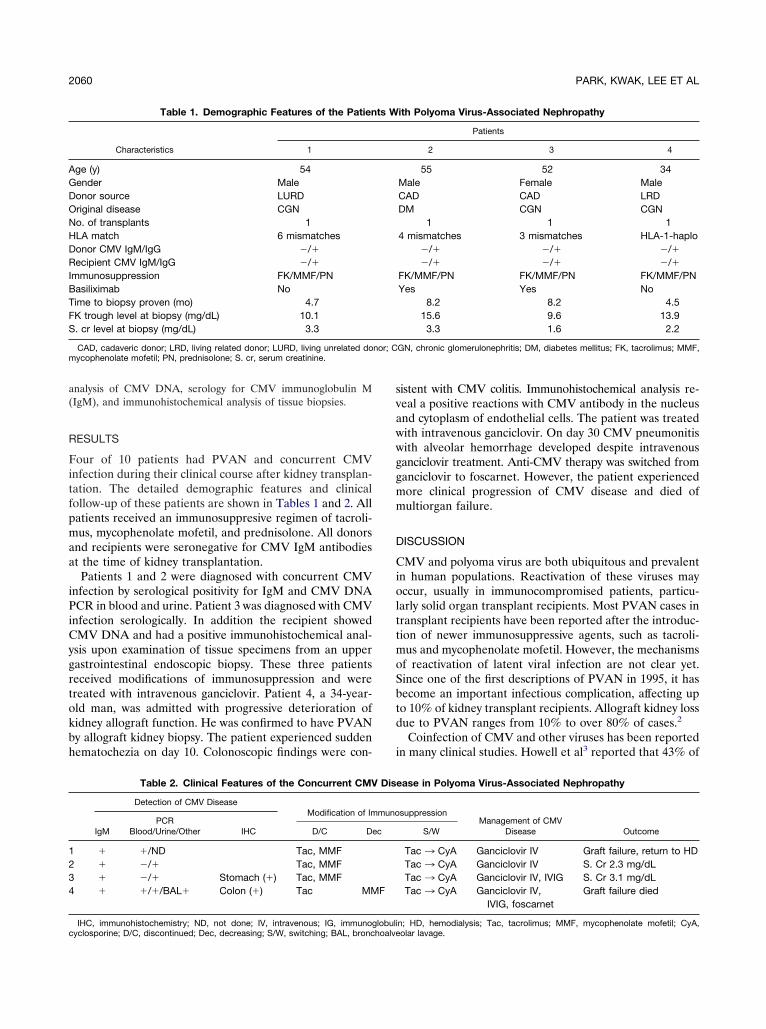
our of 10 patients had PVAN and concurrent CMVnfection during their clinical course after kidney transplan-ation. The detailed demographic features and clinicalollow-up of these patients are shown in Tables 1 and 2. Allatients received an immunosuppresive regimen of tacroli-us, mycophenolate mofetil, and prednisolone. All donors
nd recipients were seronegative for CMV IgM antibodiest the time of kidney transplantation.
Patients 1 and 2 were diagnosed with concurrent CMVnfection by serological positivity for IgM and CMV DNACR in blood and urine. Patient 3 was diagnosed with CMV
nfection serologically. In addition the recipient showedMV DNA and had a positive immunohistochemical anal-
sis upon examination of tissue specimens from an upperastrointestinal endoscopic biopsy. These three patientseceived modifications of immunosuppression and werereated with intravenous ganciclovir. Patient 4, a 34-year-ld man, was admitted with progressive deterioration ofidney allograft function. He was confirmed to have PVANy allograft kidney biopsy. The patient experienced suddenematochezia on day 10. Colonoscopic findings were con-
Table 1. Demographic Features of the Patien
Characteristics 1
ge (y) 54ender Maleonor source LURDriginal disease CGNo. of transplants 1LA match 6 mismatchesonor CMV IgM/IgG �/�ecipient CMV IgM/IgG �/�
mmunosuppression FK/MMF/PNasiliximab Noime to biopsy proven (mo) 4.7K trough level at biopsy (mg/dL) 10.1. cr level at biopsy (mg/dL) 3.3
CAD, cadaveric donor; LRD, living related donor; LURD, living unrelated doycophenolate mofetil; PN, prednisolone; S. cr, serum creatinine.
Table 2. Clinical Features of the Concurrent CMV
Detection of CMV DiseaseModification of Im
IgMPCR
Blood/Urine/Other IHC D/C D
� �/ND Tac, MMF� �/� Tac, MMF� �/� Stomach (�) Tac, MMF� �/�/BAL� Colon (�) Tac MM
IHC, immunohistochemistry; ND, not done; IV, intravenous; IG, immunoglobuliyclosporine; D/C, discontinued; Dec, decreasing; S/W, switching; BAL, bronchoalve
istent with CMV colitis. Immunohistochemical analysis re-eal a positive reactions with CMV antibody in the nucleusnd cytoplasm of endothelial cells. The patient was treatedith intravenous ganciclovir. On day 30 CMV pneumonitisith alveolar hemorrhage developed despite intravenousanciclovir treatment. Anti-CMV therapy was switched fromanciclovir to foscarnet. However, the patient experiencedore clinical progression of CMV disease and died ofultiorgan failure.
ISCUSSION
MV and polyoma virus are both ubiquitous and prevalentn human populations. Reactivation of these viruses mayccur, usually in immunocompromised patients, particu-
arly solid organ transplant recipients. Most PVAN cases inransplant recipients have been reported after the introduc-ion of newer immunosuppressive agents, such as tacroli-us and mycophenolate mofetil. However, the mechanisms
f reactivation of latent viral infection are not clear yet.ince one of the first descriptions of PVAN in 1995, it hasecome an important infectious complication, affecting upo 10% of kidney transplant recipients. Allograft kidney lossue to PVAN ranges from 10% to over 80% of cases.2
Coinfection of CMV and other viruses has been reportedn many clinical studies. Howell et al3 reported that 43% of
ith Polyoma Virus-Associated Nephropathy
Patients
2 3 4
55 52 34Male Female MaleCAD CAD LRDDM CGN CGN
1 1 14 mismatches 3 mismatches HLA-1-haplo
�/� �/� �/��/� �/� �/�
FK/MMF/PN FK/MMF/PN FK/MMF/PNYes Yes No
8.2 8.2 4.515.6 9.6 13.93.3 1.6 2.2
GN, chronic glomerulonephritis; DM, diabetes mellitus; FK, tacrolimus; MMF,
ase in Polyoma Virus-Associated Nephropathy
suppressionManagement of CMV
Disease OutcomeS/W
Tac ¡ CyA Ganciclovir IV Graft failure, return to HDTac ¡ CyA Ganciclovir IV S. Cr 2.3 mg/dLTac ¡ CyA Ganciclovir IV, IVIG S. Cr 3.1 mg/dLTac ¡ CyA Ganciclovir IV,
IVIG, foscarnetGraft failure died
ts W
Dise
muno
ec
F
n; HD, hemodialysis; Tac, tacrolimus; MMF, mycophenolate mofetil; CyA,olar lavage.

PwttivtapciBw
upcahainva
cpba
baptrc
iaetcng
R
pc
vn
mt
pe
POLYOMA VIRUS AND CYTOMEGALOVIRUS 2061
VAN patients showed intercurrent systemic infectionsith CMV among kidney transplant recipients who were all
reated with ganciclovir. Among them, two-thirds of pa-ients were diagnosed on esophageal or gastric biopsy spec-mens. Toyoda et al4 reported that plasma polyoma BKirus (BKV) positivity was highly associated with coinfec-ion with CMV in kidney transplant recipients showingllograft dysfunction. Of 12 patients who were BKV PCR-ositive in plasma, 6 (50%) showed CMV PCR positivity. Inomparison, the incidence of Epstein-Barr virus PCR pos-tivity was 8.3% in plasma of same patient group. PlasmaKV positivity preceded detection of CMV, or both virusesere concurrently detected in most patients.The involvement of PVAN in reactivation of CMV is
ncertain. Hirsch et al5 reported that 40% of kidney trans-lant recipients with PVAN had both CMV and BKV repli-ation. However, there was no correlation in the statisticalnalysis. Kristoffersen et al1 demonstrated that BKV en-anced the expression of CMV immediate early (IE1 and 2)s well as the early protein pp65 during double infectionsn semipermissive cells. It was established that the phe-omenon is due to heterologous transcriptional transacti-ation of the CMV major IE promoter by the BKV large Tntigen.
In our series, four patients experienced PVAN compli-ated by concurrent CMV infection within the first yearosttransplantation. All patients were diagnosed on theasis of serology and CMV DNA determination. Addition-
lly, two patients were diagnosed with gastric or colonicsr
iopsy specimens. All patients were treated with ganciclovirnd modification of immunosuppression. The majority ofatients had favorable clinical courses with ganciclovirherapy. A patient developed a disseminated, ganciclovir-esistant, CMV disease and deteriorated in a fatal clinicalourse.
In summary, we observed PVAN with concurrent CMVnfection in kidney transplant recipients who showed vari-ble clinical courses including mortality. Transplant recipi-nts with PVAN seem to show a high rate of CMV reactiva-ion. Kidney transplant recipients with PVAN should belosely monitored for CMV infection. Further studies areeeded to elucidate the influence of PVAN on the patho-enesis of CMV infections.
EFERENCES
1. Kristoffersen AK, Johnsen JI, Seternes OM, et al: The humanolyomavirus BK T antigen induces gene expression in humanytomegalovirus. Virus Research 52:61, 1997
2. Hirsch HH, Brennan DC, Drachenberg CB, et al: Polyoma-irus-associated nephropathy in renal transplantation: interdiscipli-ary analysis and recomendations. Transplantation 79:1277, 20053. Howell DN, Smith SR, Butterly DW, et al: Diagnosis andanagement of BK polyomavirus interstitial nephritis in renal
ransplant recipients. Transplantation 68:1279, 19994. Toyoda M, Puliyanda DP, Amet N, et al: Co-infection of
olyomavirus-BK and cytomegalovirus in renal transplant recipi-nts. Transplantation 80:198, 2005
5. Hirsch HH, Knowles W, Dickenmann M, et al: Prospective
tudy of polyomavirus type BK replication and nephropathy inenal-transplant recipients. N Engl J Med 347:488, 2002