Embed Size (px)
Citation preview
Tuberculosis Control Plan v4
Policy No: IC20 Version: 4.0
Name of Policy: Tuberculosis Policy – Prevention and Control
Effective From: 28/11/2014
Date Ratified 17/10/2014 Ratified Infection Prevention & Control Committee Review Date 01/10/2016 Sponsor Director of Nursing, Midwifery and Quality Expiry Date 16/10/2017 Withdrawn Date
This policy supersedes all previous issues.

Tuberculosis Control Plan v4 2
Version Control
Version Release Author/Reviewer Ratified by/Authorised
by
Date Changes (Please identify page
no.) 1.0
July 2000
July 2000
2.0
03/11/2008 Dr S J Hudson Mrs V Atkinson
RIDP Strategic Committee
Central Team
November 2008
January 2009
3.0
13/10/2011 Dr S J Hudson
Infection Prevention &
Control Committee
28 September
2011
3.1 28/08/2012 Dr S J Hudson/ Mrs L Flude
Infection Prevention &
Control Committee
27/07/2012 Audit revision
4.0 28/11/2014 Dr S J Hudson Infection Prevention &
Control Committee
17/10/2014 Contacts updated Duties – P5 no Head of Risk Management P9 6.6 To reflect NICE Guidance P10 6.8 To reflect NICE Guidance P10 6.9 To reflect NICE Guidance Occupational Health Screening – P18 6.29 Diagnosis of TB in a staff member – updated

Tuberculosis Control Plan v4 3
CONTENTS Page(s)
1. Introduction 5 2. Scope 5 3. Aims 5 4. Duties – roles and responsibilities 5 ‐ 6 5. Definition of terms 7 6. Policy – identification of cases 7 ‐ 19 6.1 Admission to hospital 7 6.2 Risk Assessment 8 6.3 Multi‐Drug Resistant TB (MDR TB) 8 6.4 Isolation 9 6.5 Categories of Isolation Accommodation may be used 9 6.6 Patient Care in Isolation Rooms 9 6.7 Visitors 9 ‐ 10 6.8 Transfers 10 6.9 Discontinuation of Isolation 10 6.10 Discharge from Trust Premises 11 6.11 Patients with Drug Sensitive TB 11 6.12 Patients with MDR TB 11 6.13 Patients Who Seek Their Own Discharge 11 6.14 Death of a Patient and Post Mortem 12 6.15 Arrangements for Follow‐up and Outpatient Visits in General 12 6.16 Inter Current Interventions 12 6.17 Contact Tracing 12 6.18 Identification of Contacts 13 6.19 Action to be taken on the Diagnosis of Smear‐Positive Pulmonary Tuberculosis in a Patient 13 6.19.1 Patient Contacts 13 6.19.2 Staff Contacts 14 ‐ 15 6.20 Contacts in Outpatient Clinics 15 6.21 How Far Back to Trace Contacts 15 6.22 Priorities in Contact Tracing 15 6.23 Infection Prevention and Control in Healthcare Facilities 15 ‐ 16 6.24 Staff Protections – Risk Assessment Prior to Clinical Procedures 16 6.25 Patient Focused Hygiene Methods (cough hygiene) 16 6.26 Personal Respiratory Protection 16 6.27 Environmental/Engineering Controls 17 6.28 Notification 18 6.29 Protection of Staff Against Tuberculosis 18 6.30 BCG Vaccination Programme 19 6.31 Prevention and Management of Infection in Patients With Autoimmune Rheumatic Disease 19

Tuberculosis Control Plan v4 4
7. Education and training 19 8. Equality and diversity 20 9. Monitoring compliance 20 Appendix 1: References 21 Appendix 2: Isolation Decisions For Patients With Suspected Respiratory TB 22 Appendix 3: Negative Pressure Facilities 23 Useful contacts: Rachel Andrews/Carole MaClean Nurse Specialist TB Control Low Fell Clinic
Beacon Lough Gateshead Mobile: 07977 284427/07717878850 Low Fell Clinic: 0191 2834660
Health Protection Team North East Public Health England Centre Floor 2, Citygate Gallowgate Newcastle upon Tyne NE1 4WH Tel: 0300 303 8596 option 1

Tuberculosis Control Plan v4 5
Tuberculosis Policy – Prevention and Control
1. Introduction
This policy for use within the Trust has been drawn up taking into account relevant guidance and published work to reduce the burden of tuberculosis through the early identification, treatment and follow up for all people with suspected tuberculosis and their contacts, together with immunisation and screening programmes. (See appendix 1) It recognises that it is the responsibility of the Consultant in Communicable Disease Control (CCDC) to take the lead in establishing the collaborative arrangements necessary for the prevention of the spread of tuberculosis. Individual patient management and chemotherapy are outside the scope of this policy.
2. Scope
This policy applies to all healthcare professionals within Gateshead Health NHS Foundation Trust.
3. Aim
The aim of the policy is to reduce to patients and staff the risk of transmission of tuberculosis by early identification of suspected and known cases of tuberculosis. It outlines arrangements for identification, treatment and follow up for all people with suspected tuberculosis and their contacts, together with immunisation and screening programmes.
4. Duties – roles and responsibilities
The Chief Executive has responsibility for ensuring the Trust has robust and effective Infection and Prevention Control Policies The Directors of Infection Prevention and Control have executive responsibility for Infection Prevention Control and oversee Infection and Prevention Control activity via the Infection and Prevention Control Committee. Consultant Microbiologist will give advice against this policy and liaise directly with Public Health England. Will notify Occupational Health of any trust staff or inpatient cases of infective pulmonary tuberculosis. Head of Infection Prevention and Control ‐ will give advice against this policy. Ensure this policy is updated every two years or in line with current national guidance. The Infection and Prevention Control Team –will give advice and support on management and policy interpretation. (See 9 Monitoring and compliance). The Infection Prevention and Control Committee is responsible for the ratification of Trust wide infection prevention and control policies, procedures, and guidance, providing advice and support on the implementation of policies and monitoring the progress of the annual

Tuberculosis Control Plan v4 6
infection control programme. All incidents involving TB should be reviewed by the Trust IPCC and included in the Annual Report. Managers will ensure that all staff are aware of and follow this policy and are aware of their own roles and responsibilities to ensure safe practice. Health care professionals will ensure that this policy is followed to ensure safe practice. Suspected cross infection investigations will be coordinated by the relevant Trust manager. Lead Tuberculosis Physician (locally agreed physician) with particular expertise and responsibility for treating tuberculosis patients, who works together with a TB nurse specialist. For adults the physician is a respiratory physician and a paediatrician for children. The Communicable Disease Control Doctor (CCDC), PHE takes the lead in establishing the collaborative arrangements necessary for the prevention of the spread of infections. In the event of an outbreak/suspected outbreak an Outbreak Control Team (OCT) should be formed to manage the outbreak. This will be led by the Trust. The CCDC or deputy will be part of the OCT. There is a specific requirement in RIDDOR for employers to report tuberculosis infection in employees when they have been working with persons, animals, human or animal remains or any other material which might be a source of infection. All incidents should be reviewed by the Trust Infection Prevention and Control Committee (IPCC) and included in the Annual Report. Trust Communications Officer is responsible for producing media related messages related to any Trust incident. They will be given essential background information via the relevant manager and IPCT to assist in a collaborative statement which will be approved by the Chief executive officer or their deputy. Trust Clinical Staff are responsible for adherence to IPC policy with particular attention to IC 2 Personal Protective Equipment in Clinical Practice and IC 6 Isolation Policy. TB should be suspected in anyone, regardless of HIV status, with a cough without other cause lasting more than 3 weeks with or without weight loss, anorexia, fever, night sweats or haemoptysis When TB is suspected in a patient the medical microbiologist should always be informed (contactable on a 24 hour basis via QEH switchboard) in order that discussion can take place with the team responsible for the patients care about appropriate accommodation and rapid diagnostic tests. The matron/ward departmental manager will draw up a list of staff and patient contacts in conjunction with the Infection Prevention & Control Team and send it directly to Occupational Health. See also 6.19.2 Staff Contacts. All patients with suspected or confirmed tuberculosis should be referred to the locally designated tuberculosis physicians. See contents page for useful contacts. Tuberculosis in HIV infected patients and also in patients in whom the risk of Multi Drug Resistant TB (MDRTB) is high or identified will be managed in association with Infectious

Tuberculosis Control Plan v4 7
Disease Physicians. Patients will usually be transferred to ward 19 Royal Victoria Infirmary for further management.
5. Definition of terms
Infectious tuberculosis: active tuberculous disease which presents a risk of transmission of infection to others. For most practical purposes, this means sputum smear‐positive pulmonary tuberculosis ie pulmonary tuberculosis in which acid fast bacilli (AFB) are present on direct microscopy of sputum. Disease of other parts of the respiratory tract or the oral cavity, though rare, must also be considered infectious. Factors which increase infectiousness include the presence of cavities in the lungs, laryngeal tuberculosis and cough. More stringent criteria need to be applied if the patient is in contact with immunocompromised individuals or has drug‐resistant disease, because of the more serious consequences for the recipient if transmission of infection occurs. For infection control purposes, therefore, patients can be divided into: Infectious: i. all new patients with suspected or confirmed pulmonary or other respiratory tract tuberculosis until the sputum status is established or the diagnosis is excluded. At least three consecutive smears of good quality sputum specimens taken on different days must be examined before concluding a patient with pulmonary disease is not infectious. ii those with confirmed sputum smear‐positive pulmonary disease; iii those with active disease of the bronchi or larynx; Potentially infectious: Those with sputum smear‐negative pulmonary disease in whom one or more cultures are positive, or the culture results are not yet know.
6. Policy – identification of cases
6.1 Admission to hospital
• Patients do not necessarily require admission to hospital either for investigation or initiation of treatment for TB.
• People with drug sensitive tuberculosis can be treated at home if this does not put others at risk and suitable arrangements can be made for supervising therapy.
• Out‐patient management is not appropriate for infectious or potentially
infectious patients if they live in a hostel or other communal establishment, unless suitable accommodation and support services are available.
Tuberculosis Control Plan v4 8
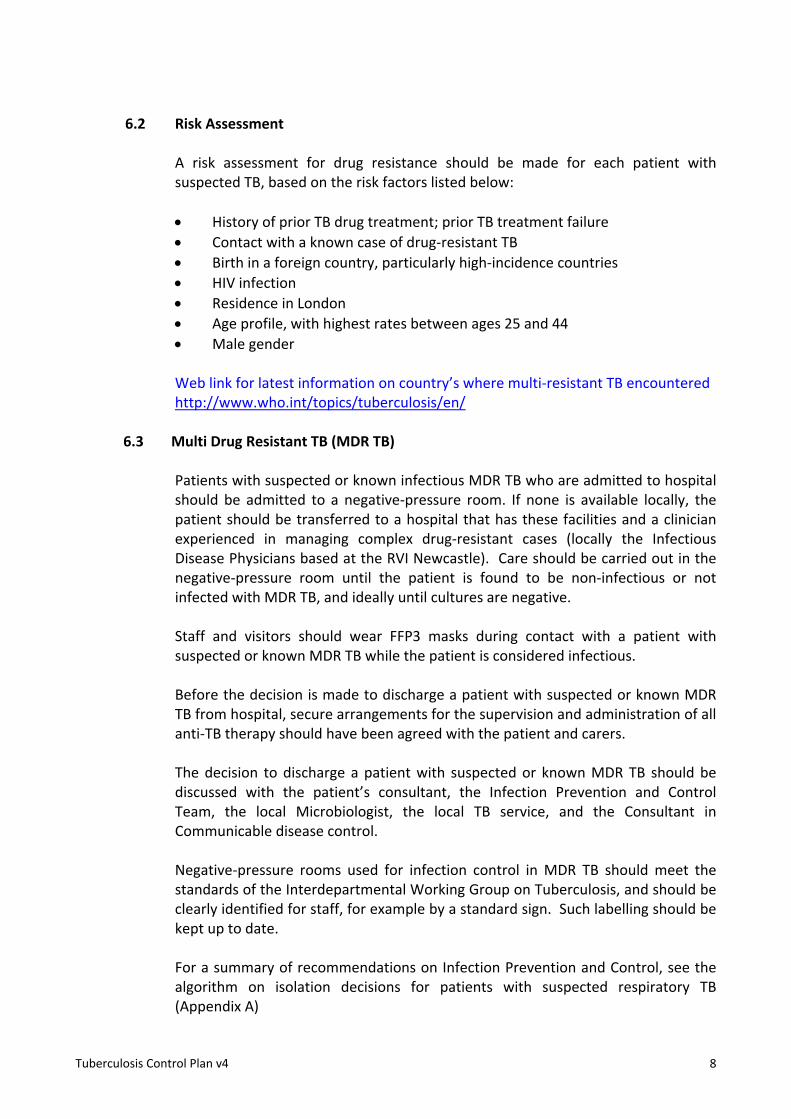
6.2 Risk Assessment
A risk assessment for drug resistance should be made for each patient with suspected TB, based on the risk factors listed below:
• History of prior TB drug treatment; prior TB treatment failure • Contact with a known case of drug‐resistant TB • Birth in a foreign country, particularly high‐incidence countries • HIV infection • Residence in London • Age profile, with highest rates between ages 25 and 44 • Male gender
Web link for latest information on country’s where multi‐resistant TB encountered http://www.who.int/topics/tuberculosis/en/
6.3 Multi Drug Resistant TB (MDR TB)
Patients with suspected or known infectious MDR TB who are admitted to hospital should be admitted to a negative‐pressure room. If none is available locally, the patient should be transferred to a hospital that has these facilities and a clinician experienced in managing complex drug‐resistant cases (locally the Infectious Disease Physicians based at the RVI Newcastle). Care should be carried out in the negative‐pressure room until the patient is found to be non‐infectious or not infected with MDR TB, and ideally until cultures are negative.
Staff and visitors should wear FFP3 masks during contact with a patient with suspected or known MDR TB while the patient is considered infectious. Before the decision is made to discharge a patient with suspected or known MDR TB from hospital, secure arrangements for the supervision and administration of all anti‐TB therapy should have been agreed with the patient and carers. The decision to discharge a patient with suspected or known MDR TB should be discussed with the patient’s consultant, the Infection Prevention and Control Team, the local Microbiologist, the local TB service, and the Consultant in Communicable disease control.
Negative‐pressure rooms used for infection control in MDR TB should meet the standards of the Interdepartmental Working Group on Tuberculosis, and should be clearly identified for staff, for example by a standard sign. Such labelling should be kept up to date.
For a summary of recommendations on Infection Prevention and Control, see the algorithm on isolation decisions for patients with suspected respiratory TB (Appendix A)

Tuberculosis Control Plan v4 9
6.4 Isolation
Patients with respiratory TB should be separated from immunocompromised patients, either by admission to a single room on a separate ward, or to a negative‐pressure room on the same ward.
6.5 Categories of isolation accommodation may be used:
• Negative‐pressure single room with automatically controlled air pressure • Single rooms that are not negative pressure. • See Infection and Control Policy No 6 ‐ Isolation Policy for further advice
regarding respiratory isolation
6.6 Patient care in isolation rooms
• Patients require careful explanation about the need for them and their visitors to adhere to infection control measures. Document advice and information provided in the nursing care plan. Once a diagnosis has been confirmed complete a Known Infection/Colonisation record and place in front of medical notes behind patient demographics.
• Healthcare workers caring for people with TB should comply with standard infection control precautions. Wearing of masks is indicated when:
• MDR TB is suspected (FFP3 masks must be used while the patient is
considered infectious).
• Aerosol‐ generating procedures are being performed (FFP 3 masks must be used)
• When such personal respiratory protective equipment is used, the reason
should be explained to the person with TB. Aerosol‐generating procedures such as bronchoscopy, sputum induction or nebuliser treatment should be carried out in an appropriately engineered and ventilated area for:
• All patients with HIV regardless of whether a diagnosis of TB has been
considered
• All patients in whom TB is considered a possible diagnosis, in any setting. Patients need to understand that they must remain in the room with the door closed during the period that they are infectious.
• Patients may need support during withdrawal from addictive substances.
6.7 Visitors

Tuberculosis Control Plan v4 10
• Only those persons, including small children who have been in close contact with the patient before the diagnosis should be allowed to visit patients with smear positive pulmonary disease whilst they are in isolation. Close contacts should have been screened first and active tuberculosis excluded. When masks are being recommended to visitors to an individual patient, visitors need to be instructed on how to use them and comply with other infection control procedures. A guide to wearing PPE must be displayed in the patients’ antechamber or if in a standard single room beside the patients’ washbasin. See Infection Prevention and Control Policies No 2 – Personal Protective Equipment and policy No. 6 ‐ Isolation Policy for detailed guidance.
• People visiting patients with tuberculosis may themselves be
immunocompromised due to their own medical conditions which could make them more susceptible to infection. In conjunction with the physician in charge staff will need to assess the likely risk of transmission from the index case and advise an immunocompromised visitor not to visit. All staff and visitors must report to the nurse in charge when first visiting the patient as per Infection Prevention and Control Policy No.6 ‐ Isolation Policy.
6.8 Transfers
• Ambulance staff ‐ transporting an infectious patient ‐ need sufficient information for their own protection while maintaining patient confidentiality. Infectious patients with uncontrolled cough should wear a surgical mask Patients with known infectious MDR‐TB should wear FFP masks.
• Other transfers ‐ patients may also need to be transferred to other wards,
departments or hospitals whilst infectious. Each case will need to be managed on an individual basis ensuring that receiving staff receive sufficient information for their own protection, whilst maintaining patient confidentiality. Patients needing transfer outwith their room are advised to wear a surgical mask if breathing spontaneously. Ventilated patients do not require further protection. Staff do not need to wear an FFP3 mask when patients are transferred.
6.9 Discontinuation of Isolation
The decision to discontinue isolation, or to transfer a patient to a lower category of isolation is a clinical one, made by the clinician and medical microbiologist taking into account the factors outlined above in the original assessment, i.e. the infectiousness of the patient, susceptibility of contacts and any drug resistance.
The following criteria will be used in considering the discontinuation of isolation for patients with drug sensitive pulmonary and non Multi Drug Resistant pulmonary tuberculosis (MDR TB) in the hospital setting.
• The patient has completed 2 weeks of appropriate chemotherapy or

Tuberculosis Control Plan v4 11
• They are discharged from hospital
6.10 Discharge from Trust Premises
The Specialist TB Control Nurse must always be involved in discharge planning as they are responsible for monitoring the agreed plan, so that alternative arrangements can be put in place, should it not be possible to adhere to agreed plans. In addition to the usual arrangements being made in accordance with Trust policy the discharge plan needs to take into account:
• the type of accommodation the patient is being discharged to, and likely
contacts • whether the patient should still be considered infectious • who is going to supervise(and/or observe therapy) This is essential to prevent
the development of a MDR TB. • arrangements for follow up, including transport • what support services are required and who is to provide them • the need for and arrangements for future microbiological tests • the ability of the patient/and or carers to understand any risk he/she might
pose to others and how to minimise that risk. 6.11 Patients with Drug Sensitive TB
If close home contacts may be HIV ‐ infected or otherwise severely immunocompromised the patient should have had in addition at least 3 negative sputum microscopy smears taken on different days over a 14 day period, before discharge, unless the contacts have been screened and are on tuberculosis chemoprophylaxis or treatment.
6.12 Patients with MDR TB
May remain, or be intermittently sputum positive for many months, years and may never become sputum smear or culture negative. It may be impractical and/or unreasonable to insist on three consecutive negative sputum smears before discharging the patient home. Decisions about discharge will need to be made at consultant level on a case by case basis, the discussion involving the CCDC, clinicians and other relevant carers.
6.13 Patients Who Seek Their Own Discharge
Patients who insist upon taking their own discharge whilst still infectious should have the necessary arrangements to protect their contacts at home explained to them. They should be told that if they do not agree to these arrangements, compulsory admission to an isolation room or ward may be required under the Health Protection (Part 2A orders) Regulations 2010.

Tuberculosis Control Plan v4 12
6.14 Death of a Patient and Post Mortem
All patients with tuberculosis should be placed in a body bag (see Infection Prevention and Control Policy No. 8 – Cadaver Policy). The Histopathologist should always be informed when TB is suspected when a post mortem is requested.
6.15 Arrangements For Follow Up And Outpatient Visits In General
HIV Related Tuberculosis Patients with drug sensitive pulmonary tuberculosis, whether HIV related or not, are likely to be rendered non‐infectious after 2 weeks treatment with a standard regime. However until drug susceptibility tests are confirmed, or they become sputum negative they should be separated from other immunocompromised patients in outpatient clinics.
Drug Resistant Tuberculosis
Patients with drug resistant tuberculosis should preferably be seen outside an HIV setting, promptly, and if possible at the end half of the day after other patients have left the department. Patients with infectious MDR‐TB who need x‐rays should as far as possible be booked appointments at the end of the day and should wear a FFP3 mask while going through patient areas. These arrangements should continue until 3 consecutive negative sputum cultures have been obtained and the patient is complying with and responding to treatment.
Even when treatment has been completed, patients who subsequently develop respiratory symptoms should let the receptionist or clinic nurse know on arrival, or when making an appointment and should be seen at appropriate times or in rooms that have adequate ventilation (ideally confirmed negative pressure ventilation). Domiciliary visits for clinical assessments should be considered for patients who have MDR‐TB, who are sent home before they are culture negative or who may have relapsed.
6.16 Inter Current Interventions
Patients with tuberculosis will sometimes require surgery or other procedures. The implications for staff, equipment and environment should be discussed on a case by case basis with the involvement of the consultant microbiologist
6.17 Contact Tracing
Organisation – Consultant in Communicable Disease Control (CCDC)
• Has ultimate responsibility for the decision as to which of the identified contacts of index cases of tuberculosis should be screened and for co‐ordinating this.

Tuberculosis Control Plan v4 13
• Is responsible for ensuring that contact tracing takes place and that appropriate arrangements are in place.
• Co‐ordinates the screening of children and teachers in schools where there has been tuberculosis.
6.18 Identification of Contacts
Clinicians who see initial index cases will draw up lists of contacts to forward to the TBNS. The TBNS is responsible for identifying contacts within the community that require screening. In the case of children Mantoux testing is carried out within the Children’s department. For adults Mantoux testing is performed by the TBNS prior to patients being seen in the adult chest clinic The TBNS may also receive, via the CCDC details of Gateshead residents who are contacts of cases of TB identified elsewhere.
6.19 Action to be taken on the Diagnosis of Smear‐Positive Pulmonary Tuberculosis
in a Patient
If the patient has been isolated since admission, no further action need be taken. A problem which occurs sometimes, however, is that of the patient who has been on the open ward for some time (which may be up to several weeks) before the diagnosis is made. During this time, both staff and other patients will have come into contact with the patient. When this happens, the following action should be taken.
6.19.1 Patient Contacts
Following diagnosis of TB in a hospital inpatient, a risk assessment should be undertaken. This should take into account:
• The degree of infectivity of the index case • The length of time before the infectious patient was isolated • Whether other patients are unusually susceptible to infection • The proximity of contact.
Contact tracing and testing should be carried out only for patients for whom the risk is regarded as significant. Patients should be regarded as at risk of infection if they spent more than 8 hours in the same bay as an inpatient with sputum smear‐positive TB who had a cough. The risk should be documented in the contact’s clinical notes, for the attention of the contact’s consultant. A list of such patients will be drawn up by clinical staff in conjunction with the IPCT and given to a chest physician. The contact should be given ‘Inform and advise’ information, and their GP should be informed with a standard letter. If patients were exposed to a patient with sputum smear‐positive TB for long enough to be equivalent to household contacts (as determined by the risk assessment), or an exposed patient is known to be particularly

Tuberculosis Control Plan v4 14
susceptible to infection, they should be managed as equivalent to household contacts. Such patients will be included in the list. If an inpatient with sputum smear‐positive TB is found to have MDR TB, or if exposed patients are HIV‐positive, contact tracing should be in line with The Interdepartmental Working Group on Tuberculosis Guidelines In cases of doubt when planning contact tracing after diagnosing sputum smear‐positive TB in an inpatient, further advice should be sought from the local PHE Health Protection Team/ CCDC.
• Visitors: visitors to the wards would not usually be followed up.
6.19.2 Staff Contacts
The risk of transmission of TB to a member of staff is small; there is probably no greater incidence of TB in health care staff than in the general population (with the possible exception of laboratory staff and those who work regularly with patients with TB). However, a list of close contacts of the patient should be made by the Matron/Ward Manager, in conjunction with the Infection Prevention and Control Team (IPCT). For this purpose, a close contact is defined as: Staff who have clinical contact with a patient exceeding 8 hours cumulatively Staff who perform a bronchoscopy on the patient Staff who perform any of the following procedures, even if this is limited to a single contact:
• induction of sputum • suctioning airways • fine‐needle aspiration • swallowing assessments • chest physiotherapy Staff members are not defined as close contacts who:
• have no face‐to‐face contact with the patient • do not have clinical contact (e.g. domestic staff, ward clerks, and
porters) • have only single or infrequent contact with the patient (with the exception of the staff listed above)
Using the above criteria, the ward/departmental manager should draw up a list of close contacts in conjunction with the IPCT. The list should then be sent to Occupational Health, who will check the list for anyone who might be regarded as particularly vulnerable to TB. This would include:

Tuberculosis Control Plan v4 15
• Staff who have not received BCG immunisation (these should be
very few) or who have been immunised but do not have a visible scar.
• Staff who are themselves immunocompromised.
These staff will be reviewed by an Occupational Health Physician. Any staff about whom there is clinical concern after such assessment should be referred to the chest clinic.
• Immunocompetent staff do not usually require follow‐up unless
they were regular carers for the patient and thus had prolonged close contact, or carried out a high risk procedure.
• In an outbreak: the need for more extensive contact tracing must
be considered on a case by case basis including the need to trace all immunocompromised patients or staff who visited the ward during the stay of the index case. This would be based on individual case risk assessment.
6.20 Contacts in Outpatient Clinics
Contact tracing will generally be restricted to immunocompromised contacts known to have used the same rooms or areas as the index case and again the 8 hour exposure guide will be applied. If transmission is demonstrated to have occurred in the outpatient setting, any immunocompromised patient attending on the same day as the index case should be followed up.
6.21 How far back to Trace Contacts
Advice will need to be taken from the physician in charge of the index case as to how long it is likely that the index patient was infectious.
6.22 Priorities in Contact Tracing
Priority will be given to those thought to have been at highest risk, e.g. those with the greatest exposure and those most susceptible, eg immunocompromised individuals (although the HIV status of contacts may not be known) and young children.
IT WOULD BE HELPFUL IF SPUTUM COULD BE COLLECTED FROM HIV INFECTED CONTACTS WHO ARE COUGHING PRIOR TO THEM ATTENDING HOSPITAL IF THIS POSSIBLE.
6.23 Infection Prevention and Control in Healthcare Faciltites
Aerosol Generating Procedures

Tuberculosis Control Plan v4 16
Under no circumstance should aerosol generating procedures such as sputum induction, the administration of medication by nebuliser and bronchoscopy be carried out on a patient who may have tuberculosis in open ward or bay or unventilated area. They should be conducted only in an appropriate room or enclosing device with adequate local exhaust ventilation. Sputum induction should be avoided all together in a patient with suspected drug resistant tuberculosis. If sputum can not be produced spontaneously it is preferable, and better samples are usually obtained, if the diagnosis is confirmed by bronchoscopy with appropriate precautions. See Infection Prevention and Control Policy No. 2 – Personal Protective Equipment Policy. Other procedures such as respiratory function tests may also provoke coughing (and thus generate aerosols) which may continue after the procedure. These should not be performed on patients who have, or may have pulmonary tuberculosis nor generally should chest physiotherapy, unless it is essential and performed in a suitable facility with due attention to infection control.
6.24 Staff Protection – Risk Assessment Prior to Clinical Procedures
A risk assessment should be performed prior to clinical procedures in all patients. 6.25 Patient Focused Hygiene Methods (cough hygiene)
Two patient focused hygiene measures can help reduce aerosolisation of infected droplet nuclei.
• Patients should be taught to cover both the nose and mouth with a tissue
whenever they cough or sneeze. • Those with sputum positive disease and a cough who are unable to
co‐operate with this practice and all the patients with infectious MDR‐TB should wear a mask during transportation through other patient areas. The mask is to prevent aerosolisation of droplets (as opposed to masks worn to provide personal protection against inhalation of droplets). For this purpose a surgical mask is acceptable.
6.26 Personal Respiratory Protection
Respiratory protection is recommended to be worn:
• By all persons entering the room of a patient with suspected or confirmed infectious MDR‐TB
• During bronchoscopy and other cough inducing procedures (3M FFP3 respirator masks EN 149:2001)
By all persons present in the room For suspected or confirmed non MDR smear positive patients: by those healthcare workers (and other carers in regular or prolonged close contact).

Tuberculosis Control Plan v4 17
• Managers should ensure that all staff are trained in the use of appropriate respiratory protection. See Infection Prevention and Control Policy No. 2 – Personal Protective Equipment Policy.
6.27 Environmental/Engineering Controls
• Bronchoscopy ‐ should whenever possible be performed in an appropriate negative pressure suite with adequate ventilation. All staff involved in the procedure should wear a 3M FFP3 respirator mask EN 149:2001 and all unnecessary staff and other patients should be excluded during the procedure. Some smear‐negative patients may become smear‐positive after bronchoscopy. This may be a temporary phenomenon, but such patients should be treated as smear‐positive (i.e. isolated) until they become smear‐negative again. However, it is not recommended that the sputum of each patient with TB who undergoes a bronchoscopy should be checked after the procedure; therefore patients should normally remain in isolation after bronchoscopy until coughing has returned to normal, which would usually take 24‐48 hours. Staff performing the bronchoscopy should wear a FFP3 mask during the procedure.
• Fine‐Needle Aspiration ‐ this procedure poses a negligible risk to staff, but it is recommended that staff performing the procedure on a patient with confirmed or suspected TB should wear a FFP3 mask.
• Waiting Areas in Chest Clinics/TB Clinics ‐
• Patients with infections or potentially infectious form of tuberculosis should wear a surgical mask. Patients with known infectious MDR‐TB should wear FFP3 masks.
• Patient focused hygiene measures (cough hygiene) can help reduce aerolisation of infected droplet nuclei.
• Confirmation that the patient is no longer infectious should be sought from the TB physician (this will normally mean that three consecutive sputum smears on separate days have been negative on microscopic examination).
• Visits to other departments ‐ This is covered in the Isolation Policy ‐ IC 6. However, it should be noted that some departments have small rooms with poor ventilation. To avoid a risk of infection to other patients, patients with smear‐positive TB should be seen, wherever possible, at the end of an afternoon session. All smear‐positive patients should wear a mask if being transported through patient or public areas of the hospital. A routine surgical mask is satisfactory for this purpose and should be changed at hourly intervals. If the patient is known or suspected to be infected with MDR‐TB, then advice on any additional procedures, including the use of HEPA masks, should be sought from the IPCT, a chest physician, or an infectious diseases physician.
• Terminal Cleaning ‐ terminal cleaning of rooms and areas used by patients with TB/MDR TB should be carried out using chlorine 5,000 ppm.

Tuberculosis Control Plan v4 18
• Endoscope Disinfection ‐ tuberculosis may be transmitted via inadequately disinfected endoscopes. The correct disinfection of these instruments is dealt with in – Please refer to IC 16 Cleaning, Disinfection Maintenance and Use of Endoscopy Equipment Policy.
6.28 Notification
All cases of suspected and confirmed tuberculosis should be notified to the Consultant in Communicable Disease Control (CCDC) who is the Proper Officer of Gateshead, Sunderland and South Tyneside Metropolitan Borough Councils: Health Protection Team North East Public Health England Centre Floor 2, Citygate Gallowgate Newcastle upon Tyne NE1 4WH Tel: 0300 303 8596 option 1 Notification forms are available from: [email protected] Although the tuberculosis notification form does not mention HIV status, it is helpful if those carrying out contact tracing are made aware informally, with the patient’s consent, of dual infections since some of the contacts may also be HIV infected and this alters some of the actions needed for a proper assessment of contacts.
6.29 Protection of Staff Against Tuberculosis
• Immunisation of Staff ‐ this is dealt with in the Staff Immunisation Policy (Please refer to IC 5 – Immunisation Policy for Healthcare Workers). Immunisation with BCG remains an important means of preventing TB in health care staff in the UK. For this reason, every effort should be made to ensure that staff who are in contact with patients or clinical specimens have been immunised with BCG.
• Immunocompromised Staff including those with HIV ‐ the Occupational Health Physician will advise staff with underlying medical conditions including the HIV infected worker on whether alternative work should be recommended to avoid possible exposure to tuberculosis.
• Diagnosis of TB in a Staff Member ‐ occasionally, TB may be diagnosed in a member of staff, other than as part of a control of infection exercise as detailed above. It is extremely important that the Occupational Health Department be informed of the diagnosis. Contacts of the case would normally be dealt with by the chest clinic, who may wish to involve the IPCT if patients have been exposed to infection. In addition, the Occupational Health Department must inform the IPCT if the infection is thought to have been occupationally acquired, since other patients and/or staff members

Tuberculosis Control Plan v4 19
may have been exposed to the same source of infection. The CCDC/Health Protection team should be involved if patients have been exposed, as some of these may have been discharged.
6.30 BCG Vaccination Programme
NB BCG should not be given to any person known or likely to be immunocompromised including those with HIV
Neonatal BCG Programme Currently BCG is routinely offered to all of the following at risk groups. This should be discussed with pregnant mothers by either the Community Midwives in the case of home delivery, or by midwives in the antenatal clinic Queen Elizabeth Hospital. There is then further opportunity for mothers who have had their babies in hospital for it to be discussed in the post natal ward. For children born at home, the community midwife should inform Dr Bosman’s secretary on 445 2741.
‐ Children whose ethnic origins involve countries where there is a high
incidence of TB ‐ Children who will be spending time abroad in countries where TB is more
prevalent or where immunisation is required. ‐ Children with a family contact history of TB over the last 10 years Parents of all the above should routinely be offered BCG for their babies prior to hospital discharge. However, depending upon staff vaccine availability they may be requested to attend the Children’s TB clinic for BCG to be given there. There may be other unusual circumstances such children from homeless families, children born abroad, but then moving to this country in first few weeks of life etc. Tuberculin Testing in Neonates and Children Under School Age It is not necessary to tuberculin test children under the age of 6 years to giving BCG vaccination. Children above this age should be seen in the Children’s TB clinic, where a Mantoux test will be done.
Paediatric Department web link: http://staffzone/trust‐documents/clinical‐documents/by‐department/childrens‐services.php
6.31 Prevention and Management of Infection in Patients with Autoimmune Rheumatic Disease
See Trust website link ‐
http://staffzone/trust‐documents/clinical‐guidelines/by‐department/rheumatology.php
7. Education and training
All trust staff attend a corporate and local induction programme. Staff must be familiar with the policy outlined within this document as it is their responsibility to adhere to Trust

Tuberculosis Control Plan v4 20
policy. Staff managers must ensure that personal protective equipment is available for all staff and fit for purpose. See Infection Prevention and Control Policy No.2 ‐ Personal Protective Equipment Policy. Annual infection prevention and control updates are mandatory for all staff and include the management of respiratory illness.
8. Equality and diversity
The Trust is committed to ensuring that, as far as reasonably practicable, the way we provide services to the public and the way we treat our staff reflects their individual needs and does not discriminate against individuals or groups on any grounds. The policy has been appropriately assessed.
9. Monitoring compliance
Performance indicators for this policy include measures of adherence to the Infection Prevention and Control Policies No.2 ‐ Personal Protective Equipment and No.6 ‐ Isolation Policy and the individual management of known/suspected cases of pulmonary Tuberculosis across the health economy. A risk assessment is made by the visiting IPCT member for each case and education and advice is provided to ensure safety of staff, patients and visitors as per The Health Act 2008.
Compliance with this policy will be monitored by Infection Prevention and Control on a case to case basis and will address any issues not currently complied with and monitor until patients discharge. Weekly Ward Quality Measure audits which are submitted centrally via the trust Safecare dashboard will monitor compliance against the Personal Protective Equipment Policy No. 2. Point prevalence weekly isolation audit performed by IPCT reported at weekly IPC meetings will monitor compliance against the Isolation Policy No. 6. Exceptions to practice such as inappropriate PPE and inability to isolate will be discussed and minuted at the Infection Prevention & Control weekly surveillance meetings and taken forward to the Infection Prevention & Control Committee. Clinicians will be asked to Datix any known or suspected symptomatic respiratory TB patient where incorrect PPE is being worn or is not placed in a single room.

Tuberculosis Control Plan v4 21
Appendix 1
References 1 NHS Estates (2005) In patient accommodation: options for choice. Isolation facilities in acute settings HBN4 supplement 1. London: The Stationery Office. Available from www.dh.gov.uk 2 Countries with more than 40 cases per 100,000 per year, as listed by the Health Protection Agency (go to www.hpa.org.uk and search for ‘WHO country data TB’). 3 European standard EN149:2001; masks should meet the standards in ‘Respiratory protective equipment at work: a practical guide HSG53’ published by the Health and Safety Executive (2005). Available from www.hsebooks.com/Books 4 The Interdepartmental Working Group on Tuberculosis (1998) The prevention and control of tuberculosis in the United Kingdom: UK guidance on the prevention and control of transmission of 1. HIV‐related tuberculosis 2. drug‐resistant, including multiple drug‐resistant, tuberculosis. London: Department of Health. Available from www.dh.gov.uk 5. National Institute for Health and Clinical Excellence (2011). Clinical Guideline 117 Tuberculosis: clinical diagnosis and management of tuberculosis, and measures for its prevention and control. London: NICE 6. NHS Estates (2005) In patient accommodation: options for choice. Isolation facilities in acute settings HBN4 supplement 1. London: The Stationery Office. Available from www.dh.gov.uk 7. European standard EN149:2001; masks should meet the standards in ‘Respiratory protective equipment at work: a practical guide HSG53’ published by the Health and Safety Executive (2005). Available from www.hsebooks.com/Books 8. The Interdepartmental Working Group on Tuberculosis (1998) The prevention and control of tuberculosis in the United Kingdom: UK guidance on the prevention and control of transmission of 1. HIV‐related tuberculosis 2. drug‐resistant, including multiple drug‐resistant, tuberculosis. London: Department of Health. Available from www.dh.gov.uk

Tuberculosis Control Plan v4 22
Appendix 2:
Isolation Decisions For Patients With Suspected Respiratory TB Yes No Yes No Yes No Yes No No Yes Yes Yes No
Known or suspected MDR TB based on risk
assessment?
Admit to negative‐pressure room
Admit to single room
Sputum smear positive (1 or more from 3 samples)?
Risk for MDR TB?
Risk for MDR TB?
Does ward have immunocompromised
patients?
Does ward have immunocompromised
patients?
Negative‐pressure room (irrespective of
HIV status). Molecular probed for rifampicin resistance

Tuberculosis Control Plan v4 23
Appendix 3
List of Isolation Facilities Ward 1 6 cubicles Ward 2 6 cubicles Ward 4 6 cubicles Ward 3 (SSU) 2 cubicles EAU 6 cubicles Ward 8 2 cubicles (1 with negative pressure facilities) Ward 9: 12 cubicles (4 with negative pressure facilities) Ward 11 5 cubicles (2 with negative pressure facilities) Ward 12 6 cubicles (2 with negative pressure facilities) Ward 14 6 cubicles (2 with negative pressure facilities) Ward 20 12 cubicles Maternity (post natal) 4 cubicles Critical Care Unit 5 cubicles (3 with negative pressure facilities) Jubilee Unit Ward 21 6 cubicles (1 with negative pressure facilities) Ward 22 6 cubicles (1 with negative pressure facilities) Ward 23 6 cubicles (1 with negative pressure facilities) Ward 24 6 cubicles (1 with negative pressure facilities) Ward 25 6 cubicles (1 with negative pressure facilities) Sunniside 7 cubicles St Bedes 8 cubicles Cragside 12 cubicles
Single room on ward
Negative‐pressure room Standard
ward





























