Embed Size (px)
Citation preview


Please Silence Your Cell Phones
Thank You

WHO Classification of Uterine Tumors 2014
RJ Kurman, ML Carcangiu, CS Herrington, RH Young, Ed
Joanne Rutgers, M.D.Cedars‐Sinai Medical Center
Los Angeles, CA

Disclosure of Relevant Financial Relationships
The USCAP requires that anyone in a position to influence or control the content of all CME activities disclose any relevant relationship(s) which they or their spouse/partner have, or have had within the past 12 months with a commercial interest(s) [or the products or services of a commercial interest] that relate to the content of this
educational activity and create a conflict of interest. Complete disclosure information is maintained in the USCAP office and has been reviewed by the CME Advisory Committee.
Dr. J. Rutgers declares she has no conflict(s) of interest to disclose.

Clinical History• 67 year old G4P1 with personal history of colon cancer 10 years ago
• 2 weeks of vaginal bleeding• Ultrasound: large uterine mass• Hysterectomy, BSO, staging performed
• Uterine intracavitary polypoid 9 cm mass


IHC• Desmin ‐• Myogenin ‐
keratin
vimentin

Final diagnosis
• Carcinosarcoma• [Malignant Mixed Mullerian Tumor (MMMT)]• Homologous type

Outline
• Staging and Classification– History
• WHO 2014 Classification• Clinical, risk factors• Pathologic, IHC, genetics• Ddx• Pathogenesis


Pre‐2008
• Uterine Sarcomas– MMMT (CS) 40%– Leiomyosarcoma– ESS, low grade and high grade
• All uterine ca & sa staged using one system:
• I confined to uterus• II cervix• III pelvic, nodes• IV bladder/rectal or distant metastases

Earlier studies
• Heterologous MMMT had worse prognosis– Rhabdomyosarcoma– Chondrosarcoma and osteosarcoma no significant impact
• High rate of hematogenous spread
Rose 1989, Norris 1966

1990’s: emphasis on carcinomatous component
• Carcinomatous not sarcomatous element determines prognosis – Endometrioid, Type I: favorable– Serous, clear cell, Type II: unfavorable
• Heterologous elements do not affect prognosis
Bitterman 1990, Silverberg 1990

1990’s: Carcinoma driver of prognosis
• LVI relates to prognosis• LN mets as frequent in CS as EM cancer• Carcinoma most common in LVI, LN, and peritoneal metastases
• Shared risk factors as EM ca • CS as Metaplastic carcinoma
Yamada 2000, McCluggage 2002, Zelmanowicz 1998

2008‐2009 FIGO staging systems
• Kept CS with EM Ca• Slight modifications to staging system for EM Ca
• Two new staging systems for sarcoma:
• Leiomyosarcoma and Endometrial Stromal Sarcoma
• Adenosarcoma
2010 AJCC 7th Ed

WHO 2014
• CS preferred term over MMMT• Classified morphologically as one of the mixed epithelial‐mesenchymal uterine tumors
• ‘Biphasic tumor composed of high‐grade carcinomatous and sarcomatous elements’

WHO: CS
• Ca & sa ‘closely admixed but do not merge’• Homologous
– High grade, non‐specific
• Heterologous (50%)– Rhabdomyosarcoma, chondrosarcoma, rarely osteosarcoma, neuroectodermal


CS: Clinical
• Postmenopausal; mean age 65• More common in Black women• Vaginal bleeding, or prolapsing polypoid mass
Bland 2009; Felix 2013

Extra‐uterine CS
• Cervix• Fallopian tube• Ovary• Extra‐genital
Associated endometriosis

Risk Factors
• Radiation• Tamoxifen• Estrogen replacement therapy• Metabolic factors (BMI, diabetes)

Hormonal Risk Factors Similar for EM ca & sa
Felix 2013
0
0.5
1
1.5
2
2.5
3
3.5
BMI Diabetes Estrogen
EMCaCSsarc
OddsRatio

5 Year survival: Worst of any “EM Ca”
• <5% uterine malignancies but 15% of deaths
• No significant improvement in survival over last few decades
• Non‐invasive CS 25% recurrence
Type I 90%
Type II 50‐60%
CS 35%

Prognostic Factors
• Stage• LVI• Nodal status• Rhabdo in low stage CS
Ferguson 2007
Stage 5 yr survival
I 56%
II 31%
III 13%
IV 0

Treatment
• Hyst, BSO, staging incl nodal dissection• Radiation of uncertain benefit• Chemotherapy
– Standard chemo: platinin, taxanes– ifosfamide
Temkin 2007

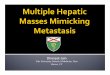
Metastases
• Pelvic, para‐aortic nodes + at same rate as high grade EM Ca
• High incidence hematogenous metastases– Lung 48%– Brain 7%– Bone 19%– Visceral organs 30%
Rose 1989

Composition of Metastases
73
2
26 Carcinoma
Sarcoma
Carcinoma andSarcoma
55
27
18
Sreenan and Hart, 1995
At Presentation Recurrence

CS metastatic to lung


Microscopic: Intimate admixture

Carcinoma
Endometrioid Serous
Clear cell UndifferentiatedSquamous

Sarcoma: Homologous

Sarcoma: Heterologous
myogenin

Practical Tip: Curettage/Biopsy:
• Only anaplastic, high grade, mixed, difficult to classify carcinoma is present
• High grade ca & only rare foci (<1 mm) high grade spindled sarcoma
• When only high grade sarcoma is present
• (Incidence of CS >>>undiff ut sarc or rhabdo)
• Both components may not be present• One can suggest that CS may be seen in hysterectomy when:

Practical tip: How much sarcoma is required to diagnosis CS?
• Problem: ca > sa; sa may only be present in superficial, polypoid portions
• When available, consider both EMB & hyst, and if CS dx was well established on EMB, do not overturn dx based on scant sa in hyst
• On hyst in a well sampled tumor if only sa < 1 mm, ‘not enough’ to establish CS
Soslow.Histopathology 2013


Keratin Vimentin
• Usually marks appropriately• EMoid Adenoca often co‐expresses ker & vim• sarc focally ker +
Meis 1990

Other IHC
• P53• WT1• p16• PAX8 (carcinoma)• ER, PR variable, usually negative
• Desmin: LMS, Rhabdo• Myo D1, myogenin: Rhabdo
• S‐100: chondrosarc
Buza 2009; Franko 2010; Holmes 2014


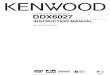
Uterine Adenocarcinomas
Type I (Endometrioid) Type II (Serous)
• PTEN• KRAS• Beta catenin (CTNNB1)• PI3KCA• ARID 1a• MSI/MLH1 methylation
• P53• p16

G. Larry Maxwell et al. Clin Cancer Res 2005;11:4056-4066
Genetics• Gene expression profile show CS as distinct from Type I or II
©2005 by American Association for Cancer Research

CS: Genetics
• Chromosomal abnormalities (high copy number) (8q c‐myc; 20q)
• P53 early event• Rare MSI/Lynch• EGFR• (HER‐2 rare)
0
20
40
60
80
100
p53 PI3K CA PTEN ARID1a Kras
TCGA

50% CS mutations in PI3KCA/AKT and/or RAS/braf pathway
Saegusa 2009; Biscuola 2013
PTEN
PTEN

CS: Clonality
• >85% are monoclonal• 10‐15% biclonal (‘collision tumors’)
Wada 1997; Thompson 1996; Gorai 1997


WHO: Mixed Epithelial and Mesenchymal Tumors
Glands StromaAdenomyoma Benign BenignAtypical polypoid adenomyoma
Atypical, low grade endometrioid adenocarcinoma
Benign
Adenofibroma Benign BenignAdenosarcoma Benign Low grade
sarcomaCarcinosarcoma High grade
carcinomaHigh grade sarcoma

Adenosarcoma with Sarcomatous Overgrowth
• Def: sarc > 25%, without admixed epithelium• Typically high grade sarc• Heteologous incl rhabdo, chondroid• Similar poor outcome as CS Krivak 2001

Ddx: Endometrial Carcinoma variants
• Solid spindled• Benign heterologous elements• Corded and Hyalinized Endometial Carcinoma• Undifferentiated carcinoma

Solid spindled Em Ca
Keratin Reticulin

CHEC: Corded & Hyalinized Endo CA
Murray, Young 2005

CHEC
• Low grade spindle cells and low grade adenocarcinoma
• Merging of the epithelial and spindled elements
• Frequent foci of abrupt keratinization within the spindled elements

IHC: CHEC & spindled EMCa vs. CSP53WT1p16
Beta‐catenin
E‐cadherin
ERPR
CHEC/ Spindled ‐
+ both components
‐ (CHEC) +
CS + ‐ ‐ +/‐
Wani 2009

Ddx: Undifferentiated/Dedifferentiated carcinoma
EMA Reticulin

Un‐ or de‐differentiated carcinoma
• Dyscohesive, patternless sheets, not cohesive or trabecular
• No glandular diff• Small to medium , uniform cells, nucleoli
• Abrupt foci keratinization
• Rhabdoid cells in a myxoid background
• LVI common • Significantly more aggressive than grade 3 EmCa
• May occur in young individuals
• Frequent DNA MMR abnormalities (Lynch)

IHC: Undifferentiated carcinoma
vimentin
EMA
• Keratin ‘negative’ at low power, rare cells +
• CK18, EMA• Loss of E‐cadherin• vimentin + (!)• P16• Neuroendocrine markers: –or <10%
• If diffusely + classify as neuroendocrine carcinoma
EMA


Pathogenesis
1. Collision2. Composition3. Arise from
Adenosarc 4. Combination =
Divergent5. Conversion =
Metaplastic ca
• 2 clones • 10‐15% CS are bi‐clonal
• Histologically identical to other CS, or appear as two adjacent tumors

Pathogenesis
1. Collision
2. Composition3. Arise from
Adenosarc 4. Combination =
Divergent5. Conversion =
Metaplastic ca
• Pseudosarcomatous stroma
• NOT true for CS

Pathogenesis
1. Collision2. Composition
3. Arise from Adenosarcoma
4. Combination = Divergent
5. Conversion = Metaplastic
• AS develops both sa & ca overgrowth (Seidman year)
• 10‐15% CS show lower grade areas resembling AS.
• This pathway may explain CS with more abundant sarcoma

Pathogenesis1. Collision2. Composition3. Arise from Adenosarc
4. Combination = Divergent
5. Conversion = Metaplastic ca
• Monoclonal• One clone or progenitor cell diverges into either ca or sa
• Supported by experimental data
• Accounts for admixture without merging of 2 components, & variable composition of mets
• Allows for ‘stemness’, EMT & MET
Fujii 2000; Emoto 1992, 93; Abeln 1997;Ishiwata 1987

Pathogenesis
1. Collision2. Composition3. Arise from
Adenosarc 4. Combination =
Divergent5. Conversion =
Metaplastic carcinoma
• Monoclonal• Ca ‘converts’ to sa• Some molecular studies show add’l genetic abnl in sa
• “stable” EMT• Most widely quoted theory• Ca, not sa is driver of prognosis• Some oncologists want to lump all mixed epith/mesen tumors in body together: sarcomatoid carcinoma renal upper GI, resp, metaplastic ca breast

Epithelial‐Mesenchymal Transition (EMT) & Mesenchymal‐Epithelial Trans (MET)
• Embryogenesis: epithelium of blastocyst forms mesoderm (EMT) & later mesoderm gives rise to organs w/ epith incl. uterus (EMT)
• Wound healing• Cancer: EMT promotes invasion, metastases, & ‘stemness’

EMT and MET• Epithelial cadherins: E‐cadherin
• Mesenchymal cadherins: N‐Cadherin
• Snail, slug, ZEB, Twist suppress E‐cadherin & maintain ‘stemness”; all upregulated in mesen component of CS
• Epithelial component of CS• Undiff ca, CHEC
Mattias-Guiu; Romero-Perez Mod Path 2013; Romero-Perez Hum Path 2013; Castilla J Pathol 2011; Lopez-Garcia 2010; Chiyoda 2012


Conclusions
• CS preferred term over MMMT–Homologous or Heterologous sa
• CS is staged using EmCa system• CS has worse prognosis than ser ca• Major Ddx are EM Ca variants (CHEC, Undiff) H&E more useful than IHC

Conclusions
• Most CS are monoclonal • Metaplastic ca is most widely quoted theory
– In my opinion some CS do look like metaplastic carcinoma
• Combination (Divergent) theory best explains majority

WHO Authors
Did not dispute classifying CS with EM CA for management took a balanced approach using a morphologic classification
of CS as a mixed epith‐mesen

Important Information Regarding CME/SAMs
The Online CME/Evaluations/SAM claim process will only be available on the USCAP website until October 2, 2015.
No claims can be processed after that date!
After October 2, 2015 you will NOT be able to obtain any CME or SAMs credits for attending this meeting.

Please go to the USCAP website to complete your Evaluation of the course and claim CME and/or SAMs Credits.
Thank You!