Embed Size (px)
DESCRIPTION
dermatologyskin pityriass rosea
Citation preview

Pityriasis Rosea
Pityriasis rosea is an acute exanthematous eruption with a distinctive morphology and often with a characteristic self-limited course. First, a single (primary, or "herald") plaque lesion develops, usually on the trunk, and 1 or 2 weeks later a generalized secondary eruption develops in a typical distribution pattern; the entire process remits spontaneously in 6 weeks.
Epidemiology and Etiology
Age of Onset
10 to 43 years, but can occur rarely in infants and old persons.
Season
Spring and fall.
Etiology
Herpes virus type 7 is suspected.
History
Duration of Lesions
A single herald patch precedes the exanthematous phase; which develops over a period of 1 to 2 weeks. Pruritus—absent (25%), mild (50%), or severe (25%).
Physical Examination
Skin Lesions
Herald Patch
80% of patients. Oval, slightly raised plaque 2 to 5 cm, salmon-red, fine collarette scale at periphery; may be multiple
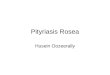
Pityriasis rosea Overview of exanthem of pityriasis rosea with the herald patch shown in the inset. There are papules and small plaques with oval configuration that follow the lines of cleavage. The fine scaling of the salmon-red papules cannot be seen at this magnification, while the collarette of the herald patch is quite obvious. Inset: Herald patch. An erythematous (salmon-red) plaque with a collarette scale on the trailing edge of the advancing border. Collarette means that scale is attached at periphery and loose toward the center of the lesion

Exanthem
Fine scaling papules and plaques with marginal collarette (Fig. 7-1). Dull pink or tawny. Oval, scattered, with characteristic distribution with the long axes of the oval lesions following the lines of cleavage in a "Christmas tree" pattern (Image 7-1). Lesions usually confined to trunk and proximal aspects of the arms and legs. Rarely on face.
Atypical Pityriasis Rosea
Lesions may be present only on the face and neck. The primary plaque may be absent, may be the sole manifestation of the disease, or may be multiple. Most confusing are the examples of pityriasis rosea with vesicles or simulating erythema multiforme. This usually results from irritation and sweating, often as a consequence of inadequate treatment (pityriasis rosea irritata).
Differential Diagnosis
Multiple Small Scaling Plaques
Drug eruptions (e.g., captopril, barbiturates); secondary syphilis (obtain serology); guttate psoriasis (no marginal collarette); erythema migrans with secondary lesions; erythema multiforme; and tinea corporis.
Laboratory Examination
Dermatopathology
Patchy or diffuse parakeratosis, absence of granular layer, slight acanthosis, focal spongiosis, microscopic vesicles. Occasional dyskeratotic cells with an eosinophilic homogeneous appearance. Edema of dermis, homogenization of the collagen. Perivascular infiltrate mononuclear cells.
Course
Spontaneous remission in 6 to 12 weeks or less. Recurrences are uncommon.
Management
Symptomatic
Oral antihistamines and/or topical antipruritic lotions for relief of pruritus. Topical glucocorticoids. May be improved by UVB phototherapy or natural sunlight exposure if treatment is begun in the first week of eruption. Short course of systemic glucocorticoids.