Embed Size (px)
Citation preview

Evaluation of the Global Polio Eradication Initiative ��
�
Report on the independent evaluation of the major barriers to interrupting poliovirus transmission in Afghanistan
Michael Toole
Stephanie Simmonds
Benjamin Coghlan
Najibullah Mojadidi �
�
Final Report
October 2009
�

Independent evaluation of the Global Polio Eradication Initiative, Afghanistan, August 2009
�
� ��
CONTENT OF REPORT
List of abbreviations
Acknowledgements
Executive Summary and Recommendations
Map of Afghanistan
CHAPTER 1: POLIO SITUATION IN AFGHANISTAN CHAPTER 2: KEY COMPONENTS OF POLIO PROGRAM CHAPTER 3: HEALTH SYSTEM AND SERVICE DELIVERY
FACTORS AFFECTING PROGRAM PERFORMANCE CHAPTER 4: COMMUNITY ISSUES AFFECTING PROGRAM
COVERAGE CHAPTER 5: NON-HEALTH FACTORS AFFECTING PROGRAM
PERFORMANCE CHAPTER 6: TECHNICAL ISSUES THAT MAY BE BARRIERS TO
ERADICATION CONCLUSIONS Annex 1: Persons Met
Annex 2: Schedule
� �
Stephanie Simmonds Ben Coghlan
Michael Toole
Najibullah Mojadidi

Independent evaluation of the Global Polio Eradication Initiative, Afghanistan, August 2009
�
� ��
ABBREVIATIONS
AFP Acute Flaccid Paralysis AGE Anti-Government Elements AVA Afghanistan Veterinary Association BHC Basic Health Centre BPHS Basic Package of Health Services BVW Basic Veterinary Worker CHW Community Health Worker CIDA Canadian International Development Agency DC District Coordinator EC European Commission EPI Expanded Programme on Immunization ERC Expert Review Committee EPHS Essential Package of Hospital Services GAVI Global Alliance for Vaccines and Immunization ICRC International Committee of the Red Cross ISAF International Security Assistance Force KAP Knowledge, Attitudes, and Practices MoA Ministry of Agriculture MoPH Ministry of Public Health MoPH-SM Ministry of Public Health – Strengthening Mechanism MRRD Ministry of Rural Reconstruction and Development NEMT National EPI Management Team NGO Non-Governmental Organization NID National Immunization Day NWFP North-West Frontier Province of Pakistan OPV Oral Polio Vaccine MDGs Millennium Development Goals mOPV Monovalent OPV tOPV Trivalent OPV PEI Polio Eradication Initiative PEMT Provincial EPI Management Team PHD Provincial Health Director PRT Provincial Reconstruction Team QIP Quick Impact Project RED Reach Every District REMT Regional EPI Management Team SIA Supplementary Immunization Activity SNID Sub-National Immunization Day SOP Standard Operating Procedures SOS Sustainable Outreach Services UNAMA United Nations Assistance Mission in Afghanistan UNDSS United Nations Department of Safety and Security USAID United States Agency for International Development VAPP Vaccine-associated paralytic poliomyelitis VFU Veterinary Field Unit WB World Bank WHO World Health Organization WPV Wild Polio Virus

Independent evaluation of the Global Polio Eradication Initiative, Afghanistan, August 2009
�
� ��
ACKNOWLEDGEMENTS We would like to express our sincere appreciation for the excellent support, advice, and hospitality provided by the polio eradication initiative team at the central, regional, and provincial levels of Afghanistan. We were impressed with the level of organisation, scheduling, logistics and security achieved in such a challenging environment. We would particularly like to thank Dr Tahir Mir, Mr Mamdouh Samuel, and Mr Hamid Pason for helping to make our visit so productive and efficient.
We really appreciated having Dr. Najibullah Mojadidi work with us. His wise counsel was invaluable.
We recognise the extraordinary efforts made by the 54,000 people directly involved in the national polio eradication initiative and are genuinely impressed by the remarkable achievements. We appreciate that many of our meetings were on Fridays and Saturdays thus taking participants away from their families on these days of rest.
In a relatively short period of time, we were able to meet with polio eradication team-members from all seven regions and from 16 provinces. We realise that participation in these meetings required lengthy travel and valuable time away from work. We see this as a reflection of a high degree of commitment to polio eradication.
We extend our thanks to the many partners and stakeholders in the polio eradication initiative who took the time out to meet with us and share their knowledge and experience, including the MoPH, WHO, UNICEF, UNAMA, CIDA, ISAF, the World Bank, ICRC, USAID, OCHA, Ibn Sina, ADHS, and a number of NGOs in the Eastern Region (HealthNet, AMI, ARDC, BRAC, Hewad, CWSPA, and IMC).
Finally, we would like to express our sincere gratitude to our driver Habib, who was our ever reliable guide and friend from early each morning till late in the evening.
�
�
�

Independent evaluation of the Global Polio Eradication Initiative, Afghanistan, August 2009
�
� ��
EXECUTIVE SUMMARY
The polio eradication initiative (PEI) has achieved remarkable success in an increasingly challenging environment. For the majority of the Afghan population (84%), ongoing polio transmission has ceased. Indeed, the range of wild polio virus (WPV) has reduced from six of seven regions in 2000 to four regions in 2009, and 80-90% of all confirmed cases reported annually since 2006 have been from the Southern region.
There is a very high level of political commitment, coordination by partners, and technical quality of PEI team work. The high level of planning, review, and analysis of supplementary immunization activities (SIAs) is impressive. There is regular coordination with the PEI in Pakistan.
The high quality and coverage of acute flaccid paralysis (AFP) surveillance is being maintained, even in security-compromised areas. An independent evaluation in 2008 found that it is highly unlikely that polio cases are missed in the four regions assessed.
Despite the contraction of the area of polio transmission, the annual number of confirmed polio cases is not diminishing and appears to have remained static for the last four years: 18 cases reported during 2009 up until mid-August is consistent with the reported incidence in 2008. The reasons for this include non-health sector barriers, health system and service delivery barriers, community issues and potential technical barriers.
Insecurity poses the most significant non-health sector barrier to achieving high polio vaccination coverage throughout the country. The security situation is unstable, unpredictable, and threatened by a range of armed factions. Conflict-related and customary movements of large populations between Pakistan and Afghanistan and between provinces within the country have the potential to introduce WPV into areas where it has long been absent.
Changing policies of ISAF and Taliban, which focus not so much on pursuing the enemy but stabilising populations and enabling the provision of social services, offer both opportunities and threats. Direct provision of vaccination by uniformed personnel must be avoided and the neutrality of the PEI must be protected and promoted. High profile political endorsement of the polio eradication program may no longer be appropriate and, in some security-compromised provinces, may have a negative effect. All government associated initiatives, particularly successful ones, are potential targets for anti-government elements. Similarly, supplementary immunization activities (SIAs) should be de-linked from events that risk aligning the PEI with real or perceived political agendas; for example, UN Peace Day.
The main health system and service delivery barriers to achieving polio eradication include significant disruption of routine EPI services by the high number of SIAs; under-resourced health facilities, especially sub-centres; low salaries and incentives for vaccinators; inconsistent engagement in SIAs by NGOs contracted to implement the Basic Package of Health Services (BPHS); inability to conduct adequate supervision, monitoring and evaluation in insecure areas; inadequate EPI outreach; a confusing number of donor initiatives; replacement of the experienced NGO responsible for BPHS in Helmand Province; and lack of involvement of private practitioners in routine EPI services and SIAs.
The main community barriers include inadequate flexibility in accessing children safely. A number of examples of negotiation through different local intermediaries, including NGO district staff, hired negotiators, mullahs, and tribal elders, points to the success of discrete, local negotiations with anti-government elements through a

Independent evaluation of the Global Polio Eradication Initiative, Afghanistan, August 2009
�
� ��
flexible range of intermediaries. These examples also highlight that there is no single “right way” to engage with communities in security-compromised areas.
While there appears to be high community awareness and acceptance, polio vaccination is not perceived to be a high priority by most communities. Although male elders, mullahs, and teachers have been engaged to mobilise communities, greater efforts are needed to engage with individual male household heads to improve coverage of birth dose OPV and to ensure that mothers make all their children, including newborns, sleeping and sick children, available for SIAs. Excellent innovative strategies have been developed to mobilise women, however, their application may be confined to narrow geographic areas.
A number of technical barriers to polio eradication may warrant further investigation and include the relatively high proportion of polio cases in children who have received more than ten oral polio vaccine (OPV) doses; evidence that several recent polio cases occurred in children who were in contact with young adults recently returned from Pakistan (and who may have diminished immunity and be shedding WPV); lack of epidemiological evidence to continue the high number of SIAs in provinces where WPV is not circulating; and lack of an adequate explanation of the high male: female ratio of reported polio and non-polio AFP cases
RECOMMENDATIONS
Short-term/Immediate
Primary responsibility
1. Promote the neutrality of the polio program.
1.1 Reduce the visible involvement of political figures in vaccination campaigns.
Government of Afghanistan (GoA)
1.2 De-link the SIAs from associated events that might be used by anti-government elements to politicise the polio eradication initiative; for example, UN Peace Day.
United Nations, ISAF
1.3 Focus on discrete, local negotiations with anti-government elements through a flexible range of intermediaries.
GoA and PEI Country Partners
1.4 Finalise the draft standard operating procedures (SOP) for NATO/ISAF civil military engagement and disseminate the guidelines to field personnel.
NATO/ISAF, UN
2. Devolve responsibility for detailed district-by-district, cluster-by-cluster planning of SNIDs, with flexible dates and flexible local approaches to achieving access to communities.
2.1 Continue to expand the range of potential stakeholders in facilitating access to high-risk districts. There needs to be more management risk-taking through discrete negotiation with a range of intermediaries including NGO district staff, hired negotiators, mullahs, tribal elders, and district veterinarians, and direct negotiation with AGE, to gain access to contested areas.
Provincial and district PEI teams
2.2 Consider add-ons (other than Vitamin A) to sub-NIDs, such as other health and non-health goods seen as
National PEI Partners
Independent evaluation of the Global Polio Eradication Initiative, Afghanistan, August 2009
�
� ��
important by a community. Notice has to be taken of what each community expresses as its priorities. Add-ons could range from bed nets (for the biting nuisance of mosquitoes in areas where there is no malaria) or high-energy nutritious biscuits to vaccination for animal diseases or improved water supplies.
Provincial and district PEI teams
3. Strengthen program management
3.1 Urgently reconsider the criteria for selection of BPHS service providers and provide greater weight to previous field experience and ability to negotiate access to communities in insecure areas. This is an urgent priority in Helmand Province.
Ministry of Public Health (MOPH)
3.2 Tighten procedures for selecting cluster supervisors, volunteer vaccinator teams, mobilisers, and campaign monitors to strengthen the ability of the program to assess and validate performance at the community level.
Provincial and district PEI teams
3.3 Clarify the role and responsibilities of health posts and CHWs in routine EPI and SIAs but also of other basic health facilities, health personnel and other stakeholders.
MOPH
3.4 All categories of medical/nursing personnel in comprehensive and basic health centres and sub-centres should have vaccination included in their routine duty statements.
MOPH
3.5 Address human resources constraints, such as low salaries of vaccinators and low incentives of volunteers.
MOPH/UNICEF
3.6 Insist on a more effective engagement by NGOs implementing BPHS in both routine EPI services and SIAs. Consider including performance incentives based on survey-verified routine EPI coverage in NGO contracts.
MOPH/World Bank/USAID/EC
3.7 Add a routine EPI indicator to the Balanced Scorecard. MOPH/Johns
Hopkins
Medium Term
Primary Responsibility
4. Maintain the neutrality of the polio program.
4.1 While ISAF is a key stakeholder in some provinces/districts and should participate in planning and review meetings, continue to give careful consideration to the nature of their role in actual service delivery. Uniformed soldiers directly providing health services in security-compromised areas may fuel local suspicions that activities such as immunization are part of the
ISAF/UN

Independent evaluation of the Global Polio Eradication Initiative, Afghanistan, August 2009
�
� ��
military strategy and should be avoided.
5. Adjust the strategy of the polio program from regular, frequent national immunization days to focused SNIDs in high-risk areas.
The current high frequency of NIDs and SNIDs is leading to fatigue, inability to conduct detailed strategic planning in high-risk areas, disruption to routine EPI services in some fixed sites, and increasingly, resentment of the polio program by other mid-level health program managers.
We realise that reducing the number of NIDs in some other countries, without ensuring concomitant strengthening of routine EPI, has led to the re-appearance of WPV transmission; for example, in Punjab province of Pakistan. Thus, implementation of this recommendation would need to proceed with the utmost caution.
5.1 Reduce the number of NIDs starting in mid-2010 after a rigorous technical analysis, which includes modelling of likely immunity in each province, based on routine EPI coverage, SIA access and coverage, and exposure to migrants from areas where WPV is circulating. The six NIDs planned for 2009 should be conducted as scheduled.
National PEI Partners
5.2 Reduce the number of NIDs in a carefully phased manner; for example after careful analysis of likely immunity, a NID could be replaced by a SNID consisting of as many as 33 of the country’s 34 provinces. The excluded province(s) could be chosen on the basis of the performance of the relevant BPHS NGOs in achieving high coverage of OPV4 in 0-18 month olds.
Critical in this process is the performance of NGOs contracted to implement BPHS (see 3.6).
National PEI Partners
5.3 Continue to pilot and evaluate innovative methods of community mobilisation, such as “women’s courtyards”, district and sub-district level volley-ball, football and cricket games, and cluster jirgas of community elders while recognising that such strategies may only be acceptable within relatively narrow geographic areas.
UNICEF communication officers; provincial and district PEI teams
5.4 While men, such as mullahs, tribal elders and teachers, are already being engaged by the PEI to mobilise community support for SIAs, more attention should be targeted at individual male heads of households.
Provincial and district PEI teams
5.5 Consider piloting group education sessions in different regions for “expectant fathers” either at health facilities or traditional meeting places, such as mosques. A key message is the importance of the birth dose of OPV (and HBV), but could be combined with other important messages related to maternal and newborn health, such as early warning signs of labour and pregnancy complications, nutrition, and neonatal tetanus prevention.
Provincial and district PEI teams

Independent evaluation of the Global Polio Eradication Initiative, Afghanistan, August 2009
�
� �
5.6 Maintain intensive cross-border immunization and close coordination with PEI activities in Pakistan.
In addition to synchronising the timing of SIAs, synchronise communication strategies with Pakistan.
National PEI Partners; provincial and district PEI teams
5.7 Actively seek collaboration and coordination with the national animal health program, with its network of 625 veterinary field units, veterinarians, paravets, and basic veterinary workers. This collaboration should particularly involve the Afghanistan Veterinary Association (AVA) which has many members in the southern provinces.
MOPH, WHO, Ministry of Agriculture and Livestock, AVA
6. Increase base level of immunity in children through strengthened routine EPI services
6.1 Strengthen routine EPI services in all parts of the country to achieve 90% coverage by OPV4 through better resourcing of health centres at all levels, accelerated outreach (mini-SIAs), and more mobile teams.
MOPH, UNICEF, WHO, and BPHS NGOs
6.2 Standardise population denominators by conducting a technical workshop to review the current range of population estimates (between 26 and 33 million) and agree on a single figure for coverage of EPI and other health programs, such as antenatal care.
MOPH, WHO, UNICEF
6.3 The presentation of district EPI coverage data ideally should include comments on recent population movements if known to give an idea of recent changes in numerators and denominators.
Provincial and district PEI teams
6.4 Harmonise donor initiatives to strengthen routine outreach and mobile EPI services such as Sustainable Outreach Services (SOS), Reach Every District (RED), and Quick Impact Projects (QIP).
MOPH, WHO
7. Maintain the high quality of AFP surveillance
7.1 Expand surveillance in districts reporting fewer than 2 AFP cases per 100,000 per year by recruiting new community informants, such as Basic Veterinary Workers (BVW).
MOPH, WHO
7.2 Institute measures to improve the timeliness of case notification and investigation in order to reduce the number of inadequate cases and recall bias in the investigation.
MOPH, WHO
7.3 Strengthen the link between AFP surveillance and service provision in order to maintain commitment to the system. More generally, there is a need for feedback mechanisms for other vaccine preventable diseases (VPD) listed as nationally notifiable diseases, which is a way of ensuring that polio surveillance activities do not weaken other VPD surveillance.
MOPH, WHO
7.4 Strengthen coordination of AFP surveillance in Afghanistan and the border areas of Pakistan and with
MOPH, WHO

Independent evaluation of the Global Polio Eradication Initiative, Afghanistan, August 2009
�
� ��
other states bordering Afghanistan.
8. Strengthen program management.
8.1 Address resource constraints at the sub-centre level and clarify the responsibilities of nurses and midwives in immunization in the absence of designated vaccinators.
MOPH
8.2 Consider including under-five nutritional status and access to clean water and sanitation in the indicators used in the gap analysis to identify high-risk districts.
National PEI Partners
8.3 Involve private practitioners and non-health service providers in both routine EPI and SIAs.
Provincial and district PEI teams
8.4 Involve a broader range of stakeholders to enable adequate supervision and M&E of routine EPI and SIAs.
Provincial and district PEI teams
8.5 Develop communication strategies to improve the retention rate of routine immunization cards.
MOPH, UNICEF
8.6 Clarify referral procedures for AFP cases that require rehabilitation services. Currently, most provincial hospitals have inadequate physiotherapy capacity to provide effective care. The ICRC will cover the cost of treatment and transport to their six orthotic centres.
MOPH
Longer Term
9 Conduct operational research to clarify the following issues
9.1 – Polio infection in children with high number of OPV doses.
– Possible infection of some children by older children or adults returning from Pakistan.
– High male: female ratio of reported AFP cases.
WHO
10. As polio case numbers decline with improved immunization coverage, strengthen the quality of the review of ‘inadequate’ AFP cases.
10.1 This could be achieved by ensuring in-person review by members of the ERC, and/or strengthening the capacity of AFP focal points to collect sufficient clinical information for the ERC to make a firm diagnosis (e.g. videos of clinical examinations; access to medical investigations and imaging) and to follow-up cases for the requisite period.
MOPH, WHO
10.2 Although the reasons why cases were ‘inadequate’ are routinely reviewed within the current system, this practice may also need to be improved. In particular, lessons learned from individual cases about how to improve early detection should be shared with all surveillance system stakeholders.
MOPH, WHO

Independent evaluation of the Global Polio Eradication Initiative, Afghanistan, August 2009
�
� �
Map of Afghanistan

Independent evaluation of the Global Polio Eradication Initiative, Afghanistan, August 2009
�
� ��
CHAPTER 1. POLIO SITUATION IN AFGHANISTAN
Geographical distribution of polio cases, 2000-2009
For the majority of the Afghan population (84%), ongoing polio transmission has ceased. Indeed, the range of wild polio virus (WPV) has reduced from six of seven regions in 2000 to four regions in 2009, and 80-90% of all confirmed cases reported annually since 2006 have been from Southern region alone. Of these, three-quarters were detected in just 10 insecure districts within the region (Dihrawud, Kandahar, Maywand, Nad Ali, Panjwayi, Sangin, Shah Wali Kot, Spin Boldak, Tirin Kot, Musa Qala). Despite the contraction of the area of polio transmission, the annual number of confirmed polio cases is not diminishing and appears to have remained static for the last four years.
Confirmed cases of polio P1 and P3 [and compatible cases], 2000-09
Region 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
(Jan – Jul)
Central 3 - 1 - - - [1] - - - 1
Southern 11 9 [6] 5 [1] 3 [1] 3 [1] 9 [3] 28 [6] 15 [2] 25 [1] 15 [2]
South Eastern 5 1 [2] - 2 - - - - - -
North 1 - [1] - - - - - - - [1] -
North East - - [7] 2[4] - - [1] - 1 - - [1] -
Western 4 - 1 [1] 1 [2] - - 1 - 3 1
Eastern 8 1 [1] 1 1 [1] 1 - 1 2 3 1
Country 32 11 [17] 10 [6] 7 [4] 4 [2] 9 [4] 31 [6] 17 [2] 31 [3] 18 [2]
Confirmed (P1 and P3) and compatible cases of polio, 2000-09
22
10
5 42
5
29
6
25
14
10
1
5
3
2
4
2
11
6
4
17
4
6
2
3
2
2
6
4
0
5
10
15
20
25
30
35
40
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
(Jan-
Jul)
Nu
mb
er
of
case
s
P1 P3 Compatible
Polio serotypes and relationship of reported cases with cases in Pakistan
Three-quarters (76%) of viral isolates since 2006 have been serotype 1 (P1) and 24% serotype 3 (P3). Southern region and Farah province of Western region have ongoing transmission of indigenous P1 and P3 viruses. P1 isolates are part of the same cluster (A-3A) of the single remaining local lineage of P1 viruses in Afghanistan, although the degree of genetic variation of some of the isolates indicates prolonged, uninterrupted (and unidentified) circulation. These viruses are related to isolates from Pakistan (Balochistan and northern Sindh) and are indicative of the customary large scale population movements between these areas.

Independent evaluation of the Global Polio Eradication Initiative, Afghanistan, August 2009
�
� ��
The few cases occurring outside the southern polio transmission zone have also been linked with isolates from Pakistan. P3 viruses from Eastern children in 2008 are similar to viruses circulating in the North West Frontier Province (NWFP) (cluster B-1C), and the two P1 cases identified in Central and Eastern region in 2009 were genetically related to isolates in NWFP (cluster B-4A). Both of these latter cases were also loosely linked to young adult contacts with recent travel to this area of Pakistan.
No cases of paralysis from vaccine derived polio viruses have been detected to date.
Age, gender and vaccination status of polio cases
Except for 2000 and 2003, more than 75% of children diagnosed with polio have been aged less than 36 months. More boys than girls have been affected.
Since 2006, just over half the cases were among children who received fewer than the expected number of OPV doses (21% had not received a single dose; 34% were given between one and three doses). The remaining children were reportedly given four or more doses (3% received four doses; 21% between 5 and 10 doses; and 22% more than 10 doses), raising concerns about correct reporting of doses given, viability of the vaccine or other factors interfering with the development of immunity.
The social characteristics of cases from Southern region and Farah province of Herat in 2008-09 were examined. The majority were from fixed communities (95%) in rural areas (73%) distant from health facilities (average distance: 22km) and with no access to clean drinking water (85%).
Doses received, age and sex of confirmed cases of polio, 2000-09
Measurement 2000
(n=32) 2001
(n=11) 2002
(n=10) 2003 (n=7)
2004 (n=4)
2005 (n=9)
2006 (n=31)
2007 (n=17)
2008 (n=31)
2009 (n=18)
Median 2.0 4.0 7.0 6.0 6.0 9.0 4.0 2.0 3.0 1.0
Mean 2.7 4.8 5.8 6.4 8.3 9.4 6.1 4.4 5.7 6.5
Min 0 2 1 0 3 4 0 0 0 0
Max 9 8 12 14 18 17 28 16 17 25
Doses received
>3 19% 73% 70% 63% 75% 100% 52% 35% 48% 33%
Median 22.5 13.0 13.0 20.5 27.0 20.0 18.0 18.0 18.0 18.0
IQR 17-48 11-18 11-23 14-51 22-35 14-30 16-30 11-24 14-24 12-35
Mean 36.2 14.5 15.3 39.3 29.5 22.8 24.4 19.9 26.5 24.2
Min 9 7 1 7 16 10 8 3 9 8
Age of child
Max 148 24 30 120 48 42 120 72 96 54
Sex ratio (M:F) NA NA NA NA NA NA 1.2 2.4 1.8 1.2
Doses received and age of compatible cases of polio, 2001-09
Measurement 2001
(n=17) 2002 (n=6)
2003 (n=4)
2004 (n=2)
2005 (n=4)
2006 (n=6)
2007 (n=2)
2008 (n=3)
2009 (n=2)
Median 4.0 4.0 5.5 0.5 5.0 8.0 9.5 13.0 1.5
Mean 5.1 4.2 5.3 0.3 2.8 7.0 6.8 11.0 1.3
Min 0 2 0 0 2 2 4 9 1
Max 9 7 10 1 15 17 15 14 2
Doses received
>3 59% 67% 75% 0% 50% 83% 100% 100% 0%
Median 30.0 12.0 15.5 30.0 22.5 18.0 40.0 36.0 13.0
IQR 19-48 10-15 13-24 27-33 15-59 17-21 35-45 27-42 11-16
Mean 37.6 12.5 21.0 30.0 52.0 18.8 40.0 34.0 13.0
Min 5 8 13 24 7 14 30 18 8
Age of child
Max 96 18 40 36 156 24 50 48 18
Sex ratio (M:F) NA NA NA NA NA 1.5 1.0 0.5 1.0

Independent evaluation of the Global Polio Eradication Initiative, Afghanistan, August 2009
�
� ��
AFP surveillance data analysis, including gender and vaccination status
Compared to confirmed and compatible cases of polio, cases of non-polio AFP are older and have had more doses of OPV. Boys are more likely than girls to be diagnosed with paralysis caused by polio or a non-polio condition. It is not clear if this is due to reporting bias or real differences in risks, exposures, treatment or immunity.
Doses received and age of cases of non-polio AFP, 2006-09
Criteria 2006 (n=952) 2007 (n=1097) 2008 (n=1348) 2009 (n=676)
Mean 52 51 49 51
Median 36 36 36 36 Age of child
Range 0-179 0-179 0-179 0-177
Mean 12 12 13 13
Median 12 12 12 13 Doses of OPV received
Range 0-36 0-32 0-36 0-33
Sex of child Sex ratio (M:F) 1.4 1.3 1.2 1.3
Active surveillance in some regions (Western, Central) has declined in 2009 compared to previous years. Surveillance links with the border areas of Pakistan are weak and recommendations to strengthen links with central Asian states have not yet been implemented. It is unclear if the system could detect cases of polio in older children or young adults (see chapter 2 for more details about the surveillance system).
Vaccine associated paralytic poliomyelitis (VAPP)
The polio eradication initiative also reviews AFP cases to determine if there have been cases of VAPP. From 2001 to 2007 there were 3 cases with classic clinical signs of paralytic polio, recent vaccination with OPV and isolation of a Sabin-like virus from stools.
SIA coverage data by region/province/age/gender
Multiple methods are used to assess coverage of NIDs and SNIDs (see Chapter 2). Post campaign analysis in individual clusters in 2009 found that coverage exceeded 90% in the majority of surveyed clusters with the exception of those in the Northeast (mean of 19% of clusters) and North (24%) regions, and combined South region and Farah province of West region (50%).
Other assessments bear out these trends: finger mark surveys in markets in South/ Farah have been consistently below 80% in 2009 whereas other regions have recorded coverage above 90%; surveys of households around AFP cases confirm poor coverage in the South compared to elsewhere in the country; and southern children identified with non-polio AFP have received a lower number of total OPV doses relative to cases living in other parts of Afghanistan despite having had the highest number of SIAs conducted in 2009. Furthermore, some districts in the South have been inaccessible purportedly due to insecurity, and assessments of campaign quality have been unsupervised in parts of Southern region.
Routine EPI (OPV3) data by region/province/age/gender
Estimates of routine EPI coverage are uncertain because the target population is not precisely known (see chapter 2 for range of figures). Population movement may alter local targets and service providers may intentionally select lower denominators to inflate the coverage they achieved. For example, household surveys of EPI coverage around AFP cases, which are fairly randomly distributed throughout Afghanistan, generally show much lower coverage than reported by routine EPI providers and well below benchmark levels. Similarly, less than 80% of non-polio AFP cases among

Independent evaluation of the Global Polio Eradication Initiative, Afghanistan, August 2009
�
� ��
children aged 6-23 months detected in 2009 had received 3 or more doses through the routine EPI service in all regions except Central. In South region and Farah province less than a quarter of these children had been vaccinated 3 or more times. Differences in EPI data for doses given at the same age indicate that there are persistent problems with delivery of early doses of OPV – for instance, while the national coverage of BCG is high (87%), the birth dose of OPV, which was introduced in 2004, is poorly delivered (38%).
Comparison of routine EPI coverage from household surveys and administrative reports, 2006 vs 2009
2006 2009 Region Routine EPI coverage from
household surveys* OPV3 coverage from
routine EPI data Routine EPI coverage
from household surveys* OPV3 coverage from
routine EPI data
Central 36-85% 71% 57-89% 77%
Eastern 71-80% 87% 68-87% 110%
Northeast 36-62% 72% 57-67% 88%
Northern 37-80% 70% 32-76% 90%
South Eastern 23-66% 77% 47-63% 78%
Southern 5-56% 45% 6-38% 63%
Western 20-72% 77% 39-78% 80%
* Range in mean routine EPI coverage from surveys of households about AFP cases in provinces within region
Findings of Knowledge, Attitude and Practice (KAP) surveys
Community based KAP studies conducted throughout Afghanistan in 2008 found that while most people knew about the polio immunization campaign itself, fewer were aware that multiple doses of OPV were necessary (54%) or that OPV would prevent paralysis (43%). Even fewer respondents identified paralysis as a sign of polio infection (39%) or knew that there was no effective treatment (19%).
If a child did not receive OPV during an SIA, parents were asked the reason why. Frank refusals were uncommon and have been significantly reduced following social mobilisation activities. The most commonly cited reason was that the child was not home. Investigations are currently underway to assess if this was actually a passive means of refusal. Parents also refused because their child was sick, sleeping or newborn. In the South, West and Northeast, however, a significant proportion of missed doses were because the immunization team did not visit the house.
Summary
Indigenous WPV of both serotypes persists in the most insecure areas of southern Afghanistan (including Farah province of Western region) where immunity is low due to inadequate OPV coverage rates from routine EPI and SIAs. Sporadic cases in other regions with viruses related to isolates from neighbouring areas of Pakistan highlight the need to maintain surveillance and immunisation coverage.
The sizeable minority of cases who received more than four doses of OPV raises questions about why these children did not develop protective immunity. The reasons why more boys than girls have had confirmed and compatible polio and non-polio AFP remain unclear, but reporting bias needs to be excluded. Most cases are among children aged less than 36 months and in most cases reflect a failure of both routine EPI and SIAs.
Despite the limitations of the context, the surveillance system for AFP is highly sensitive and representative, and produces high quality, useful data. There remain issues of delayed reporting in remote and insecure communities limiting virological confirmation in a minority of cases.
Coverage data of SIAs and routine EPI from multiple sources show continual improvement from year to year in all regions except the South where access is

Independent evaluation of the Global Polio Eradication Initiative, Afghanistan, August 2009
�
� ��
restricted and verification is difficult. Administrative reports of EPI coverage are consistently higher than data derived from other sources and may be overestimating coverage particularly among younger children. In part, this is due to the inconsistent application of denominators to calculate routine coverage.
KAP studies have identified reasons for failure, some of which require additional qualitative investigation. Most are potentially modifiable with tailored pre-campaign social mobilisation activities and improved supervision and verification of team performances.
Wild PV in Afghanistan, 2009
B-4A
A-3D
A-3A
PEND
Data up to 1 Aug 09
NSL1
NSL3
Southern Region: only area with continued
indigenous WPV transmission
including Farah (A-3A lineage circulation
since 2007)
Eastern Region: cross-border
infection / re-infection from NWFP/
tribal areas
B-4A, B-1C & B-4A

Independent evaluation of the Global Polio Eradication Initiative, Afghanistan, August 2009
�
� ��
CHAPTER 2: KEY COMPONENTS OF POLIO PROGRAM
Main components of national strategy
The main elements of the polio eradication initiative (PEI) are:
• Strengthening routine EPI, including OPV4 dose at 18 months of age.
• Supplementary immunization activities (SIA), including national immunization days (NID) using trivalent vaccine, sub-national immunization days (SNID), using either trivalent or monovalent vaccine, and cross-border vaccination.
• Acute flaccid paralysis surveillance.
These activities also include cross-cutting activities, such as communication and coordination; monitoring, evaluation, and review.
National, provincial and district level structure and responsibilities
Oversight of SIAs is provided by a national EPI management team (NEMT), including MoPH, WHO, and UNICEF. There is also a national inter-sectoral committee (Polio Action Group), with review and coordination functions.
There is an equivalent team at the regional (REMT) and provincial (PEMT) levels, that includes WHO regional and provincial polio officers and UNICEF polio communication officers. There are regional and provincial coordination committees, the latter chaired by the provincial health director (PHD).
District coordinators (DC) are usually appointed by the NGO responsible for implementing the BPHS. DCs and district coordinating committees select cluster supervisors, who in turn select two volunteers at each sub-cluster (village) level. In high-risk districts, there are district and cluster communication focal points.
Frequency of NIDs and SNIDs
Six NIDs using trivalent vaccine and five SNIDs using either trivalent or monovalent vaccine have been planned for 2009. NIDs were conducted in January, March, May and July and are scheduled for October and November. In February, a SNID provided measles vaccine and OPV (mOPV1 in three southern provinces – Nimroz, Helmand, and Kandahar -- and mOPV3 in three eastern provinces – Nangahar, Kunar, and Laghman -- and one south-eastern province, Paktia). In April, a broader SNID using mOPV1 included all southern, eastern, and south-eastern provinces and Farah in the western region. There have also been “mop-up” campaigns comprising short-interval additional OPV doses.
A SNID in 13 southern districts is planned for September 13-15; however, the original plan to use mOPV1 may need to be revised since three cases of polio type 3 have been reported in Helmand and Kandahar during the past two months. A further SNID in southern, eastern, SE, provinces and Farah is scheduled for December.
Organization of NIDs and SNIDs
Provincial and district coordination committees oversee pre-campaign advocacy and social mobilization involving meetings with provincial and district governors and councils, shuras, and messages through the mass media. Each cluster supervisor supervises a varying number of village vaccinator teams (average five), depending on the geographic terrain, population density, and distances between villages. In many areas, Imams, community elders, and teachers have been engaged to mobilize communities. In several campaigns, there have been high-profile launches by the President, Ministers, provincial governors, and UN agency country representatives.

Independent evaluation of the Global Polio Eradication Initiative, Afghanistan, August 2009
�
� ��
NIDs represent a massive mobilization of human resources. Around 54,000 people were directly involved in the last campaign, including 46,500 volunteer vaccinators and 1,300 community mobilisers.
In April 2009, total responsibility for implementing SIAs was handed over to NGOs with BPHS contracts in seven districts of Helmand and Kandahar on a trial basis.
Detailed micro-planning has been promoted right down to the cluster and village levels. Cluster supervisors conduct monitoring, supervision of village teams, and daily performance reviews during campaign days and community mobilisers facilitate access by vaccinators to households. Post-campaign assessments are conducted by independent monitors (teachers, students, etc), including finger-marking surveys in markets of vaccination coverage and analyses of the reasons for missed children. Each monitor visits at least three team areas and at least ten families in each area.
Household Monitoring Form
Approaches to less accessible areas
High-risk districts have been identified using a gap analysis that includes a range of variables, including vaccine coverage, reported polio cases, and health service access. In these mostly security-compromised areas, a range of intermediaries have negotiated access to communities, including NGO and MOPH staff, hired negotiators, and non health sector personnel. Communication strategies have deliberately designed to target these high-risk districts. Further discussion on access can be found in chapter 3.
Communication and social mobilization
The communication strategy seeks to be evidence-based, targeted to address documented gaps in knowledge, promote immunization seeking behaviours and capitalize on opportunities. The strategy has been informed by KAP surveys, pilot studies, annual national reviews since 2006, regional meetings, and a high-level meeting in Geneva in 2007. The communication strategy is now firmly targeted towards high-risk populations in 13 high-risk southern districts. Communication
childre
n r
ep
ort
ed
livin
g in h
ou
se
childre
n r
ep
ort
ed
vaccin
ate
d
childre
n r
ep
ort
ed
livin
g in h
ou
se
childre
n r
ep
ort
ed
vaccin
ate
d
Tota
l
With F
inger
Mark
ing
Team
not
co
me
Ab
sent
New
born
Sic
k
Sle
ep
Gu
est
Refu
sal
Yes No
Rad
io
TV
Mu
llah
Teach
er
CH
W
Co
mm
un
ity
lead
er
Po
ste
rs
villa
ge w
om
en
No
ne
��������
����
��� ���������
�������������
������������� �
����������
�������������
������ �
����������
�������������
������������ �
�������
������������
������ �
����������
!"��
�����
#��� �������
��$����%���
��&������'�(�
)*�+�)�&
,-�./.0���
1���
2�.�
�!���
�3��
� ��� .��
�.4.��
5�
'� �
�678��9-:�
����
��9-:�
��);�
)<=�
�>?�6���
����@�
Market= M Travelling=T School=S Relative House=R Working in the field=F RHA�������B �
Household Monitoring Checklist - : C�-�D��E9.<��������� Round2��:
FGG.H��2��-����������IJ�������������0��������$��K�78
Ho
use N
o F
rom
Do
or
Mark
ing
2)L!��
nu
mb
er
fam
ilie
s liv
ing
in
ho
use
Vaccination teams going house-to-house 6M)%�����������*��.� yes � [ ] no ��� [ ] Mosque Announcements Made �����N����5O������"�������.P : yes � [ ] no ��� [ ]
Team Visited the area N�2���Q������-��RJ�,+�=��'�:�.P : yes � [ ] no��� [ ] Team No �2)L!��'�:� :________
Correct
Door
marking
��������IJ�S��������������N�����GG����2)!O�'�Specific
Address/Name of
Head Household
( �����'���IJ�90��T�����U.GG���)LGG���GG���GG.����������GG���GGIJ���G=�������IJ��������V�.0��.����J����������S��-�-��&������)L����W��+�GG=�U.��X� *�
Coverage % = (vaccinated/Total children in house)*100
����'�G�Y���� �����G��������G��������������Z2�����GG�����[���U.�
100�\�����GG �����GG���-:�������
After visiting the 10 houses go and find team/supervisor and check back of Tally sheets. How many of the children you
have listed as absent are recorded by the team on the back of tally sheet [_________ ] [________ % ] �DGG����G���]-��������
�������N���GG�^�3.��_G=���'G�:��2)G�J��GIJ�`�!a��)G*�+�)�&���CG�-���_G=�����<���������b%������2���C;�-������bQ�����4.��)�=�.���'�:��c.�d��<=����SQ�
( ������GG���GGIJ���GG�����������V�.0�.������������������G��S��-G�-��&������)�����W�+�GG=�������IJ��������
Missed Area: (If 3 or more houses are missed in 10 houses) Yes [ ] No [ ]
Cluster ________________ )<��� Village/Street. ______________________ �J��e��� Date________________ ��(L�
Province____________C.H� District ______________ @-��-� Name of Monitor _______________ f�<����� Agency/Organization__________ ��%���gd)�
% %
������ ������������
�����<���������GG��S��-��_=��
����!3����f�);�����e��<�
Communication data ��V��� ����3�����,_d��Children
seen by
monitor
Poorly Covered Area:(If 4 or more children are missed or coverage is less than 90%) Yes [ ] No [ ]
Total � !"� :
Children <5
years of age
How many of
them are <1
year?
���'���IJ-��>9�����������2)!O
Reasons for Missed
F��A���3�����e@<�
If t
he c
hild
is
absent
giv
e the
reaso
ns
accord
ing t
o t
he
cod
e
���2��)*
�+�)�&�f����h)�����
@3�-��2)=����@.�F.H�
MA�@���TA)i=S�����
How did you hear about NID?( Yes or No)�GG�3������.��!���.P
,-�GG.����GGIJ� d�9��9.�GG�H����

Independent evaluation of the Global Polio Eradication Initiative, Afghanistan, August 2009
�
� �
action plans are integrated into SIA micro-planning at the cluster and sub-cluster levels.
In addition to communicating through mass media (print, radio, and TV), innovative means have been used to communicate messages locally via sporting events, parades, and a women-to-women strategy through Women’s Courtyards. Jirgas, or traditional tribal assemblies, including mullahs, community elders, and teachers, have been convened to promote vaccination. A radio serial New Home New Life was developed in Pashtun through a partnership with the BBC Trust.
The effectiveness of various approaches in achieving high OPV coverage has been evaluated through random cluster surveys. For example, in Spin Boldak district of Kandahar, after implementing a targeted communications strategy in 2009, the refusal rate during SIAs declined from 34% in April to 23% in May to 14% in June.
In Kandahar City, SIA coverage in June 2009 was 99% in clusters where the women’s courtyard approach was used compared to 91% in other clusters.
Post-campaign assessments continue to find relatively high numbers of “absent children”, including newborns. There is some concern that these children represent “silent refusals” and will be the subject of ongoing qualitative research. Micro surveys have been planned over three rounds to gather qualitative data about “absent children”.
Cross-border activities and coordination with Pakistan
Around 1.5 million children are vaccinated with OPV annually at 11 border crossings. In 2008, more than 800,000 children were vaccinated at the Torkham border post. In areas that are traversed by semi-nomads, such as Khost and Farah, mapping of movements and focused social mobilisation has achieved high OPV coverage among these groups. NIDs in the two countries are synchronised, with Pakistan commencing their campaigns on Day 3 of the Afghan campaigns. There are frequent meetings between Afghan and Pakistan PEI teams, both centrally and locally. Chapter 5 discusses further the issue of population mobility.
Routine EPI system
The National EPI Department was established in October 2002. Routine vaccines include HBV and HiB. The program receives co-financing from GAVI, which has enabled expansion of the cold chain to accommodate 120 million doses of vaccine. There have been no stock-outs of EPI vaccines since 2006.
Routine EPI is largely provided through fixed sites – district hospitals, comprehensive and basic health centres, and sub-centres, the latter covering a catchment of
Women’s Courtyard in Jalalabad District, Nangahar Province
Independent evaluation of the Global Polio Eradication Initiative, Afghanistan, August 2009
�
� ���
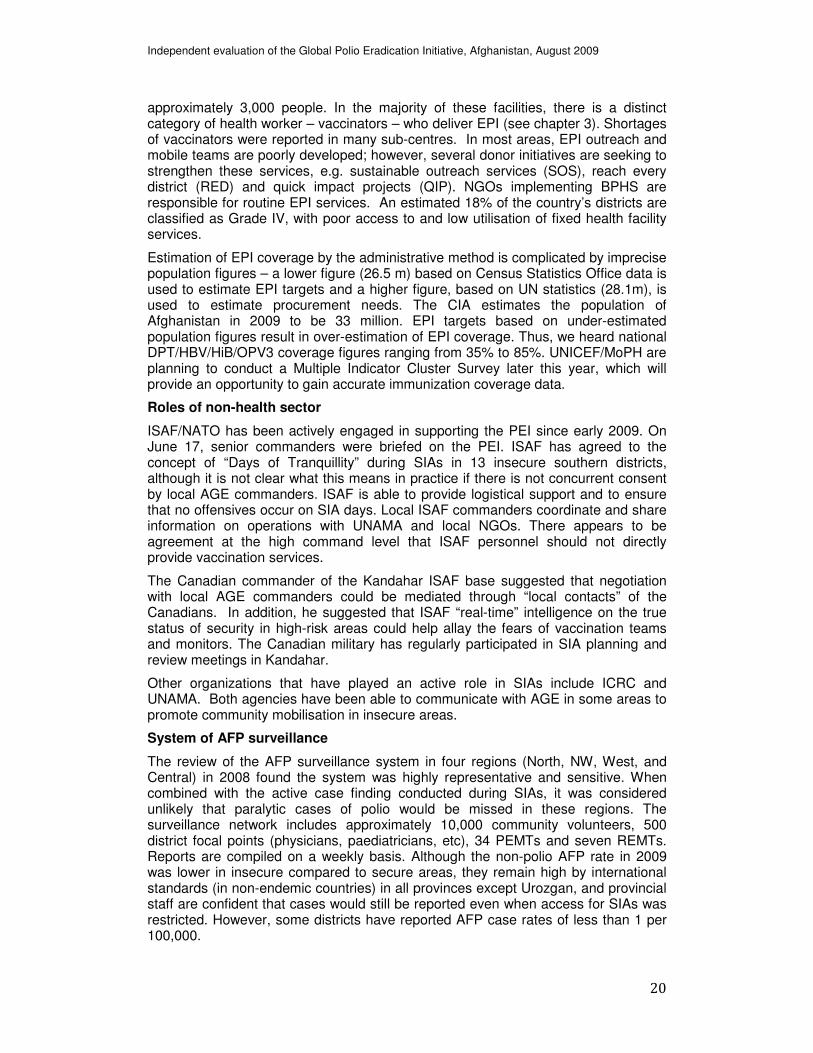
approximately 3,000 people. In the majority of these facilities, there is a distinct category of health worker – vaccinators – who deliver EPI (see chapter 3). Shortages of vaccinators were reported in many sub-centres. In most areas, EPI outreach and mobile teams are poorly developed; however, several donor initiatives are seeking to strengthen these services, e.g. sustainable outreach services (SOS), reach every district (RED) and quick impact projects (QIP). NGOs implementing BPHS are responsible for routine EPI services. An estimated 18% of the country’s districts are classified as Grade IV, with poor access to and low utilisation of fixed health facility services.
Estimation of EPI coverage by the administrative method is complicated by imprecise population figures – a lower figure (26.5 m) based on Census Statistics Office data is used to estimate EPI targets and a higher figure, based on UN statistics (28.1m), is used to estimate procurement needs. The CIA estimates the population of Afghanistan in 2009 to be 33 million. EPI targets based on under-estimated population figures result in over-estimation of EPI coverage. Thus, we heard national DPT/HBV/HiB/OPV3 coverage figures ranging from 35% to 85%. UNICEF/MoPH are planning to conduct a Multiple Indicator Cluster Survey later this year, which will provide an opportunity to gain accurate immunization coverage data.
Roles of non-health sector
ISAF/NATO has been actively engaged in supporting the PEI since early 2009. On June 17, senior commanders were briefed on the PEI. ISAF has agreed to the concept of “Days of Tranquillity” during SIAs in 13 insecure southern districts, although it is not clear what this means in practice if there is not concurrent consent by local AGE commanders. ISAF is able to provide logistical support and to ensure that no offensives occur on SIA days. Local ISAF commanders coordinate and share information on operations with UNAMA and local NGOs. There appears to be agreement at the high command level that ISAF personnel should not directly provide vaccination services.
The Canadian commander of the Kandahar ISAF base suggested that negotiation with local AGE commanders could be mediated through “local contacts” of the Canadians. In addition, he suggested that ISAF “real-time” intelligence on the true status of security in high-risk areas could help allay the fears of vaccination teams and monitors. The Canadian military has regularly participated in SIA planning and review meetings in Kandahar.
Other organizations that have played an active role in SIAs include ICRC and UNAMA. Both agencies have been able to communicate with AGE in some areas to promote community mobilisation in insecure areas.
System of AFP surveillance
The review of the AFP surveillance system in four regions (North, NW, West, and Central) in 2008 found the system was highly representative and sensitive. When combined with the active case finding conducted during SIAs, it was considered unlikely that paralytic cases of polio would be missed in these regions. The surveillance network includes approximately 10,000 community volunteers, 500 district focal points (physicians, paediatricians, etc), 34 PEMTs and seven REMTs. Reports are compiled on a weekly basis. Although the non-polio AFP rate in 2009 was lower in insecure compared to secure areas, they remain high by international standards (in non-endemic countries) in all provinces except Urozgan, and provincial staff are confident that cases would still be reported even when access for SIAs was restricted. However, some districts have reported AFP case rates of less than 1 per 100,000.

Independent evaluation of the Global Polio Eradication Initiative, Afghanistan, August 2009
�
� ��
Performance indicators in most provinces meet international benchmarks. The few exceptions are delays in case investigation and stool collection in remote and insecure sites. The higher than expected rate of detection of cases of AFP throughout Afghanistan can be partly explained by the deliberately liberal case definition adopted to maintain a highly sensitive system.1 It may also be due to a high burden of non-polio enteroviruses given the high percentage of EV isolated from stool specimens (and the high proportion of AFP cases attributed to Guillian Barre Syndrome2).
AFP cases where a stool specimen is collected more than 14 days after the onset of paralysis are reviewed by a regional panel and then referred to an expert review committee (ERC) in Kabul.
Afghanistan: Non-Polio AFP Rate by Province, 2007 to 2009
2009
2008
2007
0-0.991-1.99
2-4.99
5+
Data up to 6 Jun 09
��������������������������������������������������������
�Note that the surveillance review in 2008 found that health workers in Afghanistan may not apply the case definition for AFP as ‘liberally’ as health staff in other endemic countries. Additionally, they may be erroneously excluding cases initially reported as AFP.
��Note that the 2008 surveillance review team thought that there was an unusually high proportion of non-AFP cases attributed to Guillian Barre Syndrome.

Independent evaluation of the Global Polio Eradication Initiative, Afghanistan, August 2009
�
� ���
CHAPTER 3: HEALTH SYSTEM AND SERVICE DELIVERY FACTORS AFFECTING PROGRAM PERFORMANCE
The Afghan health system
Afghanistan has impressively developed its health system from a ministry run by mullahs under the Taliban pre-2002 to a system that has the capacity to address local and national priorities as well as international concerns such as the health MDGs. Equity and the right to health have been key values of the Ministry of Public Health (MoPH) since 2002. When considering polio eradication the current key health system challenges are to do with political leadership, roles and responsibilities and management style and practices.
Political leadership – There has been highly visible political leadership of the polio eradication initiative in Afghanistan. At different times, the President, Minister of Health, and governors of provinces have all taken turns to lead NIDs and sub-NIDs. This worked well in the past; it was the right thing to do then and it produced good results. However, now is the time to promote the neutrality of the program, and to distance it from any political, institutional, organisational, and military links. The health system has to adapt and take risks in developing different ways to achieve eradication such as building local trust, developing negotiating skills and reducing fear.
For a fuller discussion of the advantages and disadvantages of high profile political endorsement of polio campaigns see chapter 5.
Roles and responsibilities – Clarity and understanding about roles and responsibilities is a key health system characteristic. Even more so in the conflict affected context in Afghanistan where there is a multitude of local and international stakeholders, each determined to play a well-intentioned role in the PEI. The MoPH is in the driving seat and needs to play a leading role in defining the responsibilities of the many partners in the program.
Key international partners providing technical support are the World Health Organization (WHO) supporting AFP surveillance, SIAs, and routine EPI and UNICEF overseeing communications and some aspects of EPI such as the cold chain, vaccine procurement, and support for vaccinator per diems. While these aspects of the program are almost faultless, its management needs attention. The sound technical analysis, implementation and surveillance have tended to take precedence resulting in the relative neglect of key management factors hampering achievement of results. The following sub-section on management style and practices has further detail.
Funding is from a number of donors including Rotary International, the Canadian International Development Agency (CIDA), and the Japanese International Cooperation Agency. CIDA has taken a particular interest in implementation of the polio eradication program in Kandahar province where the Canadian military is playing a lead role in the fight against insurgency – see chapter 5 for a discussion of issues related to governments being both aid donors and combatants.
�
President Hamid Karzai and public health minister Dr. Muhammad Amen Fatimi launch the NID in July 2009

Independent evaluation of the Global Polio Eradication Initiative, Afghanistan, August 2009
�
� ���
As outlined in the section below on health service delivery, local and international NGOs are responsible for the delivery of the basic package of health services (BPHS) in much of the country through the mechanism of contracting out. EPI is a service in the package and so NGOs have a contractual responsibility to provide it. However, one of the key tools used to assess performance in delivering the BPHS, the balanced scorecard, does not have EPI as an indicator of quality.
Contracts for delivering basic health care mention the need to ‘support’ NIDs. This term ‘support’ is interpreted differently by different NGOs, from doing nothing to coordination and/or providing vehicles and vaccinators based in their health centres. According to many people met during this evaluation, especially in the Eastern Region, providing static health centre vaccinators for NIDs is distracting from routine provision of EPI. Where there are no vaccinators in a health facility (e.g. sub-centre) or they are absent, there seems to be some confusion about the role that nurses can play in immunization. Some managers think that nurses cannot give vaccines, oral and/or injection. This is a misconception that is resulting in lost opportunities.
There also seems to be some confusion about the role of health posts and community health workers (CHWs) in routine EPI and SIAs. While the BPHS states that EPI should be delivered by health posts this is interpreted by some as meaning that health posts should help with the delivery of EPI through outreach and mobile health services from basic health centres. Also, some see CHWs as being overwhelmed by tasks other than SIAs and do not involve them even for community mobilisation. The MoPH needs to clarify the role and responsibilities of basic health facilities, health personnel and other stakeholders in routine EPI and SIAs.
There are some districts where the delivery of BPHS and more specifically routine EPI and NIDs is not possible because of on-going insecurity. In some places such as Helmand province, private practitioners tend to remain in place, sometimes with their own pharmacies. Some are already involved in AFP surveillance. They could be contracted to provide EPI on a results basis. Ideally, they should also be contracted, perhaps through something like a voucher scheme, to provide other services such as the integrated management of childhood illness and antenatal, delivery, and newborn care. At present, such services are not affordable by the poor or they go into debt in order to pay. Supervision is a challenge but risks have to be taken if EPI and other services are to reach those in conflict affected areas.
Management style and practices - A key factor affecting performance is that the management of the PEI in some provinces has tended to adhere to one prescribed way of going about things. There has to be a change from such a culture as the reality is that in those areas affected by conflict, where there are the highest numbers of polio cases, the context varies district by district, community by community. For example, the acceptability of female vaccinators and female mobilisers can vary greatly within a relatively narrow geographic area.
There is no ‘one best way’ to manage the final phase of polio eradication. There needs to be much more flexibility combined with management risk-taking. Local level stakeholder analysis and negotiation needs to happen and practices adapted
�
Mobile health team supported by BRAC Nimroz Province

Independent evaluation of the Global Polio Eradication Initiative, Afghanistan, August 2009
�
� ���
accordingly. This calls for local leadership in determining approaches, in negotiation, and in managing personnel. Such leadership exists (although variable, particularly in the South; a challenge is to recognise and make the best use of it. In this way appropriate management action will be taken at the local level to address areas of need as defined by epidemiological, administrative, communication, and security data compiled at provincial and national levels.
Human resource management
There are a number of personnel management factors affecting performance. These range from fear and low morale among polio and other health workers to the attitudes about polio among middle level health managers, and from the supervision of NIDs and routine EPI to the recruitment of volunteers and payment of per diems.
Health personnel in conflict-affected provinces/districts have good reasons to be fearful. Insurgents often target them and their health facilities. ISAF forces have hit facilities and personnel with bombs or sniper fire by mistake. Health facilities have been taken over by insurgents, ISAF or the Afghan military. Communities may distrust health personnel for many reasons. Management of such fear is not easy. It needs a mix of approaches that help build trust between different stakeholders.
Some middle level health managers (not directly involved in the PEI), particularly doctors, are voicing scepticism about the need for such a high focus of attention on polio. They have never seen a polio case, have higher priorities, and resent the resources being spent on SIAs. They are therefore not supportive of the program. Such attitudes need to be better managed by MoPH and WHO, perhaps through regular well disseminated statements about the evidence for, and benefits of, continuing efforts towards polio eradication.
Experience in recent months in Helmand province has shown that better negotiation at the local level has allowed SNIDs in previously unreached communities including supervision by district personnel. Otherwise, there has been minimal supervision of routine EPI and other BPHS services in Helmand by provincial and central levels since 2004. This has impacted on an ability to validate that activities were conducted and assess their quality, and on the management of morale.
The challenges associated with supervision also play their role in the recruitment of volunteers and the payment of their per diems. Recruitment was variously described as haphazard, inefficient, and inappropriate for the prevailing culture. This is probably a reflection of the fact that so many SIAs are being undertaken with subsequent loss of management oversight. Finally, questions have been raised as to whether people being recruited for SIAs in some places are really those who could best contribute. The per diem is non-competitive with even the most basic of locally available day jobs, so SIAs do not always attract the best personnel.
Health service delivery in Afghanistan
Afghanistan developed its BPHS during 2002/3 and the third edition is currently being finalised. A complementary essential package of hospital services (EPHS) was developed in 2005. The main objective of the BPHS is to set priorities in health service delivery at each of the five levels of sub-provincial health facilities i.e. health post, sub-centre, basic health centre, comprehensive health centre, and district hospital. The services in the package are intended to have the greatest impact on mortality and morbidity. They address maternal and newborn health, child health and immunization, public nutrition, communicable diseases, mental health, disability and the supply of essential drugs. For child health and immunization the directive has always been to ensure the integrated management of childhood illness and the delivery of the EPI through routine, outreach and mobile services. In line with the

Independent evaluation of the Global Polio Eradication Initiative, Afghanistan, August 2009
�
� ���
2004 Constitution, Afghan health policies since 2005 have stated that immunization, among other activities in the BPHS, must be free to any citizen of Afghanistan.
Three donors fund implementation of the BPHS -- the World Bank, the European Commission (EC), and USAID. Implementation is nationwide through either the contracting out of basic health services to NGOs in about 80% of the country, or through government run services, the MoPH strengthening mechanism (MoPH-SM). Progress is being monitored through annual health service performance assessments and the use of a balanced scorecard.
Overall, many stakeholders see the BPHS and its implementation as a success story. However, challenges in the access to and quality of services are also acknowledged. Specific to polio eradication, these include:
Access – Political, security, cultural and geographical factors are all playing a role in affecting access by children to both routine EPI and SIAs. In insecure districts and provinces, particularly in the south of the country, the link between the government and the polio program is having a negative impact on access to routine EPI and during SIAs. Anything to do with government, particularly successful, is deemed worth targeting by the Taliban. Two polio workers were killed a couple of years ago in Kandahar province and in Helmand province the NGO implementing BPHS lost 12 staff between 2006 and 2008 due to insurgencies and/or targeting. Even finger marking as proof of polio vaccination can be interpreted by insurgents as having associated with the ‘enemy’.
It is well known that civilians suffer from both direct and indirect consequences of conflict. One of the indirect results is lack of access to health services. In Helmand province in 2007 there was thought to be no delivery of the BPHS in at least 50% of districts. Staff had fled for safer locations. Towards the end of 2008, about 90,000 children in three districts were not vaccinated against polio as the violence meant that routine EPI from fixed sites or through outreach or mobile services was not possible nor were SIAs. The situation has improved recently due to a mix of factors, such as (1) the ability of ISAF to now stay in those geographical areas that they free from Taliban control and (2) health and other personnel negotiate more effectively with the Taliban and/or community shura (traditional committees).
While geographical access has vastly improved since 2002, there are still some remote areas of the country where it can be 20 or more kilometres to the nearest health facility, such as was observed for polio cases in Southern region during 2008-09 (Chapter 1). And in winter, a health facility can be relatively close by but snow and ice make it inaccessible.
�

Independent evaluation of the Global Polio Eradication Initiative, Afghanistan, August 2009
�
� ���
Access to women and their children is a key cultural factor, especially in the conservative south of the country. Some communities will not allow women, even if wearing the burquah, to see, or be seen by a male stranger. So, if the latter is a vaccinator knocking on the door during an immunization day, access to a child inside will be denied. On the other hand, where there are only males staffing a health post or centre, women may well not attend for routine EPI. In addition, a newborn child is sometimes not seen by a stranger or named for the first 40 days of its life.
All these factors affect access to routine EPI whether provided in a health facility or through outreach or mobile services but also access during SIAs.
Quality – Factors affecting the quality of the EPI and SIAs include fear, fatigue, insufficient resources, and lack of -- or insufficient -- supervision and monitoring and evaluation. Living and working with fear is known to be affecting the quality of service delivery. Consultations may be rushed, services not provided at all for days and weeks, the contractual responsibility of NGOs to ‘support’ SIAs may be neglected or ignored, and there may be inadequate continuing education or training in seriously affected conflict areas.
Fatigue - Polio eradication fatigue affecting quality can be of at least four types. First, the fatigue associated with the on-going conflict and the difficulties of trying to deliver quality EPI and SIAs in dangerous environments. Second, the fatigue from too many vertical SIAs resulting in poor quality commitment and implementation of work, especially as the monetary incentives have risen very little over the past ten years. Additionally, the high priority given to SIAs has overridden the routine delivery of EPI services. Vaccinators in static health centres, for example, are being taken away from their routine work and could be spending about 15 days working on each SIA, seriously affecting the quality of EPI delivery.
A third cause of fatigue is associated with the proliferation of vertical donor initiatives directly or indirectly impacting on immunization. These include sustainable outreach services (SOS), reach every district (RED) and quick impact projects (QIPs). Finally, there is fatigue among some communities at having so many interventions to eradicate polio, particularly when many parents do not understand the need for multiple doses, when polio is a rare disease and vaccination is not viewed as a priority for communities.
To counter this it may be useful to consider add-ons to sub-NIDs, providing health or non-health goods seen as important by a community. Currently, vitamin A is also provided during many SIAs. While this is an important public health measure it is not something that communities perceive as important. Notice has to be taken of what each community expresses as its priorities. These could be provided in Helmand province through the quick impact project (QIP) scheme implemented by the provincial reconstruction team (PRT) and through the potential USAID QIP program for provinces in the south affected by conflict.
Lack of resources - Some basic health centres and sub-centres even in stable areas do not have adequate resources to ensure the maintenance of the cold chain.
Young women in a courtyard in Jalalabad

Independent evaluation of the Global Polio Eradication Initiative, Afghanistan, August 2009
�
� ���
In conflict affected areas, resources are often available but not in the right place at the right time because of difficulties in transporting supplies through front lines. This is affecting service quality.
The quality of the referral system for the treatment of cases of paralysis is weak. Staff either do not know where to refer cases e.g. to special ICRC centres or that the referral costs will be covered by the ICRC, therefore the referral is not taken up by the family because of the (hidden) costs involved. In addition, there are also inadequate resources at both district and health centre levels to provide rehabilitation services, despite disability being part of the BPHS. Moreover, most provincial hospitals lack physiotherapy capacity to provide these services.
Supervision and monitoring - The systems and capacity to supervise and to monitor and evaluate the quality of BPHS implementation and more specifically routine EPI and SIAs are in place. The problem is that in conflict affected districts they are not being used. For example, the balanced score card, one of the tools to evaluate the contracting out and in of health services, has not been used in Helmand and Kandahar since 2004. MoPH Kabul and provincial level staff are too afraid, or sometimes not allowed to travel to or within the provinces. In addition, the card lacks an indicator judging the quality of the EPI. This is a major omission.
Summary
During the post conflict period (2002-2004) Afghanistan put in place a sound health development framework. However, since 2005, progress in health has been slowing or has stalled in a number of districts and provinces. Both the health system and health services are currently functioning in a challenging context dominated by increasing insecurity and complex politics and power processes. The key health system and service delivery barriers to polio eradication are all to do with the approach to work and its management in such a complex context. As discussed in Chapter 2, there is sound technical analysis, implementation and surveillance. People know ‘what’ to do -- the challenge is ‘how’ to go about the work, especially in those areas of the country where insurgents are killing or intimidating people including health personnel.

Independent evaluation of the Global Polio Eradication Initiative, Afghanistan, August 2009
�
� ���
CHAPTER 4: COMMUNITY ISSUES AFFECTING PROGRAM PERFORMANCE
Communities as partners – The eradication program has a wealth of experience over the past few years of working at the community level. But it would seem that there has been insufficient analysis or discussion as to whether the ways of working in peaceful areas have relevance to areas where there is insecurity or conflict. In the sub-section on management style and practices in Chapter 3 there is mention that the management of the PEI has tended to adhere to one prescribed way of going about things. A reality is that in peaceful areas there may well be little genuine working ‘with’ communities. NIDs are frequently done by outsiders with something of a top-down approach. However, the complexities of delivering vaccines in times of insecurity necessitate a change.
There is no one ‘right way’ to engage with communities in security-compromised areas. But experience in Helmand province in the provision of water supplies and more recently in immunization is showing that constructive dialogue, listening and responding to community needs, priorities and cultural values and the development of trust are playing a key role. When communities are made to feel they are genuine partners, that their views are listened to, they are prepared to consider options to allow key interventions to be implemented. In each locality, it is important to involve both men and women in ways that reflect their local status and decision-making roles.
Men in the community are critical to enabling participation by women in SIAs. No man, whatever his political or tribal affiliation, wants to see his children or women ill or die. Compared with the rest of the country, communities in the south tend to be quite conservative. Men are usually the local intermediaries and they are crucial for the necessary dialogue with mullahs, elders or some other respected member(s) of society, no matter what political or other affiliation. The PEI has quite rightly worked with male mullahs and elders to mobilise community engagement. However, greater efforts should be made to convince male heads of households to enable access by vaccinators to their women and children. It is important to engage men while their wives are pregnant to ensure that they understand the importance of the birth dose of OPV so that they encourage women to take their newborn infants to health centres and to allow access in the home to newborns during SIAs.
Elderly women and mothers-in- law in the home also play a critical role in household decision making. It is therefore important to bring women into the communication loop in addition to targeting individual men and community shura. In some communities there may well be a respected woman - sometimes because of the status of her husband - who is allowed to go from house to house. This is thought to be the case of the wives of barbers in Helmand province but maybe not be the case in Kandahar. Having female volunteer vaccinators is acceptable in some areas of the country (e.g. Jalalabad) but not others (e.g. Khost).
Earlier, the value of listening and responding to community needs and priorities was mentioned. Demand for polio vaccination may well be non-existent because people may not have seen a case for years. Communities usually have other priorities, sometimes in the health sector, sometimes not. It may be useful therefore to provide an add-on to any sub-NID, something that responds to a stated priority. Again, this is going to vary from community to community and between SIAs in any one community. But add-ons could range from bed nets (for the biting nuisance of mosquitoes in areas where there is no malaria) to high-energy nutritious biscuits, from vaccination for animal diseases to improvement in water supplies. As mentioned in chapter 3, the Helmand PRT has funds from a QIP that could be spent on such add-ons. There may be something similar in Kandahar province. USAID is planning and hoping to have a QIP for all southern provinces affected by insecurity.

Independent evaluation of the Global Polio Eradication Initiative, Afghanistan, August 2009
�
� ��
Undertaking immunization at the community level
Planning for SIAs has to be done community by community to respond to local priorities, socio-cultural factors, and attitudes and beliefs about vaccination. In this way approaches to community mobilization for routine EPI and SIAs will be appropriate as will the role of women as vaccinators. Communities may well feel that they are being listened to with trust gradually developed on both sides. This can only be beneficial to the program.
The selection of volunteer vaccinators and of post-campaign monitors seems to be somewhat ad hoc. With so many NIDs and sub-NIDs, attention to detail can only be suffering. This selection is the responsibility of district coordinators, coordinating committees, and cluster supervisors. We were informed that in security-compromised areas, provincial PEI staff are unable to visit these districts and villages to verify the quality of performance of these community-level personnel.
For routine and/or sub-NIDs, bridging into non-secure areas could be via other actors. Mention was made in chapter 3 of using private practitioners. In communities the health of livestock is often a top priority. Where there is an animal health program, the links could be made with veterinary workers to combine activities, improving access and developing a cost-efficient approach. This is further developed in Chapter 5.
Post-campaign monitoring surveys consistently find low rates of refusals (2-3% of missed children during 2009); however, there continue to be high rates of absent children (40-50%) and missed newborns (20-30%). Some believe that these latter two categories may represent “silent refusals”; so more operational research is warranted on this issue.
Summary
The community level, including the pivotal role of certain men and older women, is the key to the successful eradication of polio in Afghanistan. In the (deteriorating) conflict context, it is only at the very local level that the means for immunization, supervision, surveillance and monitoring and evaluation can be negotiated and be made to happen. Individual men, such as village notables, elders, mullah, teachers, and CHWs, village ‘khala’ or midwives, and community shura often have the power to provide the humanitarian space necessary to deliver essential services. To successfully work with communities, they need to be considered as genuine partners, no matter what political or tribal affiliations may be held by individual members. And trust must be a core value, enabling successful implementation in insecure areas of the country.
�Female vaccinator during SIA

Independent evaluation of the Global Polio Eradication Initiative, Afghanistan, August 2009
�
� ���
CHAPTER 5: NON-HEALTH FACTORS AFFECTING PROGRAM PERFORMANCE
Security situation
Insecurity poses the most significant barrier to achieving high polio vaccination coverage throughout the country. The security situation is unstable, unpredictable, and threatened by a range of armed factions. The UN Department of Safety and Security (UNDSS) reported an increase in security incidents nationally from just over 600 in January 2009 to more than 1100 in June. Currently, the most security-compromised districts are in the southern provinces of Helmand, Kandahar, Urozgan, and Nimroz provinces and the western province of Farah, where insurgent forces are active. Security in previously stable areas has recently deteriorated due to insurgency, for example, in Kundoz province (NE), Kapisa and Worduk provinces (Central), Nuristan province, especially Barge Matal District (East), and Paktia and Ghazni provinces (SE). In the western province of Herat, insecurity is due to a mix of insurgency and criminality. All cases of polio reported since 2006 have occurred in the provinces marked red, orange, or yellow in the UN security map of August 2009.
Anti-government elements (AGE) do not comprise a homogeneous force under a single central command. Violence affecting access by vaccination teams to certain areas may be due to local tribal factions, organized criminals, and Taliban insurgents loyal to Mullah Omar. Some of these factions have been alienated by policies of local patronage. The letter of support for the polio eradication program issued by the Quetta Shura has been helpful in gaining access to certain insecure areas but not effective in other areas where additional negotiation is required with local AGE commanders.
Insecurity in the NWFP and Federally Administered Tribal Areas of Pakistan is also impacting on the PEI in eastern and SE Afghanistan. Inability to maintain high levels of vaccine coverage and effective AFP surveillance in these areas poses a threat of imported WPV, exacerbated by the movement into Afghanistan of people displaced by the conflict in Pakistan.
Inaccessible districts and proportion of target children inaccessible
While some districts in some other provinces are inaccessible during some SIAs, the southern region continues to suffer the most consistent security barriers. During the 12 SIAs between January 2008 and April 2009, six districts were inaccessible during nine or more rounds, seven during between five and eight rounds, and a further 16 between 1-4 rounds. Overall, around 17% of children were missed during this period. Post-campaign assessments have consistently found OPV coverage to be around 70% in SIAs in the southern region.
�

Independent evaluation of the Global Polio Eradication Initiative, Afghanistan, August 2009
�
� ��
Nevertheless, there has been some improvement since April 2009. The proportion of children living in inaccessible areas of the South declined from 16% in May to less than 5% in July. Post-campaign assessed OPV coverage increased from 70% in March to 78% in June. Although the proportion of monitored clusters reporting OPV coverage greater than 95% following SIAs in the South increased from 25% in April to 32% in June, the proportion with coverage less than 90% remained static at 52%, indicating that certain areas remain firmly inaccessible.
Examples of AGE-controlled districts where access has been achieved
Musa Qala and Nauzad districts of Helmand province (both high-risk) had been inaccessible since early 2008; however, local non-health sector negotiators have been able to ensure 100% access in the May and June campaigns. In AGE-controlled Nadeali district, which was inaccessible until May 2009, the NGO IbnSina, responsible for delivery of the BPHS in Helmand, was able to access the population in June through placing transit teams at the Lashkargah bridge.
Similarly, the NGO Bakhtar Development Network was able to negotiate access to Nawa District in Ghazni province in July after having been missed for 11 months. Other examples were provided to us from Eastern, SE and SW provinces of effective low-level negotiation to access high-risk areas through elders, mullahs, and local Taliban commanders. In one district of Herat, the Taliban commander reported back on the outcome of the campaign. In the highly insecure district of Bakwa in Farah province, separate negotiations have to be conducted with 14 different tribal groups to achieve access.
Implications of recent military policy changes
In 2009, a change in NATO/ISAF policy has seen a shift away from “pursuing the enemy” to “stabilising” populations and enabling the delivery of essential services. Military offensives will only target areas where it is feasible to maintain ongoing control. This policy shift is apparently mirrored by recent directives from the Quetta Shura to Taliban commanders; thus setting up a major battle to “win the hearts and minds of the people”.
This policy shift poses both significant opportunities and threats for the PEI. The opportunities consist of potentially sympathetic attitudes by local military commanders to requests for access and the temporary cessation of hostilities. The threats include (1) the potential direct delivery of vaccination and other health services by military forces and (2) combatants on both sides taking credit publicly for campaign achievements. For example, we were informed that in Bakwa district of Farah province, health facilities were being variously managed by ISAF, Afghan Defence Force, and Taliban personnel. Such a scenario might be repeated in Barge Matal district of Nuristan, which ISAF forces have recently occupied but Taliban forces continue to control access roads and service providers cannot enter.
On a positive note, we were re-assured by senior NATO/ISAF commanders that it was not their intention to directly deliver health services thereby risking alienating communities hostile to the Afghan Government and foreign military forces. A draft manual of Standard Operating Procedures (SOPs) for the support of social services in stabilised populations has been developed by NATO. However, it has not been
�

Independent evaluation of the Global Polio Eradication Initiative, Afghanistan, August 2009
�
� ���
finalised and its contents have not yet been widely disseminated in the field. We heard expressions of frustration by some ISAF commanders that if service providers were not available in a newly stabilised area “…how could I prevent my soldiers from stepping in and saving lives?”
Impact of high-profile endorsement of campaigns
It is legitimate to commend the strong endorsement of the PEI by the President, ministers, governors, and other political figures. We saw extensive evidence of a high level of community awareness and acceptance of polio vaccination. We were repeatedly told that negative attitudes towards vaccination and refusals were very rare. This must in part be attributed to the high level of political commitment.
However, we were also informed on many occasions, especially in the eastern and southern provinces that this high-profile endorsement of SIAs by politicians aligned with the Government of Afghanistan may be counter-productive in security-compromised areas.
We were told that the Taliban will oppose any program that they perceive to be important to the government. Thus, while continued commitment to the program at the highest level of government is important to ensure allocation of essential resources, it may now be timely to express that commitment privately.
Moreover, it is equally important that military officers, both Afghan and ISAF, not make public statements about the PEI that may lead the Taliban to oppose it merely because it is perceived to be a military priority. Some foreign governments have both military forces and aid programs in Afghanistan, some of which support the PEI. This raises the possibility that in areas controlled or influenced by anti-government elements, immunization activities may be perceived by community leaders to be intertwined with military operations. The neutrality of the polio program must be protected.
UN agency representatives should be cautious about publicly endorsing or taking credit for a program whose success could be perceived as one important element in maintaining popular support for the government. The planned linkage of the September SNID with UN Peace Day should be an internal matter only. Publicly linking the two events may further promote the perception that United Nations and Government of Afghanistan agendas are identical.
Population mobility
The transmission of WPV in Afghanistan is directly linked to circulation of WPV in Pakistan. There are two transmission corridors between the countries – Kandahar-Sindh and Eastern Region-Peshawar Valley (NWFP). Very high numbers of people cross the Pakistan-Afghanistan border in each direction for economic, social, and security reasons. For example, each day an average of 15,000 people cross the six border points between Nangahar and NWFP.
Most of this movement is for social and economic reasons and continues a long tradition of cross-border movement. In addition, a surge of violence in NWFP's
�
Torkham border post

Independent evaluation of the Global Polio Eradication Initiative, Afghanistan, August 2009
�
� ���
Swat, Buner and Lower Dir districts in 2009 forced more than 2 million people to flee their homes, some of whom may have entered Afghanistan. It is difficult to estimate the number of “true” refugees fleeing Pakistan’s violence because they cannot be differentiated from Afghan refugees returning after spending many years in Pakistan. We were told that 146 families from Balochistan recently arrived in Kabul, among whom 240 children were vaccinated with OPV.�
There are an estimated 270,000 internally displaced persons within Afghanistan; most have fled violence in the southern region of the country where WPV is circulating and OPV coverage rates are low. In addition, UNHCR estimates that since 2005, up to 50,000 refugee returnees have remained unable to return to areas of origin due to security constraints, and have sought shelter in spontaneous camps in eastern Afghanistan.
Role of Afghan Army and Police
As the key organs of maintaining peace and security, the Afghan Defence Force and Police can play an important role in ensuring an enabling environment to conduct vaccination campaigns. While awareness of PEI is high at the central level through inter-ministerial committees, we heard numerous stories of suspicion and obstruction at the local level. In areas that are only marginally secure, the movement of vaccinators from house to house has been misinterpreted in some areas, especially by the police. We heard that this has been particularly the case when female vaccinators move around in areas where the perpetrators of security threats have been disguised in burquas.
Potential role of integrating campaigns with animal health vaccination
The final stage of the PEI in Afghanistan could benefit from collaboration with partners whose programs share many of the same challenges but who also have networks that could complement the efforts being made to vaccinate children in hard-to-reach communities.�
There are approximately 625 Veterinary Field Units (VFU) nationwide. Currently, the Ministry of Agriculture maintains 150 of these units but will soon hand over 120 to the private sector. After this handover, more than 200 VFUs will be managed by the Afghanistan Veterinary Association (AVA), which has seven regional offices, including Kandahar, Nangahar, and Herat. We were informed that the AVA has a large number of members in the southern and eastern provinces.
A VFU is a small veterinary office or clinic located in a district to provide animal health care services to the farmers and animals of the nearby villages. VFU staff provide vaccination, de-worming, medical and surgical treatments to the district animals – at the VFU and in the field. They are also responsible for surveillance of animal diseases and train community-based Basic Veterinary Workers (BVW). The Ministry of Agriculture estimates that 40% of villages in the country have BVWs.
Vaccination of cattle against haemorrhagic septicaemia

Independent evaluation of the Global Polio Eradication Initiative, Afghanistan, August 2009
�
� ���
Vaccines against a wide range of animal diseases are procured by the AVA or the Dutch Committee for Afghanistan and maintained in a parallel cold chain down to the level of the VFU.
The similarities between the animal health program and the PEI are illustrated by a massive animal vaccination campaign undertaken during the summer in Badakhshan aiming to vaccinate millions of sheep, goats and other livestock brought to summer pastures in the Sheva Valley. This campaign required the mobilization of communities through village shura and the participation of numerous VHU staff, BVWs, and community mobilisers. Given the high priority accorded by rural communities to animal health and the extensive network of experienced district- and village-based vaccinators and volunteers, it may be useful to explore closer collaboration between the PEI and the animal vaccination program.
One example of how animal vaccination networks have been used to help achieve high coverage in NIDs is in Chad. This experience was described in a paper3, whose conclusions were as follows:
��������������������������������������������������������
��Schelling E, Bechir M, Ahmed MA, Wyss K, Randolph TF, Zinsstag J. Human and animal vaccination delivery to remote nomadic families, Chad. Emerg Infect Dis. 2007 Mar;13(3):373-9.�
Sustained vaccination programs are essential tools for both the public health and veterinary sectors. Combined human and livestock vaccination reduces operational costs of interventions requiring costly transportation and is adapted to livestock holders who highly value the approach that considers the health both of the family and of the animals that contribute importantly to their livelihood. In Chad, a common policy agreement between the two sectors on cooperation in rural zones should define a cost-sharing scheme. By optimizing the use of limited logistical and human resources, public health and veterinary services will be strengthened, especially at the district level, and, in turn, will be more prepared and operational in responding to endemic and epidemic diseases.

Independent evaluation of the Global Polio Eradication Initiative, Afghanistan, August 2009
�
� ���
CHAPTER 6. TECHNICAL ISSUES THAT MAY BE BARRIERS TO ERADICATION
Frequency and flexibility of SIAs
Less frequent but higher quality national campaigns could ensure greater coverage and minimize adverse impacts on routine EPI and other basic health services. Flexibility with the timing of sub-national immunisation days could improve micro-planning and negotiating access to populations in insecure areas including for post-campaign assessments.
A rigorous, technical assessment of the minimum number of NIDs necessary to ensure sufficient immunity among the target age group is required before any reduction can be recommended. The analysis could consist of modelling likely immunity in each province, based on routine EPI coverage, SIA access and coverage, and exposure to migration from areas where WPV is circulating. (The role of NIDs in strengthening AFP surveillance should not be forgotten.) A similar analysis could be conducted for SNIDs considering needs at provincial, district or even sub-district levels. The current gap analysis used to classify high-risk areas appears to be a comprehensive tool but could perhaps also include under-five nutritional status and access to clean water and sanitation.
Maintenance of high quality AFP surveillance and continued efforts to improve routine EPI are essential.
Confirmed cases of polio in children with more OPV doses than recommended
Since 2006, 43% of children with polio reportedly received 5 or more doses of OPV; 22% had received over 10 doses. For any vaccine with less than 100% efficacy, it is common that an increasing proportion of cases will be observed among vaccinated children as coverage increases and disease incidence declines. Nonetheless, a better understanding of the reason(s) why these children still developed paralytic polio could identify potentially modifiable factors.
Previous assessments of the cold chain have not revealed any major problems and it is unlikely that multiple batches of the vaccine were non-viable. On the other hand, validation of doses given is problematic in Afghanistan when only a minority of families retains their immunization cards for documentation of routine EPI antigens and parents consistently over-report doses received during SIAs.
Individual factors interfering with immunity may be important in Afghanistan. For instance, high circulation of non-polio enteroviruses has been cited as an impediment to developing protective immunity after vaccination in several states in India. The relatively high proportion of enteroviruses isolated in specimens from some provinces lends support to this theory. More tenuously, the listing of Guillian Barre syndrome as the most common cause of non-polio AFP in most regions could suggest the presence of enteric organisms (and/or respiratory pathogens) that could cause diarrhoea and interfere with immunizations. We did not review population nutritional data but malnutrition may also play a role in poor immune responses to vaccination in several settings. In some individuals, primary immunodeficiencies may explain paralytic polio despite many OPV doses, but cases are nonetheless sentinel indications of circulating wild virus.
Investigations of cases could go further in attempting to elucidate pertinent factors, particularly for cases occurring outside the Southern endemic area of transmission and will become more important as the number of annual cases declines.

Independent evaluation of the Global Polio Eradication Initiative, Afghanistan, August 2009
�
� ���
Possibility of transmission of WPV by infected adults with diminished immunity
Epidemiological investigations into the polio cases detected in Central region (Kapisa province) and Eastern region (Nuristan province) in 2009 found that the only pertinent contact was with young adults who had recently returned from Pakistan. While no cases of polio have been seen in older age groups in Afghanistan, sporadic cases in countries free of wild polio virus have shown the potential role of young adults in the spread of polio. For example, a young student from Pakistan was diagnosed with polio in Australia after returning from a vacation in his own country. In the absence of rapidly ensuring high coverage with OPV of each new birth cohort in Afghanistan and Pakistan, consideration could be given to investigating the role of infected young adults and identification of appropriate responses if required. For instance, compulsory travel vaccinations are standard for travel to some parts of the world and Saudia Arabia insists on OPV for all arrivals regardless of age. Other Gulf States are investigating the feasibility of following this course under the new international health regulations. Any recommendations would need to ensure that the current polio program in Afghanistan was not adversely affected by the introduction of new measures targeting older age groups.
Specificity and sensitivity of AFP surveillance and future review of “inadequate” AFP cases by ERC once incidence of confirmed polio cases declines to near zero
The quality of inclusion and exclusion of AFP cases throughout Afghanistan varies and stakeholders called for additional training of provincial focal points by the ERC. (Some stakeholders indicated that more female paediatricians would improve the quality of information collected on female cases.) Falsely excluding AFP cases without adequate examination was felt by the 2008 surveillance review team to be more of an issue than erroneous inclusions. So while the system may be sensitive in the first instance – through employment of a loose case definition and provision of incentives to reporters – cases of AFP may be missed through misclassification during the initial case investigation.
As case numbers decline with improved immunization coverage, the quality of the review of inadequate cases may need to be increased. For example, this could be achieved by ensuring in-person review by members of the ERC, and/or strengthening the capacity of AFP focal points to collect sufficient clinical information for the ERC to make a firm diagnosis (e.g. videos of clinical examinations; access to medical investigations and imaging) and to follow-up cases for the requisite period.
Although the reasons why cases were ‘inadequate’ are routinely reviewed within the current system, this practice may also need to be improved. In particular, lessons learned from individual cases about how to improve early detection should be shared with all surveillance system stakeholders.
High male: female ratio of reported AFP cases
For most provinces in Afghanistan more boys than girls are reported to the AFP surveillance system. The reason(s) why are not clear but may include reporting biases due to gender differences in health seeking behaviours, differential exposures due to the behaviour of boys and restrictions on movements of girls, different nature of medical treatment offered (e.g. injections causing traumatic neuritis) and different rates of primary immunodeficiencies (which in many settings more commonly affect males). Identification of relevant factors could improve the quality of surveillance and possibly even lead to interventions to reduce AFP cases.

Independent evaluation of the Global Polio Eradication Initiative, Afghanistan, August 2009
�
� ���
Sensitivity of surveillance of vaccine-associated paralysis
Data collection from AFP cases allows a retrospective assessment of probable cases of VAPP. This could be compared with an assessment of the expected number of cases for the number of doses delivered annually. If older age groups were targeted for OPV then this process of review may need to be conducted more regularly.

Independent evaluation of the Global Polio Eradication Initiative, Afghanistan, August 2009
�
� ���
CONCLUSIONS
1. The PEI has achieved remarkable success in an increasingly challenging environment. For the majority of the Afghan population (84%), ongoing polio transmission has ceased. Indeed, the range of wild polio virus has reduced from six of seven regions in 2000 to four regions in 2009, and 80-90% of all confirmed cases reported annually since 2006 have been from the Southern region. Of these, three-quarters were detected in just 10 insecure districts within the region (Dihrawud, Kandahar, Maywand, Nad Ali, Panjwayi, Sangin, Shah Wali Kot, Spin Boldak, Tirin Kot, Musa Qala).
2. There is a very high level of political commitment, coordination by partners, and
technical quality of PEI team work. The high level of planning, review, and analysis of SIAs is impressive. There is regular coordination with the PEI in Pakistan.
3. The high quality and coverage of AFP surveillance is being maintained, even in
security-compromised areas. An independent evaluation in 2008 found that it is highly unlikely that any polio cases are not being reported in four of the seven regions. Active surveillance in some regions (Western, Central) has declined in 2009 compared to previous years. Surveillance links with the border areas of Pakistan are weak and recommendations to strengthen links with central Asian states have not yet been implemented. It is unclear if the system could detect cases of polio in older children or young adults.
4. Despite the contraction of the area of polio transmission, the annual number of
confirmed polio cases is not diminishing and appears to have remained static for the last four years, with 18 cases reported during 2009 up until mid-August, consistent with the reported incidence in 2008. There is a relatively low routine coverage of OPV3/OPV4 nationally, although this is difficult to estimate by the administrative method because target figures are based on inaccurate population statistics.
5. Since 2007, security has been deteriorating in many previously stable provinces
(eg, Kapisa, Paktia, Kundoz, and Ghazni). The shared border with insecure areas of Pakistan, such as Kurram, Bajaur, North and South Waziristan, where vaccination and AFP surveillance may be sub-optimal poses a major threat of importation into eastern and southern provinces.
6. The main health system and health service barriers to achieving polio
eradication include the following factors:
• Significant disruption of routine EPI services by the high number of SIAs. This was highlighted particularly during discussions with health staff in the eastern and southern provinces, where there are almost monthly NIDs and SNIDs and where vaccinators from fixed facilities are mobilised for SIAs.
• Health facilities, especially sub-centres are often inadequately resourced to provide routine EPI services.
• Inconsistent understanding of responsibilities of sub-centre health staff; in some provinces, nurses and midwives are not expected to provide EPI in the absence of designated vaccinators.
• In a number of southern, south-eastern, and eastern provinces there is an inability to conduct adequate supervision, M&E, and data validation. This is

Independent evaluation of the Global Polio Eradication Initiative, Afghanistan, August 2009
�
� ��
due to a combination of inability to access insecure areas and a lack of trained supervisory staff.
• Inadequate EPI outreach and mobile teams as well as a confusing number of donor initiatives (eg, SOS, RED, Quick Impact, IMCPN).
• The replacement of the NGO responsible for BPHS in Helmand Province, IbnSina, which has many years of experience working in a conflict-affected environment, by an international NGO may have a negative impact on future SIAs.
• Private practitioners are not adequately involved in the provision of routine EPI services, especially those who continue to work in insecure areas.
• There is not a functional referral system for polio and other AFP cases to effective rehabilitation services, such as those provided by the ICRC.
• The Balanced Scorecard for monitoring BPHS lacks an indicator for EPI service delivery.
7. The main community barriers to achieving polio eradication include the following:
• A certain lack of flexibility in accessing children safely. There is no one “right way” to engage with communities in security-compromised areas, while there are a number of examples of negotiation through different local intermediaries, including NGO district staff, hired negotiators, mullahs, and tribal elders.
• Bridging into non-secure areas could be via a broader range of actors, eg, private practitioners and veterinary workers.
• In some areas, men may need to be the greater focus of community mobilisation to enable access to women and their children (especially newborns) and to allow women to move around as mobilisers and/or vaccinators.
• Recruitment of volunteers for SIAs was variously described as haphazard, inefficient, inappropriate for the prevailing culture and a means for friends to earn money. This is probably a reflection of the fact that so many SIAs are being undertaken with subsequent loss of management efficiency.
• The selection of volunteer vaccinators needs to reflect cultural and political realities, e.g. female vaccinators are acceptable in some areas (e.g. Nangahar) but not in others (e.g. Paktia).
• While we found little evidence of resistance to immunization and low refusal rates, demand for polio vaccination is relatively low because it is not perceived by communities to be a high priority. While vitamin A is given currently, it might be worth linking polio vaccination with delivery of services perceived to be of higher priority (e.g. nutrition, bednets, and animal vaccines).
8. The main PEI management barriers to success include the following:
• A key factor affecting performance is that the management of the PEI has tended to adhere to one prescribed way of going about things. There needs to be much more flexibility combined with management risk-taking.
• Issues related to human resource management (e.g., low salaries of vaccinators and incentives for volunteers) need to be addressed. There is
Independent evaluation of the Global Polio Eradication Initiative, Afghanistan, August 2009
�
� ���
also a need to manage fatigue associated with the difficulties of trying to deliver quality EPI and SIAs in dangerous environments, the high frequency of SIAs, and the proliferation of so many vertical donor initiatives directly or indirectly impacting on immunization.
• Some middle level health managers (not directly involved in the PEI), particularly doctors, are voicing scepticism about the need for such a high focus of attention on polio. They have never seen a polio case, have higher priorities, and resent the resources being spent on SIAs. They are therefore not supportive of the program.
• Lack of consistent understanding of roles of NGOs in the implementation of SIAs. The degree of engagement in SIAs by NGOs implementing the BPHS is highly variable and inconsistent.
9. The main coordination and communication barriers to success include:
• High profile political endorsement of the polio eradication program may no longer be appropriate and, in some security-compromised provinces, may have a negative effect. Anything to do with government, particularly successful, is deemed worth targeting by the Taliban.
• Moreover, it is equally important that military officers, both Afghan and ISAF, not make public statements about the PEI that may lead the Taliban to oppose it merely because it is perceived to be a military priority.
• UN agency representatives should be cautious about publicly endorsing or taking credit for a program whose success could be perceived as one important element in maintaining popular support for the government.
• Perceived fear by service providers is not always adequately addressed and could benefit from better information on the actual security situation in contested areas.
• Not all communication strategies may be appropriate in all high-risk areas (e.g., women’s courtyards may not be suitable in rural areas). A broad range of strategies appropriate for specific cultural groups (eg, women’s literacy classes that are being used in Kandahar and Helmand provinces to communicate vaccination messages) needs to be further trialled and implemented.
• Inadequate strategies to address the barriers to communication between all stakeholders (e.g., MOPH, NGOs, UN, ISAF, ICRC, AGE).
10. The main technical barriers to polio eradication include:
• Some polio cases have occurred in children who have received more than 10 OPV doses. The recent cases in Nuristan and Kapisa are examples of this issue.
• There is evidence that several recent polio cases occurred in children who had neither travelled to nor been in contact with children from endemic zones. However, they were in contact with older children or young adults who had returned from Pakistan (who may have diminished immunity).
• We found a lack of epidemiological evidence to continue the high number of SIAs in provinces where WPV is not circulating.
• We found a lack of evidence to explain the high male: female ratio of reported polio and non-polio AFP cases.

Independent evaluation of the Global Polio Eradication Initiative, Afghanistan, August 2009
�
� ��
11. The main non-health sector barriers to polio eradication include:
• Insecurity poses the most significant barrier to achieving high polio vaccination coverage throughout the country. The security situation is unstable, unpredictable, and threatened by a range of armed factions.
• Changing policies of ISAF and Taliban, which focus not so much on pursuing the enemy but stabilising populations and enabling the provision of social services. This change offers both opportunities and threats.
– Opportunities to provide access to service providers.
– Risk of direct service provision by combatants, which may be inconsistent with the basic humanitarian principles of neutrality, impartiality, and independence.
• The movement of large populations both between Pakistan and Afghanistan and between provinces within the country has the potential to introduce WPV into areas where it has long been absent. Population migration also constrains local program planning because the size of the target population during SIAs may be under-estimated.
• Possible contradiction between military and humanitarian objectives of major donor governments. A number of governments have both military forces and aid programs, some of which support the PEI. This raises the possibility that in areas controlled or influenced by anti-government elements, immunization activities may be perceived by community leaders to be intertwined with military operations. The neutrality of the polio program must be protected.
• Lack of active involvement of non-health ministries in the field. For example, there is minimal collaboration with the national network of animal health, including 625 veterinary field units and a large number of community-based basic veterinary workers. There is a need to communicate the purpose of immunization campaigns to all levels of the Afghan military and police.
�
Internally displaced persons living in Kabul

Independent evaluation of the Global Polio Eradication Initiative, Afghanistan, August 2009
�
� ���
Annex 1: Persons Met
Government of the Islamic Republic of Afghanistan
Dr. Najibullah Mojadidi, Senior Advisor on Health & Education to the President
Ministry of Public Health, Kabul
H.E. Dr. Muhammad Amen Fatimi, Minister of Health
Dr Nadera Hayat Burhani, Deputy Minister, Health Care Services and Promotion
Dr Faizullah Kakar, Deputy Minister of Health, Technical Affairs
Dr Ahmad Shah Salehi, Director Health Economics and Financing Directorate
Dr Mohammad Taufiq Mashal, Director, Preventive Medicine and Primary Health Care
Dr Agha Gul Dost, Director EPI
Dr. Gula Khan, medical officer
Dr. Nafi, medical officer
Ministry of Agriculture, Kabul
Dr Mohammad Anwar Sadaf, Acting Director General, Livestock and Animal Health
United Nations Assistance Mission in Afghanistan
Mr Kai Eide, UN Special Representative in Afghanistan
World Health Organization, Kabul
Mr. Peter J.Graaff, Country Representative
Dr. Tahir Pervaiz Mir, Polio Medical Officer
Dr. Ali Ahmad Zahid, Polio surveillance
Dr. Rohullah Habib
Mr Mamdouh Samuel
Mr Mohammad Zahid
Mr Haroon, Data analyst
Mr Hamid Pason
UNICEF, Kabul
Ms Catherine Mbengue, Country Representative
Gopal Sharma, Deputy Representative
Ms Savita Naqvi, Chief of Program Communication
Dr Zahra Mohammed, EPI Specialist
Dr. Saboor Bahrami, EPI Officer
Dr. Attai Mohammad, Health Officer, Central Region
Mr.Juma Din, Security Officer

Independent evaluation of the Global Polio Eradication Initiative, Afghanistan, August 2009
�
� ���
International Security Assistance Force
Rear-Admiral Matthieu Borsboom, Deputy Chief of Staff Stability, Kabul
Brigadier-General Jonathan Vance, Commander, Canadian Forces, Kandahar
Colonel Richard Dixon, Civil-Military Cooperation. RC South
Lt Col Dr Jo Palmer, Health Advisor, RC South, Task Force Helmand
World Bank, Kabul
Kees Kostermans, Lead Public Health Specialist, South Asia, Washington DC
Tekabe A Belay, Senior Economist (Health), Washington DC
Dr G Sayeed, Public Health Specialist, Kabul Office
International Committee of the Red Cross
Reto Stocker, Head of Delegation
Dr Jose Bastos, Health Coordinator
Office for the Coordination of Humanitarian Affairs
Lucio Melandri, Humanitarian Affairs Officer, Civil-Military Coordination
Canadian Embassy/Canadian International Development Agency
Cindy Termorshuizen, Deputy Head of Mission
Rifah Khan, Second Secretary, Development.
Cindy McAlpine, Kandahar.
Chantal Ruel, Kandahar.
United States Agency for International Development
Tara Milani, Health Development Officer
Bradley Bessire, Director, Office of Social Sector Development
Faiz Mohammad, Health Team Leader
Japanese International Cooperation Agency
Sachiko Goto, Assistant Resident Representative
Afghan Health and Development Services, Kabul
Dr Mohammad Fareed, Deputy Director
Ibn-e-Sina, Kabul
Dr Mirza Jan, Country Director
Dr Faiz Mohammad Atif, Director of Operations
Eastern Region
HE Mohammad Aleem Isehaq Zai, Deputy Governor, Nangahar Province
Dr. Khushal Zaman, WHO medical officer
Prakash Tuladhar, UNICEF Chief of Office Eastern Region
Dr Abdul Wahidi, Health and Nutrition Specialist Eastern Region
Dr. Ajmal Pardis, Nangahar provincial health director

Independent evaluation of the Global Polio Eradication Initiative, Afghanistan, August 2009
�
� ���
Dr. Hakim Jan, regional polio officer
Dr. Safeer Mohammad, assistant regional polio officer
Dr. Abdul Basir, Nangahar provincial polio officer
Dr. Asad Ullah Fazli, Kunar provincial health director
Dr. Mohammad Sardar, Kunar provincial polio officer
Dr. Wahid Azizi��Kunar provincial polio officer
Dr. Latif, Laghman provincial health director
Dr. Shafiq Ullah, provincial polio officer, HealthNet
Dr Attanullah, Aide Medicale Internationale (AMI)
Dr Arsallah, EPI Focal Point, AMI
Dr Abdul Raziq, AMI Kunar
Dr A. Ouyu, Afghan Reconstruction and Development Centre (ARDC)
Dr Safiullah, Medical Supervisor, ARDC
Dr Jaleed Ali, Project Manager, BRAC Afghanistan
Dr Noor Gossan, Medical Coordinator, BRAC
Dr Ezatullah, Hewad
Dr Haznat Ali Hamad, Church World Service – Pakistan/Afghanistan (CWSPA)
Dr M. Daud, International Medical Corps (IMC)
Dr Gul Asquer, IMC
Southern Region��
HE Tooryalai Wesa, Kandahar Provincial Governor
Dr. Abdikarim Asseir, PMO, Kandahar
Helene Kadi, Chief UNICEF Field Office, Southern Region
Sardar Popal, Acting Polio Communication Officer, Southern Region
Dr. Javed Iqbal, PMO
Dr. Rahmatullah Kamwak
Dr. Najibullah Zafarzay (RPO)
Dr. Hamidullah (ARPO)
Dr. Mohammad Essa (Kandahar provincial polio officer)
Dr. Abdul Qayoom Pokhla (Kandahar provincial health director)
Independent evaluation of the Global Polio Eradication Initiative, Afghanistan, August 2009
�
� ���
Haji Nazar Mohammad (REMT)
Dr. Fazal Rahman
Dr. Asif Gul (Nimroz PPO)
Dr. Noor Ahmad Shirzad (Nimroz PHD)
Mr. Sayed Askar Shah (Nimroz PEMT)
Dr. Un-Sul Haq Rahimi (BARAK)
Dr. Abdul Rahman Jawad (Urozgan PPO)
Dr. Khan Agha Maikhil (Urozgan PHD)
Mr. Saif-u-din (Urozgan PEMT)
Dr. Ajab Noor (Zabul AHDS)
Dr. Mohammad Tahir (Zabul PPO)
Dr. Gul Ahmad (Zabul PHD)
Mr. Adam Khan (Zabul PEMT)
Dr. Fazal Rahman (Zabul Ibn Seena)
South Eastern Region
Dr. Shamsher Ali, STC, WHO
DR. Naik Mohammad, RPO WHO
Dr Abdul Khalil, UNICEF Health specialist, South Eastern Region
Dr. Nadir Noori, PHD, Paktia
Mr. Habib Ullah, PEMT, Paktia
North/North-East Regions
Dr.Magdi Sharaf, WHO medical officer
Dr.Abdul Rahman Ghafoory, Regional Polio Officer
Basir Ahmad Afzali, REMT
Marwais Rabie, PHD, Balkh province
Dr. Wahid Bhurt, Medical Officer, Kunduz
Dr. Saboor Sozan, REMT Kunduz
Dr. Abdul Ahad Hakimi
Dr. Assadullah Naimi, APW Fiazabad
Dr. Aziz Ullah Safar, PHD, Kunduz

Independent evaluation of the Global Polio Eradication Initiative, Afghanistan, August 2009
�
� ���
Western Region
Dr. Hakim Sadiq, Regional Polio Officer
Dr Gholam Said Rashed, PHD Heart
Dr Wahid Rahmani, REMT
Iskandar Hena, Medical Officer
Dr Rabbani Wardak, UNICEF Health and Nutrition specialist
Central Region
Dr Pirzad, National Expert Review Committee (ERC)
Dr Ahmoni, ERC.
Dr Shoban, Chair of ERC.
Dr. Ghulam Raziq Sidiqi, Regional Polio Officer
Dr. Fazel Karim, PHD, Kabul
Dr. Naseer Tahiri, PEMT Kabul
Michael and WHO driver, Habib

Independent evaluation of the Global Polio Eradication Initiative, Afghanistan, August 2009
�
� ���
Annex 2: Schedule
August 6 (Thursday)
• Arrival 19.30 (Dr.Tahir, Mamdouh, Savita to meet mission at Kabul Airport)
• Security Briefing 20.30 at Hotel Heetal Plaza by Mr.Juma Din UNICEF Security Officer
August 7 (Friday)
• Activity 1: Plenary Session at 9.00 AM-11.00 AM: Venue Main Conference Hall WHO
o PE Operation and Service Delivery System Dr. Dost o Polio Situation update and Epidemiology Dr.Tahir Mir o National Update on Polio Communication Dr. Nafi / Savita o Country Update on routine EPI services Dr Dost
Participants: 5 participants each from Central, North and North East Region (PHD, REMT, WHO M.O, RPO,UNICEF Officer), Country Team Members (Dr.Tahir, Dr.Dost, Dr.Gula Khan, Dr.Nafi, Dr.Roohulla, Dr.Ali Ahmed, Dr.Brando, Dr.Zara, Dr Bahrami,Savita), WR & UNICEF Representatives.
• Activity 2: Group Discussions by each Region 11.00 to 16.30 Venue is Polio Meeting Room
o Central Region Team (PHD Kabul, REMT, WHO M,O, RPO C.R, UNCEF C.R) 11.00-12-30
o North East Region Team (PHD Kunduz, REMT, WHO M.O, RPO N.E, UNICEF N.E) 13.30-15.00
o Northern Region Team (PHD Mazar, REMT, WHO M.O, RPO North, UNICEF North) 15.00-16.30
August 8 (Saturday)
• Activity 1: Meeting members of National Expert Review Committee (ERC) 8.30-09.45 am
o Chairperson & members of National Expert Review Committee
• Activity 2: Meeting with Dr. Nadera Hayat Burhani, Deputy Minster of Public Health 10.00-11.00 am at office of Minister
• Activity 3: Meeting with Ibn-e-Sina (BPHS NGO) at 14.00 to 15.00 at Ibn-e-Sina (Arzan Qeemat)
• Activity 4: Meeting with Dr Sayed & Kees in World Bank 1530 - 1630
• Activity 5: Meeting with NATO / ISAF at ISAF HQ 1800 - 1900
August 9 (Sunday)
• Activity 1: Travel to Jalalabad by USAID flight 0900
• Activity 2: Field visit to Sub district B (Behsud): Briefing on Polio vaccination Campaign and Communication initiative by the local teams 9.30 – 10.30
• Activity 3: Plenary Session: Venue MoPH 10.30 am – 11.30 am o Regional Polio update and Epidemiology - WHO o Update on Communication Initiative - UNICEF
• Activity 4: Group Discussions: o Session I: All PHDs and PEMTs: Venue MoPH 11.30 AM – 12.30 PM

Independent evaluation of the Global Polio Eradication Initiative, Afghanistan, August 2009
�
� ���
Participants: All PHDs and PEMTs (Nangarhar, Kunar, Laghman & Nuristan), WHO M.O, RPO, UNICEF
• Activity 5: Meeting with Governor of Nangarhar followed by Lunch 12.30 PM– 2.00 PM
• Activity 6: Meeting with BPHS NGO at HNI office (HNI, BRAC, ARCS and CWS are responsible for the health service delivery in Nangarhar, AMI in Laghman and Kunar and IMC in Nuristan) 2.00 – 3.30 PM
• Activity 7: Security briefing by the UNDSS ER UNICEF Office 3.30 – 4.00 PM
• Group Discussions: (continued) o Session II: UNICEF Group: Venue UNICEF 4.00 - PM – 5.00 PM o Session III: WHO Group: Venue WHO 5.00 – PM - 6.00 PM
• Dinner at WFP Guest House with Regional heads of UN agencies (UNDSS, UNICEF, UNAMA, OCHA, WFP, UNHCR and ICRC) 8.00 PM August 10 (Monday)
• Activity 1: Departure Jalalabad 0730 & reaching Kabul by UNHAS flight at 0930
• Activity 2: Plenary Session with Southern Region Team at 1030 to 1200 Venue WHO Main conference room Kabul
o Regional Polio update and Epidemiology By WHO M.O o Update on Polio Communication in SR By UNICEF
Participants: All PHDs and PEMTS from South (Zabul, Kandahar, Helmand, Uruzgan, Nimroz, Farah), WHO South (M.Os, NHC, RPO, ARPO, 06 PPOs), UNICEF South (Head of the office, 03 PPCOs, RPPCO , FP Farah)
• Activity 3: Group Discussions 1300 to 1600 Venue Polio meeting room WHO Office
o Group 1: All PHDs and PEMTs, 1300 - 1400 o Group 2: UNICEF Group 1400 - 1500 o Group 3: WHO Group 1500 - 1600
August 11 (Tuesday)
• Activity 01: Travel to Kandahar by CIDA flight around 0700
• Activity 02: Meeting at KAF (0900 -1130) o Meeting with TFK, o Meeting with ROCK, o Meeting CIDA
• Activity 3: Travel back to Kabul by CIDA flight
• Activity 4: Meeting with AHDS (BPHS NGO) at 14.30 to 15.30 at AHDS (Shahre Nao)
o Country office will be requested to invite Kandahar office In-charge in this meeting.
• Activity 5: Meeting with DFID (responsible person for Helmand) at 16.00 to 17.00 at DFID office. Status TBC
August 12 (Wednesday)
• Activity 1: Meeting with ICRC at 08.00-09.00 at ICRC Office

Independent evaluation of the Global Polio Eradication Initiative, Afghanistan, August 2009
�
� ��
• Activity 2: Meeting with SRSG at 0930-1000 at SRSG Office
• Activity 3: Meeting with USAID at 11.00- 12.00 at USAID Office
• Activity 4: Meeting with Animal Health Department, Ministry of Agriculture (Mike) at 11.00 – 12.00
• Activity 5: Meeting with Ibn-e-Sina (BPHS NGO) at LUNCH at WHO
• Activity 6: Group Discussions by Region 13.30 to 16.30 Venue is Polio Meeting Room
o South-Eastern Region Team (PHD Gardez, REMT, WHO M,O, RPO S.E, UNCEF S.E) 13.30 - 15-00
o Western Region Team (PHD Herat, REMT, WHO M.O, RPO West, UNICEF West) 15.00 - 16.30
August 13 (Thursday)
• Activity 1: De-briefing Meeting with H.E Minister of Public Health & Polio Partners at 1330 - 1530 at MoPH
• Activity 2: Meeting with CIDA at 1600 -1630 at Canadian Embassy
August 14 (Friday)
Informal meeting & discussion with WHO and UNICEF Polio Team at 1000
August 15 (Saturday)
• Departure: Kabul to Dubai by UNHAS
Eastern Region UN security team with Ben and Stephanie