Embed Size (px)
Citation preview
Plantar Fasciitis
Plantar Fasciitis:Diagnosis and Therapeutic Considerations
Mario Roxas, ND
AbstractPlantar fasciitis is the most common causeof inferior heel pain. The pain and discomfortassociated with this condition can have adramatic impact on physical mobility. The etiologyof this condition is not clearly understood andis probably multi-factorial in nature. Weightgain, occupation-related activity, anatomicalvariations, poor biomechanics, overexertion,and inadequate footwear are contributingfactors. Although plantar fasciitis is generallyregarded as a self-limited condition, it cantake months to years to resolve, presenting achallenge for clinicians. Many treatment optionsare available that demonstrate variable levels ofefficacy. Conservative therapies include rest andavoidance of potentially aggravating activities,stretching and strengthening exercises, orthotics,arch supports, and night splinting. Otherconsiderations include use of anti-inflammatoryagents, ultrasonic Shockwave therapy, and, in themost extreme cases, surgery. This article reviewsplantar fasciitis, presents the most effectivetreatment options currently available, andproposes nutritional considerations that may bebeneficial in the management of this condition.(Altern Med Rev 2005;10{2):83-93)
IntroductionDescription
Plantar fasciitis (PF) is a degenerative syn-dn)me of the plantar fascia resulting from repeatedtrauma at its origin on the calcaneus.' PF is reportedto be the most common cause of inferior heel pain inadults.- Other names for PF include painful heel syn-drome, heel spur syndrome.^ runner's heel, subcalca-neal pain, calcaneodynia. and calcancal periostitis.^
The word "fasciitis" assumes inflammation is an in-herent component of this condition. However, recentresearch suggests that some presentations of PF man-ifest non-inflammatory, degenerative processes andshould more aptly be termed "plantar fasciosis.""'•'' Inthe United States, more than two million individu-als are treated for PF on an annual basis, accountingfor 11-15 percent of professional visits related to footpain." It is estimated that 10 percent ofthe U.S. pop-ulation will experience plantar heel pain during thecourse of a lifetime.^ PF affects individuals regard-less of sex. age. ethnicity, or activity level. It is seenin physically active individuals such as runners andmilitary personnel, but is also prevalent in the generalpopulation, particularly in women ages 40-60.-^''
Etiology and PathophysiologyThe plantar fascia is a thickened fibrous sheet
of connective tissue that originates from the medialtubercle on the undersurface ofthe calcaneus and fansout. attaching to the plantar plates of the metatarso-phalangeal joints to form the medial longitudinal archof the foot. It provides key functions during runningand walking. In general, the purpose of the plantarfascia is twofold - to provide support ofthe longitu-dinal arch and to serve as a dynamic shock absorberfor the foot and entire leg.
As one walks, the heel makes contact withthe ground. Just after this contact, the tibia turns in-ward and the foot pronates. stretching the plantarfascia and tlattening the arch. This allows the foot toaccommodate for irregularities in the walking surface
Mario Roxas, ND - Technical Advisor. Thome Research; Associate Editor,Alternative Medicine Review. Private practice, Beaverton, OR.Correspondence Address: 11385 SW Scholis Ferry Rd., Beaverton OR 97008Email: [email protected]
Alternative Medicine Review • Volume 10, Number 2 • 2005 Page 83
Plantar Fasciitis
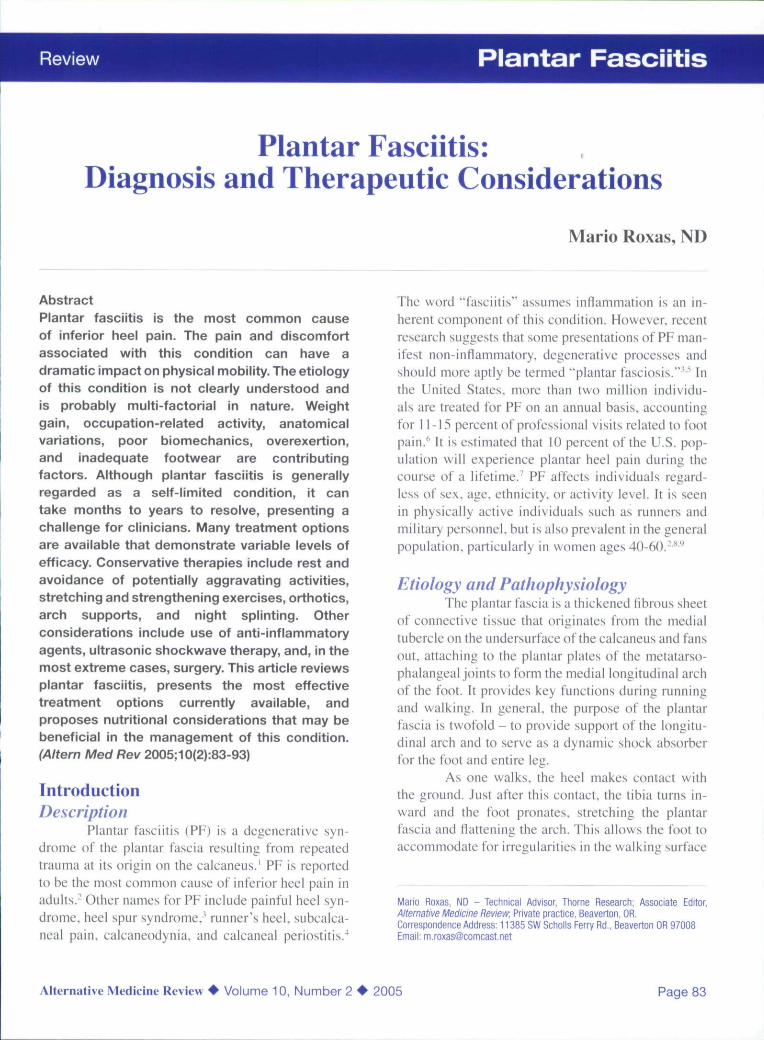
Figure 1. Micro-tears Lead to a ChronicInflammatory Response
Heel Bone
Inflamed Fascia
Plantar Fascia
Adapted from; Singh D, Angel J, Bentley G, Trevino SG.Fortnightly review. Plantar tascittis. e/WJ 1997;315:172-^75-
absorb shock.In the presence of aggravating factors, the re-
petitive movement of walking or running can causemicro-tears in the plantar fascia. The affected site isfrequently near the origin of the plantar fascia at themedial tuberosity ofthe calcaneus (Figure 1). Biopsyspecimens of the affected tissue reveal degenerativechanges in the fascia, with or without iibroblasticproliferation and chronic inflammatory changes.-''
The etiology of PF is poorly understood.While this condition can occur in association withvarious arthritides. the etiology is unknown in ap-proximately 85 percent of cases.'" ln athletes. PF ap-pears to be associated with overuse, training errors,training on unyielding surfaces, and improper or ex-cessively worn footwear. Sudden increases in weight-bearing activity, particularly those involving running,can cause micro-trauma to the plantar fascia at a rate
that exceeds the body's ability to recover." When PFoccurs in elderly adults, it is often attributable to poorintrinsic muscle strength and poor force attenuation,secondary to acquired pes planus (excessive prona-tion ofthe foot) and compounded by a decrease in thebody's healing capacity." Similarly, individuals withdiabetes mellitus may suffer from PF as a result of pe-ripheral motor neuropathy leading to muscle atrophy,changes in anatomical structure ofthe feet (clawtoes.pes cavus or high arches, prominent metatarsal heads,etc.). and functional alterations in gait.'-
Risk FactorsPF is likely the result of multiple factors. Re-
cent case-controlled studies have identified obesityor sudden weight gain, reduced ankle dorsiMexion.pes planus. and occupations that require prolongedweight-bearing as the greatest risk factors associatedwith PF.
One study observed that individuals with abody mass index (BMl) > 30 kg/m- (the cutoff forgrade-II obesity) had an odds ratio of 5.6 for PF com-pared to those with a BMI < 25 kg/nr.'" The samestudy observed that risk of PF increases as the rangeof ankle dorsifiexion decreases. Individuals with <10"of ankle dorsitkxion had an odds ratio of at least 2.1for PF. The ratio increased dramatically as the rangeof dorsiHcxion decreased.'"
Reports state that 81 -86 percent of individu-als with symptoms consistent with PF have excessivepronation.' Individuals with pes planus, associatedwith low arches or flat feet.'''" are thought to be atgreater risk for PF. However, individuals with pes ca-vus'^" '̂ arc also potentially at risk due to the inabilityto effectively dissipate tensile forces during weight-bearing activities.' Other potential anatomical risksinclude leg length discrepancy, excessive lateral tibialtt)rsion. and excessive femoral anteversion."'"*'•''
People with occupations requiring prolongedweight-bearing have long been considered at risk ofPF because ofthe repetitive tensile load placed on thefascia.-'' "
Heel spurs have commonly been implicatedas a risk factor for PF. Approximately one-half of pa-tients diagnosed with PF have heel spurs."' althoughit is unclear how much influence heel spurs actually
Page 84 Alternative Medicine Review • Volume 10, Number 2 • 2005
Review Plantar Fasciitis
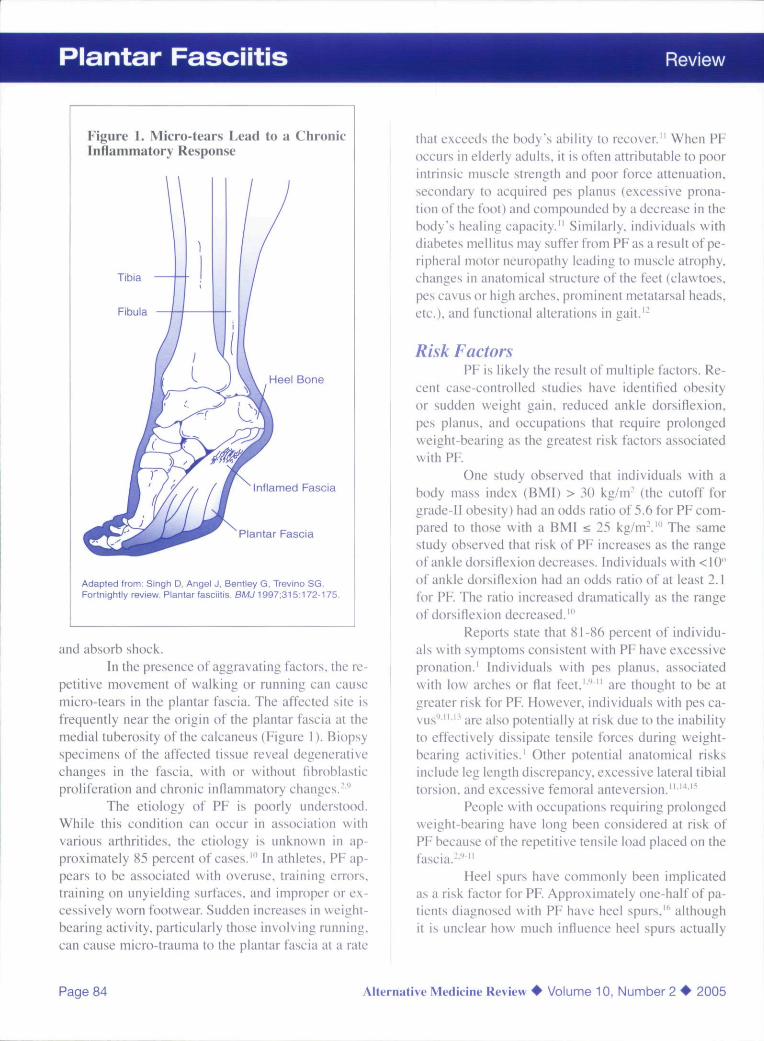
Figure 2. Causes of Interior Heel Pain
Plantar Fascia• Plantar fasciitis - pain with first steps of the day• Plantar fascia rupture - sudden, acute, knife-like pain, ecchymosis
Soft Tissues• Fat pad syndrome - atrophy of heel pad• Heel bruise - history of acute impact injury• Bursitis - swelling and erythema of posterior heel• Tendonitis - pain with resisted motions
SkeletalBony point tenderness• Calcaneal stress fracture - pain with weight-bearing;
worsens with prolonged weight bearing• Paget's disease - bowed tibias, kyphosis, headaches• Tumor - deep bone pain; constitutional symptoms late in the course• Calcaneal apophysitis (Sever's disease) - posterior heel pain
in adolescents
NeurologicalRadiating burning pain, numbness anij tingling, especially at night• Tarsal tunnel syndrome - diffuse nerve symptoms over plantar surface• Posterior tibial nerve entrapment - medial plantar heel symptoms• Abductor digiti quinti nerve entrapment - burning pain in heel pad area
Adapted from:
Young CC, Rutherford DS, Niedfeldt MW. Treatment of plantar fasciitis. Am Fam Physician 2001 ;63:467-474;477-478.Erratum in: Am Fam Physician 2001:64:570.
Singh D, Angel J, Bentley G. Trevino SG, Fortnightly review. Plantar fasciitis. SyWJ 1997:315:172-175.
have on the condition. One study reviewing the ra-diographs of l.OOO patients found 13.2 percent hadheel spurs;of these, only 39 percent (5.2% ofthe totalsample) reported any history of subcalcaneal pain.'
Signs and SymptomsThe classic presentation of PF is pain on the
sole of the foot at the inferior region of the heel. Pa-tients report the pain to be particularly bad with thefirst few steps taken on rising in the morning or af-ter an extended refrain from weight-bearing activity.The pain can be so severe the patient limps or hobblesaround with the affected heel off the ground. After afew steps and through the course of the day. the heelpain diminishes, but returns if intense or prolongedweight-bearing activity is undertaken. Initial reportsof the heel pain may be diffuse or migratory: how-ever, with time it usually focuses around the area of
the medial calcaneal tuberosity. Generally, the painis most significant when weight-bearing activities areinvolved, and can often be correlated to increasedamount or intensity of physical activity prior to onsetof symptoms.
DiagnosisDiagnosis of PF is usually made on the basis
of history and physical examination. Pain on first ris-ing in the morning is typical of PF. and may be help-ful in distinguishing it from other forms of heel pain(Figure 2). For example, in the case of a calcanealstress fracture or nerve entrapment, pain would actu-ally increa.se with more walking, rather than diminishafter the first few steps.-" Associated paresthesia isnot a common characteristic of PF." Nocturnal painshould raise suspicion of other causes of heel pain.such as tumors, infections, and neuralgia (including
Alternative Medicine Review • Volume 10, Number 2 • 2005 Page 85
Plantar Fasciitis
tarsal tunnel syndrome).- PF is usually unilateral, butup to 30 percent of cases have a bilateral presenta-tion.'̂ Bilateral disease in young patients may indicateReiter's syndrome. Patients should also be questionedabout other features of seronegative arthritides.-
Physical examination presents with localizedtenderness at the antero medial aspect ofthe calcane-us. Pain may be exacerbated by passive dorsiflexionof the toes or having the patient stand on the tips ofthe toes." Tightness of the Achilles tendon (with dor-siflexion at the ankle limited by 5" or more) is foundin almost 80 percent of patients.-
Diagnostic imaging is rarely indicated forinitial evaluation and treatment, but may be helpfulin certain cases to rule out other causes of heel pain.Plain radiographs can rule out calcaneal stress frac-ture and may detect an underlying spondyloarthrop-athy.'' Bone scans and magnetic resonance imaging(MRI) may also serve useful, but are not routinelyused.'' Ultrasonography is another u.seful tool to di-agnose PF.'^
Current Treatment OptionsPF is considered a .self-limiting condition.
However, the typical resolution time is anywherefrom 6-18 months, sometimes longer." which canlead to frustration on both the part of the physicianand patient. Most experts agree that early recogni-tion and treatment of PF leads to a shorter courseof treatment and greater probability of success withconservative therapies.-'"' Of the many treatmentoptions available for PF. one of the most effective isalso the most fundamental - rest and avoidance ofaggravating activity provides significant relief. Onestudy cited rest as the treatment that worked best for25 percent of PF patients.'^
Proper ShoesShoes should have adequate arch support
and cushioned heels. Worn or ill-fitting shoes can ex-acerbate PF due to lack of proper cushioning. Overtime, running shoes can lose a significant amount ofshock absorption. Consequently, a new pair of run-ning shoes can do much to decrease foot pain. Forindividuals with pes planus. shoes with longitudinalarch support can help decrease the pain associatedwith long periods of standing." A change in footwear
was cited by 14 percent of PF patients as the treat-ment that worked ' — "*
Arch Supports and OrthoticsMechanical (strapping, taping, etc.) or ac-
commodative (heel cups, orthoties, ete.) treatmentsmay be effective components of a PF treatmentplan.''' A randomized clinical study of 103 patientscompared three treatment categories: anti-inliamma-tory (corticosteroid injections); accommodative (vis-coelastic heel cup): and mechanical (low-Dye tapingfor one month followed by rigid custom orthotics fortwo months). After three months of treatment. 70 per-cent of participants in the mechanical treatment grouprated their outcome as "excellent" or "fair" comparedto the anti-inflammatory and accommodative treat-ment groups, with only a 33- and 30-percent excel-lent outcome, respectively (p=0.005).-"-'
In a study of 236 participants, prefabricatedshoe inserts were superior to both custom-made or-thotics and stretching alone, with over 80 percent ofpeople in the prefabricated insert group showing im-provement after eight weeks, compared to 68 percentwith custom-made orthotics and 72 percent in thestretching group.''
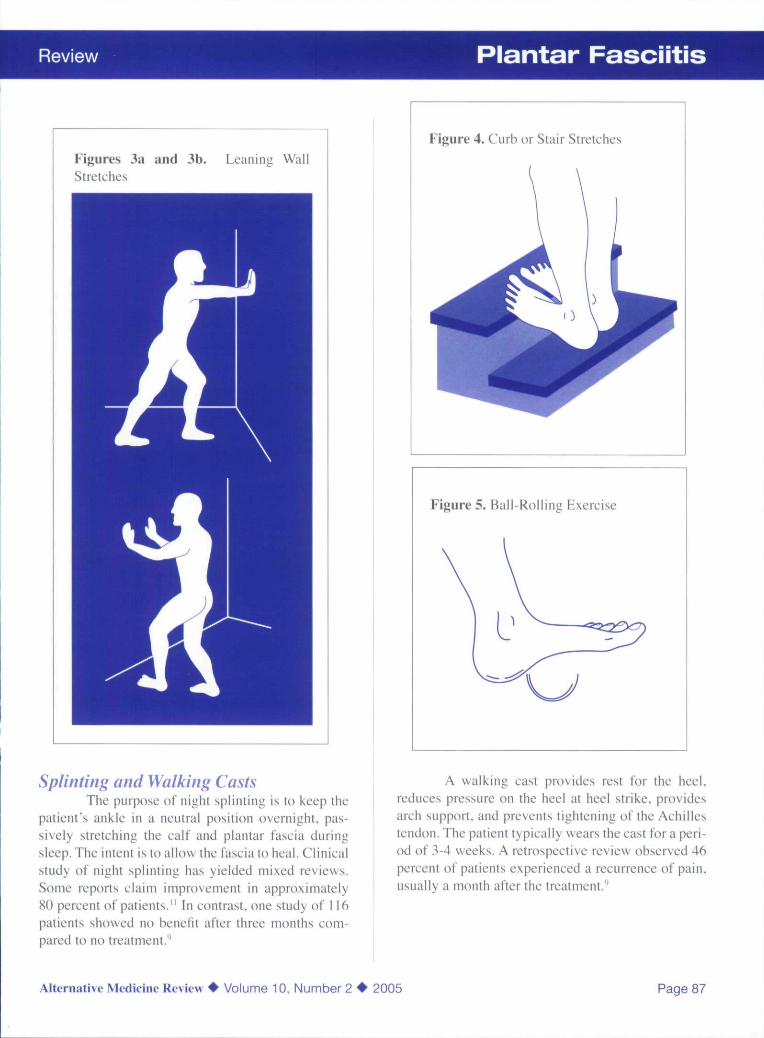
Stretching and StrengtheningStretching and strengthening programs are
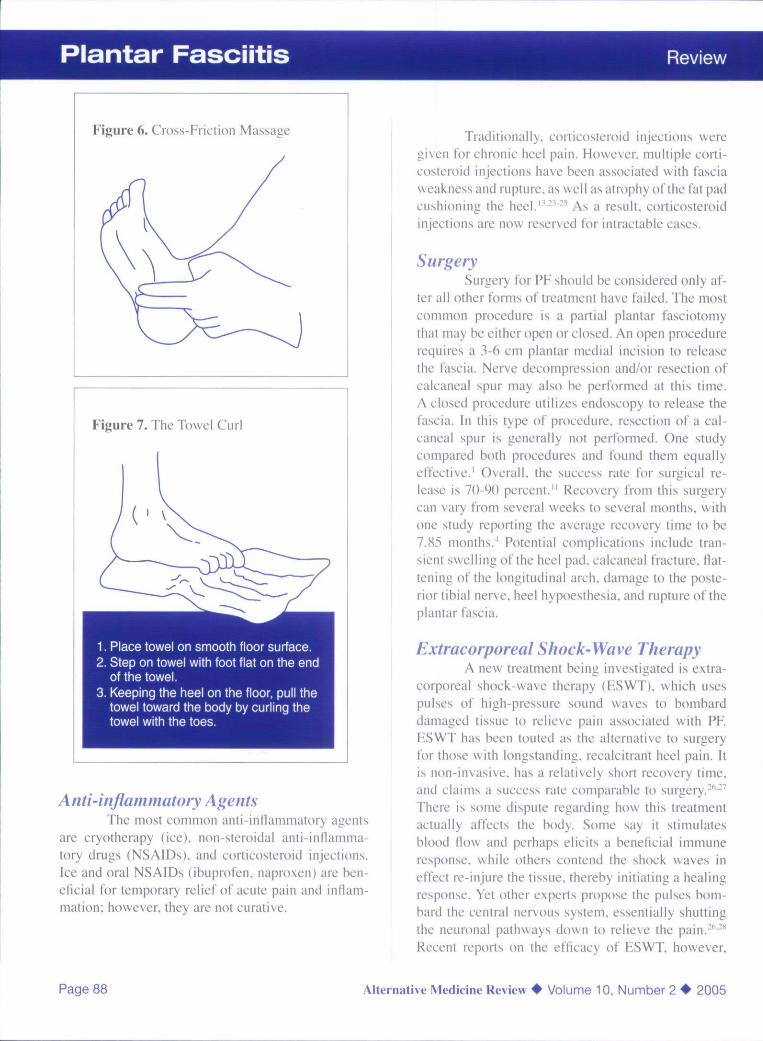
valuable because they can help correct functionalrisk factors, such as tightness of the Achilles tendonand weakness of intrinsic muscles of the foot. Onestudy cited stretching and strengthening exercisesas the treatment that worked best for 29 percent ofPF patients.'^ Commonly used stretches are leaningwall stretches (Figures 3a and 3b) and curb or stairstretches (Figure 4), which focus on stretching thegastrocnemius and soleus muscles. Rolling the footover a 15-oz can or tennis ball (Figure 5) helps stretchthe plantar fascia. Cross-friction massage above theplantar fascia (Figure 6) can be beneficial on wakingto help stretch and warm up the fascia before the firststeps ofthe day. Strengthening exercises are focusedon the intrinsic muscles of the foot and include tow-el curls (Figure 7). toe taps, and picking up marbleswith the toes."--
Page 86 Alternative Medicine Review • Volume 10, Number 2 • 2005
Review Plantar Fasciitis
Figures 3a and 3b.Stretches
Leaning Wall
Splinting and Walking CastsThe purpose of night splinting is to keep the
patient's ankle in a neutral position overnight, pas-sively stretching the calf and plantar fascia duringsleep. The intent is to allow the fascia to heal. Clinicalstudy of night splinting has yielded mixed reviews.Some reports claim improvement in approximately80 percent of patients." In contrast, one study of 116patients showed no benefit after three months com-pared to no treatment.''
Figure 4. Curb or Stair Stretches
Figure 5. Ball-Rollm" Exereise
A walking cast provides rest for the heel,reduces pressure on the heel at heel strike, providesarch support, and prevents tightening of the Achillestendon. The patient typically wears the cast for a peri-od of 3-4 weeks. A retrospective review observed 46percent of patients experienced a recurrence of pain,usually a month after the treatment."
Alternative Medicine Review • Volume 10, Number 2 • 2005 Page 87
Plantar Fasciitis Review
Figure 6. Cross-Friction Massage
Figure 7. The Towel Curl
1. Place towel on smooth floor surface.2. Step on towel with foot flat on the end
of the towel.3. Keeping the heel on the floor, pull the
towel toward the body by curling thetowel with the toes.
Anti-inflammatory AgentsThe most common anti-inflammatory agents
are cryotherapy (ice), non steroidal anti-inllamma-tory drugs (NSAIDs). and corticosteroid injections.Ice and oral NSAIDs (ibuprofen. naproxen) are ben-eficial for temporary relief of acute pain and inflam-mation; however, they are not curative.
Traditionally, corticosteroid injections weregiven for ehronie heel pain. However, multiple corti-costeroid injections have been associated with fasciaweakness and rupture, as well as atrophy ofthe fat padcushioning the heel.'^-'-^ As a result, corticosteroidinjections are now reserved for intractable eases.
SurgerySurgery for PF should be considered only af-
ter all other forms of treatment have failed. The mostcommon procedure is a partial plantar fasciotomythat may be either open or closed. An open procedurerequires a 3-6 cm plantar medial incision to releasethe fascia. Nerve decompression and/or resection ofcalcaneal spur may also be performed at this time.A closed procedure utilizes endoscopy to release thefaseia. In this type of procedure, resection of a cal-caneal spur is generally not performed. One studycompared both procedures and found them equallyeffective.' Overall, the success rate for surgical re-lease is 70-90 percent." Recovery from this surgerycan vary from several weeks to several months, withone study reporting the average recovery time to be7.85 months.^ Potential complications inelude tran-sient swelling ofthe heel pad. calcaneal fracture, flat-tening ofthe longitudinal arch, damage to the poste-rior tibia! nerve, heel hypoesthesia. and rupture oftheplantar fa.scia.
Extracorporeal Shock-Wave TherapyA new treatment being investigated is extra-
corporeal shock-wave therapy (ESWT). which usespulses of high-pressure sound waves to bombarddamaged tissue to relieve pain associated with PF.ESWT has been touted as the alternative to surgeryfor those with longstanding, recalcitrant heel pain. Itis non-invasive, has a relatively short recovery time.and claims a success rate comparable to surgery.-'''•'There is some dispute regarding how this treatmentactually affects the body. Some say it stimulatesblood flow and perhaps elicits a beneficial immuneresponse, while others contend the shock waves ineffect re-injure the tissue, thereby initiating a healingresponse. Yet other experts propose the pulses bom-bard the central nervous system, essentially shuttingthe neuronal pathways down to relieve the pain.-''**Recent reports on the efficacy of ESWT. however.
Page 88 Alternative Medicine Review • Volume 10, Number 2 • 2005

Review Plantar Fasciitis
have not been stellar. One randomized, double-blind,placebo-controlled trial from Australia determined itto be no better than placebo.-'' Two other trials con-ducted in Germany arrived at the same conclusion.̂ "^ '̂One study involving 150 patients demonstrated a suc-cess rate of 56 percent in the active group versus 45percent in the control group.-'' Nevertheless, the U.S.Food and Drug Administration has approved twoshock-wave machines for treatment of PF and tenniselbow.-** More studies are necessary to determine howeffective this treatment is for PF.
Alternative Treatment OptionsMagnetic Insoles
Use of magnetic insoles has been consideredby some clinicians as a treatment for PF. but avail-able data regarding efficacy is limited, and results aremixed at best. One trial involved 375 patients withdiabetic peripheral neuropathy, randomly assignedto wear either magnetized soles or placebo for fourmonths. Results were marginal, showing 10-12 per-cent reductions in numbness and tingling, burning.and pain.'-''Another randomized trial of 101 patientswith plantar heel pain concluded magnetic insoleswere no more beneficial than placebo.'^
AcupunctureAcupuncture has been proposed as an effec-
tive treatment for PF: however, most reports have beenanecdotal in nature.''̂ Research regarding its efficacyis quite limited at this time, but does show promise.One study was performed on 11 patients using acu-puncture in conjunction with electrical stimulation.Patients were treated once weekly for 3-6 weeks.Post-treatment results demonstrated a significant re-duction in the mean score for overall pain (from 5.7to 3.0 on a UVpoint visual analog scale).^''
Nutritional ConsiderationsThere is a dearth of clinical research regarding
nutrition in the specific management of PF. This is notto say. however, that support is unavailable. The fol-lowing are selected considerations to assist the clini-cian as pait of the overall management of PF.
Vitamin CWidely known for its antioxidant proper-
ties.'̂ '** vitamin C is also an essential component forhealthy connective tissue repair. It is necessary forthe hydroxylation of proline and lysine residues inprocollagen, a precursor to collagen. Hydroxypro-lines .stabilize the triple-helix structure of collagen."'A deficiency in vitamin C can result in abnormal col-lagen fibers, as well as other changes in the intracel-lular matrix, that can contribute to decreased tensilestrength of fibrous ti.ssues,"*" such as those found inthe plantar fascia. Recommended dosing of vitaminC for the purpose of tissue repair is 1-3 g daily untilresolution.^'"''
ZincZinc, an essential trace mineral, is utilized
in over 300 known enzymatic reactions. It is a keyelement in tissue regeneration and repair, working inconcert with vitamin C to increase tensile strengthof wounded tissue.̂ ^ Research conducted on animalmodels suggests decreased protein and collagen syn-thesis may be due in part to zinc deficiency, leadingto delayed wound healing.̂ '̂ '̂' Zinc deficiency is acommon occurrence/^ particularly in individualswith chronic injuries and high stress levels. Intenseexercise can affect zinc utilization.^' Further inves-tigation is required to determine the efficacy of zinc-supplementation for wound healing. However, exist-ing data suggests supplementation to be a reasonableconsideration to prevent consequences of deficiency.Recommended dosage for zinc is 15-30 mg
GlucosamineGlucosamine may be helpful in the manage-
ment of PF because it serves as a potential alternativeto NSAID use and is a key biochemical component inthe repair and regeneration of connective tissue.
Several studies have compared glucosaminesulfate (GS) with NSAIDs.^"^- Although the con-text of these studies on GS has been with regard totreatment of osteoarthritis. it may be reasonable toconsider its application in PF. Three independent,double-blind studies (involving 200. 178, and 40 pa-tients with osteoarthritis. respectively) compared theeffects of GS to ibuprofen.^""' In the first study, overa four-week period, pain and function improved more
Alternative Medicine Review • Volume 10, Number 2 • 2005 Page 89
Plantar Fasciitis Review
rapidly in the ibuprofen group compared to the GSgroup for the first two weeks. However, at the end ofthe fourth week, there were no significant differencesbetween the two groups, suggesting GS was as ef-fective as ibuprofen in alleviating OA symptoms.^"Similar results were determined in the .second study. '̂The third study observed patients over an eight-weekperiod. At the end ofthe study, the GS group report-ed greater improvement than the ibuprofen group.'̂ -Fairly consistent in these trials was the observationthat GS provided longer lasting benefit and was bet-ter tolerated than NSAIDs. despite the fact that GShas little direct anti-inllammatory effect and no directanalgesic properties."^* This may be explained in partbecause, although NSAIDs provide symptomatic re-lief from pain and inilammation. they do nothing torepair tissue trauma. By contrast. GS provides the nu-tritional components that not only improve symptomsbut aid in the body's reparative process.
Glucosamine is the foundational structure ofmany compounds associated with repair and regener-ation of connective tissue. It is the essential substratefor hyaluronic acid and other glycosaminoglycansused in maintaining healthy joint function.̂ "* hi vitrostudies suggest glueosamine stimulates the synthesisof glycosaminoglycans and collagen.̂ ^ Recommend-ed dosage for glucosamine is 500 mg three times dai-ly in the form of glueosamine sulfate."'^''
BrninelainBromelain is the singular name used for a
family of proteolytic enzymes found in the pineappleplant {Ananas comosus). Bromelain is commonlyused in treating inflammation and soft tissue injuriesand. as such, may be beneficial in the managementof PF. It has been shown to accelerate healing frombruises and hematomas.^' One open-case observationstudy demonstrated the eflicacy of bromelain on 59patients with blunt injuries to the musculoskeletalsystem. It was reported that use of bromelain reducedswelling, tenderness, and pain, both at rest and duringmovement. ̂ ^
The anti-inflammatory activity of bromelainmay be due in part to inhibition of bradykinin pro-duction at the site of inilammation by way of limit-ing plasma kallikrein and librin formation.^'"'' Fur-thermore, bromelain has been shown to stimulate
conversion of plasminogen to plasmin, thereby in-creasing fibrinolysis/''
There are several designations used to in-dicate the activity of bromelain. The most commonmeasures of bromelain activity arc milk clotting units(mcu) and gelatin dissolving units (gdu). One gduapproximately equals 1.5 mcu. Typically, en/ymaticactivity is given as a measure of mcu or gdu per gramof bromelain; e.g.. 2.000 mcu/g or 1.333 gdu/g. re-spectively.
Recommended dosage for bromelain is 500-2,000 mg daily (with at least 2.000 mcu/g) in divideddoses.''--'''
Fish OilOils from deep sea fish are a rich source of
omega-3 polyunsaturated fatty acids, particularlyeicosapentaenoic acid (BPA) and docosahexaenoicacid (DHA). These fish oils have been observed tosuppress production of inflammatory mediators inpatients with autoimmune conditions, such as rheu-matoid arthritis. A double-blind, placebo-controlledstudy on 49 patients with rheumatoid arthritis foundthose given lish oil daily for 24 weeks showed lessmorning stiffness and fewer tender joints than con-trol group counterparts.'*^ This may be due to reducedsynthesis of key inflammatory mediators - leukotri-enes, interleukin-2, and tumor necrosis factor. Suchanti-inflammatory properties may in tum be benefi-cial in the management of PF.
The natural ratio of EPA to DHA is approxi-mately 3:2. accounting for 30 percent ofthe fatty acidcontent in fish oil. Therapeutic dosages for fish oilrange from 1-10 g daily, depending on severity, andmay require 2-6 months to manifest effect. Recom-mended dosage for PF is 2-3 g daily.
ConclusionPF is generally regarded as a self-limited
condition, with more than 80 percent of cases re-solving within 12 months, regardless of therapy. Avariety of treatment options are available to patients.The most prudent approach to therapy is to employconservative treatments first. Primary considerationsfor treatment should Include temporary refrain fromintense weight-bearing activity as much as possible;avoidance of walking barefoot on hard surfaces; and
Page 90 Alternative Medicine Review • Volume 10, Number 2 • 2005
Review Plantar Fasciitis
replacement of any worn or ill-litting shoes withnew. more accommodating footwear. Stretching andstrengthening exercises can be beneficial for treat-ment and prevention of recurrence.
Use of mechanical devices may be an optionfor individuals for whom the condition does not im-prove. However, efficacy of these treatments is ques-tionable. Other treatment options may be beneilcial.including extracorporeal Shockwave therapy, mag-netic insoles, and acupuncture. Surgery should onlybe considered for patients with considerable disabil-ity for whom conservative treatment has not helpedafter at least 12 months.
Non-steroidal anti-inflammatory drugs areused conventionally for temporary pain relief, but of-fer no support for resolution of the condition. Cor-ticosteroid injections provide temporary relief frompain and are recommended only in extreme cases, asthey may increase the risk of infection and contributeto further degeneration of the plantar fascia and heelfat pad. Alternatively, nutritional considerations suchas vitamin C. zinc, glucosamine sulfate. bromelain.and lish oil may be incorporated to address the painand inflammatory symptoms associated with PF. andto help support the healing process systemically.
References1. Cornwall MW. McPoil TG. Plantar fasciitis:
etiology and trciitnient. J Orthop Sports Pins Tlicrl999;29:756-76().
2. Singh D. Angel J. Bcntk-y G. Trevino SG.Fortnightly review. Plantar fasciiti.s. BMJ1997:315:172-17.S.
3. Leinont H, Ammiiati KM, Uscn N. Plantarfasciitis: a degenerative process (fasciosis)without iiillanimation../ Am PixHcur Med A.'^.\(>c
4.
5.
6.
Davies MS. Weiss GA, Saxby TS. Plantar fasciitis:how sLiceessful is surgical intervention? Fool AnkleIni I999:2():8().VS()7.^Aldridge T. Diagnosing heel pain in adults. AmFam rii\sician 2(K)4;7():.332-338.Pfeffer G, Bacehetti P. Detand J, et al. Comparisonof cusUMii and prefabricated orthoses in the inilialtreatment of proximal plantar faseiitis. Foot Anklehll I999;2O:214-22I.Cravvtord !•'. Atkins D. Edwards J. Interventionsfor ireaiiny plantar heel pain. Cochninc DatabaseSvsi Rev 2'()(K);(3):CD(K){14I6. Update in: CocliraneDatabase Sxsi Rev 2{)()3;(3):CD0()()416.
8. Riddle DL. Pulisie M. Sparrow K. Impaet ofdemographie and impainnenl-related variables ondisability associated with plantar taseiitis. FoolAnkle l^[2{)04a5:^\\-^\l.
9. Buchhindcr R. CltnJLal practice. Plantar fasciitis. NFniil J Med 2()(I4:3?O:2159-2166.
10. Riddle DL, Pulisie M. Pideoe P. Johnson RE. Riskfactors for plantar fasciitis: a matehed ease-eontrolstudy. J Bone Joint Swg Am 20()3;85-A:872-877.Et-ratuni in:,/ Hone Joint Siir^ Am 2OO3;85-A: 1338.
11. Young CC, Rutherford DS. Niedfeldt MW.Treatment of plantar faseiitis. Am Fam Physician2001:63:467-474.477-478. Erratum in: Am FamPlty.si(ian2O()\-M:5H).
1 2. D'Anibrogi E. Giurato L, D'Agostino MA, et al.Contribution of plantar faseia to the inereasedforefoot pressures in diabetie patients. DiabetesO//r 2003:26:1525-1529.
13. Tallia AK Cardone DA. Diagnostic and therapeutieinjectitin ofthe ankle and foot. Am Fam Physician2003:68:1356-1362.
14. Messier SP, Pittala KA. Etiologie faetors associatedwith selected runnine injuries. Med Sei SporlsExcrc 1988:2O:5Ol-.5O5.
15. Warren BL. Anatomical factors assoeiated withpredicting plantar fasciitis in long-distance runners.Med Sci Sports flxeic 1984:16:60-63.
16. DeMaio M, Paine R. Mangine RE. Dre/D Jr.Plantar fasciitis. Orthopedics 1993:16:1153-1163.
17. Aklirat M. Sen C. Gunes T. Ultrasonographicappearance ofthe planlar fasciitis. Clin Imaging2003:27:353-357.
18. Wolgin M. Cook C. Graham C, Mauldin D.Conservative treatment of plantar heel pain: long-term tol!ow-up. Fool Ankle Int 1994:15:97-102.
19. Seligman DA. Dawson DR. Cuslomi/ed heel padsand soft orthotics to treat heel pain and plantarfasciitis. Anh Phys Med Rehabil 2003:84:1564-1567.
20. Lynch DM. Goforth WP. Martin JE. et al.Conservative treatment of plantar fasciitis. Aprospective study. J Am Podiair Med Assoc1998:88:375-380.
21. StadlerTA. Johnson ED, Stephens MB. Clinicalinquiries. What is the best treatment for plantarfaseiitis? J Fam Pract 2003:52:714-717.
22. Niedleldt MW. A friend told me my heel pain isprobably plantar faseiitis. What is this eondilion.and how is it treated? He(ddj Ne^vs 2002:8:12.
23. No authors listed. Plantar faseiitis. Repeatedeortieosteroid injections are safe. Can FamPhysician 1998:44:45.51.
24. Crawford F, Atkins D. Young P. Edwards J. Steroidinjeetion for heel pain: evidenee of short-termeffectiveness. A randomized eontrolied trial.Rheimuaohgy {O.xjord} 1999:38:974-977.
Alternative Medicine Review • Volume 10, Number 2 • 2005 Page 91
Plantar Fasciitis
25. Barrett SJ. O'Malley R. Plantar faseiitis andother eauses of heel pain. Am Fam Physician1999:59:2200-2206.
26. Theodore GH, Bueh M. Amendola A. et al.Extraeorporeal shock wave therapy for thetreatment of plantar faseiitis. Fool Ankle ini2004:25:290-297.
27. Ogden JA. Cross GL. Williams SS. Bilateralehronie proximal planlar fasciupathy: treatmentwith eleetrohydraulic orthotripsy. Fool Ankle Int2004:25:298-302.
28. No authors listed. A new wave of treatment. Afterother treatments have failed, shoek-wave therapymay help some people with heel pain and tenniselbow. Harv Health Lett 2003:28:6.
29. Buehbinder R. f̂ tasznik R. Gordon J. et al.Ultrasound-guided extracorporeal shoek wavetherapy for plantar faseiitis: a randomizedcontrolled trial. JAMA 2002:288:1364-1372.
30. Biich M. Knorr U. Fleming L. et al. ExtraeorporealShockwave therapy In symptomatic heel spurs. Anoverview. Onhopade 2002:31:637-644. 1 Article inGerman I
31. Haake M. Buch M. Schoellner C, et al.Extracorporeal shock wave therapy for plantarfasciitis: randomised controlled multicentre trial.BMJ 2003:327:75.
32. Weintraub MI. Magnets for patients with heel pain.JAMA 2004:291:4.V44: author reply 44.
33. Weintraub MI. Wolfe Gl. Barohn RA. et al:Magnetic Research Group. Static magnetic Heldtherapy for symptomatic diabetic neuropathy: arandomized, double-blind, placebo-controlled trial.Arch Phys Med Rehabil 2003:84:736-746.
34. Winemiiler MH. Billow RG. Laskowski BR.Harmsen WS. Effect of magnetic vs sham-magnetic insoles on plantar heel pain: a randomizedcontrolled trial. JAMA 2003:290:1474-1478.Erratum in: JAMA 2004:291:46.
35. Steinmetz M. Treatment choices for plantarfaseiitis. Am Fam Physieian 1999:60:2504.
36. Perez-Millan R. Foster L. Low-frequencyeiectroacupuncture in the management of refractoryplantar fasciitis: a case series. MeJ Acupunci2001:13:47-49.
37. Ftei B. Stocker R. England L. Ames BN.Ascorbate: the most effective antioxidant in humanblood plasma. Adv E.\p Med Biol 1990:264:155-163.
38. Frei B. Stocker R. Ames BN. Antioxidant defensesand lipid peroxidation in human blood plasma.Proe Nail Acad Sei USA 1988:85:9748-9752.
39. Gross RL. The effeet of aseorbate on woundhealing., tnl Ophfhalmol Clin 2000-A0:5\-51.
40. Porto da Rocha R. Lucio DP. Souza Tde L. et al.Effects of a vitamin pool (vitamins A. E. and C) onthe tissue necrosis process: experimental study onrats. Aesthenc Plast Suri> 2(K)2:26:197-202.
41. Lcvcnson SM. Demetrioii AA. Metabolic factors.In: Cohen IK, Diegelmann RF. Linblad WJ. eds.Wound Healing: Biochemical and Clinical Aspects.Philadelphia. PA: WB Saunders Co: 1992:264.
42. Kelly GS. Sports nutrition. In: Pizzorno J. MurrayM, eds. 'ie.xihook of Natural Medicine Vol 1. 2nded. Edinburgh: Churehill Livingstone: 20{K):528.
43. Murray M. Encyclopedia ofNulritionalSupplements. Rocklin. CA: Prima Publishini::1996:78.
44. Kaplan B. Gonul B. Dineer S. et al. Relationshipsbetween tensile strength, ascorbic acid.hydroxy pro line, and zinc levels of rabbit full-thickness ineision wound healing. Siir^i Today2004:34:747-751.
45. Agren MS. Franzen L. Infiuence of zinc deficiencyon breaking strength of 3-week-c)ld skin incisionsin the rat. Acta Chir Scand 1990:156:667-670.
46. Fetnandez-Madrid F, Prasad AS, Oberleas D. Httectof zinc deficiency on nucleic acids. et)llagen. andnoncollagenous protein ofthe connective tissue. JLab Clin Med 1973:82:951-961.
47. Kelly GS. Spoils nutrition. In: Pizzorno J, MurrayM. eds. Te.xtbook of Naiural Medicine Vol 1. 2nded. Edinburgh: Churchill Livingstone: 2000:530.
48. Murray M. Encyclopedia of NutritionalSitpplenienis. Rocklin, CA: Prima Publishing:1996:188.
49. Rovati LC. Clinical research in osteoarthritis:design and results of short-term and long-term trialswith disease-modifying drugs. //;/ J Tissue React1992:14:243-251.
50. Muller-Fassbender H, Bach GL, Haase W. et al.Glucosamine sulfate eompared to ibuprofen inosteoanhritis ofthe knee. Osieoarihrliis Cartilage1994:2:61-69.
5 I. Qiu GX. Gao SN. Giacovelii G. et al. Efficacyand safety of glucosamine sulfate versusibuprofen in patients with knee osteoarthritis.Ar:.neimitielfor.\chnnii 1998:48:469-474.
52. Lopes Vaz A. Dt)uble-blind clinical evaluation ofthe relative efficacy of ibuprofen and glucosaminesulphate in the management of osteoarthrosisol" the knee in out-patients. Cnrr Med Res Opin1982:8:145-149.
53. Murray M. Encyclopedia of NiiiriiionalSupplements. Rocklin. CA: Prima Publishing:1996:339-342.
54. McCarty ME. Glucosamine for wound healing. MedHypotheses 1996:47:273-275.
Page 92 Alternalive Medicine Review • Volume 10, Number 2 • 2005
Review Plantar Fasciitis
55. Zupanets lA. Bezdeiko NV. Dcdukh NV. OtrishkoIA. Experimcnlal study (if the effect of glucosaminchydroehloiidc (ni metabolic and repair processes inct)niiective tissue structures. Eksp Klin Fanmikol2002:65:67-69. [Article in Russian|
i>6. Murray M. Pi//.oriio J. Glucosaniine. In: Piz/orno.1. Murray M. eds. Texihook of Natural MedicineVol 1. 2nd ed. Edinburgh: Churchill Livingstone;2000:761-765.
51. Blonstein .11,. Control of swelling in boxinginjuries. Practitioner l%y;203:206.
5S. Masson M. Broinelain in blunt Injuries of theloeomotor system. A study of observed applicationsin general practice. Fort.schr Mat \^95:\ 13:303-306. [Article in Gerniaii|
59. Kuniakura S, Yamashita M, Tsurufuji S. Effect ofbronielain on kaolin-induced inllamniation in rats.Eur J Pharmacol 1988:150:295-301.
60. Uchida Y. Katt)ri M. Independent consumption ofhigh and low molecular weight kininogens in vivo.Adv Exp Meci Hiol 1986:198>t A: 113-118.
61. Taussig SJ. Batkin S. Bronielain, the enzymecomplex of pineapple {Anaiias i-onuisns) and itsclinical application. An update. J Ethnopliarnmcol1988:22:191-203.
62. Gaby AR. The story (if bronielain. Nutr Healinfi1995:3.4.11.
63. Murray M. Pizzorno J. Bromelain. In: PizzornoJ. Murray M. eds. Te.xthook of Natural MedicineVol I. 2nd ed. Edinburgh: Churchill Livingstone:2000:622.
64. Kremer JM. Lawrence DA. Jubiz W. et al.Dietary iish oil and olive oil supplementation inpatients with rheumatoid arthritis. Clinical andimnuinologic effects. Arthritis Rheum 1990:33:810-820.
Alternative Medicine Review • Volume 10, Number 2 • 2005 Page 93





![Plantar Fasciitis€¦ · Plantar Fasciitis [ 2 ] Heel bone (Calcaneus) Area of pain Plantar fascia. What causes Plantar Fasciitis? Suddenly increasing activity levels, or being overweight,](https://img.pdfslide.us/doc/110x75/5f03fb297e708231d40bba04/plantar-fasciitis-plantar-fasciitis-2-heel-bone-calcaneus-area-of-pain-plantar.jpg)
























