Embed Size (px)
Citation preview

Translational Science
Poly (ADP) Ribose Glycohydrolase Can BeEffectively Targeted in Pancreatic CancerAditi Jain1,2, Lebaron C. Agostini1,2, Grace A. McCarthy1,2, Saswati N. Chand2,AnnJosette Ramirez1,2, Avinoam Nevler1,2, Joseph Cozzitorto1,2,ChristopherW. Schultz1,2, Cinthya Yabar Lowder1,2, KateM. Smith3, Ian D.Waddell3,Maria Raitses-Gurevich4, Chani Stossel4,5, Yulia Glick Gorman4, Dikla Atias4,Charles J. Yeo1,2, Jordan M.Winter6, Kenneth P. Olive7, Talia Golan4,5,Michael J. Pishvaian8, Donald Ogilvie3, Dominic I. James3, Allan M. Jordan3, andJonathan R. Brody1,2
Abstract
Patients with metastatic pancreatic ductal adenocarcinoma(PDAC) have an average survival of less than 1 year, under-scoring the importance of evaluating novel targets withmatched targeted agents. We recently identified that poly(ADP) ribose glycohydrolase (PARG) is a strong candidatetarget due to its dependence on the pro-oncogenic mRNAstability factor HuR (ELAVL1). Here, we evaluated PARG as atarget in PDAC models using both genetic silencing of PARGand established small-molecule PARG inhibitors (PARGi),PDDX-01/04. Homologous repair–deficient cells comparedwith homologous repair–proficient cells were more sensitiveto PARGi in vitro. In vivo, silencing of PARG significantly
decreased tumor growth. PARGi synergized with DNA-damaging agents (i.e., oxaliplatin and 5-fluorouracil), but notwith PARPi therapy. Mechanistically, combined PARGi andoxaliplatin treatment led to persistence of detrimental PAR-ylation, increased expression of cleaved caspase-3, andincreased gH2AX foci. In summary, these data validate PARGas a relevant target in PDAC and establish current therapiesthat synergize with PARGi.
Significance: PARG is a potential target in pancreatic canceras a single-agent anticancer therapy or in combination withcurrent standard of care.
IntroductionPancreatic ductal adenocarcinoma (PDAC) is estimated to
become the second leading cause of cancer-related death in theUnited States, with a 5-year survival rate of only 9% (1, 2).Despiterecent advancements in treatment options for PDAC, the prog-nosis remains poor. In 2008, global genomic analyses on human
pancreatic cancers revealed 12 core signaling pathways that werealtered in the majority of PDAC (3–5), and subsequent sequenc-ing studies have supported and expanded upon these initialfindings (6, 7). Initial results from the "Know Your TumorInitiative" for patients with PDAC, as well as several relatedpublications (5–8), have identified certain patient populationswith 27% highly actionable mutations. Actionable mutationscommonly found were in DNA repair genes (BRCA1/2 or ATM;8.4%) and cell-cycle genes (CCND1/2/3 or CDK4/6; 8.1%;refs. 6, 7). Germline or sporadic mutations in homologousrecombination genes found in PDAC and several other cancerscompromise repair of damaged DNA, most likely helping tofacilitate tumorigenesis (8–11). Selectively targeting alternativeDNA repair pathways in such tumors provides a putative "per-sonalized" therapeutic strategy via a synthetic lethalapproach (12, 13).
In patients carrying germline or somatic defects in homolo-gous-repair (HR) genes, DNA repair is heavily dependent onPARPs (e.g., PARP1; refs. 7, 11). Hence, these tumors are highlysusceptible to PARP inhibitors (PARPi; refs. 13–15). Recent dataare also emerging with the use of PARPi in the treatment ofPDAC (16–20). Many clinical trials are ongoing for locallyadvanced or metastatic PDAC, either with single-agent PARPi(olaparib, veliparib, talazoparib, rucaparib) or in combinationwith standard chemotherapy, including gemcitabine, FOLFIRI-NOX, and cisplatin (16–20). A recent dose-escalation, phase I trialwith talazoparib as a single agent confirmed responses in patientswith PDAC (21). Three PARPi are approved for patients withmetastatic breast and ovarian cancer, and are being used routinely
1The Jefferson Pancreas, Biliary and Related Cancer Center, Department ofSurgery, Thomas Jefferson University, Philadelphia, Pennsylvania. 2Sidney Kim-mel Cancer Center, Thomas Jefferson University, Philadelphia, Pennsylvania.3Drug Discovery Unit, Cancer Research UK Manchester Institute, The Universityof Manchester, Manchester, United Kingdom. 4Oncology Institute, Chaim ShebaMedical Center, Tel Aviv University, Tel Aviv, Israel. 5Sackler Faculty of Medicine,Tel Aviv University, Tel Aviv, Israel. 6Surgical Oncology, University HospitalsCleveland Medical Center, Cleveland, Ohio. 7Department of Medicine andHerbert Irving Comprehensive Cancer Center, Columbia University Irving Med-ical Center, New York, New York. 8Department of Gastrointestinal MedicalOncology, TheUniversity of Texas,MDAndersonCancerCenter, Houston, Texas.
Note: Supplementary data for this article are available at Cancer ResearchOnline (http://cancerres.aacrjournals.org/).
L.C. Agostini and G.A. McCarthy contributed equally as second authors of thisarticle.
Corresponding Author: Jonathan R. Brody, Thomas Jefferson University, 1015Walnut Street, Curtis 618, Philadelphia, PA 19107. Phone: 215-955-2693; Fax: 215-923-6609; E-mail: [email protected]
Cancer Res 2019;79:4491–502
doi: 10.1158/0008-5472.CAN-18-3645
�2019 American Association for Cancer Research.
CancerResearch
www.aacrjournals.org 4491
on October 3, 2020. © 2019 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 4, 2019; DOI: 10.1158/0008-5472.CAN-18-3645

as standard of care (22, 23). However, while PARPi can be veryeffective, resistance to PARPi is an evolving concern (24–26). Inaddition, it is becoming increasingly apparent that not all tumorsthat share phenotypic features of BRCA1/2–mutant tumors(BRCAness) respond to PARPi therapies. Besides conventionalresistance mechanisms (26), recent studies from our groupshowed that PDAC cells develop resistance to DNA-damagingagents through post-transcriptional upregulation of WEE1 andpoly (ADP-ribose) glycohydrolase (PARG), mediated by the pro-oncogenic, RNA-binding protein, HuR (27, 28).
While WEE1 has been explored as a target in PDAC by us andothers (27, 29), PARG has been explored by others as a target incolon cancers, lung cancers, and acutemyeloid leukemia (30–32).PARG is an enzyme that breaks down poly (ADP-ribose) (PAR)chains for a number of different cellular processes including thefollowing: release and recycling of repair proteins, break repairresolution, and replication fork progression. PAR chains areadded by the PARP enzymes as covalentmodifications to acceptorproteins, primarily in response to DNA damage by PARP1 andPARP2 (33, 34). This reversible post-translational modification iscritical for signaling and recruitment of repair factors, and hastypically been targeted via PARPi to prevent or weaken the DNAdamage response (28, 33–35). Other studies have demonstratedthat inhibiting PARG could: (i) sensitize cells to radiation (36);(ii) slow down DNA repair and cause mitotic abnormalities (37);and (iii) synergize with silencing of BRCA1, BRCA2, PALB2,FAM175A (ABRAXAS), and BARD1 genes to increase DNA dam-age and stall replication forks (38, 39). Finally, we recentlyshowed that the pro-oncogenic factor, HuR, upregulates PARGin a cancer-specificmanner (28), providing a strong rationale (i.e.,a therapeutic window) to explore targeting PARG in PDAC cells.Thus, we hypothesized that targeting PARG could provide analternative and complementary therapeutic strategy to treatingPDAC (38, 40). To date, no one has explored targeting PARG inboth homologous repair–deficient and -proficient (HR-D andHR-P) PDAC cells due to a lack of available specific and potentPARGi. Herein, we evaluate for the first time targeting PARG,through both genetic silencing and small-molecule inhibi-tors (38, 41, 42) in preclinical models of PDAC.
Materials and MethodsCell lines
HR-P: MIA PaCa-2, PANC-1, and HR-D: Hs 766T PDAC cellswere obtained from ATCC. Normal HPNE cells were purchasedfrom ATCC. DLD1.BRCA2 and RKO.FANCC isogenic colorectalcell lines were a generous gift from Dr. Scott Kern (JohnsHopkins University School of Medicine, Baltimore, MD) andwere generated by targeted disruption of either BRCA2 orFANCC (Fanconi Anemia pathway) DNA repair genes byhomologous recombination and provide excellent cancermodels for studying drug sensitivity in a HR-deficient back-ground (43, 44). PDAC PDX–derived cells were obtained fromDr. Golan (Tel Aviv University, Tel Aviv, Israel; SupplementaryTable S1A; ref. 45). These cells were derived from pancreaticascites or pleural effusion cancer cells from patients with PDACand represent clinically relevant models to study PARG as atarget because many of these models recapitulate metastaticPDAC, and have been characterized for BRCA1/2 mutationsand KRAS status. KPC BRCA2 wild-type (WT) and BRCA2 nullcell lines were a kind gift from Dr. Kenneth P. Olive (Columbia
University, New York, NY; refs. 46, 47). PDX cell lines werecultured in RPMI in a humidified incubator at 37�C and 5%CO2,as recommended. All other cell lines were cultured in DMEMmedium supplemented with 10% FBS, 1% L-glutamine, and 1%penicillin–streptomycin. All cell lines were short-tandem repeat–authenticated, and were Mycoplasma-tested monthly, using PCR-based Mycoplasma Detection Kit (# MP0035, Sigma Aldrich).We also evaluated cell lines for maintenance of a definingoncogenic driving mutation (i.e., Kras). Cells were passaged atleast twice after thawing before experimental use.
Generation of doxycycline-inducible shPARGThepCW-shPARGplasmidwas prepared usingGibson cloning:
A pCW-cas9 tetracycline inducible plasmid (# 50661, Addgene)was enzyme-digested with NheI and BamHI (New England Bio-Labs) as per the manufacturers' specifications and run through a0.75% agarose gel for subsequent purification with the QIAquickGel Extraction Kit (Qiagen) to extract the TET-inducible pCWvector backbone. An shPARG insert flanked by BamHI enzymerestriction sites and an upstream NheI restriction site was pur-chased from IDT, PCR amplified using designed cloning primers(forward primer: 50-cagatcgcctggagaattggGGATCCGCTAGCGC-CACC-30 (17), reverse primer: 50-aaggcgcaaccccaaccccgGGATCC-CAAAAAGCGATCTTAGGAAAC-30) and gel-purified as detailedpreviously. The insert was then Gibson-cloned into the vectorusing the NEBuilder HiFi DNA Assembly Cloning Kit (# E5520S,New England BioLabs) at a vector and insert count of 0.05picomols and 0.12 picomols, respectively. The newly formedplasmid was used to transform NEB 5-alpha–competent cells(# C2988J, New England BioLabs). After a 24-hour incubationat 37�C, individual clones were then selected, cultured, andsequenced for validation using sequencing primers (primer 1:50-GGGCTGCCTTGGAAAAG-30, primer 2: 50-CAGATCGCCTG-GAGAATTG-30).
Lentivirus production and generation of shPARG cell linesA commercially available unique 29mer shRNA construct
against human PARG in a lentiviral GFP vector (# TL310610,Origene) was packaged in HEK 293T cells using a LentiviralPackaging Kit (# TR30037, Origene). MIA PaCa-2 and PANC-1cellswere infectedwithvirusparticleswith theadditionof1mg/mLPolybrene (# TR-1003-G, Sigma Aldrich). Cells were then puro-mycin (# P8833, Sigma Aldrich) -selected and validated for PARGmRNA and protein knockdown.
Modified siRNA for transient knockdownMIA PaCa-2 and PANC cells were transfected with custom-
mademodified control and PARG siRNA oligonucleotides (Geni-sphere LLC; PARG sense 50-UACCAGAGCAGUUUAGUAA-30).Transfections with unmodified ON-TARGET plus NontargetingControl siRNA (GE Dharmacon, #D-001810-01-05) andON-TARGET plus PARG siRNA (GE Dharmacon, # LU-011488-00-0002) were used as controls. All transfections were performedusing 30 nmol/L of oligonucleotides and Lipofectamine 2000(Life Technologies, #11668) according to the manufacturer'sinstructions.
Drugs and inhibitorsOlaparib (PARPi #S1060) and oxaliplatin (# S1224) were
obtained from Selleck Chemicals. 5-Fluorouracil (5-FU)(# F6627) was obtained from Sigma Aldrich. Cell active
Jain et al.
Cancer Res; 79(17) September 1, 2019 Cancer Research4492
on October 3, 2020. © 2019 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 4, 2019; DOI: 10.1158/0008-5472.CAN-18-3645

small-molecule PARG inhibitors PDDX-001/PDD00017273(hereafter referred to as PDDX-01) and PDDX-02/PDD00017238(hereafter referred to as PDDX-02) were synthesized as describedpreviously (42, 48) and were utilized because they have beenreported to demonstrate robust pharmacology against PARGwithgreat potency and specificity, as compared with other knowninhibitors of PARG. PDDX-004/PDD00017272 (hereafterreferred to as PDDX-04) was synthesized in collaboration withDr. Joseph Salvino from The Wistar Institute (Philadelphia, PA)and this compound has the exact quinazolinedione core asPDDX-01 as published before (42). Compounds were either resus-pended in DMSO or water to stock concentrations of 10 mmol/L.
Cell survival and combination analysesA total of 800 cells/well were plated in 96-well plates in 100 mL
of cell culture medium, and treated with drugs after 24 hoursat indicated concentrations. Percentage cell survival relative tocontrol treatments was assessed after 5 days, by staining cellswith Quant-iT Pico Green Reagent (#P7581, Life Technologies)for 1 hour and measuring fluorescence using a fluorescencemicroplate reader (excitation�480nm, emission�520nm) (49).IC50 values were determined through nonlinear regressionanalysis.
Cell survival for siDDR experiments was analyzed by MTTassay. A total of 1,000 cells/well were plated in 96-well plates in100 mL of cell culture medium, and treated with drugs after24 hours at indicated concentrations. After 5 days, MTT reagent(5 mg/mL in 1�PBS) was added to each well and plates wereincubated for 4 hours at 37�C. Following incubation, media wasremoved and purple formazan crystals were dissolved in DMSO(100mL). Absorbancewas read at 570 nmand results were plottedas percentage relative survival.
Combination analyses were performed by plating cells in 96-well plates at 1,000 cells/well. After 24 hours, cells were treatedwith PDDX-01 (dose range, 1.5 mmol/L–25 mmol/L) and eitherolaparib (dose range, 1.5 mmol/L–25 mmol/L), oxaliplatin(dose range, 0.03 mmol/L–1 mmol/L), or 5-FU (dose range,0.75 mmol/L–25 mmol/L) in a 5 � 5 or 5 � 6 matrix. Eachtreatment was done in triplicate wells. Cells were treated for5 days, and percentage cell survival relative to control treatmentswas assessed by staining cells with Quant-iT Pico Green Reagent.Each experiment was done at least three times. After Pico Greenanalysis, synergistic/antagonistic/additive combinations wereanalyzed by using Combenefit software, which provides synergydistribution plots by comparing experimental data to mathemat-ical models (e.g., bliss model) of dose responses for additive/independent combinations (50). In brief, the software first readseach experimental dose response as a matrix of percentage of thecontrol and each single-agent effect is fitted with a dose–responsecurve. Bliss Independence model then compares experimentalcombination dose–response surface to the model-generated doseresponse, resulting in a synergy distribution plot. The Bliss Inde-pendence model calculates the expected effect of two drugs asfollows:EffectAþB ¼ EffectAþEffectB � ðEffectA � EffectBÞwhere Aand B represent two different drugs (51). If the actual effect isgreater than that calculated with the Bliss Independence model,this implies synergism ¼ indicates additivity, and less thanindicates antagonism. Combenefit determines synergy as thechange in efficacy of a combination of drugs as compared withexpected. So, for instance, if two drugs through the Blissmodel areexpected to kill 50% of cells but instead kill 75, this would be a
synergy score of 50 as at this combination there is a 50% increasein the expected effectiveness of the combination. Drug matrixheatmap 5� 5 or 5� 6 grid illustrating bliss index and percentageinhibition are shown for n ¼ 3.
Colony formation analysesLong-term colony formation assays were performed as
described previously (52) and colonies were counted using ImageJ software.
qRT-PCR and mRNA expression analysesTotal RNA was extracted using the RNeasy Mini Kit (Qiagen).
cDNA was made using 1,000 mg total RNA using Applied Biosys-tems High Capacity cDNA Reverse Transcriptase Kit (Life Tech-nologies) and qPCR (qRT-PCR) was performed as describedpreviously (49). Relative quantification was performed using the2-DDCt method.
Immunoblot analysesCells were lysed in ice cold RIPA Buffer (#sc-24948A, Santa
Cruz Biotechnology Inc.) supplemented with fresh proteaseinhibitors (#78430, Life Technologies), immunoblotted, andmembraneswere scanned andquantitated usingOdyssey InfraredImaging System (LI-COR Biosciences) as described previous-ly (49). Primary antibodies used were GAPDH (1:10,000;#2118, Cell Signaling Technology), PARP1 (1:1,000; #sc-365315,Santa Cruz Biotechnology Inc.), PAR (1:1,000; #4335-MC-100,Trevigen), PARG (#NBP2-46320, 1:1,000; Novus), cleavedcaspase-3 (1:1,000), caspase-3 (1:1,000), and Histone H3(#9661, #9662, and #4499, Cell Signaling Technology) followedby LI-COR IRDye secondary antibodies.
ImmunofluorescenceA total of 5,000 cells were plated onto coverslips in 24-well
tissue culture plates and allowed to adhere for 24hours. After drugtreatment for indicated times and concentrations, coverslips werewashedwith 1� PBS,fixed (4%paraformaldehyde for 10minutesat room temperature), permeabilized (0.1% Triton-X), blockedand immunostained with gH2AX 1:500 (#05-636 MilliporeSigma) antibody overnight, 4�C, followed by secondary antibody(Alexa-488 F anti-mouse, #A-10680, Life Technologies) for 1hourafter washing. After the final wash step, coverslips weremounted onto slides using DAPI ProLong Gold AntifadeMounting Medium (#P36931, Life Technologies). Slides wereimaged with a Leica DM4B fluorescence microscope and fociwere counted using Image J software (28, 53). Percentage ofcells expressing >10 gH2AX foci per treatment condition � SDwas calculated and plotted.
PAR ELISAPARylation was analyzed in total protein lysates using HT
Colorimetric PARP/Apoptosis Assay as described previously (28).
Apoptosis assaysApoptosis was detected by Western blot analysis for cleaved
caspase-3 in drug-treated cells at different time points (27).
Chromatin tetheringTreated cells were washed with ice-cold 1�PBS, gently scraped
and collected in 1mL 1�PBS, and pelleted by spinning at 400� gfor 5 minutes. Sequential fractionation was performed with
PARG as a Target in PDAC
www.aacrjournals.org Cancer Res; 79(17) September 1, 2019 4493
on October 3, 2020. © 2019 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 4, 2019; DOI: 10.1158/0008-5472.CAN-18-3645

ice-cold 0.1% Triton X-100 in cytoskeletal PIPES buffer asdescribed previously (54). The final pellet (containing chroma-tin-boundproteins) and total cell pelletswere lysed inRIPAbuffer.Equal amounts of proteinwere loaded ontowells andmembraneswere immunoblotted with primary and corresponding secondaryantibodies.HistoneH3was used as a positive control andGAPDHas a negative control for the chromatin-bound fraction.
Xenograft studyDoxycycline-inducible shPARG knockdown model. Doxycycline-inducible shPARG cell lines were generated for MIA PaCa-2 cells.A total of 3 � 106 cells/flank (MIA.shPARG) were then injectedsubcutaneously (100 mL) in 5- to 6-week-old Hsd:AthymicNude-Foxn1nu female mice (Envigo RMS, Inc.). Cells were pre-pared in 80% DPBS and 20% Matrigel (#356237, Corning LifeSciences). Mice bearing established tumors (50–100 mm3, MIA.shPARG) were randomized into two treatment groups (n ¼ 5 foreach group) and one group was administered doxycycline chow(200 mg/kg, Bio-Serv) to downregulate PARG expression.
Statistical considerations. Mouse weights and tumor sizes weremeasured three times/week and tumor volumes were calculatedusing the formula: Volume ¼ (Length �Width2)/2. Relative foldchange in tumor volumes was plotted. Relative fold changerepresents fold change in tumor volume relative to tumor volumeon day 1 of randomization of mice into doxycycline/no doxycy-cline groups. No significant loss in body weight was observed(<5%) for all groups. Animals were euthanized when averagetumor volume reached 2,000 mm3.
All mouse protocols were approved by the Thomas JeffersonUniversity Institutional Animal Care and Use Committee.
Statistical analysisStatistical analyseswere performedusing the oneor two sample
t test as indicated in figure legends. GraphPad Prism 7.04 softwarewas used for analysis. Results are expressed as mean� SEM, if notspecifically indicated.
ResultsPARG silencing inhibits PDAC tumor growth in vivo and in vitro
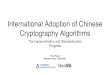
In vitro characterization of MIA.shPARG and Lenti.shPARG celllines confirmed a decrease in mRNA and protein expression ofPARG (Supplementary Fig. S1A and S1B). For in vivo–doxycycline-induced shPARG knockdown model, 5- to 6-week-old athymicnude female mice were injected with 100 mL of cell suspensionsubcutaneously in eachflank, andmicewere randomized into twogroups of: (i) no doxycycline and (ii) doxycycline chow. In thedoxycycline chow arm, knockdown of PARG significantlydecreased tumor growth in MIA.shPARG (P � 0.05), comparedwithmice in the no doxycycline group (Fig. 1A). At the conclusionof the study, tumors were harvested (Fig. 1A) and validated forPARG mRNA knockdown. mRNA expression analysis showsPARG levels were significantly decreased in groups fed on doxy-cycline chow with no change in a negative control, PARP1mRNAexpression (Fig. 1B). Lentivirus shPARG cell lines also show adecrease in growth rate as compared with a shScramble (control)cell line in vitro (Fig. 1C).
Silencing of PARG in the doxycycline-inducible MIA.shPARGor lentiviral shPARG models sensitized cells to oxaliplatin, as
indicated by a decrease in relative cell survival compared withcontrol arms (Fig. 1D; Supplementary Fig. S1C). Confirmingprevious reports, silencing of PARG decreased the sensitivity ofcells to olaparib (Fig. 1E; ref. 55). Collectively, these findingsimply that PARG targeting mediates a reduction in PDAC cellsurvival and tumor growth in vivo.
PARG inhibitors decrease cell survival of cancer cell lines withgenetically diverse backgrounds in vitroShort-term drug sensitivity assays. After establishing PARG as atherapeutic target from our in vivo studies, we assessed the efficacyof small-molecule inhibitors of PARG (PARGi; ref. 42) on cellsurvival of PDAC, PDX, and KPC cell culture models (Fig. 2A–D).Both MIA PaCa-2 and PANC-1 HR-P PDAC cell lines were treatedwith increasing doses of PARGis and olaparib to determine IC50
concentrations. Hs 766T, PDAC PDX, and KPC BRCA2 WT andBRCA1/2–null cell lines were treated with PDDX-01 and olapariband cell survival was evaluated using a cell survival, Pico Greenassay (49). PARG inhibition was especially effective against cellswith an HR deficiency (HR-D); Hs 766T, HR-D PDX cells(SPC_122), and KPC BRCA2--null cells were more sensitive toPARGi compared with their counterpart HR-P cells (Fig. 2A–D).Interestingly, with regard to our PDX lines, the cell line thatresponded the most to PARGi was SPC_122 (validated as BRCA1mutant) and those that did not respond were SPC_144 (BRCAWT) and SPC_126 (BRCA2 mutant). Of note, SPC_126 (Supple-mentary Table S1A) is obtained from a liver biopsy from a patientwho became clinically resistant to therapy (i.e., previouslyexposed to PARPi/platinum therapy and recurred, and is alsoresistant to PARPi therapy in vitro and in vivo; ref. 45). These datasuggest that PARGi may not be the best therapeutic option inPARPi-resistant tumors.
In addition, we found that PARG is differentially expressed inPDAC and PDXmodels (Supplementary Fig. S2A; SupplementaryTable S1B). We observed that high PARG–expressing cell linesresponded better to PARGi treatment (SPC_122), as comparedwith cell lines with medium expression of PARG protein (MIAPaCa-2, PANC-1, SPC_144, and others). The "normal" epithelialHPNE cells with low levels of PARG protein expression (Supple-mentary Fig. S2A; Supplementary Table S1B) did not respond toPARGi, supporting the possible therapeutic windowwe describedpreviously (28). We did find a perfect correlation (R2¼ 1) in PDXmodels, SPC_122 (high PARG expression/PARPi na€�ve; Supple-mentary Fig. S2B), and SPC_126 (low PARG expression/PARPiresistant; Supplementary Fig. S2B) PDX lines, which corroboratesprevious published findings (55). However, we did not find acorrelation between PARG expression and PARPi response acrossPDAC lines (Supplementary Fig. S2A and S2C), which suggeststhat defects in HR genes should still be the gold standard bio-marker for PARPi therapy.
To analyze the spectrum of PARGi effects in isogenic models,and the possible therapeutic window between normal andsomatic mutations found in a tumor, we also utilized genet-ically modified DLD1 (DLD1.BRCA2) and RKO (RKO.FANCC)colorectal cancer cells (43, 44). We have previously tested theselines against various DNA damage agents and disruption ofBRCA2 or FANCC renders them sensitive to oxaliplatin andPARPi (43). Our results show that both BRCA2 and FANCCnull cells required lower doses of PARGi to achieve IC50 whencompared with isogenic parental cells (SupplementaryFig. S2D).
Jain et al.
Cancer Res; 79(17) September 1, 2019 Cancer Research4494
on October 3, 2020. © 2019 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 4, 2019; DOI: 10.1158/0008-5472.CAN-18-3645

To further characterize synthetic lethality with PARG inhibitionand defects in genes involved in DNA damage response pathwaysin an isogenic model, we utilized HR-P PDAC cells, MIA PaCa-2,and PANC-1. Using siRNA oligos against BRCA1, BRCA2, ATM,and BARD1, we compared drug sensitivities of olaparib andPDDX-01 in these knock-down conditions to a scramble siRNAcontrol arm. In our screen, as expected, we found an increase insensitivity to olaparib with BRCA1/BRAC2 knockdown, whileonly BRCA2 knockdown increased sensitivity to PDDX-01, dem-onstrating synthetic lethality of PDDX-01 and BRCA2 in PDAC
cells (Fig. 2E; Supplementary Fig. S3A). Knockdown efficiencies ofall the genes inbothMIAPaCa-2 andPANC-1 cells are representedin Supplementary Fig. S3B.
Drug combination analyses. To test the efficacy of PARGi incombination with other commonly used DNA damaging agentsand PARPi (olaparib) in PDAC cells, we utilized Combenefitsoftware (50) to analyze synergy, additivity or antagonismbetween the combinations. The bliss index of combination anal-yses shows that PARGi (PDDX-01) did not synergize with
A B
C−D
OX
+DO
X
MIA.shPARG
ED
0
1
2
3
4
5
6
0 5 10
Fold
cha
nge
in g
row
th
(nor
mal
ized
to d
ay 1
)
Days
shSCR
shPARG
0.1 1 100
50
100
Oxaliplatin, μmol/L μmol/L
μmol/L
Rel
ativ
e su
rviv
al (%
)
Rel
ativ
e su
rviv
al (%
)R
elat
ive
surv
ival
(%)
Rel
ativ
e su
rviv
al (%
)
shSCR
shPARG*
*
*
* *
0.1 1 100
50
100
Oxaliplatin,
shSCRshPARG
*
0.1 1 10 1000
50
100
Olaparib, μmol/L
shSCRshPARG
*
*
*
0.1 1 10 1000
50
100
Olaparib,
shSCRshPARG
**
*
*
* *
PARG PARP10.0
0.5
1.0
1.5
2.0
Rel
ativ
e ex
pres
sion
( nor
mal
ized
to 1
8S)
MIA.shPARG −DOXMIA.shPARG +DOX
*
5 10 15 20 25 30 3505
1015202530354045505560
Days postrandomization
Rel
ativ
e fo
ld c
hang
e in
tum
or v
olum
e
MIA.shPARG +DOXMIA.shPARG −DOX
*P = 0.0032
Figure 1.
Knockdown of PARGwith shPARG decreases PDAC tumor growth in vivo and in vitro. A, Left, athymic nude mice bearing MIA.shPARG xenografts wererandomized into�doxycycline (DOX) andþdoxycycline arms, and relative fold change in tumor volume was plotted. � , P < 0.05 using two-sample t tests. Right,representative images of tumor extracted after completion of in vivo study fromMIA.shPARGmice (n¼ 5/group). B, Relative mRNA expression of PARG andPARP in harvested tumors fromMIA.shPARG (�/þdoxycycline) in vivo.Mean� SEM; n¼ 3; � , P¼ 0.01 to 0.05. C, In vitro fold change in growth of lentiviral.shPARG PANC-1 cells compared with shScramble. Lentiviral shPARG knockdown enhances sensitivity of cells to oxaliplatin (D) and decreases sensitivity toolaparib in PANC-1 (E; top) and MIA PaCa-2 (bottom) cells in vitro. Representative graphs from n¼ 3 are shown. � , P < 0.05 using two-sample t tests.
PARG as a Target in PDAC
www.aacrjournals.org Cancer Res; 79(17) September 1, 2019 4495
on October 3, 2020. © 2019 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 4, 2019; DOI: 10.1158/0008-5472.CAN-18-3645

olaparib and the combination is mostly antagonistic as seen inthe bliss matrix for olaparib and PARGi in both MIA PaCa-2and PANC-1 cells (Fig. 3A and B). However, when PARGi wasutilized with oxaliplatin or 5-FU (Fig. 3A and B), inhibition ofPARG synergized with these compounds, with some drugcombinations being more synergistic than others. It is interest-ing to note that single-agent PARGi, although not as effective inHR-P PDAC cells as HR-D cells, acts as a similar sensitizer toother DNA damage agents (oxaliplatin and 5-FU) in these celllines. There was no synergy seen in HR-D cells HS 766T witheither oxaliplatin/PARGi or 5-FU/PARGi combinations (Sup-plementary Fig. S4A and S4B).
Clonogenicity assays (long term assays). To understand the long-term effects of PARGi on PDAC cells, we performed clonogenic
assays. Both MIA PaCa-2 and PANC-1 cells were treated withPDDX-01 at increasing doses, and colonies were stained andcounted after 14 days (Fig. 4). PDDX-001 did not significantlyreduce colony formation in either MIA PaCa-2 (Fig. 4A) orPANC-1 cells (Fig. 4B), confirming our results from short-termcell survival assays. From our combination analyses, we furthertested the combination of PARGi and oxaliplatin/olaparib inboth these cell lines. Interestingly, inhibition of PARG byPDDX-01 sensitized both MIA PaCa-2 and PANC-1 cells tooxaliplatin (Fig. 4A and B), both of which are HR-P PDAC celllines. Similar to the results from combination analyses, PDDX-01 did not synergize with olaparib in decreasing colony for-mation of PDAC cells. Together, these data indicate that PARGihas activity and efficacy against PDAC cells and could beutilized to increase the sensitivity of oxaliplatin and other DNA
A
B
0.1 1 100
25
50
75
100
125SPC_126SPC_122SPC_144
D
0.01 0.1 1 100
50
100
PARG Inhibitor PDDX-01, mmol/L PARG Inhibitor PDDX-02, mmol/L PARG Inhibitor PDDX-04, mmol/L
PARG Inhibitor PDDX-01, mmol/LPARG Inhibitor PDDX-01, mmol/LPARG Inhibitor PDDX-01, mmol/L
PARG Inhibitor PDDX-01, mmol/L PARG Inhibitor PDDX-01, mmol/L PARG Inhibitor PDDX-01, mmol/L
Rel
ativ
e su
rviv
al (%
)R
elat
ive
surv
ival
(%)
Rel
ativ
e su
rviv
al (%
)
Rel
ativ
e su
rviv
al (%
)
Rel
ativ
e su
rviv
al (%
)
Rel
ativ
e su
rviv
al (%
)
Rel
ativ
e su
rviv
al (%
)
Rel
ativ
e su
rviv
al (%
)
Rel
ativ
e su
rviv
al (%
)
MIA PaCa-2PANC-1
0.01 0.1 1 100
50
100
MIA PaCa-2PANC-1
0.01 0.1 1 100
50
100
MIA PaCa-2PANC-1
0.1 1 10 1000
50
100
150
siCTRLsiBRCA1siBARD1siBRCA2siATM
E
C
0.1 1 10 1000
50
100
150
siCTRLsiBRCA1siBARD1siBRCA2siATM
MIA PaCa-2 PANC-1
0.1 1 10 1000
50
100
K8484 BRCA WTB3096 BRCA2 Null
0.1 1 10 1000
50
100
150
Day 3Day 5Day 7
0.1 1 10 1000
50
100
150
Day 5Day 7
Day 3
MIA PaCa-2 Hs 766T
Figure 2.
PARG inhibition is synthetic lethal with HR deficiency in PDAC cells. A, Pico Green assays were performed after 5 days of treatment with PDDX-01, PDDX-02,and PDDX-04 to analyze relative cell survival in PDAC cells (MIA PaCa-2, PANC-1). B–D, Relative cell survival of MIA PaCa-2 and Hs 766T treated with PDDX-01over 3, 5, and 7 days; KPC BRCAWT and KPC BRCA2–null cells as well as pancreatic cancer patient-derived xenograft cell lines (SPC_126, SPC_122, SPC_144).E, Synthetic lethality with PDDX-01 and siRNA DDR genes in MIA PaCa-2 and PANC-1 cells. Representative graphs from n¼ 2 forA and n¼ 3 for B–E are shown.
Jain et al.
Cancer Res; 79(17) September 1, 2019 Cancer Research4496
on October 3, 2020. © 2019 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 4, 2019; DOI: 10.1158/0008-5472.CAN-18-3645

Figure 3.
PARGi synergizes with DNA damage agents and not with PARPi. Drug matrix heatmap 5� 5 (olaparib and 5-FU) and 6� 5 (oxaliplatin) grid showing Bliss indexand dose response as analyzed by Combenefit analysis for MIA PaCa-2 (A) and PANC-1 cells (B). Combinations that are synergistic appear blue on the heatmap.
PARG as a Target in PDAC
www.aacrjournals.org Cancer Res; 79(17) September 1, 2019 4497
on October 3, 2020. © 2019 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 4, 2019; DOI: 10.1158/0008-5472.CAN-18-3645

A
B
NT 1.2 2.5 5 10 20 1 1+PDDX-01(20)
10 10+PDDX-01(20)
0
50
100
PDDX-01 Oxaliplatin Olaparib
*
*
n.s.
NT 1.2 μmol/L 2.5 μmol/L
5 μmol/L 10 μmol/L 20 μmol/L
Oxaliplatin 1 μmol/L
Oxali +PDDX-01
Olaparib 10 μmol/L
Olap +PDDX-01PA
NC
-1M
IA P
aCa-
2
NT 1.5 3.1 6.2 12.5 25 1.2 1.2+PDDX-01(6.2)
15 15+PDDX-01(6.2)
0
50
100
% R
elat
ive
colo
nies
% R
elat
ive
colo
nies
PDDX-01 Oxaliplatin Olaparib
**
***
n.s.
NT 1.5 μmol/L 3.1 μmol/L
6.2 μmol/L 12.5 μmol/L 25 μmol/L
Oxaliplatin 1.2 μmol/L Olaparib 15 μmol/L
Oxali +PDDX-01 Olap +PDDX-01
Figure 4.
PARGi decreases colony formation in PDAC cells in combination with oxaliplatin. MIA PaCa-2 (A) and PANC-1 (B) cell lines were treated with increasing doses ofPDDX-01 (mmol/L) alone and in combination with oxaliplatin (oxali) or olaparib (olap), and resulting colonies were fixed and stained with crystal violet solution.Representative images with graphs of relative colonies are shown. Mean� SEM; n¼ 3. �, P¼ 0.01 to 0.05; �� , P¼ 0.001 to 0.01; ��� , P¼ 0.0001 to 0.001, n.s.nonsignificant using two-sample t tests.
Jain et al.
Cancer Res; 79(17) September 1, 2019 Cancer Research4498
on October 3, 2020. © 2019 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 4, 2019; DOI: 10.1158/0008-5472.CAN-18-3645

damage agents (like 5-FU) but not PARPi (olaparib) for thetreatment of PDAC.
PARGi affects PARylation dynamics of PDAC cells and regulatesPARG activity
To further assess themechanismof PARGi-induced cytotoxicityand whether PARGi causes an increase in PAR accumulation inPDAC cells, we performed chromatin tethering assays (54). We
analyzed PARP and PAR protein expression in chromatin-boundfractions after treatment with PARGi alone or in combinationwith oxaliplatin or olaparib in PDAC cell lines. GAPDHwas usedas a negative control and histone H3 expression was used as apositive control for chromatin fractions. PDDX-01 increasedchromatin bound PAR expression in both MIA PaCa-2 andPANC-1 cells treated alone as shown in Fig. 5A and B. We alsoobserved a synergistic effect of PARGi with oxaliplatin as seen
MIA PaCa-2
Chr
omat
in-b
ound
Tota
l pro
tein
PARP1
GAPDH
Histone H3
PARP1
GAPDH
Histone H3
PARG
PAR
PANC-1A BPDDX-01(25 μmol/L)
Olap (10 μmol/L) Oxali (2 μmol/L)
− ++
+
Histone H3
Histone H3
Chr
omat
in-b
ound
PARP1
PARP1
GAPDH
PAR
PARG
GAPDH
PDDX-01(20 μmol/L)Olap (10 μmol/L)Oxali (1 μmol/L)
C
D
PA
NC
-1
PDDX-01(5 μmol/L)Oxali (1 μmol/L)
Stauro (5 μmol/L)
α-Tubulin
Cleaved caspase-3
Caspase-3
24 48 72Time (hours)
Control
PDDX-01+Oxali
PDDX-01
Oxaliplatin
Control PDDX-01 Oxali PDDX-01+Oxali0
20
40
60
80
100
%Ce
lls>1
0γγ H
2AX
f oci ***
****
***
PA
NC
-1−−
−−
−
−+−
−−+
+−+
Tota
l pro
tein
− ++
+−−
−−
−
−+−
−−+
+−+
+
−−
−−−
+−−
+−
−+−
+ −−−
+−−
+−
−+−
+ −−−
+−−
+−
−+−
+
Figure 5.
PARGi induces PAR accumulation. MIA PaCa-2 (A) and PANC-1 (B) cells were treated with either PDDX-01, olaparib or oxaliplatin, alone or in combination for24 hours, and chromatin and whole-cell fractions were isolated. RepresentativeWestern blot images are shown from n¼ 3. GAPDH and Histone H3 served ascontrols for whole-cell fraction and chromatin fractions, respectively. C, PARGi in combination with oxaliplatin causes cleavage of caspase-3. PANC-1 cells weretreated with PDDX-01, oxaliplatin, or combination, and apoptosis was assessed byWestern blot analysis for cleaved caspase-3 at 24-, 48-, and 72-hour timepoints. Representative image from n¼ 3 is shown. D, PARGi induces DNA damage in combination with oxaliplatin. gH2AX foci increases with the combination ofPDDX-01 and oxaliplatin at 24 hours in PANC-1 cells. Representative graphs of cells with >10 foci are shown. Mean� SD; n¼ 3. � , P < 0.05; ��� , P < 0.001.
PARG as a Target in PDAC
www.aacrjournals.org Cancer Res; 79(17) September 1, 2019 4499
on October 3, 2020. © 2019 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 4, 2019; DOI: 10.1158/0008-5472.CAN-18-3645

in Figs. 3 and 4, which could not be attributed to synergisticincrease in accumulated PAR with the combination (43). Con-trary to this affect, and as previously shown (55), olaparib notonly decreased relative PARylation as a consequence of inhibitingPARP1 activity alone, but also prevented PARGi-induced increasein PAR (Fig. 5A and B), implying that inhibition of PARGidoes not benefit PARPi therapy, in agreement with previousresults (55).
To evaluatewhether PARG inhibitors affect relative PARylation,whole-cell PARylation was assessed by ELISA assays (28). AllPARGi compounds significantly lead to persistence of whole-cell PARylation, as analyzed by ELISA assays (Supplementary Fig.S5A) in both HR-P and HR-D PDAC cells. PARPi (olaparib) wasused as the negative control, which has previously been shown toeffectively prevent PAR polymer formation (28).
PARGi affects apoptosis and amarker of DNAdamage responseIn an effort to find the mechanism of synergy between PARGi
and oxaliplatin in PDAC cells, we assessed apoptosis by cleavedcaspase-3 expression in both MIA PaCa-2 and PANC-1 cells.Increase in cleaved caspase-3 with oxaliplatin was seen as earlyas 24 hours for both MIA PaCa-2 cells and PANC-1 cells (Fig. 5C;Supplementary Fig. S6A). This suggests that activation of caspasesis a possible mechanism of synergistic cell death between PARGiand oxaliplatin.
In addition,we analyzed gH2AX expression as amarker ofDNAdamage and found a significant increase in gH2AX foci in com-bination treatments across both the cell lines, indicating anincrease in DNA damage (Fig. 5D; Supplementary Fig. S6B).Taken together, these results demonstrate that targeting PARGwith DNA damage agents induces DNA damage and apoptosis inPDAC cells.
DiscussionCurrent standard-of-care chemotherapeutic regimens show
only modest increases in overall survival of patients withPDAC (56, 57). Thus, there remains a desperate need to findtargets and therapies, which eventually could be personalized forPDAC (2–7, 10, 58). Recently, a successful phase II study ofolaparib (PARPi) showed significant clinical activity in patientswith BRCA1/2 (HR-D)–mutant pancreatic cancer previously trea-ted with gemcitabine (19). However, many studies have alreadystarted to emerge with PARPi resistance (24–26). Previously, wepublished that PARPi treatment causes an increase in PARGprotein through a novel posttranscriptionalmechanism regulatedby stress-responsive RNA binding protein, HuR in PDAC (28).On the basis of these data and the fact that PARG is part of theDNA repair process, we explored PARG as a therapeutic target inPDAC by first utilizing shRNA genomic approaches to silencePARG expression and activity, and then validating these find-ings through the use of established small-molecule PARGinhibitors (38, 42).
The data presented herein also demonstrate that small-molecule inhibitors of PARG decrease cell survival, proliferation,and induce DNA damage in PDAC cells when used as mono-therapy or in combination with DNA damage agents in vitro(Figs. 2–5). IC50 values of PARGi values indicate that in variousisogenic and nonisogenic PDAC cell models PARG inhibitorsare more effective against HR-D cells when compared with HR-P cells, highlighting previous reports that PARG targeting may
have beneficial synthetic lethal effects on cells with HRdeficiencies (35–38, 59). In sum, these data suggest PARGi shouldbe explored as a novel synthetic lethal approach in PDAC tumorsthat share molecular features with BRCA-mutant PDAC subtypes.
Althoughour study shows that PARGi ismore effective inHR-DPDAC cells, PARGi caused increased PARylation and a significantdecrease in PARG activity in both HR-D and HR-P PDAC cells,without directly affecting protein levels of either PARG or PARP1.The increase in PARylation after PARGi emphasizes the specificityof PARGi and the importance of PARG as a primary PAR catab-olizing enzyme (60). This also suggests that PARG may be amore favorable target over other DNA repair proteins like PARP1,which has multiple family members (33, 41). Although theseinhibitors currently have limited bioavailability (42), our resultssupport development of these lead compounds for morefavorable bioavailable small-molecule PARGis for effective target-ing of PARG in vivo. In an ongoing effort, we have startedinvestigating a 3DNA-nanocarrier delivery of modified siPARGto target PARG with a tumor-specific targeting moiety in vivo(Supplementary Fig. S7).
Combination treatments of PARGi with either oxaliplatin or5-FU (components of FOLFIRINOX) in HR-P PDAC cell linesprovide evidence that targetingPARGcould synergizewith currentstandard-of-care treatments for PDAC (Fig. 3). Our results high-light that PARGi is antagonistic with olaparib (PARPi), as ana-lyzed through bliss index of combination treatments (Fig. 3).These results are in agreement with a recent study published byGogola and colleagues that show loss of PARG as a resistancemechanism to PARPi therapy in murine mammary tumor cellsand that PARP1 signaling is rescued by PARGi-mediated PARaccumulation (55). To understand the increased sensitivity ofoxaliplatin in presence of PARGi, we looked at PAR levels inchromatin fractions. Accumulation of PAR polymers and furtherloss of NADþ pools are reported to cause cytotoxicity (61–63).From our results, we did not find a synergistic increase in accu-mulation of PAR with the combination of oxaliplatin and PARGi(Fig. 5A and B). However, we found an increase in DNA damageand elevated cleaved caspase-3 expression with the combination,both of which could implicate mechanisms behind synergy seenwith oxaliplatin and PARGi (Fig. 5C and D; Supplementary Fig.S6A and S6B). Future studies will determine the precise mecha-nism of increased sensitivity of 5-FU or oxaliplatin with PARGi inan in vivo setting. Overall, these findings favor targeting PARG incombination with DNA-damaging agents (e.g., oxaliplatin) andwarrants further in vivo dose optimization and sequencing (i.e.,timing) studies.
Taken together, we strongly believe this work provides the firstevidence that acute targeting of PARG should be pursued as atreatment strategy for PDAC with both HR-proficient and -defi-cient genetic backgrounds. More sophisticated, ongoing in vivostudies will evaluate next-generation PARG-targeting strategies(i.e., other small molecules and siPARG nanotherapy) in combi-nation with other DNA-damaging agents for the treatment of allpancreatic cancers.
Disclosure of Potential Conflicts of InterestG.A. McCarthy reports receiving a commercial research grant from
Genisphere, LLC. T. Golan reports receiving a commercial research grantfrom MSD and AstraZeneca, has received speakers bureau honoraria fromAbbvie, and is a consultant/advisory board member for Abbvie and Teva.D.I. James is a consultant for Cancer Research UK. J.R. Brody reports receiving
Jain et al.
Cancer Res; 79(17) September 1, 2019 Cancer Research4500
on October 3, 2020. © 2019 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 4, 2019; DOI: 10.1158/0008-5472.CAN-18-3645

a commercial research grant from Genisphere, LLC. No potential conflicts ofinterest were disclosed by the other authors.
Authors' ContributionsConception and design: A. Jain, L.C. Agostini, S.N. Chand, C.W. Schultz,J.R. BrodyDevelopment of methodology: A. Jain, L.C. Agostini, G.A. McCarthy,S.N. Chand, J. Cozzitorto, D. Ogilvie, D.I. James, A.M. JordanAcquisition of data (provided animals, acquired and managed patients,provided facilities, etc.): A. Jain, G.A. McCarthy, S.N. Chand, A. Ramirez,A. Nevler, J. Cozzitorto, C.W. Schultz, C.Y. Lowder, M. Raitses-Gurevich,C. Stossel, Y.G. Gorman, D. Atias, C.J. Yeo, K.P. Olive, T. Golan, D.I. JamesAnalysis and interpretation of data (e.g., statistical analysis, biostatistics,computational analysis): A. Jain, L.C. Agostini, G.A. McCarthy, S.N. Chand,C.W. Schultz, M.J. Pishvaian, D.I. James, J.R. BrodyWriting, review, and/or revision of the manuscript: A. Jain, L.C. Agostini,G.A. McCarthy, A. Nevler, C.Y. Lowder, I.D. Waddell, C.J. Yeo, J.M. Winter,T. Golan, M.J. Pishvaian, D.I. James, A.M. Jordan, J.R. BrodyAdministrative, technical, or material support (i.e., reporting or organizingdata, constructing databases): A. Jain, S.N. Chand, C.J. Yeo, D.I. James,J.R. BrodyStudy supervision: A. Jain, S.N. Chand, I.D. Waddell, C.J. Yeo, J.M. Winter,J.R. Brody
Others (synthesis of compound used in the study): K.M. SmithOthers (provision of small molecule tools): A.M. Jordan
AcknowledgmentsWe would like to thank Genisphere LLC (Dr. Robert Getts, Hatfield, PA) for
providing us with the modified siPARG. Mark Levine's contributions to thiswork were made in memory of Ethel Levine. This work was supported by NIH-NCI R01 CA212600 (to J.R. Brody) and R37CA227865 (to J.M. Winter and J.R.Brody), and was also supported by the NCI of the NIH under Award NumberP30CA056036 SKCC Core Grant (Thomas Jefferson University). Additionalwork is supported by a 2015 Pancreatic Cancer Action Network AmericanAssociation for Cancer Research Acceleration Network Grant (15-90-25-BRODto J.R. Brody and M.J. Pishvaian). This work is also generously supported by aMary Halinski Fellowship (to A. Nevler) and the W. Kim Foster PancreaticCancer Research Endowment. K.M. Smith, I.D. Waddell, D. Ogilvie, D.I. James,and A.M. Jordan are supported by Cancer Research UK (grants C480/A11411and C5759/A17098).
The costs of publication of this articlewere defrayed inpart by the payment ofpage charges. This article must therefore be hereby marked advertisement inaccordance with 18 U.S.C. Section 1734 solely to indicate this fact.
Received November 20, 2018; revised May 6, 2019; accepted July 1, 2019;published first July 4, 2019.
References1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J Clin
2016;66:7–30.2. Sheahan AV, Biankin AV, Parish CR, Khachigian LM. Targeted therapies in
the management of locally advanced and metastatic pancreatic cancer: asystematic review. Oncotarget 2018;9:21613–27.
3. Jones S, Zhang X, Parsons DW, Lin JC, Leary RJ, Angenendt P, et al. Coresignaling pathways in human pancreatic cancers revealed by global geno-mic analyses. Science 2008;321:1801–6.
4. Bailey P, Chang DK, Nones K, Johns AL, Patch AM, Gingras MC, et al.Genomic analyses identifymolecular subtypes of pancreatic cancer. Nature2016;531:47–52.
5. Waddell N, Pajic M, Patch AM, Chang DK, Kassahn KS, Bailey P, et al.Whole genomes redefine the mutational landscape of pancreatic cancer.Nature 2015;518:495–501.
6. Pishvaian MJ, Bender RJ, Halverson D, Rahib L, Hendifar AE, Mikhail S,et al. Molecular profiling of pancreatic cancer patients: initial results fromthe know your tumor initiative. Clin Cancer Res 2018;24:5018–27.
7. Pishvaian MJ, Brody JR. Therapeutic implications of molecular subtypingfor pancreatic cancer. Oncology 2017;31:159–66.
8. Aguirre AJ, Nowak JA, Camarda ND, Moffitt RA, Ghazani AA, Hazar-Rethinam M, et al. Real-time genomic characterization of advanced pan-creatic cancer to enable precision medicine. Cancer Discov 2018;8:1096–111.
9. ChouA,Waddell N, CowleyMJ,Gill AJ, ChangDK, PatchAM, et al. Clinicaland molecular characterization of HER2 amplified-pancreatic cancer.Genome Med 2013;5:78.
10. Sjoquist KM, Chin VT, Chantrill LA,O'Connor C,Hemmings C, ChangDK,et al. Personalising pancreas cancer treatment: when tissue is the issue.World J Gastroenterol 2014;20:7849–63.
11. Frank TS, Sun X, Zhang Y, Yang J, Fisher WE, Gingras MC, et al. Genomicprofiling guides the choice of molecular targeted therapy of pancreaticcancer. Cancer Lett 2015;363:1–6.
12. Papeo G, Casale E, Montagnoli A, Cirla A. PARP inhibitors in cancertherapy: an update. Expert Opin Ther Pat 2013;23:503–14.
13. Kawahara N, Ogawa K, Nagayasu M, Kimura M, Sasaki Y, Kobayashi H.Candidate synthetic lethality partners to PARP inhibitors in the treatmentof ovarian clear cell cancer. Biomed Rep 2017;7:391–9.
14. Lumachi F, Chiara GB, Foltran L, Basso SM. Proteomics as a guide forpersonalized adjuvant chemotherapy in patients with early breast cancer.Cancer Genomics Proteomics 2015;12:385–90.
15. Weren RD,Mensenkamp AR, SimonsM, EijkelenboomA, Sie AS, OucheneH, et al. Novel BRCA1 and BRCA2 tumor test as basis for treatment
decisions and referral for genetic counselling of patients with ovariancarcinomas. Hum Mutat 2017;38:226–35.
16. Lowery MA, Kelsen DP, Capanu M, Smith SC, Lee JW, Stadler ZK, et al.Phase II trial of veliparib in patients with previously treated BRCA-mutatedpancreas ductal adenocarcinoma. Eur J Cancer 2018;89:19–26.
17. National Cancer Institute. FOLFIRI or modified FOLFIRI and veliparib assecond line therapy in treating patients with metastatic pancreatic cancer.Available from: https://clinicaltrials.gov/ct2/show/NCT02890355.
18. National Cancer Institute. Gemcitabine hydrochloride and cisplatinwith or without veliparib or veliparib alone in treating patients withlocally advanced or metastatic pancreatic cancer. Available from: https://clinicaltrials.gov/ct2/show/NCT01585805.
19. Kaufman B, Shapira-Frommer R, Schmutzler RK, Audeh MW, FriedlanderM, Balma~na J, et al. Olaparib monotherapy in patients with advancedcancer and a germline BRCA1/2 mutation. J Clin Oncol 2015;33:244–50.
20. Pishvaian MJ, Slack R, Witkiewicz A, He AR, Hwang JJ, Apte SK, et al.A phase I/II study of the PARP inhibitor, ABT-888 plus 5-fluorouracil andoxaliplatin (modified FOLFOX-6) in patients with metastatic pancreaticcancer. J Clin Oncol 29:15s, 2011 (suppl; abstr TPS170).
21. de Bono J, Ramanathan RK,Mina L, Chugh R,Glaspy J, Rafii S, et al. Phase I,dose-escalation, two-part trial of the PARP inhibitor talazoparib in patientswith advanced germline BRCA1/2mutations and selected sporadic cancers.Cancer Discov 2017;7:620–9.
22. Walsh C. Targeted therapy for ovarian cancer: the rapidly evolving land-scape of PARP inhibitor use. Minerva Ginecol 2018;70:150–70.
23. Keung MYT, Wu Y, Vadgama JV. PARP inhibitors as a therapeutic agent forhomologous recombination deficiency in breast cancers. J Clin Med 2019;8. doi: 10.3390/jcm8040435.
24. Turner NC, Ashworth A. Biomarkers of PARP inhibitor sensitivity.Breast Cancer Res Treat 2011;127:283–6.
25. Fojo T, Bates S. Mechanisms of resistance to PARP inhibitors–three andcounting. Cancer Discov 2013;3:20–3.
26. Pishvaian MJ, Biankin AV, Bailey P, Chang DK, Laheru D, Wolfgang CL,et al. BRCA2 secondary mutation-mediated resistance to platinum andPARP inhibitor-based therapy in pancreatic cancer. Br J Cancer 2017;116:1021–6.
27. Lal S, Burkhart RA, Beeharry N, Bhattacharjee V, Londin ER, Cozzitorto JA,et al. HuR posttranscriptionally regulates WEE1: implications for the DNAdamage response in pancreatic cancer cells. Cancer Res 2014;74:1128–40.
28. Chand SN, Zarei M, Schiewer MJ, Kamath AR, Romeo C, Lal S, et al.Posttranscriptional regulation of PARG mRNA by HuR facilitates DNArepair and resistance to PARP inhibitors. Cancer Res 2017;77:5011–25.
PARG as a Target in PDAC
www.aacrjournals.org Cancer Res; 79(17) September 1, 2019 4501
on October 3, 2020. © 2019 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 4, 2019; DOI: 10.1158/0008-5472.CAN-18-3645

29. Karnak D, Engelke CG, Parsels LA, Kausar T, Wei D, Robertson JR, et al.Combined inhibition of Wee1 and PARP1/2 for radiosensitization inpancreatic cancer. Clin Cancer Res 2014;20:5085–96.
30. Rotin LE, GrondaM,MacLeanN,Hurren R,Wang X, Lin FH, et al. Ibrutinibsynergizes with poly(ADP-ribose) glycohydrolase inhibitors to induce celldeath in AML cells via a BTK-independentmechanism. Oncotarget 2016;7:2765–79.
31. Fauzee NJ, Li Q, Wang YL, Pan J. Silencing poly (ADP-ribose) glycohy-drolase (PARG) expression inhibits growth of human colon cancer cellsin vitro via PI3K/Akt/NFkappa-B pathway. Pathol Oncol Res 2012;18:191–9.
32. Nakadate Y, Kodera Y, Kitamura Y, Tachibana T, Tamura T, Koizumi F.Silencing of poly(ADP-ribose) glycohydrolase sensitizes lung cancer cellsto radiation through the abrogation of DNA damage checkpoint.Biochem Biophys Res Commun 2013;441:793–8.
33. Cortes U, Tong WM, Coyle DL, Meyer-Ficca ML, Meyer RG, Petrilli V, et al.Depletion of the 110-kilodalton isoform of poly(ADP-ribose) glycohy-drolase increases sensitivity to genotoxic and endotoxic stress in mice.Mol Cell Biol 2004;24:7163–78.
34. Min W, Cortes U, Herceg Z, Tong WM, Wang ZQ. Deletion of the nuclearisoformof poly(ADP-ribose) glycohydrolase (PARG) reveals its function inDNA repair, genomic stability and tumorigenesis. Carcinogenesis 2010;31:2058–65.
35. Koh DW, Lawler AM, Poitras MF, Sasaki M, Wattler S, Nehls MC, et al.Failure to degrade poly(ADP-ribose) causes increased sensitivity to cyto-toxicity and early embryonic lethality. Proc Natl Acad Sci U S A 2004;101:17699–704.
36. Breslin C, Hornyak P, Ridley A, Rulten SL, Hanzlikova H, Oliver AW, et al.The XRCC1 phosphate-binding pocket binds poly (ADP-ribose) and isrequired for XRCC1 function. Nucleic Acids Res 2015;43:6934–44.
37. Ame JC, Fouquerel E, Gauthier LR, Biard D, Boussin FD, Dantzer F, et al.Radiation-induced mitotic catastrophe in PARG-deficient cells. J Cell Sci2009;122:1990–2002.
38. Gravells P, Grant E, Smith KM, JamesDI, BryantHE. Specific killing ofDNAdamage-response deficient cells with inhibitors of poly(ADP-ribose) gly-cohydrolase. DNA Repair 2017;52:81–91.
39. De Toni EN, Ziesch A, Rizzani A, T€or€okHP,Hocke S, L€u S, et al. Inactivationof BRCA2 in human cancer cells identifies a subset of tumors withenhanced sensitivity towards death receptor-mediated apoptosis. Onco-target 2016;7:9477–90.
40. Koh DW, Dawson VL, Dawson TM. The road to survival goes throughPARG. Cell Cycle 2005;4:397–9.
41. Gravells P, Neale J, Grant E, Nathubhai A, Smith KM, James DI, et al.Radiosensitization with an inhibitor of poly(ADP-ribose) glycohydrolase:a comparison with the PARP1/2/3 inhibitor olaparib. DNA Repair 2018;61:25–36.
42. James DI, Smith KM, Jordan AM, Fairweather EE, Griffiths LA, HamiltonNS, et al. First-in-class chemical probes against poly(ADP-ribose) glycohy-drolase (PARG) inhibit DNA repair with differential pharmacology toolaparib. ACS Chem Biol 2016;11:3179–90.
43. Hucl T, Rago C, Gallmeier E, Brody JR, Gorospe M, Kern SE. A syngeneicvariance library for functional annotation of human variation: applicationto BRCA2. Cancer Res 2008;68:5023–30.
44. Gallmeier E, Calhoun ES, Rago C, Brody JR, Cunningham SC, Hucl T, et al.Targeted disruption of FANCC and FANCG in human cancer provides apreclinical model for specific therapeutic options. Gastroenterology 2006;130:2145–54.
45. Golan T, Stossel C, Atias D, Buzhor E, Halperin S, Cohen K, et al.Recapitulating the clinical scenario of BRCA-associated pancreatic cancerin pre-clinical models. Int J Cancer 2018;143:179–83.
46. Olive KP, Jacobetz MA, Davidson CJ, Gopinathan A, McIntyre D,Honess D, et al. Inhibition of Hedgehog signaling enhances delivery
of chemotherapy in a mouse model of pancreatic cancer. Science 2009;324:1457–61.
47. Schreiber FS,Deramaudt TB, Brunner TB, BorettiMI, GoochKJ, StoffersDA,et al. Successful growth and characterization of mouse pancreatic ductalcells: functional properties of the Ki-RAS(G12V) oncogene. Gastroenter-ology 2004;127:250–60.
48. Waszkowycz B, Smith KM, McGonagle AE, Jordan AM, Acton B, Fair-weather EE, et al. Cell-active smallmolecule inhibitors of theDNA-damagerepair enzyme poly(ADP-ribose) glycohydrolase (PARG): discovery andoptimization of orally bioavailable quinazolinedione sulfonamides. JMedChem 2018;61:10767–92.
49. Jimbo M, Blanco FF, Huang YH, Telonis AG, Screnci BA, Cosma GL, et al.Targeting the mRNA-binding protein HuR impairs malignant character-istics of pancreatic ductal adenocarcinoma cells. Oncotarget 2015;6:27312–31.
50. Di Veroli GY, Fornari C,WangD,Mollard S, Bramhall JL, Richards FM, et al.Combenefit: an interactive platform for the analysis and visualization ofdrug combinations. Bioinformatics 2016;32:2866–8.
51. Roell KR, Reif DM,Motsinger-Reif AA. An introduction to terminology andmethodology of chemical synergy-perspectives from across disciplines.Front Pharmacol 2017;8:158.
52. RafehiH,Orlowski C,GeorgiadisGT, Ververis K, El-Osta A, Karagiannis TC.Clonogenic assay: adherent cells. J Vis Exp 2011;49. doi: 10.3791/2573.
53. Blanco FF, JimboM,Wulfkuhle J, Gallagher I, Deng J, Enyenihi L, et al. ThemRNA-binding protein HuR promotes hypoxia-induced chemoresistancethrough posttranscriptional regulation of the proto-oncogene PIM1 inpancreatic cancer cells. Oncogene 2016;35:2529–41.
54. Sever-Chroneos Z, Angus SP, Fribourg AF, Wan H, Todorov I, Knudsen KE,et al. Retinoblastoma tumor suppressor protein signals through inhibitionof cyclin-dependent kinase 2 activity to disrupt PCNA function in S phase.Mol Cell Biol 2001;21:4032–45.
55. Gogola E, Duarte AA, de Ruiter JR, Wiegant WW, Schmid JA, de BruijnR, et al. Selective loss of PARG restores PARylation and counteractsPARP inhibitor-mediated synthetic lethality. Cancer Cell 2018;33:1078–93.
56. SatyanandaV,Gupta R,HariDM, Yeh J, ChenKT. Advances in translationalresearch and clinical care in pancreatic cancer: where are we headed?Gastroenterol Res Pract 2019;2019:7690528.
57. Zhang Y, Hochster H, Stein S, Lacy J. Gemcitabine plus nab-paclitaxelfor advanced pancreatic cancer after first-line FOLFIRINOX: singleinstitution retrospective review of efficacy and toxicity. Exp HematolOncol 2015;4:29.
58. Rahib L, Smith BD, Aizenberg R, Rosenzweig AB, Fleshman JM, MatrisianLM. Projecting cancer incidence and deaths to 2030: the unexpectedburden of thyroid, liver, and pancreas cancers in the United States.Cancer Res 2014;74:2913–21.
59. Shirai H, Poetsch AR, Gunji A, Maeda D, Fujimori H, Fujihara H, et al.PARG dysfunction enhances DNA double strand break formation in S-phase after alkylation DNA damage and augments different cell deathpathways. Cell Death Dis 2013;4:e656.
60. O'Sullivan J, Tedim Ferreira M, Gagn�e JP, Sharma AK, Hendzel MJ, MassonJY, et al. Emerging roles of eraser enzymes in the dynamic control of proteinADP-ribosylation. Nat Commun 2019;10:1182.
61. Kim MY, Zhang T, Kraus WL. Poly(ADP-ribosyl)ation by PARP-1: `PAR-laying' NADþ into a nuclear signal. Genes Dev 2005;19:1951–67.
62. Barkauskaite E, Brassington A, Tan ES, Warwicker J, Dunstan MS, Banos B,et al. Visualization of poly(ADP-ribose) bound to PARG reveals inherentbalance between exo- and endo-glycohydrolase activities. Nat Commun2013;4:2164.
63. Alvarez-Gonzalez R, Watkins TA, Gill PK, Reed JL, Mendoza-Alvarez H.Regulatory mechanisms of poly(ADP-ribose) polymerase. Mol Cell Bio-chem 1999;193:19–22.
Cancer Res; 79(17) September 1, 2019 Cancer Research4502
Jain et al.
on October 3, 2020. © 2019 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 4, 2019; DOI: 10.1158/0008-5472.CAN-18-3645

2019;79:4491-4502. Published OnlineFirst July 4, 2019.Cancer Res Aditi Jain, Lebaron C. Agostini, Grace A. McCarthy, et al. Pancreatic CancerPoly (ADP) Ribose Glycohydrolase Can Be Effectively Targeted in
Updated version
10.1158/0008-5472.CAN-18-3645doi:
Access the most recent version of this article at:
Material
Supplementary
http://cancerres.aacrjournals.org/content/suppl/2019/07/04/0008-5472.CAN-18-3645.DC1
Access the most recent supplemental material at:
Cited articles
http://cancerres.aacrjournals.org/content/79/17/4491.full#ref-list-1
This article cites 58 articles, 18 of which you can access for free at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/79/17/4491To request permission to re-use all or part of this article, use this link
on October 3, 2020. © 2019 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst July 4, 2019; DOI: 10.1158/0008-5472.CAN-18-3645