Embed Size (px)
Citation preview

329
indicate caution in test interpretation and may be a reason forfrequent diagnostic review or the possible administration ofmultiple therapies in some instances.
We thank Dr G. Brodie, Prince Henry’s Hospital, Melbourne, for his help inproviding patients who formed the basis of this study.
Correspondence to J. I. B., Department of Neurology, Prince Henry’sHospital, St Kilda Road, Melbourne, Victoria 3004, Australia.
REFERENCES1. Gorry GA, Pauker SG, Schwartz WB. The diagnostic importance of the normal
finding. N Engl J Med 1978; 298: 486-89.2. Taylor TR, Aitcthison J, McGirr, EM. Doctors as decision-makers: a computer-assisted
study of diagnosis as a cognitive skill. Br Med J 1971; iii: 35-40.3. Weinstein MC, Fineberg HV, Elstein AS, et al. Clinical decision analysis.
Philadelphia: Saunders, 1980.4. Henson RA, Urich H. Cancer and the nervous system. Oxford: Blackwell Scientific
Publications, 1982.5. Wiebers, DO, Whisnant JP. Epidemiology. In: Warlow C, Morris PJ, eds. Transient
ischemic attacks. New York: Marcel Decker, 1982.
PLAYING THE ODDS
DAVID L. SIMEL
Department of Medicine,Durham Veterans’ Administration Medical Center,
Duke University Medical Center,Durham, North Carolina 27705, USA
SUCCESSFUL gamblers could also be good diagnosticians.Unlike many physicians, they would always "play the odds"rather than follow the "rule out" or "need to know" game.We physicians place mental bets on our patients’ likelydiagnoses and then proceed with tests which we expect tosettle our wager. Unfortunately, diagnostic tests simplychange the odds in favour or against disease; sometimes theyonly confuse the diagnosis.The McMaster University epidemiology group has given
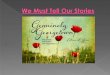
guidelines for reviewing the clinical literature. 1-8 A standard 2x 2 table (fig 1) helps in understanding the utility ofdiagnostic tests. Most physicians appreciate the concepts ofsensitivity and specificity, but their applicability to decisionsabout the management of individual patients is not obvious.
Fig I-Analysis of a diagnostic test.
For instance, would a test with a sensitivity of 70% and aspecificity of 80% help me make a diagnosis when I think thelikelihood of disease is 80% or 50%?
Every encounter with a patient, after a history has beentaken and physical examination done, leads to an estimate ofthe likelihood of certain diagnoses. The estimates can beexpressed as either the probability of disease or the odds ofdisease. The simple relationships are:
probability = odds (equation 1)
1 + odds
prior odds = probability of disease (equation 2)
probability of no diseaseFor example, if we decide that the probability of a disease is
80%, then the probability of no disease is 20%. Therefore, theodds of disease are 4/1, and there are 4 chances out of 5 thatthe disease is present:
Probability of Probability ofOdds disease (%) disease (%)0-25/1 I 20 800-50/t 33 67
0-75/1 1 43 57
1.00/1 50 50
2-00/1 66 34
4-00/1 1 80 20
8-00/1 88 12
16-00/1 94 6
probability = odds
1 + odds
prior odds = probability of disease
probability of no disease
Whether we commit ourselves on paper or just think aboutodds and probabilities, we always estimate the prior odds (orprior probability) of disease before pursuing furtherevaluations which will modify those odds. When the resultsof diagnostic tests have been collected the prior odds arerevised and the new odds become the posterior odds (orposterior probability) in favour of disease.
HOW TO CALCULATE THE POSTERIOR ODDS BEFORE A TEST
IS ORDERED
It would be very helpful to know, even before a test is
ordered, whether or not the result would alter the prior odds.Bayes’ theorem is the method for calculating posterior odds,but it is cumbersome and difficult to inemorise:
Ingelfinger et al have described a simple variation of Bayes’theorem for calculating the posterior odds of disease based ontheorem for calculating the posterior odds ofdisease based onlikelihood ratios of disease.9 I can never recall Bayes’theorem, but I can remember:
posterior odds = (prior odds) x (likelihood ratio) (equation 3)
where prior odds= probability of disease
probability of no disease
likelihood ratio for a positive test (LR+)= sensitivity
1-specificity
likelihood ratio for a negative test (LR-) 1 -sensitivityspecificity

330
Fig 2-Analysis of exercise tolerance testing as a diagnostic test forcoronary artery disease.
Data from Weintraub et all
Once the sensitivity and specificity of a diagnostic test areknown, the utility of the test can be established by calculatinglikelihood ratios for positive and negative results. Obviouslythe posterior odds depend on the prior odds. The sensitivityand specificity of tests can only be gleaned from carefulreview of the literature as guided by the McMaster group.2Weintraub et al have applied Bayes’ theorem to the
diagnosis of coronary artery disease (CAD) by exercisetolerance testing Reassessment of their data demonstratethe utility and ease of calculating the posterior odds on thebasis of the prior odds and likelihood ratio. The 2 x 2 squareanalysis of their data is shown in fig 2. Because all patientsunderwent cardiac catheterisation the CAD prevalence couldbe determined; thus the prior odds of CAD (occlusivecoronary artery disease demonstrated by cardiac
catheterisation) in a patient with angina were 2’23:1 (69%).Patients with typical angina had a CAD prevalence of 82%,whereas only 48% of patients with atypical angina had CAD.With the understanding that sensitivity and specificity areindependent of disease prevalence, the posterior odds can becalculated for the following examples.
Case 1
A 52-year-old man with a strong family history of CAD has typicalexertion-induced angina. Would the results of an exercise tolerancetest (ETT) sway me from my diagnosis of CAD if I estimate, fromWeintraub’s data, an 80% chance (4 : 1 odds) of his having CAD, atest sensitivity 0 - 72, and specificity 0 - 80 (fig 2)?Solution.-The prior odds (equation 2) are 0 - 80/0 . 20 or 4 : 1. If
the patient were to have a positive ETT result the posterior oddswould be 4 x (LR). From equation 3, the LR is 3 - 6. Therefore,the odds of CAD would rise from my prior odds of 4:1 to 14:1 (from80% to 93%). If the patient had a negative ETT, the posterior oddswould be 4 x (LR-). From equation 3, the LR- is 0 - 35. Therefore,the odds of CAD after a negative ETT would fall from 4: to 1 - 4:1 1(from 80% to 58%). I conclude that a positive ETT does not addmuch information to my diagnosis of CAD. Furthermore, a
negative ETT really would not sway me from my suspicion of CAD.I might order an ETT to screen for left main coronary artery disease,but I certainly would not need an ETT to help me diagnose CAD forthis patient.
Case 2
A 52-year-old man who appears in robust health has fleeting chestpain every few months. It has no temporal relationship to exertionand no associated symptoms. Would an ETT help me to establish adiagnosis of CAD if I think that his chest pain is atypical for angina?Solution.-In Weintraub’s study, the prevalence of CAD in
patients with atypical angina was 48%, which gives prior odds of0-92 : 1. The likelihood ratios are exactly the same as in case 1,since the sensitivity and specificity of the test do not depend on thepatient but only on the intrinsic properties of the test. Therefore,
the posterior odds of CAD after a positive ETT would be 3’ 3:1 (or77%) whereas a negative ETT would change the odds to 0 - 32 : 1 (or24%). I conclude that an ETT for my patient with atypical anginawould greatly influence the probability of CAD and would thereforebe useful in my therapeutic decisions.How can I use this information? It is impossible to
remember the sensitivity and specificity of every diagnostictest. However, when there is a diagnostic dilemma carefulevaluation of the sensitivity, specificity, likelihood ratio, andprior odds will help guide diagnostic testing. This can beespecially useful in sequential testing when the posterior oddsafter one test become the revised prior odds of a second test. Acareful analysis of diagnostic tests in light of the prior odds ofdisease would make it much easier to order appropriate testsand discourage us from playing the "rule out" game.
REFERENCES
1. Department of Clinical Epidemiology and Biostatistics, McMaster University HealthSciences Centre. How to read clinical journals: I. Why to read them and how to startreading them critically Can Med Assoc J 1981; 124: 555-58.
2. Department of Clinical Epidemiology and Biostatistics, McMaster University HealthSciences Centre. How to read clinical journals: II. To learn about a diagnostic test.Can Med Assoc J 1981; 124: 703-10.
3. Department of Clinical Epidemiology and Biostatistics, McMaster University HealthSciences Centre. How to read clinical journals: III. To learn the clinical course andprognosis of disease. Can Med Assoc J 1981; 124: 869-72.
4. Department of Clinical Epidemiology and Biostatistics, McMaster University HealthSciences Centre. How to read clinical journals: IV. To determine etiology orcausation Can Med Assoc J 1981; 124: 985-90.
5. Department of Clinical Epidemiology and Biostatistics, McMaster University HealthSciences Centre. How to read clinical journals: V. To distinguish useful from uselessor even harmful therapy. Can Med Assoc J 1981; 124: 1156-62.
6. Department of Clinical Epidemiology and Biostatistics, McMaster University HealthSciences Centre. How to read clinical journals: VI. To learn about the quality ofclinical care. Can Med Assoc J 1984; 130: 377-81.
7. Department of Clinical Epidemiology and Biostatistics, McMaster University HealthSciences Centre. How to read clinical journals: VII. To understand an economicevaluation (part A). Can Med Assoc J 1984; 130: 1428-34.
8. Department of Clinical Epidemiology and Biostatistics, McMaster University HealthSciences Centre. How to read clinical journals: VII. To understand an economicevaluation (part B). Can Med Assoc J 1984; 130: 1542-49.
9. Ingelfinger JA, Mosteller F, Thibodeau LA, Ware JH. Biostatistics in clinicalmedicine. New York Macmillan, 1983.
10 Weintraub WS, Madeira SW, Bodenheimer MM, et al. Critical analysis of theapplication of Bayes’ theorem to sequential testing in the noninvasive diagnosis ofcoronary artery disease. Am J Cardiol 1984; 54: 43-49.
"Although they also operate at more local levels, two otherinfluences are important at the national level [of publicparticipation in health affairs]-the media and pressure groups. Themedia include the press, radio and television... I have on the wholebeen impressed by the responsible attitude of journalists in all themedia, and especially of those who are specifically ’medical’ and’science’ correspondents. It is, of course, true that relations between’the media’ and ’the medical establishment’ are sometimes less thanperfect. The plodding processes of routine medical care... are dullstuff compared with ’cures’ from eating grass or consulting thewitch of Endor; and these last have greater media appeal. On thewhole, however, the gap in understanding between doctors andjournalists has been narrowing, and it is now respectable for a doctorto be named on a programme, so long as he is not making particularclaims to advance his own practice. The relationship will never befree of problems, and particular incidentscan lead to setbacks. Thenotorious BBC Panorama programme on ’brain death’ led directlyto a falling-off in the numbers of kidneys available for
transplantation; it also exposed the lack of perspective of the’current affairs’ outlook, by contrast with science programmes. Theneed for acceptable criteria of ’brain death’ stems not from
transplantation, but from the desire to save relatives from the agonyof watching for many days a ’life’ being prolonged by artificialmeans when the brain has been irretrievably damaged. The formtaken by the programme gave quite unjustified prominence to theelectroencephalogram, which is at the very most a marginalcriterion of viability."-SiR DoUGLAS BLACK. A Medical View. In:Robert Maxwell and Nigel Weaver, eds. Public Participation inHealth-Towards a Clearer View. London: King Edward’sHospital Fund, 1984. P58-59.